Anaes · Applied anatomy
Cranial nerves and autonomic ganglia
Also known as Cranial nerves · Twelve cranial nerves · Autonomic nervous system · Sympathetic chain · Stellate ganglion · Parasympathetic ganglia
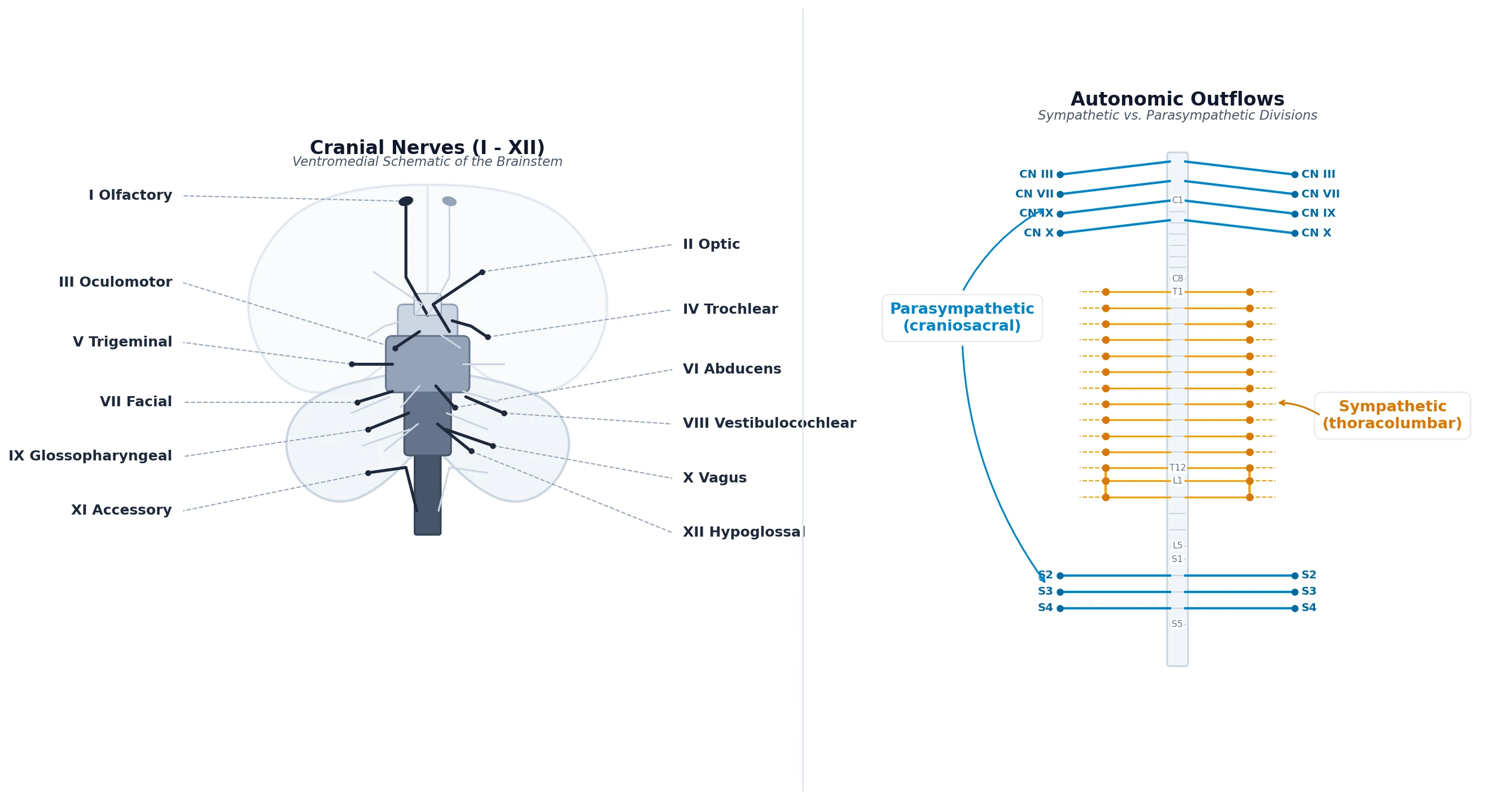
The cranial nerves and the autonomic nervous system together control the airway, the cardiovascular reflexes, the eye and the viscera — the four systems the anaesthetist manipulates most directly. The framework rests on six exam-critical ideas. First, there are TWELVE pairs of cranial nerves, classified as purely sensory (I olfactory, II optic, VIII vestibulocochlear), purely motor (III oculomotor, IV trochlear, VI abducens, XI accessory, XII hypoglossal) or mixed (V trigeminal, VII facial, IX glossopharyngeal, X vagus); the mixed nerves V, VII, IX and X carry the autonomic and sensory supply of the head, neck and most viscera. Second, the cranial nerves most relevant to anaesthesia are the TRIGEMINAL (V, the sensory supply of the face, nasal cavity and airway, in three divisions V1 ophthalmic, V2 maxillary, V3 mandibular — the latter also motor to the muscles of mastication), the FACIAL (VII, motor to the face, taste to the anterior two-thirds of the tongue, and parasympathetic to the lacrimal and submandibular glands), the GLOSSOPHARYNGEAL (IX, the sensory and taste of the posterior tongue, and the afferent limb of the gag reflex), the VAGUS (X, the parasympathetic supply of the heart, lungs and gut, the motor of the larynx via the recurrent laryngeal nerve, and the efferent limb of the gag reflex), and the HYPOGLOSSAL (XII, motor to the tongue). Third, the CAVERNOUS SINUS is a key venous compartment beside the sella turcica through which cranial nerves III, IV, V1, V2 and VI all pass with the internal carotid artery, so a cavernous-sinus lesion paralyses the eye-movement nerves and V1 while sparing the pupil (or, with the sympathetic carotid plexus, causes a Horner syndrome). Fourth, the AUTONOMIC NERVOUS SYSTEM has two complementary outflows: the SYMPATHETIC (thoracolumbar, from T1 to L2, with short pre-ganglionic fibres synapsing in the paravertebral sympathetic chain — including the stellate/cervicothoracic ganglion at the base of the neck — and the long post-ganglionic fibres travelling with the nerves and vessels) and the PARASYMPATHETIC (craniosacral, from cranial nerves III, VII, IX and X and the sacral S2-S4 outflow, with long pre-ganglionic fibres synapsing in terminal ganglia near or in the target organ). Fifth, the four cranial parasympathetic ganglia are the CILIARY (III, the pupil constrictor and ciliary muscle), the PTERYGOPALATINE (VII, the lacrimal gland and nasal mucosa), the SUBMANDIBULAR (VII, the submandibular and sublingual glands) and the OTIC (IX, the parotid gland); the vagus (X) supplies the heart, lungs and foregut directly through terminal ganglia. Sixth, the autonomic receptors determine drug action: acetylcholine acts on NICOTINIC receptors at all autonomic ganglia (and the neuromuscular junction) and on MUSCARINIC receptors at parasympathetic end-organs; noradrenaline acts on ALPHA and BETA adrenergic receptors at sympathetic end-organs. Built on the cranial-nerve compression-syndrome review (Reilly 2026), the combined autonomic-cranial neuropathy report (Tetik 2026), the cavernous-sinus perineural-spread report (Rohani 2026), the auricular vagus-nerve stimulation study (Zhang 2026), the aortic-baroreceptor autonomic-reflex study (Salman 2026), the trigeminal-facial nerve study (Vrapciu 2026), the stellate-ganglion-block study (Hollifield 2026), and the orbital-cranial-nerve MRI study (Arizono 2026).
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags

Why this matters
Cranial nerves explain awake airway topicalisation, laryngoscopy haemodynamics, post-thyroid voice change, oculocardiac reflex in squint surgery, and stellate/cervical plexus blocks. Autonomic ganglia link regional techniques to Horner syndrome and sympathetically maintained pain. [1]
The twelve — exam-focused map
| CN | Name | Core function | Anaesthetic hook |
|---|---|---|---|
| I | Olfactory | Smell | Not routinely tested under GA |
| II | Optic | Vision | Globe pressure, ischaemic optic neuropathy context |
| III | Oculomotor | Most EOM, pupil constrict | Raised ICP pupil; III palsy pattern |
| IV | Trochlear | Superior oblique | Vertical diplopia |
| V | Trigeminal | Face sensation; muscles of mastication | Airway topical (V2/V3); mastication |
| VI | Abducens | Lateral rectus | Raised ICP false-localising |
| VII | Facial | Face motor; taste anterior 2/3 | Mask trauma; nerve monitoring ENT |
| VIII | Vestibulocochlear | Hearing/balance | Middle-ear N2O issues (adjacent topic) |
| IX | Glossopharyngeal | Taste post 1/3; stylopharyngeus; afferent gag | Awake intubation topical / glossopharyngeal block |
| X | Vagus | Parasympathetic; larynx/pharynx | SLN/RLN; bradycardia; laryngospasm pathways |
| XI | Accessory | SCM, trapezius | Positioning / neck dissection |
| XII | Hypoglossal | Tongue motor | Forceful LMA/airway trauma; tongue deviation |
Trigeminal (V) — three divisions
| Division | Exit | Sensory field | Block / topical relevance |
|---|---|---|---|
| V1 Ophthalmic | Superior orbital fissure | Forehead, cornea, upper lid | Oculocardiac afferent |
| V2 Maxillary | Foramen rotundum | Midface, upper teeth, palate | Sphenopalatine / topical nasal |
| V3 Mandibular | Foramen ovale | Lower face, anterior 2/3 tongue sensation, lower teeth | Inferior alveolar; awake FOI tongue/pharynx |
IX and X for the airway
- Glossopharyngeal (IX): afferent of gag from posterior third of tongue and pharynx; topical or bilateral glossopharyngeal block enables awake intubation tolerance.
- Vagus (X): superior laryngeal nerve (internal sensory above cords; external motor to cricothyroid) and recurrent laryngeal nerve (other intrinsics + sensory below cords). Bilateral RLN injury → stridor.
- Combined topical recipe (concept): nasal (V2), tongue/pharynx (IX + V3), larynx above cords (SLN internal), trachea (RLN / spray as you go). [4]
Autonomic ganglia of exam interest
| Structure | Location | Significance |
|---|---|---|
| Stellate (cervicothoracic) ganglion | Anterior to C7 transverse process / neck of first rib | Stellate block → Horner, warm dry arm; complications: vascular, neuraxial, pneumothorax |
| Superior cervical ganglion | High neck | Head/neck sympathetics |
| Ciliary ganglion | Orbit | Pupil; parasympathetic hitch-hiking |
| Sphenopalatine ganglion | Pterygopalatine fossa | Facial pain, nasal autonomic |
Reflexes
| Reflex | Afferent | Efferent | Trigger | Response |
|---|---|---|---|---|
| Oculocardiac | Trigeminal V1 | Vagus | Traction on extraocular muscles / pressure on globe | Bradycardia ± asystole — stop traction, atropine ready |
| Gag | IX | X | Posterior tongue/pharynx | Gag |
| Laryngospasm | X (irritant) | X | Light anaesthesia, secretions, blood | Cord adduction — deepen, remove stimulus, CPAP, muscle relaxant if needed |
| Diving / cold face | Trigeminal | Vagus | Cold water on face | Bradycardia |
Horner syndrome
Ipsilateral ptosis, miosis, anhidrosis from interrupted cervical sympathetics — expected after successful stellate block; red flag after interscalene (stellate/sympathetic spread) or base-of-skull pathology; also with lower-trunk brachial plexus injury involving T1. [7]
SAQ scaffold
- Map CN V, IX, X for awake FOI topicalisation.
- RLN vs SLN motor/sensory.
- Oculocardiac reflex pathway and management.
- Stellate ganglion location and Horner triad.
- Differentiate unilateral vs bilateral RLN injury. [8]
Viva phrases
- "Trace the oculocardiac reflex." → "Afferent long/short ciliary nerves → ciliary ganglion → V1 → trigeminal ganglion → main sensory nucleus; efferent via vagus to heart."
- "Why does interscalene cause Horner?" → "Local anaesthetic spreads to cervical sympathetic chain / stellate." [1]
Common traps
- Assigning all laryngeal muscles to RLN without excepting cricothyroid.
- Treating oculocardiac with pressors first instead of releasing traction.
- Missing IX in awake airway plans.
- Confusing Horner with pure oculomotor ptosis (pupil large in III palsy, small in Horner). [2]

CN V
- Face sensation
- V2/V3 airway topical
- Mastication (V3)
- Oculocardiac afferent V1
CN IX
- Gag afferent
- Posterior third tongue
- Stylopharyngeus
- Awake FOI key
CN X
- SLN + RLN
- Parasympathetic
- Laryngospasm efferent
- Bradycardia
Stellate
- C7 / first rib neck
- Horner if blocked
- CRPS / vascular uses
- Serious injection risks
Integrated exam drill sheet
Sixty-second version
Say the definition, the critical number or sequence, the main clinical use, and the top red flag. Stop. If you cannot do this without notes, the topic is not yet learnable.
Three-minute version
Add mechanism, a comparison table spoken aloud, one special population, and one crisis stem with first actions. This is the standard viva unit.
Ten-minute mastery version
Add equipment detail or procedural steps, evidence limits, second-line options, and a teach-the-junior summary. This is Final long-case depth.
Written SAQ timing
For a 10-minute SAQ, spend one minute planning headings, seven minutes writing, two minutes checking hard stops and units. Headings should mirror examiner dimensions: definition, mechanism or anatomy, clinical application, complications, special situations.
Common mark-losing behaviours
- Lists without mechanisms
- Mechanisms without clinical action
- Doses without route or monitoring
- Landmarks without injury consequences
- Device talk without re-enable or backup plans
- Absolute claims where practice is protocol-dependent
Positive mark-gaining behaviours
- Numbers with units and approximate ranges
- Explicit assumptions for equations
- Side-by-side comparisons
- Named hard contraindications
- Monitoring endpoints
- Clear escalation
Cross-specialty board alignment
ANZCA Primary and Final, FRCA Primary and Final, ABA, EDAIC and FCAI all test these leaves repeatedly because they are portable across subspecialties. A candidate who owns flow physics, electrical safety, neck and neuraxial anatomy, vaporiser principles and core adjunct pharmacology can survive stems in ICU transfer, obstetric haemorrhage, thoracic lists and outpatient dental anaesthesia alike.
Personal rehearsal script
Read the AnswerCard twice. Cover it and rewrite it from memory. Speak the red flags. Draw one table from memory. Answer one hostile interruption. Then move on. Spaced repetition beats marathon re-reading.
Safety culture close
Every technical topic ends in patient safety: do not expand closed gas spaces, do not dilate arteries, do not leave ICD therapies off, do not apply Poiseuille in turbulence, do not ignore conus level, do not tip a full vaporiser back into service without protocol, and do not stack serotonergic weak opioids casually. Knowledge is only exam-pass when it prevents harm.
Topic-specific mastery addendum
Layered recall sequence
- Recite the AnswerCard from memory.
- Draw the key table (layers, nerves, or vaporiser types) from blank paper.
- Speak two viva stems with full answers.
- List every red flag without looking.
- Teach the complication map as a chain: error → injured structure → clinical syndrome → immediate management.
Procedural narration standard
Narrate as if a consultant is watching: position, asepsis or machine check, landmark or ultrasound view, needle or dial action, endpoint, confirmation test, contingency if endpoint missing, and documentation. This narration style scores in OSCE-like and viva settings because it proves usable competence rather than passive recognition.
Numbers and relations to keep hot
Keep a personal card of the five hottest facts for this leaf and revisit them daily for a week. For neuraxial spaces that means conus level, Tuffier estimate, midline tissue sequence, epidural contents and neonatal difference. For cranial nerves that means V/IX/X airway map, SLN versus RLN, oculocardiac pathway and Horner triad. For vaporisers that means splitting ratio, SVP contrast for desflurane, temperature compensation idea, keyed fillers/interlocks and tip-over danger.
Error museum
Build an "error museum" of classic failures: spinal at L1/2 in adults; dilating an artery; leaving vaporiser tipped in service; missing bilateral RLN injury risk; assuming magnet behaviour is universal; ignoring delayed respiratory depression after neuraxial morphine. Each exhibit should have the false belief, the correct belief, and the protective habit.
Link-forward reading
After mastering this leaf, deliberately link to the next clinical topic in the same sitting: neuraxial anatomy to CSE and caudal; cranial nerves to awake FOI and eye surgery reflexes; vaporisers to volatile agent pharmacology and circle-system low flow. Linked encoding is more durable than isolated topics.
Worked airway and reflex stems
Stem — awake fibreoptic intubation topical plan. Nose and palate: V2. Tongue and oropharynx: V3 and IX. Larynx above cords: internal branch of superior laryngeal nerve. Trachea: recurrent laryngeal nerve or spray-as-you-go. Saying the nerves while spraying proves a system.[1]
Stem — squint surgery bradycardia. Oculocardiac reflex: afferent trigeminal V1 via ciliary pathways, efferent vagus. First action is stop traction; give anticholinergic if bradycardia persists; deepen anaesthesia as appropriate; communicate with surgeon. [3]
Stem — post-thyroidectomy stridor. Bilateral recurrent laryngeal nerve injury can obstruct. Unilateral injury causes hoarseness. Cricothyroid is external SLN; other intrinsics are RLN. Airway evaluation and urgent ENT involvement may be required. [4]
Stem — interscalene block with ptosis and miosis. Horner syndrome from cervical sympathetic or stellate spread: ptosis, miosis, anhidrosis. Usually self-limited with local anaesthetic, but document and reassure while watching for more serious injectate misplacement signs. [5]
Stem — gagging despite topical. Likely missed glossopharyngeal territory on the posterior third of tongue or pharynx; re-topicalise IX field rather than only spraying the cords again. [6]
Red flags
References
- [1]Reilly M, et al. Neurovascular Compression Syndromes of Cranial Nerves: A Multidisciplinary Guide to Management Brain Sci, 2026.PMID 42352577
- [2]Tetik D, et al. Combined autonomic and cranial neuropathy following radiofrequency ablation for trigeminal neuralgia J Fr Ophtalmol, 2026.PMID 42361525
- [3]Rohani MFM, et al. Follicular Thyroid Carcinoma with Cavernous Sinus Metastasis and Perineural Spread: A Rare Manifestation of Radioiodine-refractory Disease Mol Imaging Radionucl Ther, 2026.PMID 42334179
- [4]Zhang W, et al. Transcutaneous auricular vagus nerve stimulation in adult abdominal epilepsy associated with ketosis-prone diabetes: A case report Medicine (Baltimore), 2026.PMID 42363487
- [5]Salman S, et al. Do stretch sensors expressed by aortic baroreceptors interact with circulating estradiol to mediate baroreflex sensitivity in hypertension? Front Neurosci, 2026.PMID 42359345
- [6]Vrapciu AD, et al. Trigeminal-Facial Nerve Anatomical Connections and Their Clinical Value: A Narrative Review Diagnostics (Basel), 2026.PMID 42351514
- [7]Hollifield M, et al. The Stellate Ganglion Block for PTSD: A Retrospective Clinical Case Series Int J Environ Res Public Health, 2026.PMID 42354289
- [8]Arizono E, et al. Visualization of Cranial Nerves in the Orbit Using Fat-Suppressed 3D FLAIR MR Imaging AJNR Am J Neuroradiol, 2026.PMID 42034568