Anaes · Anaesthetic adjuncts
Phenylephrine — the pure alpha-1 vasopressor
Also known as Phenylephrine · Neosynephrine · Pure alpha-1 agonist · Selective alpha-1 vasopressor · Obstetric spinal hypotension vasopressor · Non-catecholamine alpha-1 agonist
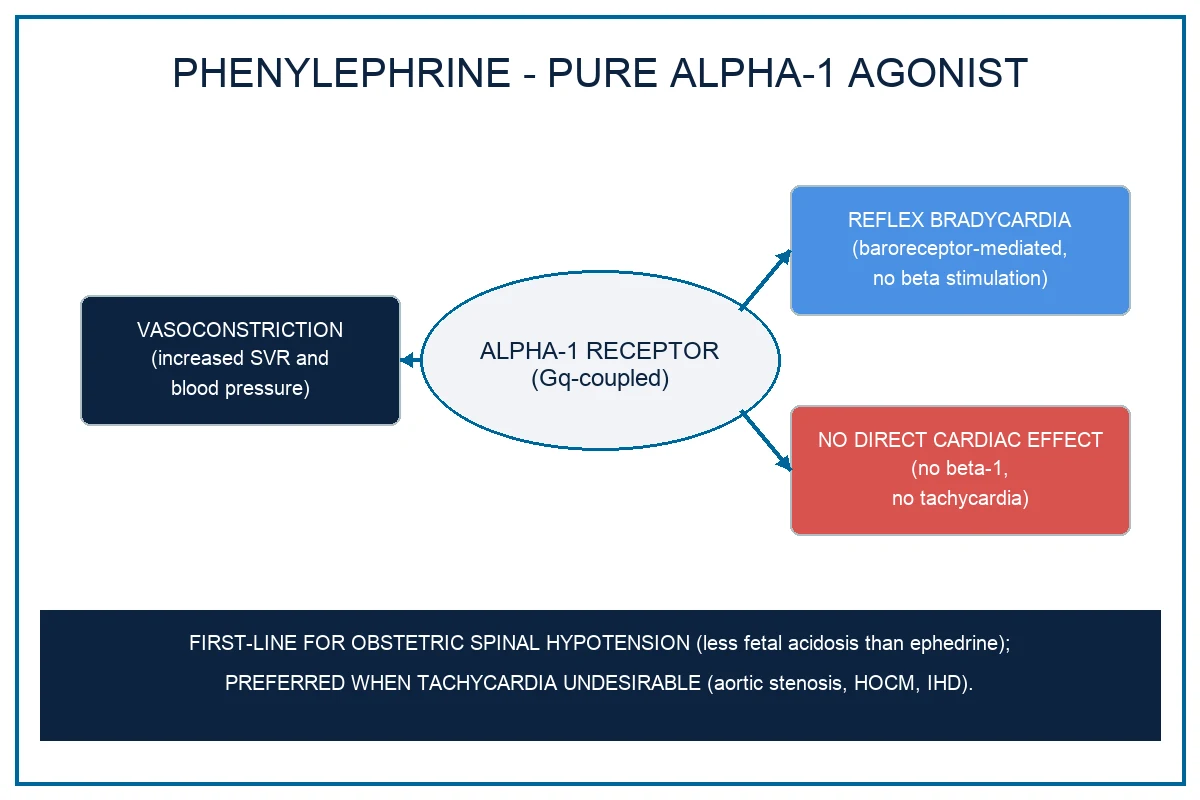
Phenylephrine is the prototype PURE ALPHA-1 ADRENERGIC AGONIST with no beta-1, no beta-2 and no alpha-2 activity at clinical doses, and this single pharmacological fact shapes everything it does. It is a synthetic phenylethylamine that is NOT a catecholamine (it lacks the 3,4-dihydroxyl catechol ring) and is therefore not a substrate for catechol-O-methyltransferase (COMT) — it is instead metabolised by monoamine oxidase (MAO), giving it a longer duration than the catecholamines and the unusual property of being orally active. It activates the alpha-1 receptor (Gq-coupled), driving phospholipase C, inositol triphosphate (IP3) and diacylglycerol (DAG), raising intracellular calcium and producing arteriolar and venous vasoconstriction, an increased systemic vascular resistance (SVR) and a rise in blood pressure. Because it has no beta-1 effect, the rise in blood pressure is met by a BARORECEPTOR-MEDIATED REFLEX BRADYCARDIA and the cardiac output (CO) may fall. The exam-critical roles follow directly: phenylephrine is the FIRST-LINE vasopressor for obstetric spinal-induced hypotension in caesarean section because it produces a higher umbilical artery pH than ephedrine (Lee 2002; Ngan Kee 2009; Singh 2020) — unlike ephedrine, it does not cross the placenta to drive fetal beta stimulation and metabolic acidosis. It is the vasopressor of choice whenever tachycardia is undesirable (aortic stenosis, hypertrophic obstructive cardiomyopathy, ischaemic heart disease), and it is used as a nasal decongestant, a mydriatic and (classically) to terminate supraventricular tachycardia through its reflex vagal effect. Onset is less than 1 minute after IV bolus, duration 15 to 20 minutes, IV bolus 50 to 100 micrograms (up to 200 micrograms), infusion 0.5 to 5 micrograms per kg per minute.
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags
Why this is examined
Intraoperative hypotension is the single most common haemodynamic disturbance of anaesthesia, and the vasopressor the anaesthetist reaches for shapes not only the blood pressure but also the heart rate, the cardiac output, the afterload and — in the obstetric patient — the fetal wellbeing. Phenylephrine occupies a precisely defined niche in the vasopressor formulary because it is the prototype pure alpha-1 adrenergic agonist. Knowing that single pharmacological fingerprint lets the candidate predict exactly when phenylephrine is the right drug and when it is the wrong one, and it makes the vasopressor-selection question one of the highest-yield, most-asked pharmacology questions across the ANZCA Primary (autonomic pharmacology, sympathomimetic amines), ANZCA Final (perioperative vasopressor selection, obstetric spinal hypotension), FRCA, EDAIC, FCAI and FCA(SA) exams. [1]
The contexts that drive the viva and SAQ territory are: [1]
- Obstetric spinal-induced hypotension in caesarean section. Phenylephrine is preferred over ephedrine on the basis of fetal acid-base status, established by the Lee 2002 Cochrane quantitative systematic review[1] and confirmed by Ngan Kee's placental-transfer study[6] and the Bayesian network meta-analyses of Singh 2020 and Fitzgerald 2020[10][11].
- Vasoplegia of any cause where tachycardia is undesirable. Aortic stenosis, hypertrophic obstructive cardiomyopathy (HOCM), ischaemic heart disease, and the regurgitant valve lesions — phenylephrine's reflex bradycardia is here a feature, not a bug.
- Vasodilatory hypotension after anaesthesia induction, in sepsis, and after cardiopulmonary bypass — phenylephrine is a reasonable short-term bridge while the cause is addressed, with the caveat that noradrenaline is preferred when the cardiac output also needs supporting (Morelli 2008 RCT[5]).
- The non-vasopressor uses that examiners love as one-line stem checks: topical nasal decongestant (alpha-1 mucosal vasoconstriction, also the basis of preparing the nasal mucosa for awake fibreoptic intubation), mydriatic, and the classical pharmacological treatment of supraventricular tachycardia (the induced rise in blood pressure triggers the baroreceptor-vagal reflex that terminates the re-entry circuit).
The candidate who can derive every clinical effect from the single fact "pure alpha-1, no beta" — the reflex bradycardia, the fall in cardiac output, the fetal pH advantage, the use in HOCM, the wrong choice in low-output shock — owns this topic. [1]
Structure and receptor pharmacology — the non-catecholamine that defines "pure alpha-1"
Phenylephrine is a synthetic phenylethylamine — structurally a benzene ring with a two-carbon ethylamine side chain (the phenylethylamine backbone shared with adrenaline, noradrenaline, dopamine, ephedrine and amphetamine). The decisive structural fact is that phenylephrine is NOT a catecholamine: it lacks the 3,4-dihydroxyl groups on the aromatic ring that define the catecholamines (adrenaline, noradrenaline, dopamine, isoprenaline, dobutamine, dopexamine). The structural consequences are mechanistic and exam-defining: [1]
- Not a substrate for catechol-O-methyltransferase (COMT). COMT is the enzyme that methylates the 3-hydroxyl of the catechol ring and rapidly inactivates the catecholamines in the liver, kidneys and other tissues. Because phenylephrine has no catechol ring, COMT cannot methylate it, and its duration of action (15 to 20 minutes by the IV route) is much longer than the catecholamines (adrenaline, noradrenaline: 2 to 3 minutes).
- Metabolised by monoamine oxidase (MAO). Phenylephrine is instead deaminated by MAO in the liver, gut and other tissues, with the metabolites conjugated and excreted renally. The MAO dependence is the basis of the MAOI pharmacokinetic interaction (potentiation and prolongation of effect; the dose must be reduced).
- Orally active. Because it is not destroyed by COMT in the gut and liver, phenylephrine survives first-pass metabolism and is the only directly-acting alpha-1 agonist that is clinically useful by the oral route (the historical basis of its over-the-counter use as an oral decongestant, and now a substitute for pseudoephedrine which has been withdrawn in many jurisdictions because of its use in illicit amphetamine manufacture). [1]
- No 3,4-dihydroxyl ring → NOT a COMT substrate
- Metabolised by MAO (half-life about 5 min; duration 15 to 20 min)
- Orally active
- Pure direct alpha-1 agonism
- No placental transfer to any clinically important extent
- No tachyphylaxis (direct action)
- Catechol ring → rapidly inactivated by COMT (and MAO)
- Half-life 2 to 3 min; duration a few minutes
- Inactive orally
- Noradrenaline: alpha-1 + alpha-2 + weak beta-1; adrenaline: full alpha + beta dose-dependent
- Cross placenta; catecholamines do reach fetal circulation
The receptor profile is what makes phenylephrine the textbook answer for "pure alpha-1". It is the cleanest example of a pure alpha-1 agonist in clinical use. It has essentially no beta-1, no beta-2 and no alpha-2 activity at clinical doses, which distinguishes it sharply from: [1]
- Noradrenaline — alpha-1, alpha-2 and weak beta-1.
- Adrenaline — alpha-1, alpha-2, beta-1 and beta-2 (dose-dependent).
- Metaraminol — predominantly alpha-1 with some indirect beta-1 (releases noradrenaline).
- Ephedrine — mixed alpha and beta, largely indirect (releases noradrenaline from nerve terminals).
- Dopamine — dose-dependent D1, beta-1, alpha-1.
- Vasopressin — V1 receptor, a completely non-adrenergic pathway. [1]
This single fact — pure alpha-1, no beta, no alpha-2 — is the answer to half the phenylephrine MCQs. [1]
Mechanism of action — the Gq/PLC/IP3/DAG cascade and the reflex arc
The alpha-1 receptor is a Gq-coupled G-protein-coupled receptor on vascular smooth muscle (alpha-1A, alpha-1B and alpha-1D subtypes, all coupled to Gq). Phenylephrine binds the receptor and activates phospholipase C (PLC), which hydrolyses membrane phosphatidylinositol 4,5-bisphosphate (PIP2) into inositol triphosphate (IP3) and diacylglycerol (DAG). The IP3 binds the IP3 receptor on the sarcoplasmic reticulum and releases calcium into the cytoplasm; the DAG activates protein kinase C. The raised intracellular calcium binds calmodulin, the calcium-calmodulin complex activates myosin light-chain kinase (MLCK), MLCK phosphorylates the regulatory myosin light chain, and the smooth muscle contracts. The result is constriction of both the arterioles (raising systemic vascular resistance) and the veins (increasing venous return and preload).[2]
Because phenylephrine has no beta-1 activity, it produces no direct chronotropy or inotropy — no direct stimulation of the sinoatrial node, the atria, the AV node or the ventricles. Because it has no beta-2 activity, it produces no skeletal-muscle vasodilation and no bronchodilation. And because it has no alpha-2 activity, it produces no central sympatholysis (in contrast to clonidine and dexmedetomidine). The pharmacology is, in effect, a single tool — vasoconstriction — which is both its strength (predictable, pure, haemodynamically clean in the right patient) and its limitation (no cardiac stimulation when cardiac output is the problem). [1]
Haemodynamic effects — the fingerprint the candidate must be able to draw
The haemodynamic signature of phenylephrine follows directly from its pure alpha-1 mechanism, and the exam candidate must be able to draw it on a graph: [1]
| Variable | Effect | Mechanism |
|---|---|---|
| Systemic vascular resistance (SVR) | Rises | Alpha-1 arteriolar vasoconstriction |
| Blood pressure (BP) | Rises | Higher SVR; venoconstriction raises preload |
| Heart rate (HR) | Falls (reflex bradycardia) | Baroreceptor-mediated vagal reflex; no direct beta-1 |
| Stroke volume (SV) | Falls or unchanged | Increased afterload; preload may rise slightly from venoconstriction |
| Cardiac output (CO) | Falls or no change | Reflex bradycardia plus increased afterload |
| Pulmonary vascular resistance | May rise | Non-selective alpha-1 vasoconstriction includes the pulmonary bed |
| Renal and splanchnic perfusion | May fall at high doses | Non-selective alpha-1 vasoconstriction |
The reflex bradycardia is the pharmacological fingerprint of phenylephrine. The mechanism is the baroreceptor reflex: the sudden rise in blood pressure stretches the carotid sinus and aortic arch baroreceptors, the increased firing travels via the glossopharyngeal (CN IX) and vagus (CN X) afferents to the nucleus tractus solitarius in the medulla, the medulla increases vagal efferent output to the sinoatrial node, and the heart rate falls. The reflex can be profound — a generous bolus for spinal hypotension may produce a normal blood pressure with a heart rate in the forties or fifties. It can be attenuated by an anticholinergic (glycopyrrolate 0.2 to 0.4 mg or atropine 0.5 to 0.6 mg) if symptomatic, but the cleaner solution is to titrate to the haemodynamic target rather than to bolus aggressively. Ngan Kee's glycopyrrolate pre-treatment study showed that an anticholinergic given before a phenylephrine infusion blunts the reflex bradycardia and stabilises the heart rate, at the cost of a slight tachycardic offset.[8]
The cardiac output may fall for two additive reasons: the reflex bradycardia reduces the number of beats per minute, and the increased afterload (the higher SVR the heart must pump against) reduces the stroke volume. The net effect on cardiac output is usually a decrease or no change — the mirror image of a beta-agonist like adrenaline or dobutamine, which raises the heart rate and the cardiac output. [1]
A practical contrast cements the point. A pure beta-agonist raises the heart rate and the cardiac output but does little to the SVR (and may lower it through beta-2 vasodilation). A pure alpha-1 agonist raises the SVR and the blood pressure but lowers the heart rate and may lower the cardiac output. Noradrenaline, with both alpha-1 and weak beta-1, raises the SVR and supports the cardiac output, which is why it is the preferred first-line vasopressor in vasodilatory shock where both are needed. Phenylephrine is the right drug when the problem is pure vasoplegia with a heart rate that should not rise; noradrenaline is the right drug when the problem is vasoplegia with a cardiac output that needs supporting. The Morelli 2008 RCT of phenylephrine versus norepinephrine for initial support of septic shock showed comparable systemic effects and a non-inferior lactate clearance, suggesting that in a selected population phenylephrine is not inferior — but noradrenaline remains the Surviving Sepsis first-line because the cardiac-output support matters in the broader shock population.[5]
Pharmacokinetics and dosing
Phenylephrine has a short, predictable pharmacokinetic profile that suits titrated bolus or infusion use. The exam-relevant values are: [1]
- Onset of action after IV bolus: less than 1 minute (essentially immediate).
- Duration of a bolus: 15 to 20 minutes (longer than the catecholamines by virtue of being a non-catecholamine; longer than a typical adrenaline or noradrenaline bolus).
- Elimination half-life: about 5 minutes — because phenylephrine is rapidly metabolised by monoamine oxidase (MAO).
- Metabolism: deamination by MAO in the liver and gut; conjugated metabolites excreted renally. NOT metabolised by COMT (no catechol ring). NOT metabolised by plasma cholinesterase (a common wrong answer).
- Excretion: renal, predominantly as inactive conjugates. [1]
Because it is so short-acting, a single bolus is good for an acute, transient blood-pressure drop (a brief spinal-induced dip, a transient surgical stimulus) but sustained hypotension is better managed by a continuous infusion, titrated to the blood pressure.[3]
The practical dosing ranges the exam candidate must know: [1]
| Route | Dose | Use |
|---|---|---|
| IV bolus | 50 to 100 micrograms (up to 200 micrograms), titrated to effect | Acute perioperative vasodilatory hypotension; obstetric spinal dip; intra-procedural transient hypotension |
| IV infusion | 0.5 to 5 micrograms per kg per minute (often quoted as 0.5 to 1.5 for obstetrics; up to 5 for refractory vasoplegia), titrated to MAP | Sustained hypotension: ongoing spinal vasoplegia, post-induction, post-CPB, ICU |
| IM / SC | 2 to 5 mg | Largely historical; rarely used in modern anaesthetic practice |
| Topical (nasal) | 0.25 to 1 per cent solution | Nasal decongestion; mucosal vasoconstriction before nasal instrumentation (awake fibreoptic intubation) |
| Ophthalmic | 2.5 to 10 per cent drops | Mydriatic; ophthalmic examination and surgery (the 10 per cent preparation carries a significant systemic absorption risk and is avoided in the elderly, the pregnant and the cardiovascularly compromised) |
| Oral | 10 mg every 4 to 6 hours (adult decongestant dosing) | Symptomatic nasal decongestion; the only directly-acting alpha-1 agonist that is clinically useful orally |
The obstetric spinal hypotension context is the most-examined and the most-precise application. Ngan Kee's 2004 phenylephrine infusion-regimen comparison established that a prophylactic infusion started immediately after the spinal and titrated to keep the systolic blood pressure at or near baseline gives smoother haemodynamics, less nausea and vomiting, and better fetal acid-base status than a reactive bolus strategy.[3] The 2013 closed-loop feedback computer-controlled infusion study extended this principle, showing that a computer-titrated phenylephrine infusion maintains the maternal blood pressure more precisely than manual titration, with fewer hypotensive episodes and less total phenylephrine used.[7] The starting infusion rate is typically within the 0.5 to 1.5 micrograms per kg per minute range, titrated briskly in the first few minutes after the spinal when the hypotension is at its peak, and a typical obstetric prophylactic dose is around 50 to 100 micrograms per minute in the first few minutes after the spinal, tapering as the block stabilises.
Clinical indications
The clinical indications for phenylephrine group into categories, all flowing from its pure alpha-1 pharmacology. [1]
Obstetric spinal-induced hypotension in caesarean section — FIRST-LINE
This is the single best-studied indication, the source of the highest-yield obstetric anaesthesia exam fact, and the modern standard of care. Neuraxial blockade in the parturient produces a sudden sympathetic block with profound vasodilation and a fall in systemic vascular resistance; the hypotension that results is nearly universal without vasopressor support and threatens uteroplacental perfusion. The question of WHICH vasopressor to use was, for decades, answered by ephedrine, but the modern evidence firmly favours phenylephrine on the basis of fetal acid-base status. The landmark is the Lee 2002 quantitative Cochrane systematic review of ephedrine versus phenylephrine for the management of hypotension during spinal anesthesia for cesarean delivery, which found that phenylephrine produced a higher umbilical artery pH than ephedrine (mean difference approximately 0.04 pH units), with no difference in maternal nausea and vomiting.[1]
The mechanism of the fetal difference is the heart of the matter. Ephedrine is a mixed alpha and beta agonist that crosses the placenta (lipid-soluble non-catecholamine, partly un-ionised). Once in the fetal circulation, its beta-1 stimulation drives fetal metabolism and produces a metabolic acidosis, reflected in a lower umbilical artery pH and a higher base deficit at delivery. Phenylephrine, acting purely on alpha-1 receptors, improves the maternal blood pressure and therefore the uteroplacental perfusion WITHOUT the fetal beta stimulation — it does not cross the placenta to any clinically important extent. The net result is a HIGHER umbilical artery pH with phenylephrine than with ephedrine, a finding reproduced across multiple trials and meta-analyses (Ngan Kee 2009 placental-transfer study[6]; Singh 2020 Bayesian network meta-analysis[10]; Fitzgerald 2020 systematic review and network meta-analysis[11]) and now embedded in obstetric anaesthesia guidelines worldwide.
The practical technique is to give phenylephrine proactively — as an infusion started immediately after the spinal and titrated to keep the maternal systolic blood pressure at or near baseline — rather than reactively treating hypotension once it has developed. The Cooper 2007 trial of intravenous vasopressors on the spread of spinal anaesthesia and fetal acid-base equilibrium confirmed that the vasopressor choice and timing shape not only the maternal blood pressure but also the spread of the block and the fetal acid-base status, reinforcing the case for a proactive phenylephrine strategy.[4] The reflex bradycardia is expected and is usually well tolerated in the young, fit obstetric patient; if it is severe, slowing the infusion or a small dose of an anticholinergic is sufficient. Ngan Kee's glycopyrrolate pre-treatment study showed that an anticholinergic given before the phenylephrine infusion blunts the reflex bradycardia and is a reasonable option where the heart rate is expected to fall uncomfortably.[8]

Vasodilatory hypotension of any cause
Phenylephrine directly corrects the mechanism of vasodilatory hypotension by raising the SVR. The contexts are: [1]
- The vasoplegia of spinal and epidural anaesthesia (the obstetric and the non-obstetric).
- The vasodilation of intravenous and volatile induction agents — propofol is the classic vasodilator; thiopental less so but still present; volatiles all reduce SVR.
- The vasodilatory component of septic shock — phenylephrine is not first-line (noradrenaline is, by Surviving Sepsis guidance), but the Morelli 2008 RCT demonstrated non-inferiority of phenylephrine to norepinephrine for initial support in a selected septic-shock population, and phenylephrine is a reasonable short-term bridge or add-on agent where noradrenaline is producing excessive tachyarrhythmia.[5]
- The vasoplegic syndrome after cardiopulmonary bypass — phenylephrine boluses are commonly used intraoperatively to maintain perfusion pressure during the rewarming and the early post-bypass period, although vasopressin and noradrenaline are preferred for sustained post-CPB vasoplegia where receptor down-regulation blunts the alpha response.
Where tachycardia is undesirable — the cardiac patient
A second high-yield indication is the patient in whom a rise in heart rate would be dangerous. The classic examples are: [1]
- Severe aortic stenosis. The stroke volume is fixed and the cardiac output is heart-rate-dependent within a narrow window — too fast and diastolic filling is cut short and myocardial oxygen demand rises, too slow and the cardiac output falls. A tachycardic response to hypotension (or to a tachycardic vasopressor like ephedrine) is poorly tolerated, while phenylephrine, by raising the SVR and producing a reflex bradycardia, can improve both the blood pressure and the coronary perfusion without driving the heart rate up.
- Hypertrophic obstructive cardiomyopathy (HOCM). The problem is dynamic left ventricular outflow tract obstruction, which is worsened by anything that reduces the preload, reduces the afterload, or increases the contractility. Phenylephrine is almost uniquely well suited here: it raises the afterload (which reduces the outflow-tract gradient by increasing the ventricular volume), it raises the venous return and preload (by venoconstriction, which further distends the ventricle and reduces the gradient), and it produces a reflex bradycardia that lengthens diastole and improves coronary filling. A vasopressor that raised the heart rate or the contractility (adrenaline, dobutamine, isoprenaline) would worsen the obstruction.
- Ischaemic heart disease. Tachycardia is the single most powerful driver of myocardial oxygen demand and the single most powerful shortener of diastole (during which the myocardium is perfused). A vasopressor that raises the heart rate to correct a blood-pressure drop may trade one problem (hypotension) for a worse one (ischaemia). Phenylephrine restores the coronary perfusion pressure (by raising the diastolic blood pressure, against which the coronary bed is perfused) while lowering or not changing the heart rate, which is the more favourable oxygen-balance trade.
- Regurgitant valve lesions (mitral and aortic regurgitation). A slower heart rate favours forward flow and a lower afterload favours the regurgitant volume reduction, so the indication is weaker than in aortic stenosis or HOCM (the afterload rise is mechanically less favourable), but in the patient who is both vasodilated and tachycardic the phenylephrine-induced reflex bradycardia is still useful. [1]

Non-vasopressor uses — the exam short-question bank
These flow from the same alpha-1 vasoconstriction and pupillary dilator smooth-muscle contraction: [1]
- Topical nasal decongestant. Alpha-1 mucosal vasoconstriction shrinks the nasal mucosa and relieves congestion, and (of anaesthetic interest) prepares the nasal mucosa for an awake fibreoptic intubation by reducing bleeding and oedema. Phenylephrine nasal spray is now used in many jurisdictions as a substitute for pseudoephedrine (which has been restricted because of its diversion to illicit amphetamine manufacture).
- Mydriatic. Alpha-1 stimulation of the radial dilator muscle of the iris produces pupillary dilation for ophthalmic examination and surgery. The 2.5 per cent preparation is standard; the 10 per cent preparation carries a significant systemic absorption risk (rise in blood pressure, reflex bradycardia, pulmonary oedema in susceptible patients) and is avoided in the elderly, the pregnant and the cardiovascularly compromised.
- Treatment of supraventricular tachycardia (SVT). This is the classical pharmacological manoeuvre, now rarely first-line (adenosine, vagal manoeuvres and electrical cardioversion have displaced it) but still an exam favourite. The principle is elegant: by raising the blood pressure, phenylephrine triggers the baroreceptor-vagal reflex, and the surge in vagal tone terminates the AV-nodal re-entry circuit that sustains the common SVTs (AVNRT and AVRT). The technique requires a continuous ECG and invasive blood-pressure monitoring, a controlled bolus titrated to a target blood pressure (typically systolic 160 mmHg), and immediate termination when the rhythm converts or the blood-pressure target is reached. It is contraindicated in the patient with significant structural heart disease or aortic stenosis (the afterload rise is dangerous) and in whom the rise in blood pressure cannot be tolerated. [1]
Comparison with other vasopressors — the spectrum
Phenylephrine is best understood by comparison, because the vasopressors form a spectrum defined by their receptor activity and the comparison is a frequent examination structure. [1]
- Receptor: PURE alpha-1
- Direct action
- Heart rate: REFLEX BRADYCARDIA
- CO: falls or unchanged
- Placenta: minimal transfer
- Tachyphylaxis: NONE
- Duration: 15 to 20 min
- Obstetric first-line on fetal pH
- Receptor: alpha-1 + alpha-2 + weak beta-1
- Direct action
- Heart rate: small rise or unchanged (beta-1 offsets reflex)
- CO: supported
- Placenta: some transfer
- Tachyphylaxis: minimal
- Duration: short (catecholamine)
- First-line for vasodilatory shock; emerging obstetric alternative
- Receptor: MIXED alpha + beta (largely indirect via noradrenaline release)
- Indirect dominant
- Heart rate: RISES (beta-1)
- CO: rises
- Placenta: CROSSES, fetal acidosis
- Tachyphylaxis: YES (store depletion)
- Duration: 30 to 60 min
- Use: hypotension WITH bradycardia only
- Versus ephedrine. Ephedrine is a mixed alpha and beta agonist that acts largely indirectly by releasing noradrenaline from sympathetic nerve terminals. It raises the blood pressure through a combination of vasoconstriction (alpha) and cardiac stimulation (beta-1), so it raises the heart rate and the cardiac output as well as the SVR. Phenylephrine, with pure alpha-1 activity, raises the SVR and the blood pressure but produces a reflex bradycardia and no direct cardiac stimulation. The clinical flashpoint is obstetric spinal hypotension: ephedrine was the historical first-line but phenylephrine is now preferred because it gives a higher umbilical artery pH (ephedrine crosses the placenta and causes fetal beta stimulation and metabolic acidosis). Ephedrine retains a role where the hypotension is accompanied by a bradycardia that phenylephrine would worsen — the niche of "hypotension WITH bradycardia". Ephedrine also shows tachyphylaxis with repeated doses (as the noradrenaline store is depleted); phenylephrine, acting directly, does not.
- Versus noradrenaline (norepinephrine). Noradrenaline is an alpha-1, alpha-2 and weak beta-1 agonist (the exam-critical point is the WEAK beta-1 — it is NOT a pure alpha agent). It raises the SVR (alpha-1) and supports the cardiac output (beta-1), so it is the preferred first-line vasopressor for vasodilatory shock (septic, post-cardiopulmonary-bypass) where both need correcting. Phenylephrine, lacking the beta-1, raises the SVR but does not support the cardiac output and may reduce it. Phenylephrine is therefore a reasonable choice for pure vasoplegia with a high-output state, but noradrenaline is the better choice when the cardiac output is low or marginal. Noradrenaline is also preferred for sustained, high-dose infusion because its beta-1 component offsets some of the reflex bradycardia. The Ngan Kee 2015 RCT showed that norepinephrine is comparable to phenylephrine for maintenance of maternal blood pressure during spinal anaesthesia for caesarean delivery, with less bradycardia, and is an emerging alternative in the obstetric context where phenylephrine-driven reflex bradycardia is poorly tolerated.[9]
- Versus metaraminol. Metaraminol is a predominantly alpha-1 agonist with some indirect beta-1 activity (it releases noradrenaline from nerve terminals and is itself a substrate for the storage vesicles, the so-called "false transmitter"). It is a popular first-line bolus vasopressor for anaesthesia-induced hypotension in many centres (especially Australia and the UK) because its slightly longer duration (10 to 20 minutes) and its small beta component give a smoother and slightly more sustained effect than phenylephrine. The reflex bradycardia is less pronounced with metaraminol than with phenylephrine because of its beta component. Phenylephrine is the cleaner pharmacological tool (pure alpha-1) and the better-studied drug in obstetrics.
- Versus vasopressin. Vasopressin acts on the V1 receptor, a completely different pathway from the adrenergic receptors. It produces vasoconstriction independent of the adrenergic system, which makes it useful in refractory vasoplegia (septic shock, post-CPB vasoplegic syndrome) where adrenergic receptors are down-regulated and catecholamines become less effective. Vasopressin does not produce a reflex bradycardia to the same degree and does not rely on functional alpha receptors. Phenylephrine and vasopressin are not direct substitutes; they are complementary drugs for different layers of the vasoplegic problem.
- Versus adrenaline. Adrenaline is the full-spectrum catecholamine (alpha-1, alpha-2, beta-1, beta-2 in a dose-dependent fashion). It is the agent of choice for anaphylaxis and cardiac arrest (where its beta-2 bronchodilation, alpha-1 vasoconstriction and membrane-stabilising effects are all needed) and the inotrope of choice for profound cardiogenic shock. Phenylephrine is the wrong drug for both — it cannot bronchodilate (no beta-2) and it cannot stimulate the arrested heart (no beta-1).
Special populations
- The obstetric patient. Phenylephrine is the first-line vasopressor for spinal-induced hypotension in caesarean section, preferred over ephedrine for the higher umbilical artery pH it produces (Lee 2002; Ngan Kee 2009; Singh 2020; Fitzgerald 2020).[1][6][10][11] The reflex bradycardia is usually well tolerated in this young, fit population. The norepinephrine-versus-phenylephrine RCT (Ngan Kee 2015) established norepinephrine as a comparable alternative with less bradycardia, expanding the modern obstetric vasopressor toolkit.[9]
- The elderly patient. The reflex bradycardia of phenylephrine is more clinically significant in the elderly, in whom conduction disease, baseline bradycardia and beta-blockade are common, and in whom a sudden drop in heart rate may produce dizziness, presyncope, a fall in cardiac output or a fall in cerebral perfusion. Titrate carefully and consider the beta-component agents (metaraminol, noradrenaline) where a pure alpha-1 reflex bradycardia is poorly tolerated.
- The cardiac patient. Phenylephrine is the vasopressor of choice in aortic stenosis, hypertrophic obstructive cardiomyopathy and ischaemic heart disease where tachycardia is undesirable, as discussed above. It is the wrong drug in low-output cardiogenic shock where the afterload rise worsens the failing ventricle (use an inotrope or inodilator instead). In pulmonary hypertension, the pulmonary vasoconstriction is a caution and a pure alpha-1 agent may worsen right-ventricular afterload.
- The paediatric and neonatal patient. Phenylephrine is used in paediatric anaesthesia for vasodilatory hypotension, titrated carefully by weight. In the preterm neonate the cerebral circulation is pressure-passive and both hypotension and rapid blood-pressure swings carry a risk of cerebral injury (intraventricular haemorrhage, periventricular leukomalacia), so vasopressor use demands the utmost titration and an institutional protocol.
- The patient on monoamine oxidase inhibitors (MAOIs). Because phenylephrine is metabolised by MAO, the concurrent use of an MAOI (phenelzine, tranylcypromine, linezolid, methylene blue) reduces its breakdown and potentiates and prolongs its effect. This is a classical pharmacokinetic interaction to flag — the dose should be reduced (typically to one-tenth of the usual starting dose) and the interval extended, with careful titration. Unlike the indirect amines (ephedrine, amphetamine, tyramine), phenylephrine does NOT trigger the "cheese reaction" hypertensive crisis with MAOIs, because it does not release noradrenaline from nerve terminals — it is a directly acting agent, so the MAOI-enlarged noradrenaline store is irrelevant. (The local anaesthetic preparation of choice in the MAOI-treated patient is a plain agent without adrenaline; if a vasopressor is needed, a carefully titrated direct agent like phenylephrine is preferred over ephedrine.)
Adverse effects and safety — derive each effect from the pharmacology
The adverse-effect profile of phenylephrine is the predictable consequence of its pure alpha-1 mechanism, and the exam candidate should be able to derive each effect from the pharmacology rather than memorise it. [1]
The principal haemodynamic adverse effect is reflex bradycardia, which can be severe and can produce a symptomatic drop in heart rate, particularly in the elderly, the beta-blocked patient and the patient with baseline bradycardia or conduction disease. The reflex is vagally mediated and can be treated with an anticholinergic (glycopyrrolate 0.2 to 0.4 mg or atropine 0.5 to 0.6 mg) if symptomatic, but the cleaner solution is titration. The cardiac output may fall, both from the bradycardia and from the increased afterload, which is why phenylephrine is the wrong drug for low-output states (cardiogenic shock, hypovolaemic shock) where the afterload rise worsens the failing or underfilled ventricle. [1]
The principal local adverse effect is tissue necrosis on extravasation, shared with all the concentrated alpha-agonists. Phenylephrine is a potent vasoconstrictor and extravasation into the perivascular tissue produces intense local ischaemia and necrosis. A secure, free-flowing intravenous line is essential, and central venous access is preferred for a sustained high-dose infusion. The antidote for extravasation is phentolamine — a non-selective alpha-blocker, 5 to 10 mg in 10 mL saline, infiltrated subcutaneously around the extravasation site, which competitively blocks the alpha-1-mediated vasoconstriction and restores tissue perfusion. Early recognition and treatment are critical. [1]
At high doses, phenylephrine reduces perfusion of the renal, splanchnic and peripheral vascular beds, because the alpha-1 vasoconstriction is non-selective across the regional circulations. This is the basis of the caution against pushing alpha-agonists to very high doses in shock, where the price of the blood pressure may be covert splanchnic and renal ischaemia. Phenylephrine also produces pulmonary vasoconstriction, raising the pulmonary vascular resistance, which is a caution in pulmonary hypertension and right-ventricular failure where an increase in afterload on the right ventricle is poorly tolerated. [1]
In the rare context of an allergic vasoplectic reaction (anaphylaxis, the Kounis syndrome), phenylephrine may help the vasoplegia but adrenaline remains the first-line anaphylaxis drug because it addresses the bronchoconstriction and the angioedema that a pure alpha-1 agent cannot. [1]
Practical administration
In practice phenylephrine is most often given as a titrated intravenous bolus or a continuous infusion. For the acute, transient blood-pressure drop a bolus of 50 to 100 micrograms (up to 200 micrograms) is drawn up and given in increments, with the effect assessed within a minute. For sustained hypotension — the ongoing vasoplegia of spinal anaesthesia, a long septic or post-CPB course — an infusion of 0.5 to 5 micrograms per kg per minute is prepared and titrated to the mean arterial pressure target. A secure, free-flowing intravenous line is essential because of the extravasation-necrosis risk; for a sustained high-dose infusion, central venous access is preferred. [1]
The haemodynamic monitoring should be proportionate to the dosing. For a single bolus in a monitored patient a non-invasive blood pressure and a continuous electrocardiogram (for the reflex bradycardia) are sufficient. For a sustained infusion, especially in the haemodynamically fragile or vasoplectic patient, an arterial line allows beat-to-beat titration. In the obstetric spinal context, the proactive infusion started immediately after the spinal, titrated to a baseline systolic target and supplemented by boluses for breakthrough dips, is now the standard of care (Ngan Kee 2004; Ngan Kee 2013 closed-loop).[3][7]
Common traps
The wrong-vasopressor mistakes
BRADY
Phenylephrine in a bradycardic, hypotensive patient worsens the bradycardia — use ephedrine or address the rate first
The bradycardia is REFLEX (baroreceptor-vagal), NOT direct — so it does NOT respond to beta-agonists, only to slowing the infusion or an anticholinergic
Phenylephrine in low-output cardiogenic shock raises the afterload against which the failing ventricle must pump and worsens the CO
The 10 per cent ophthalmic preparation carries significant systemic absorption — never use it in the elderly, pregnant or cardiovascularly compromised
The single highest-yield exam fact: phenylephrine is first-line for obstetric spinal hypotension because it gives a HIGHER umbilical artery pH than ephedrine
SAQ answer scaffold
A model answer to "Describe the pharmacology of phenylephrine and outline its clinical indications, with specific reference to its use in obstetric spinal-induced hypotension" is structured in six moves: [1]
- Structure and receptor pharmacology. Synthetic phenylethylamine, non-catecholamine (no 3,4-dihydroxyl ring → not a COMT substrate → orally active, longer duration than catecholamines), metabolised by MAO. Pure alpha-1 agonist with no beta-1, beta-2 or alpha-2 activity at clinical doses — the cleanest example in clinical use.
- Mechanism and second messenger. Alpha-1 is Gq-coupled: PLC cleaves PIP2 into IP3 and DAG; IP3 releases calcium from the SR; calcium binds calmodulin, activates myosin light-chain kinase, phosphorylates myosin light chain → vascular smooth-muscle contraction → arteriolar and venous vasoconstriction.
- Haemodynamic signature. SVR rises, BP rises, heart rate falls (baroreceptor-vagal reflex; no direct beta-1 to offset it), CO falls or unchanged (reflex bradycardia plus increased afterload). Pulmonary vascular resistance may rise; renal and splanchnic perfusion may fall at high doses.
- Pharmacokinetics and dosing. Onset under 1 minute; duration 15 to 20 minutes; half-life about 5 minutes (MAO metabolism → MAOI interaction potentiates effect). IV bolus 50 to 100 micrograms (up to 200 micrograms); infusion 0.5 to 5 micrograms per kg per minute. Orally active as a decongestant; topical nasal, ophthalmic and (classical) IV routes for SVT.
- Indications. (i) FIRST-LINE for obstetric spinal-induced hypotension — Lee 2002 Cochrane, higher umbilical artery pH than ephedrine (ephedrine crosses placenta → fetal beta stimulation → metabolic acidosis; phenylephrine does not). (ii) Vasodilatory hypotension of any cause (spinal, post-induction, post-CPB, adjunct in septic shock). (iii) Where tachycardia is undesirable — aortic stenosis, HOCM, ischaemic heart disease, regurgitant valves. (iv) Non-vasopressor: nasal decongestant, mydriatic, classical SVT termination.
- Adverse effects. Reflex bradycardia (treat by titration or anticholinergic), fall in CO (wrong drug in cardiogenic/hypovolaemic shock), tissue necrosis on extravasation (antidote: phentolamine), renal/splanchnic/pulmonary vasoconstriction at high doses, MAOI potentiation (reduce dose). No tachyphylaxis (direct action). [1]
Viva stem bank
- "Draw the haemodynamic effects of phenylephrine on a graph of heart rate, blood pressure, systemic vascular resistance and cardiac output against time after a 100-microgram IV bolus." (Test: the rise in SVR and BP, the immediate fall in HR via the baroreceptor reflex, the unchanged-or-falling CO.)
- "Compare phenylephrine and ephedrine for the treatment of spinal-induced hypotension in a parturient undergoing caesarean section." (Test: pure alpha-1 vs mixed alpha+beta; reflex bradycardia vs tachycardia; no placental transfer vs placental transfer; higher vs lower umbilical artery pH; no tachyphylaxis vs tachyphylaxis; Lee 2002 Cochrane evidence.)
- "Why is phenylephrine preferred in aortic stenosis / HOCM / ischaemic heart disease?" (Test: the heart rate should not rise — diastolic filling, myocardial oxygen demand; in HOCM specifically the afterload and preload rise and the reflex bradycardia all reduce the dynamic LVOT obstruction.)
- "What is the mechanism of the MAOI interaction with phenylephrine, and how does it differ from the MAOI interaction with ephedrine?" (Test: pharmacokinetic potentiation of phenylephrine by MAO inhibition — reduce dose; but phenylephrine does NOT trigger the "cheese reaction" hypertensive crisis because it does not release noradrenaline from nerve terminals, unlike ephedrine.)
- "Describe the cellular mechanism of the alpha-1 receptor." (Test: Gq-coupled, PLC, PIP2 to IP3 and DAG, IP3-receptor-mediated SR calcium release, calmodulin, myosin light-chain kinase, myosin light-chain phosphorylation, smooth-muscle contraction.)
- "A patient on a phenylephrine infusion through a peripheral cannula develops blanching and coolness at the IV site. What is the complication, what is the antidote, and how would you give it?" (Test: tissue extravasation and impending necrosis; phentolamine 5 to 10 mg in 10 mL saline infiltrated subcutaneously around the extravasation site; stop the infusion, aspirate any remaining drug, elevate the limb, observe.)
- "How would you set up a prophylactic phenylephrine infusion for a healthy parturient undergoing elective caesarean section under spinal anaesthesia?" (Test: infusion started immediately after the spinal; rate 0.5 to 1.5 micrograms per kg per minute titrated to baseline systolic pressure; bolus 50 to 100 micrograms for breakthrough dips; expect and tolerate reflex bradycardia; have glycopyrrolate drawn up.) [1]
References
- [1]Lee A, Ngan Kee WD, Gin T A quantitative, systematic review of randomized controlled trials of ephedrine versus phenylephrine for the management of hypotension during spinal anesthesia for cesarean delivery Anesth Analg, 2002.PMID 11916798
- [2]Cooper DW, Carpenter M, Mowbray P, Desira WR, Ryall DM, Kokri MS Fetal and maternal effects of phenylephrine and ephedrine during spinal anesthesia for cesarean delivery Anesthesiology, 2002.PMID 12459688
- [3]Ngan Kee WD, Khaw KS, Ng FF Comparison of phenylephrine infusion regimens for maintaining maternal blood pressure during spinal anaesthesia for Caesarean section Br J Anaesth, 2004.PMID 14977792
- [4]Cooper DW, Gibb SC, Meek T, Owen S, Kokri MS, Malik AT, Koneti KK Effect of intravenous vasopressor on spread of spinal anaesthesia and fetal acid-base equilibrium Br J Anaesth, 2007.PMID 17347185
- [5]Morelli A, Ertmer C, Rehberg S, Lange M, Orecchioni A, Laderchi A, Bachetoni A, D'Alessandro M, Van Aken H, Pietropaoli P, Westphal M Phenylephrine versus norepinephrine for initial hemodynamic support of patients with septic shock: a randomized, controlled trial Crit Care, 2008.PMID 19017409
- [6]Ngan Kee WD, Khaw KS, Tan PE, Ng FF, Karmakar MK Placental transfer and fetal metabolic effects of phenylephrine and ephedrine during spinal anesthesia for cesarean delivery Anesthesiology, 2009.PMID 19672175
- [7]Ngan Kee WD, Khaw KS, Ng FF, Tam YH Randomized comparison of closed-loop feedback computer-controlled with manual-controlled infusion of phenylephrine for maintaining arterial pressure during spinal anaesthesia for caesarean delivery Br J Anaesth, 2013.PMID 23015618
- [8]Ngan Kee WD, Lee SW, Khaw KS, Ng FF Haemodynamic effects of glycopyrrolate pre-treatment before phenylephrine infusion during spinal anaesthesia for caesarean delivery Int J Obstet Anesth, 2013.PMID 23692706
- [9]Ngan Kee WD, Lee SW, Ng FF, Tan PE, Khaw KS Randomized double-blinded comparison of norepinephrine and phenylephrine for maintenance of blood pressure during spinal anesthesia for cesarean delivery Anesthesiology, 2015.PMID 25635593
- [10]Singh PM, Singh NP, Reschke M, Ngan Kee WD, Palanisamy A, Monks DT Vasopressor drugs for the prevention and treatment of hypotension during neuraxial anaesthesia for Caesarean delivery: a Bayesian network meta-analysis of fetal and maternal outcomes Br J Anaesth, 2020.PMID 31810562
- [11]Fitzgerald JP, Fedoruk KA, Jadin SM, Carvalho B, Halpern SH Prevention of hypotension after spinal anaesthesia for caesarean section: a systematic review and network meta-analysis of randomised controlled trials Anaesthesia, 2020.PMID 31531852