Anaes · Measurement & monitoring physics
MRI, laser and radiation safety
Also known as MRI safety · Laser safety · Radiation protection · ALARA principle · Airway fire · Magnet quench
The anaesthetist encounters three distinct non-pharmacological hazards in the modern operating theatre and radiology suite: the magnetic resonance imaging (MRI) environment, surgical lasers, and ionising radiation. The framework rests on six exam-critical ideas. First, an MRI scanner uses three electromagnetic fields — a powerful STATIC magnetic field (B0, typically 1.5 or 3 tesla) that aligns protons and exerts the PROJECTILE EFFECT (ferromagnetic objects become dangerous projectiles), GRADIENT magnetic fields that are switched on and off and induce nerve stimulation, and RADIOFREQUENCY pulses that heat tissue (the energy deposited measured by the specific absorption rate, SAR). Second, MRI sites are divided into four ZONES for safety: Zone I (general public), Zone II (screening of patients and staff), Zone III (controlled access, the boundary past which no unscreened ferromagnetic object may pass) and Zone IV (the scanner room itself, housing the magnet and the quench button). Third, implants are classified MR-SAFE (no magnetic or RF interaction, e.g. titanium), MR-CONDITIONAL (safe only under specific conditions of field strength and SAR) or MR-UNSAFE (ferromagnetic, never scan, e.g. some aneurysm clips and older cardiac devices); modern MRI-conditional CIEDs require a specific scanning protocol. Fourth, the SUPERCONDUCTING MAGNET is kept at about 4 kelvin by liquid helium; a QUENCH (sudden loss of superconductivity) boils off helium rapidly, displacing oxygen and causing asphyxiation and frostbite risk — the quench button vents helium outside, and staff must evacuate immediately. Fifth, LASERS (Light Amplification by Stimulated Emission of Radiation) produce coherent, collimated, monochromatic light by STIMULATED EMISSION (a photon stimulates an excited electron to drop, emitting an identical photon); common surgical lasers include CO2 (10600 nm, cutting and ablation), Nd:YAG (1064 nm, coagulation and deep penetration), KTP and argon (vascular and eye), and excimer (corneal ablation); tissue interactions are photothermal, photoablation and photochemical. Laser hazards include retinal burn from a reflected beam, skin burn, laser plume inhalation, and AIRWAY FIRE (the laser igniting the endotracheal tube in an oxygen-enriched atmosphere); prevention uses a laser-resistant ETT, saline-filled cuff, wet towels around the surgical field, the lowest compatible FiO2, and laser eye protection for all staff. Sixth, IONISING RADIATION (X-ray, CT, fluoroscopy) carries a cumulative stochastic cancer and deterministic tissue risk, unlike non-ionising radiation (laser, MRI, ultrasound); protection follows the ALARA principle (As Low As Reasonably Achievable) through three measures — TIME (minimise fluoroscopy time), DISTANCE (the inverse square law means doubling the distance from the source reduces the dose to one quarter) and SHIELDING (lead aprons at 0.5 mm lead equivalence, thyroid shields, leaded glass and gonadal shields); occupational dose is monitored with a film badge or thermoluminescent dosimeter (TLD). Built on the MRI breast-tissue-expander safety study (Damiao 2026), the CIED MRI safety review (Hameed 2026), the superconducting magnet quench hazards review (Steckner 2026), the fire risks in airway procedures review (Beaulieu 2026), the airway fire prevention in the OR study (Bhat 2026), the fire safety in CO2 laser airway surgery study (Roitman 2026), the radiation exposure during fluoroscopy study (Gaida 2026), and the bronchoscopic carcinoid removal report (Gulati 2026).
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags

Why this matters to the anaesthetist
The anaesthetist works in environments with three distinct non-pharmacological hazards beyond the drug syringe: the MRI scanner (anaesthesia for the radiology suite and interventional MRI), surgical lasers (ENT, ophthalmic, plastic and airway surgery), and ionising radiation (fluoroscopy and C-arm use in theatre). Each demands a specific safety framework — the MRI projectile effect and quench hazard, the laser airway fire, and the ALARA radiation principle. A single unrecognised ferromagnetic object, one unguarded laser pulse in an oxygen-enriched airway, or cumulative unmonitored fluoroscopy exposure can maim or kill a patient or a staff member [4][7].
MRI: static magnetic field and the projectile effect
The MRI scanner generates a powerful static magnetic field (B0), typically 1.5 or 3 tesla (T) in clinical practice — about 30 000 to 60 000 times the Earth's magnetic field. This field is always on, even when no scan is running and even during a power failure. Its clinical purpose is to align the hydrogen protons in the body along the field axis, creating the net magnetisation that the RF pulses then manipulate. [1]
The dominant hazard of the static field is the projectile effect. Ferromagnetic materials (iron, nickel, cobalt, many stainless steels) experience a strong translational force and a torque in the field. A loose object becomes a dangerous projectile accelerated toward the bore. Reported projectiles include oxygen cylinders, scissors, clamps, pens, pagers, watches, floor buffers and even defibrillators. The force rises steeply near the bore mouth (the "spatial gradient"), so an object that feels harmless a metre away can become lethal in the final approach. The only protection is rigorous ferromagnetic screening of every person and object before they cross into Zone IV. Non-ferromagnetic metals (titanium, aluminium) are not attracted and do not become projectiles [1].
MRI: gradient magnetic field and nerve stimulation
The gradient magnetic fields are switched on and off rapidly during the scan to localise the signal spatially. Because a changing magnetic field induces an electric field (Faraday's law), the switching gradients can induce currents in the body. At sufficiently high rates of change (dB/dt), these currents stimulate nerves and muscles — the patient may experience a tapping sensation or, at higher levels, painful muscle twitching (peripheral nerve stimulation). Modern scanners monitor dB/dt and limit it to stay below the stimulation threshold for the vast majority of patients. [1]
MRI: radiofrequency pulses, heating and SAR
The radiofrequency (RF) pulses tip the aligned protons into the transverse plane so they can be detected. The RF energy is absorbed by tissue and deposited as heat. The energy deposited per kilogram of tissue is the specific absorption rate (SAR), measured in watts per kilogram. The scanner estimates SAR from the pulse sequence and the patient's weight and limits it to regulatory caps (whole-body SAR typically kept below 2 to 4 W per kg depending on mode). [1]
RF heating is a particular concern in patients with metallic implants (which can concentrate current and heat locally), in large patients (more tissue to deposit energy in), and with sequences that use many high-flip-angle pulses. Monitoring under MRI is also constrained: the RF field can induce currents in monitoring cables and produce burns at skin contact points, so MRI-conditional monitors with fibre-optic or high-impedance leads are used. [1]
MRI zones I to IV
The American College of Radiology defines a four-zone model to control access and prevent ferromagnetic incidents [1][2].
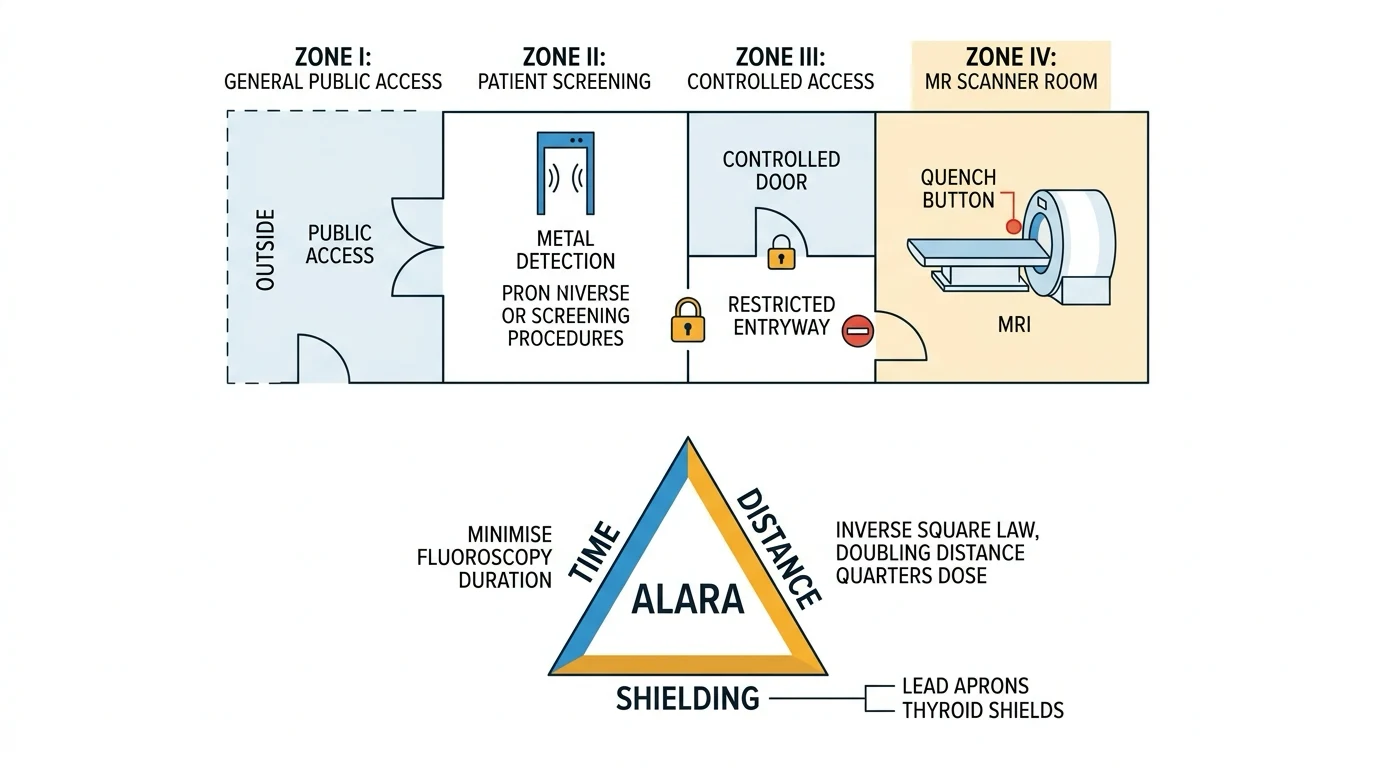
- Zone I — the area freely accessible to the general public (the street, reception, waiting room).
- Zone II — the interface where patients and staff are screened: the MR safety questionnaire, ferromagnetic detector, and removal of all metallic objects. No one passes Zone II unscreened.
- Zone III — a controlled-access area (locked doors, key-card entry) for trained MR staff. This is the boundary past which no unscreened or ferromagnetic object may pass. The console room is here.
- Zone IV — the scanner room itself, containing the magnet. Access is strictly controlled and only MR-safe or MR-conditional equipment enters. The quench button is mounted on the wall here, behind a break-glass cover. [1]
MR-safe, MR-conditional and MR-unsafe implants
Every implant and device that may enter the scanner is classified by the ASTM standard into three categories [1][2]:
- MR-SAFE — the item poses no hazard in any MRI environment; it is non-conducting, non-metallic and non-magnetic (e.g. a plastic cannula, a titanium clip that is verified non-ferromagnetic). Labelled with a green square.
- MR-CONDITIONAL — the item has been demonstrated to pose no hazard only under specific conditions of static field strength, SAR, dB/dt and orientation. The conditions (e.g. safe up to 3 T, SAR up to 2 W per kg) must be checked against the specific scanner before scanning. Many modern cardiac implantable electronic devices (CIEDs) fall here, requiring a documented scanning protocol with device interrogation before and after [2].
- MR-UNSAFE — the item is ferromagnetic or has significant RF interaction and poses a clear hazard; it must never enter the scanner room. Labelled with a red triangle with a diagonal bar. Examples include some older aneurysm clips, ferromagnetic intraocular foreign bodies, and older non-conditional pacemakers.
The anaesthetist must verify the implant status before bringing any patient or any piece of anaesthetic equipment into Zone IV. [1]
Superconducting magnet quench
The static field is generated by a large electromagnet whose windings are superconducting — they carry current with zero resistance when cooled below their critical temperature. The coolant is liquid helium at about 4 kelvin (-269 degrees Celsius). A quench is a sudden, uncontrolled loss of superconductivity: the windings develop resistance, dump their stored energy as heat, and the liquid helium boils off as a gas in seconds [3].
The hazards of a quench are: [1]
- oxygen displacement and asphyxiation — liquid helium expands about 750-fold as it vaporises; a full quench can displace the oxygen in the scanner room, causing rapid hypoxia and asphyxiation of anyone inside;
- frostbite — the escaping gas is extremely cold;
- loss of the static field — the scanner is taken offline until refilled and recommissioned. [1]
The quench button is a deliberate emergency control mounted in Zone IV (behind break-glass). Pressing it triggers a controlled quench that vents the helium through a pipe to the building exterior. It is used only when a person or ferromagnetic object is trapped against the magnet and cannot be freed by any other means, because a quench itself is hazardous and takes the scanner out of service. Staff must evacuate Zone IV immediately and not re-enter until the all-clear is given [3].
Acoustic noise
The rapidly switching gradient coils flex within the static field (the Lorentz force), producing loud acoustic noise — typically 100 to 115 decibels in a 1.5 T scanner and louder at 3 T. The noise is a hazard to the patient (hearing damage, anxiety) and to staff. Hearing protection is mandatory for everyone in Zone IV during a scan. [1]
Laser physics: stimulated emission
A laser (Light Amplification by Stimulated Emission of Radiation) produces light by a quantum process. Electrons in the lasing medium are pumped into an excited energy state (by an electrical discharge, a flashlamp or another laser). A passing photon of exactly the right energy stimulates an excited electron to drop to its lower state, emitting a second photon that is identical to the first — the same wavelength, the same phase, and travelling in the same direction. This is stimulated emission, and the optical cavity (two mirrors, one partially silvered) amplifies the beam by reflecting it back and forth through the medium. [1]
The resulting laser light has three defining properties [6]:
- monochromatic — all photons have exactly the same wavelength (colour);
- coherent — all photons are in phase (the crests and troughs align);
- collimated — the beam is parallel and barely diverges, so it can deliver very high energy density to a small spot. [1]
Common surgical lasers and tissue interaction
The wavelength determines how deeply the laser penetrates tissue and how it is absorbed [6][8]:
| Laser | Wavelength | Tissue effect | Typical use |
|---|---|---|---|
| CO2 | 10600 nm (far infrared) | Strongly absorbed by water — vaporises surface tissue, shallow penetration | Cutting and ablation of soft tissue, vocal-cord lesions |
| Nd:YAG | 1064 nm (near infrared) | Deep penetration, scatter, coagulation | Coagulation of tumours, deep lesions, bronchial lesions |
| KTP / argon | 532 / 488-514 nm (visible) | Absorbed by haemoglobin and pigment | Vascular lesions, retinal and ophthalmic surgery |
| Excimer (ArF) | 193 nm (ultraviolet) | Breaks molecular bonds without heating (photoablation) | Corneal reshaping (LASIK, PRK) |
The tissue interaction falls into three mechanisms: photothermal (the light heats and destroys tissue — CO2, Nd:YAG, KTP), photoablation (high-energy UV photons break molecular bonds without thermal damage — excimer), and photochemical (a photosensitising drug is activated by the light to produce reactive species — photodynamic therapy) [6].
Laser hazards: eye, skin, plume and airway fire
The concentrated energy of a laser beam creates several hazards [4][5][6]:
- eye damage — a reflected beam (even off a surgical instrument) can cause a retinal burn and permanent vision loss. Visible and near-infrared lasers (KTP, Nd:YAG) reach the retina; CO2 is absorbed by the cornea and lens. Wavelength-specific laser eye protection is mandatory for all staff and the patient.
- skin burn — direct or reflected beam contact burns skin.
- laser plume inhalation — the vaporised tissue smoke contains viable cellular material, carcinogens and viruses; it should be evacuated at the source.
- airway fire — the most feared anaesthetic hazard. During laser airway surgery (e.g. on the vocal cords), the laser beam can ignite a standard polyvinyl chloride (PVC) ETT in an oxygen-enriched atmosphere, producing a blowtorch-type fire in the airway that is frequently fatal [4][6].
Airway fire prevention requires removing one or more legs of the fire triangle (ignition source + oxidiser + fuel) [5][6]:
- use a laser-resistant ETT (e.g. silicone wrapped in metallic foil, or a specifically manufactured laser tube) instead of standard PVC;
- fill the ETT cuff with saline (often with methylene blue so cuff rupture is immediately visible) rather than air, and keep the cuff down away from the laser field;
- use the lowest FiO2 compatible with the patient (aim for air-entrained or low-flow techniques, FiO2 ideally 0.21 to 0.30, avoiding nitrous oxide which is also an oxidiser);
- place wet towels around the surgical field to protect adjacent tissue and drapes;
- ensure all staff wear wavelength-specific laser eye protection and that a bowl of saline for fire dousing is immediately available. [1]
Radiation safety: ALARA — time, distance, shielding
Ionising radiation (X-ray, CT, fluoroscopy) carries enough photon energy to ionise atoms and break DNA bonds, producing both stochastic (cancer, with no threshold — probability increases with dose) and deterministic (skin erythema, cataract, hair loss, with a threshold) effects. It is distinct from non-ionising radiation (laser, MRI, ultrasound), which lacks the energy to ionise and acts by heating or magnetic effects. [1]
Protection from ionising radiation follows the ALARA principle — As Low As Reasonably Achievable — through three complementary measures [7]:
- TIME — minimise the total fluoroscopy time. Use pulse-mode rather than continuous fluoroscopy, keep the beam on only when imaging is needed, and use the "last image hold" function. Time is the only factor the operator fully controls.
- DISTANCE — the inverse square law governs the dose: the dose rate is proportional to one divided by the distance squared, so doubling the distance from the source quarters the dose (one over two squared equals one quarter). Stepping back from the C-arm is the single most effective protection; never stand at the tube side of a C-arm.
- SHIELDING — interpose radiation-absorbing material between the source and the staff. Lead aprons (at least 0.5 mm lead equivalence), thyroid shields, leaded glass screens (for the anaesthetist at the head of the table), gonadal shields for the patient when possible, and lead gloves and glasses for operators near the beam. The patient is collimated to the smallest field that shows the target. [1]
Occupational dosimetry is mandatory for staff who work regularly with fluoroscopy. A film badge or thermoluminescent dosimeter (TLD) worn under the lead apron at the chest or waist records cumulative whole-body dose; a second badge outside the apron or at the collar estimates thyroid and eye dose. The annual occupational dose limit is typically 20 millisieverts averaged over five years, with no single year above 50 mSv [7].
For C-arm fluoroscopy in theatre, the anaesthetist should stand as far from the tube as possible (the scattered radiation comes from the patient, not the tube, but is highest on the tube side), behind a leaded glass screen or wearing a lead apron, and minimise the time the beam is on [7].
Clinical
- Standard approach
- Evidence-based
Alternative
- Modified technique
- Risk-benefit
Red flags
[1]References
- [1]Damiao SQ, et al. Multimodality imaging of breast tissue expanders: Types, MRI Safety and Complications Br J Radiol, 2026.PMID 42114114
- [2]Hameed S, et al. Weight-Guided Constraints for Body Model and Lead Selection in Pediatric CIED MRI Safety Simulations ArXiv, 2026.PMID 42244814
- [3]Steckner M, et al. Hazards associated with superconducting magnet quench events: system requirements, application and consequences MAGMA, 2026.PMID 42287587
- [4]Beaulieu F, et al. Fire Risks in Airway Procedures: A Clinical Review of Proactive Prevention and Emergency Response Anesthesiol Clin, 2026.PMID 41781101
- [5]Bhat S, et al. Airway Fire Prevention and Management in the Operating Room: A Mixed Methods Study on the Effectiveness of an Interprofessional Simulation-based Training Module Ann Afr Med, 2026.PMID 41728674
- [6]Roitman A, et al. Revisiting Fire Safety Guidelines in CO(2) Laser Airway Surgery Laryngoscope, 2026.PMID 40851315
- [7]Gaida JL, et al. Radiation exposure to equine surgeons during simulated digital radiography and fluoroscopy-guided fracture fixation of the distal limb Vet Surg, 2026.PMID 42359489
- [8]Gulati NB, et al. Bronchoscopic removal of bronchial carcinoid tumors: Case series and literature review J Anaesthesiol Clin Pharmacol, 2026.PMID 42088181