Anaes · Applied cardiovascular & respiratory physiology
Autonomic nervous system
Also known as Sympathetic nervous system · Parasympathetic nervous system · Adrenergic receptors · Cholinergic receptors · Alpha beta receptors · Muscarinic nicotinic
The autonomic nervous system governs the involuntary organs and is the framework for almost every anaesthetic drug and reflex. The framework rests on five exam-critical ideas: the sympathetic outflow is thoracolumbar with short preganglionic and long postganglionic fibres and ganglia near the spine, while the parasympathetic outflow is craniosacral with long preganglionic and short postganglionic fibres and ganglia near or in the target organ; acetylcholine is the neurotransmitter at ALL autonomic ganglia and at the parasympathetic postganglionic synapse, while noradrenaline is the postganglionic sympathetic neurotransmitter (except the sweat glands, which are cholinergic); the adrenal medulla is a modified sympathetic ganglion that releases adrenaline into the blood; the adrenergic receptors (alpha-1 vasoconstrict, alpha-2 presynaptic-inhibit, beta-1 cardiac, beta-2 bronchodilator and vasodilator, beta-3 lipolysis and bladder) and the cholinergic receptors (nicotinic at ganglia and the neuromuscular junction, muscarinic at postganglionic parasympathetic targets) are G-protein-coupled with predictable second messengers and effects; and almost every anaesthetic intervention is an autonomic one — vasopressors, bronchodilators, anticholinergics, beta-blockers, neostigmine — and autonomic failure (diabetes, ageing) destabilises the perioperative patient. Built on the beta-2 adrenergic receptor cardiac study (Sanches 2026), the neurocardiac-autonomic TBI review (Gumbo 2026), the formoterol beta-2 study (Abourayya 2026), the sympathetic and parasympathetic ganglion-block study (Tyagi 2026), the geriatric anaesthesia study (Prado Fonseca 2026), and the Ehlers-Danlos anaesthesia study (Unterman 2026).
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags
Why this matters to the anaesthetist
Almost every anaesthetic drug and reflex is autonomic: vasopressors, bronchodilators, anticholinergics, beta-blockers, neostigmine, the baroreflex, the oculocardiac reflex, and the haemodynamic collapse of high spinal anaesthesia. A precise map of autonomic anatomy, transmitters, receptors and second messengers turns intraoperative pharmacology and reflex bradycardia into a predictable system rather than a list of drug names [2][5].
The Primary examination expects you to state outflow levels, preganglionic versus postganglionic fibre lengths, the neurotransmitter at every synapse, G-protein and second-messenger cascades, organ-level effects, and the classic anaesthetic reflexes — then link each to a drug class. [1]
Sympathetic versus parasympathetic architecture
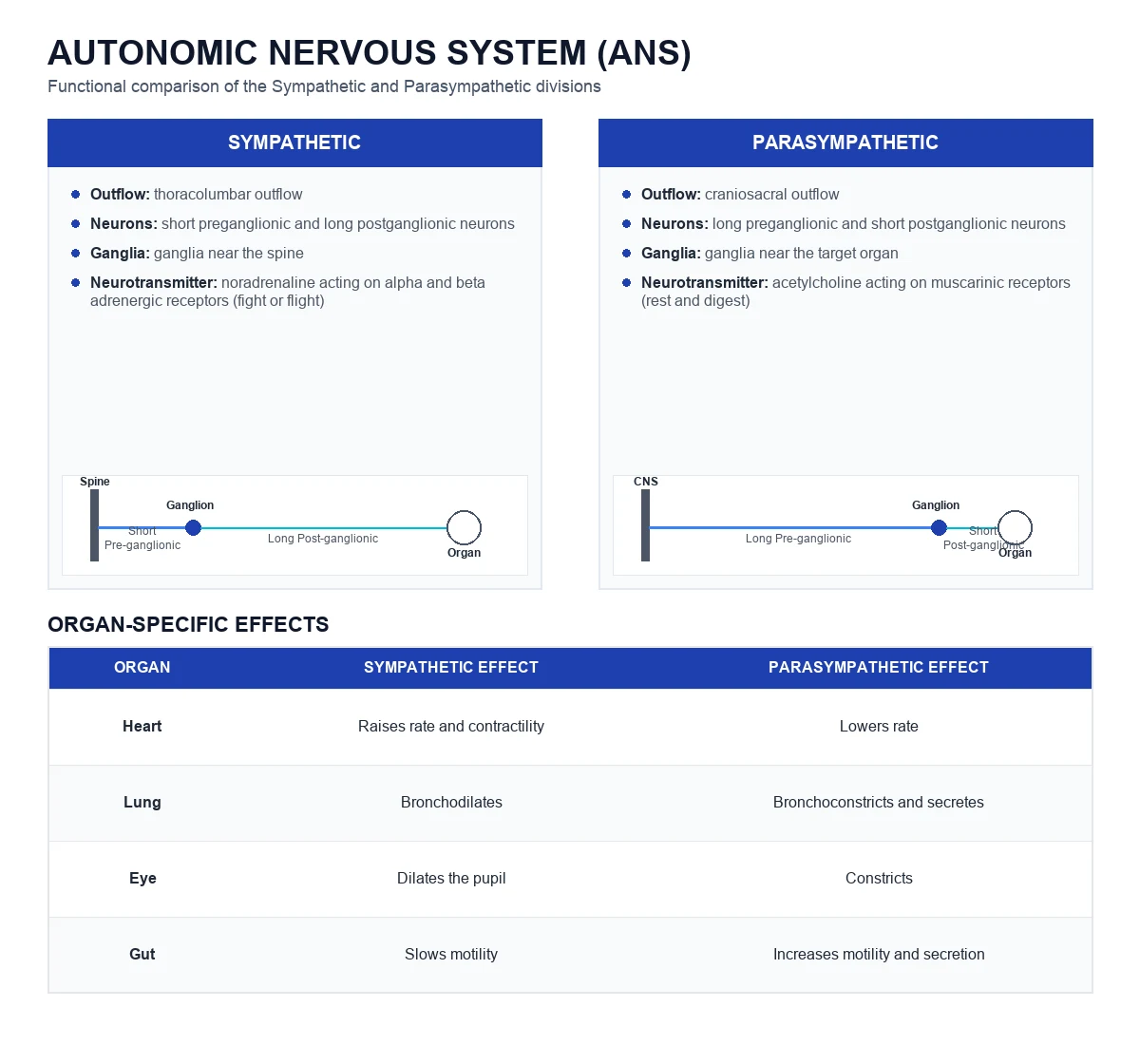
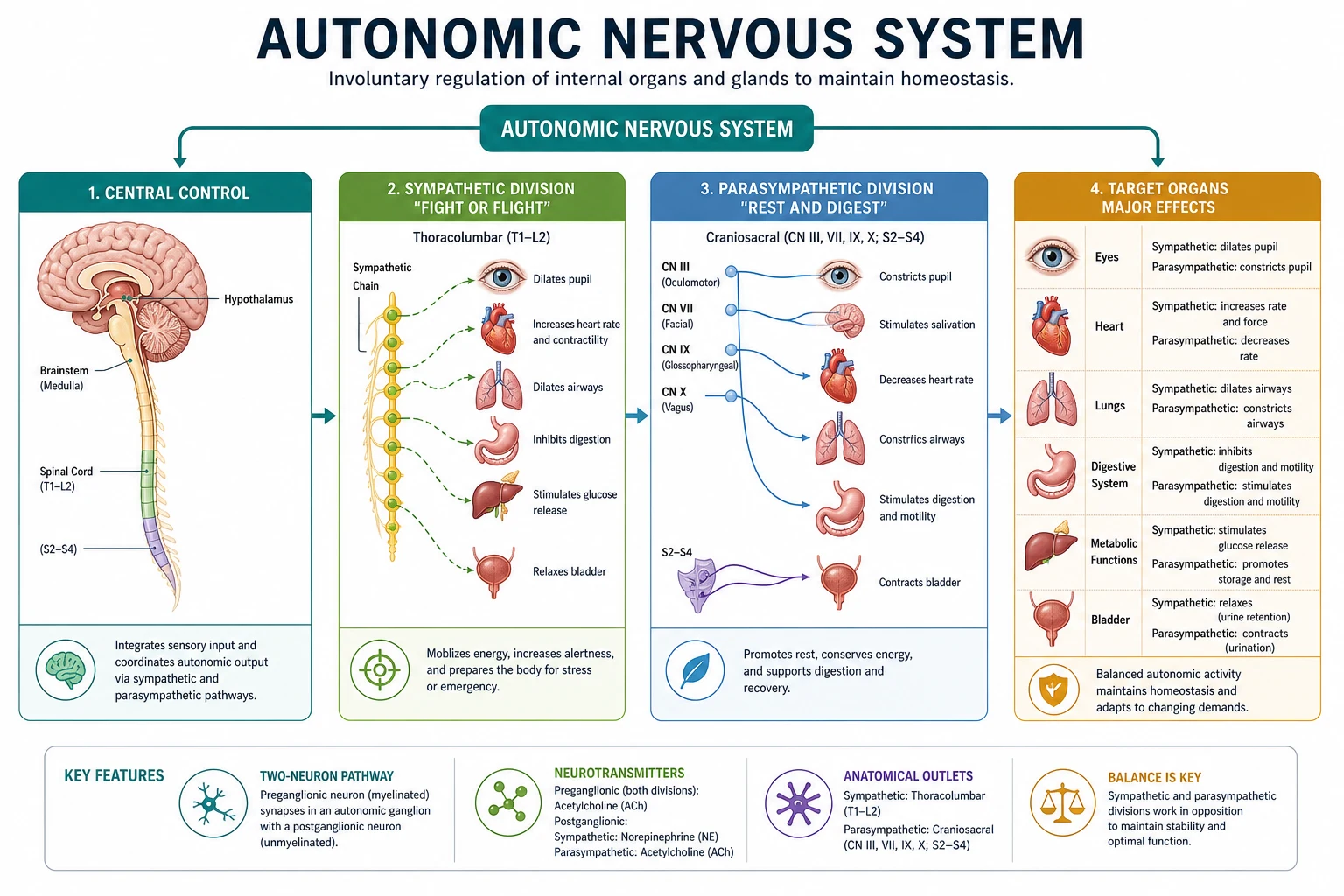
The sympathetic outflow is thoracolumbar (T1 to L2). Preganglionic cell bodies sit in the intermediolateral column of the spinal cord. Short preganglionic myelinated B fibres exit via the ventral root and white ramus, then either: (1) synapse in the paravertebral sympathetic chain at the same level; (2) ascend or descend the chain before synapsing; or (3) pass through as splanchnic nerves to prevertebral (collateral) ganglia (coeliac, superior and inferior mesenteric). Long unmyelinated postganglionic C fibres travel with somatic nerves or vessels to the target. [1]
The parasympathetic outflow is craniosacral: cranial nerves III, VII, IX and X, plus sacral segments S2 to S4. Preganglionic fibres are long; ganglia lie near or within the target organ; postganglionic fibres are short. The vagus (CN X) supplies thoracic and abdominal viscera as far as the mid-transverse colon; the sacral outflow supplies the distal colon, bladder and genitalia. [1]
Exam table (must recite): [1]
| Feature | Sympathetic | Parasympathetic |
|---|---|---|
| Outflow | T1–L2 | CN III, VII, IX, X; S2–S4 |
| Preganglionic fibre | Short | Long |
| Postganglionic fibre | Long | Short |
| Ganglion location | Near spine (paravertebral/prevertebral) | Near or in organ |
| Ganglionic transmitter | ACh → nicotinic | ACh → nicotinic |
| Postganglionic transmitter | Noradrenaline (except sweat = ACh) | ACh → muscarinic |
| Divergence | High (1 pre → many post) | Lower (more discrete) |
Neurotransmitters — the non-negotiable map
Acetylcholine (ACh) is the transmitter at ALL autonomic ganglia (nicotinic receptors) and at the postganglionic parasympathetic synapse (muscarinic receptors). Noradrenaline (norepinephrine) is the postganglionic sympathetic transmitter — except sweat glands, which are sympathetic but cholinergic (muscarinic). The adrenal medulla is a modified sympathetic ganglion receiving preganglionic cholinergic input and releasing catecholamines into blood. [1]
ACh is synthesised from choline and acetyl-CoA by choline acetyltransferase, packaged into vesicles by the vesicular ACh transporter, released by calcium-dependent exocytosis, and hydrolysed in milliseconds by acetylcholinesterase to acetate and choline (reuptake of choline is rate-limiting for synthesis). Noradrenaline is synthesised from tyrosine → L-DOPA (rate-limiting tyrosine hydroxylase) → dopamine → noradrenaline (dopamine β-hydroxylase in vesicles). Termination is mainly reuptake-1 (NET) into the nerve terminal, with MAO and COMT metabolism; only a minority diffuses away to be metabolised systemically. [1]
The adrenal medulla
The adrenal medulla is a modified sympathetic ganglion without postganglionic axons: preganglionic cholinergic fibres synapse on chromaffin cells, which release about 80% adrenaline and 20% noradrenaline into the circulation. Circulating adrenaline preferentially activates β2 receptors at low concentrations (vasodilatation in skeletal muscle beds, bronchodilatation, metabolic effects) and α1 at higher concentrations (vasoconstriction). This is the hormonal arm of the fight-or-flight response and explains why endogenous stress can raise cardiac output, glucose and bronchodilatation without a pure α-agonist picture. [1]
Cholinergic receptors
Nicotinic receptors (nAChR) are ligand-gated cation channels (pentameric). Two clinically distinct subtypes: [1]
- Ganglionic (Nn, α3β4-dominant) — all autonomic ganglia; blocked by hexamethonium (historical), partially by high-dose nicotine.
- Muscle-type (Nm, α1β1δε adult) — neuromuscular junction; blocked by non-depolarising relaxants and depolarised by suxamethonium. [1]
Muscarinic receptors (mAChR) are G-protein-coupled (M1–M5): [1]
| Receptor | G-protein | Main sites | Effect |
|---|---|---|---|
| M1 | Gq → PLC → IP3/DAG → Ca2+ | CNS, ganglia | Cognition, modulation |
| M2 | Gi → ↓cAMP, ↑K+ | Heart (SA/AV, atria) | Bradycardia, ↓AV conduction |
| M3 | Gq | Smooth muscle, glands, endothelium | Bronchoconstriction, secretion, NO-mediated vasodilatation |
| M4/M5 | Gi / Gq | CNS | Less anaesthetic focus |
Atropine and glycopyrrolate are competitive muscarinic antagonists. Atropine crosses the blood–brain barrier (central anticholinergic effects, delirium); glycopyrrolate does not (peripheral only, preferred with neostigmine for reversal). [1]
Adrenergic receptors — G-proteins and second messengers
Adrenergic receptors are G-protein-coupled with predictable cascades that examiners love: [1]
| Receptor | G-protein | Second messenger | Dominant effects |
|---|---|---|---|
| α1 | Gq | ↑IP3/DAG → ↑Ca2+ | Vasoconstriction, mydriasis, uterine contraction, sphincters |
| α2 | Gi | ↓cAMP; also K+ channels | Presynaptic inhibition of NA release; central sedation/analgesia; ↓sympathetic outflow; platelet aggregation |
| β1 | Gs | ↑cAMP → PKA | ↑HR, ↑contractility, ↑AV conduction, renin release |
| β2 | Gs | ↑cAMP | Bronchodilatation, vasodilatation (skeletal muscle), glycogenolysis, uterine relaxation, tremor |
| β3 | Gs | ↑cAMP | Lipolysis, bladder detrusor relaxation |
Viva trap: α2 receptors are presynaptic autoreceptors on sympathetic terminals and postsynaptic in the CNS (locus coeruleus, spinal cord). Clonidine and dexmedetomidine are α2 agonists: they reduce central sympathetic outflow → sedation, analgesia, bradycardia, and reduced anaesthetic requirement. Dexmedetomidine is highly α2-selective; abrupt withdrawal of chronic clonidine can cause rebound hypertension. [1]
Viva trap: Non-selective β-blockers (propranolol) block β1 and β2 — risk of bronchoconstriction in asthma and loss of β2-mediated vasodilatation. Cardioselective agents (atenolol, bisoprolol, metoprolol) prefer β1 but selectivity is relative and lost at high dose [1][3].
Organ effects — the classic opposing map
- Heart: Sympathetic β1 ↑ rate, force, conduction velocity; parasympathetic M2 (vagus) ↓ rate and AV conduction (little direct ventricular effect in humans).
- Vessels: Sympathetic α1 constricts most beds; β2 dilates skeletal muscle beds; parasympathetic causes local vasodilatation mainly via endothelial NO (M3) in some beds (e.g. erectile tissue, salivary glands) — not a general systemic vasodilator system.
- Airway: Sympathetic β2 bronchodilates; parasympathetic M3 bronchoconstricts and increases secretions.
- Eye: Sympathetic → dilator pupillae (mydriasis) and ciliary for far vision; parasympathetic → sphincter pupillae (miosis) and accommodation.
- GI tract: Sympathetic slows motility and secretion, constricts sphincters; parasympathetic increases motility and secretion.
- Bladder: Sympathetic relaxes detrusor (β3) and contracts internal sphincter (α1); parasympathetic contracts detrusor (M3) for voiding.
- Metabolic: Adrenaline via β2/β3 raises glucose and free fatty acids; α2 can inhibit insulin release. [1]
Autonomic reflexes the examiner expects
Baroreceptor reflex. High-pressure receptors in the carotid sinus (CN IX) and aortic arch (CN X) fire with stretch. Afferents reach the nucleus tractus solitarius (NTS). A rise in MAP → ↑ afferent fire → ↑ parasympathetic (vagal) and ↓ sympathetic outflow → ↓HR and vasodilatation. A fall in MAP does the reverse. Anaesthesia, volatiles, and many antihypertensives blunt the baroreflex; the elderly diabetic is the classic blunted case [5].
Oculocardiac reflex. Afferent: trigeminal (V) from orbital contents; efferent: vagus (X) → bradycardia, asystole, or junctional rhythm on eye traction (strabismus, orbital trauma). Prevention: gentle surgical technique, adequate depth, prophylactic anticholinergic in high-risk children; treatment: stop stimulus, atropine/glycopyrrolate if persists. [1]
Bezold–Jarisch reflex. Cardiac sensory receptors (inferoposterior LV wall) → profound bradycardia, hypotension and apnoea when activated (empty hypercontractile ventricle, inferior MI, some neuraxial settings). Mechanism is vagal and sympathetic withdrawal — not pure hypovolaemia alone. [1]
Cushing reflex. Raised ICP → ischaemic brainstem → massive sympathetic surge (hypertension) then baroreflex bradycardia and irregular respiration. Indicates decompensating intracranial hypertension. [1]
Diving reflex. Facial cold water → apnoea, bradycardia, peripheral vasoconstriction (trigeminal–vagal). [1]
High spinal / total spinal. Sympathectomy to high thoracic levels → vasodilatation, bradycardia (block of cardiac accelerator fibres T1–T4), and if cervical → respiratory arrest. Treatment is airway, oxygen, fluids, vasopressors (adrenaline if profound), atropine for bradycardia. [1]
Autonomic dysfunction perioperatively
Autonomic failure occurs in long-standing diabetes, ageing, Parkinson disease, pure autonomic failure, Guillain–Barré (dysautonomia), and with multi-drug antihypertensives. Consequences: postural hypotension, induction hypotension, labile HR without compensatory tachycardia, gastroparesis (aspiration risk), and blunted response to hypovolaemia. Preoperative clues: orthostatic BP fall, resting tachycardia (early cardiac autonomic neuropathy) or fixed HR, and inability to mount a fever/sweating response. Management: careful titration, reduced induction doses, ready vasopressors, avoid abrupt posture change, treat as full stomach if gastroparesis suspected [5][6].
Anaesthetic drugs as autonomic tools
- Phenylephrine: pure α1 agonist → vasoconstriction, reflex bradycardia.
- Noradrenaline: α1 + β1 (some β2) → pressor of choice in many vasodilated states.
- Adrenaline: α1 + β1 + β2 → resuscitation, anaphylaxis, low-dose inotropy/bronchodilatation.
- Ephedrine: mixed direct and indirect (releases NA) → HR and BP rise; tachyphylaxis with depleted stores.
- Metaraminol: mainly α1 with some indirect effect.
- β2 agonists (salbutamol, formoterol): bronchodilatation; tremor, hypokalaemia, tachycardia [1][3].
- β-blockers: rate and BP control; avoid non-selective agents in reactive airways.
- Anticholinergics: atropine/glycopyrrolate for bradycardia and antisialagogue effect; necessary co-administration with neostigmine.
- Neostigmine: AChE inhibitor → raises ACh at NMJ (reversal) and muscarinic sites (bradycardia, secretions, bronchospasm) — always pair with anticholinergic.
- α2 agonists (dexmedetomidine, clonidine): central sympatholysis, sedation, opioid-sparing, bradycardia/hypotension risk.
- Ganglion blocks (historical / interventional) interrupt both divisions at the synapse; modern regional techniques may target sympathetic chain for pain (e.g. stellate, lumbar sympathetic) [4].
Sympathetic emphasis
- Fight-or-flight, thoracolumbar T1–L2
- NA at most postganglionic synapses
- Adrenal medulla 80% adrenaline
- α1 constrict / β1 cardiac / β2 dilate-bronchodilate
Parasympathetic emphasis
- Rest-and-digest, craniosacral
- ACh at ganglia (Nn) and organs (M)
- Vagus dominates thoracic/abdominal control
- M2 bradycardia; M3 glands and smooth muscle
Viva traps and graph descriptions
- Draw the baroreflex loop: pressure sensor → CN IX/X → NTS → RVLM (sympathetic) and nucleus ambiguus (vagal) → effectors. Label the negative feedback.
- "What is the transmitter at the adrenal medulla synapse?" ACh on nicotinic receptors of chromaffin cells — not noradrenaline.
- "Why does neostigmine cause bradycardia?" Raised ACh at cardiac M2 receptors; always co-administer glycopyrrolate or atropine.
- "Is the sweat gland sympathetic or parasympathetic?" Anatomically sympathetic; chemically cholinergic.
- Describe α2 agonist haemodynamics: reduced central sympathetic tone → lower SVR and HR; may unmask vagal dominance; useful sedation with minimal respiratory depression compared with opioids. [1]
Second-messenger detail the Primary demands
Examiners often ask you to complete the cascade from receptor to effect: [1]
α1 (Gq): agonist → Gq-α exchanges GDP for GTP → activates phospholipase C-β → PIP2 cleaved to IP3 and DAG. IP3 opens IP3-gated Ca2+ channels on sarcoplasmic reticulum → cytosolic Ca2+ rises → calmodulin → myosin light-chain kinase in smooth muscle → contraction (vasoconstriction). DAG activates protein kinase C, modulating ion channels and sensitising the contractile apparatus. [1]
α2 (Gi): agonist → Gi-α inhibits adenylyl cyclase → cAMP falls. In presynaptic terminals this reduces voltage-gated Ca2+ channel opening and thus vesicle release of noradrenaline (negative feedback). Centrally (locus coeruleus), α2 activation hyperpolarises neurones (increased K+ conductance), reducing sympathetic outflow and producing sedation and analgesia — the mechanism of dexmedetomidine. [1]
β1/β2 (Gs): agonist → Gs-α stimulates adenylyl cyclase → cAMP rises → protein kinase A phosphorylates targets. In cardiac myocytes: phosphorylation of L-type Ca2+ channels and phospholamban accelerates Ca2+ cycling → positive inotropy and lusitropy; SA node funny current and Ca2+ currents accelerate → positive chronotropy. In bronchial smooth muscle (β2): PKA lowers cytosolic Ca2+ and promotes myosin light-chain phosphatase activity → relaxation (bronchodilatation). [1]
M2 (Gi): opposite of β1 at the heart — lower cAMP and direct βγ-mediated opening of GIRK K+ channels in atria/SA/AV node → hyperpolarisation and bradycardia/AV delay. [1]
M3 (Gq): same PLC-IP3 pathway as α1 in glands and bronchial/GI smooth muscle → secretion and constriction; on endothelium, Ca2+-calmodulin activates eNOS → NO → cGMP in smooth muscle → vasodilatation (so atropine can block some endothelial-dependent responses, and systemic muscarinic agonists can drop BP). [1]
Catecholamine synthesis, storage, release and fate
Synthesis pathway (memorise order): Tyrosine → (tyrosine hydroxylase, rate-limiting, BH4 cofactor) → L-DOPA → (DOPA decarboxylase) → dopamine → (dopamine β-hydroxylase, vesicular) → noradrenaline → (PNMT in adrenal medulla, cortisol-induced) → adrenaline. [1]
Release: action potential → N-type Ca2+ entry → SNARE-mediated exocytosis. Angiotensin II and β2 receptors can facilitate release; α2 and muscarinic M2 inhibit it. [1]
Termination: (1) Neuronal reuptake (Uptake-1, NET) — major for noradrenaline at the synapse; blocked by cocaine and tricyclic antidepressants (explains exaggerated catecholamine responses). (2) Extraneuronal uptake (Uptake-2) into tissues. (3) Metabolism by MAO (intraneuronal) and COMT (extraneuronal/liver) → VMA and metanephrines as diagnostic metabolites in phaeochromocytoma. [1]
Indirect-acting agents (ephedrine, amphetamines, tyramine) displace noradrenaline from vesicles/cytoplasm; they fail if stores are depleted (reserpine historically, chronic cocaine, denervation) — viva distinction from direct agonists. [1]
Sympathetic dermatomes and cardiac accelerators
Cardiac sympathetic afferents/efferents: T1–T4 (sometimes cited T1–T5) — the "cardiac accelerator fibres." High spinal or epidural to this level causes bradycardia not only from Bezold–Jarisch-like physiology and unopposed vagus but from direct interruption of cardiac sympathetic drive. Stellate ganglion (cervicothoracic) block can cause Horner syndrome (ptosis, miosis, anhidrosis) — a marker of successful sympathetic block to the head. [1]
Phaeochromocytoma physiology (exam link)
Tumours of chromaffin tissue secrete surges of adrenaline/noradrenaline → paroxysmal hypertension, tachycardia, arrhythmias, hyperglycaemia. Anaesthetic management rests on autonomic pharmacology: α-blockade before β-blockade (phenoxybenzamine or doxazosin first) so that unopposed α-constriction is not worsened by β2 blockade; then careful β-blockade for tachycardia. Intraoperative surges treated with phentolamine/clevidipine/SNP; post-resection hypotension from sudden catecholamine withdrawal and residual α-blockade — fluids and noradrenaline. [1]
Integrated exam table — drugs as receptor probes
| Clinical goal | Receptor strategy | Example agents |
|---|---|---|
| Raise SVR without much HR rise | α1 agonist | Phenylephrine, metaraminol |
| Raise SVR + inotropy | α1 + β1 | Noradrenaline |
| Emergency CPR / anaphylaxis | α1 + β1 + β2 | Adrenaline |
| Bronchodilatation | β2 agonist | Salbutamol |
| Rate control / reduce myocardial O2 demand | β1 antagonist | Bisoprolol, esmolol |
| Sedation + sympatholysis | Central α2 agonist | Dexmedetomidine |
| Treat bradycardia / dry secretions | Muscarinic antagonist | Atropine, glycopyrrolate |
| Reverse non-depolarising block | Raise ACh at Nm | Neostigmine (+ anticholinergic) |
Drawing tasks for the viva board
Expect to sketch: (1) two-neuron autonomic outflow with fibre lengths labelled; (2) baroreflex arc with CN IX/X and RVLM; (3) oculocardiac reflex arc (V → X); (4) receptor–G-protein–second messenger for α1 and β1. Marks are lost for swapping pre- and postganglionic lengths or for saying noradrenaline is the ganglionic transmitter. [1]
Detailed organ-by-organ autonomic map for SAQs
Iris: radial dilator (α1, sympathetic) versus sphincter (M3, parasympathetic). Mydriasis in low light and stress; miosis with opioids is central plus Edinger–Westphal tone, not a simple peripheral autonomic drug effect alone. [1]
Ciliary muscle: parasympathetic M3 contraction for near accommodation; cycloplegia with atropine-like drugs blurs near vision — warn patients after high-dose anticholinergic. [1]
Salivary and lacrimal glands: parasympathetic secretomotor (CN VII/IX pathways); sympathetic modulates composition. Anticholinergics dry the airway usefully before fibreoptics but increase mucus tenacity. [1]
Heart: SA node β1 accelerates; M2 decelerates. AV node similar. Ventricles richly β1 innervated; vagal ventricular effects modest in humans. Cardiac afferent sympathetics carry ischaemic pain (T1–T4 dermatomes). [1]
Bronchial tree: β2 dilates; M3 constricts and secretes. Non-selective β-blockade risks bronchospasm; ipratropium blocks M3 usefully in COPD. [1]
Splanchnic bed: sympathetic vasoconstriction redistributes blood in shock; neuraxial block can splanchnic-dilate and drop pressure. [1]
Uterus: α1 promotes contraction; β2 relaxes (historical tocolysis with β2 agonists). Pregnancy modifies receptor balance. [1]
Skin vessels and sweat: sympathetic noradrenergic vasoconstriction for thermoregulation; sympathetic cholinergic sweating. Blushing and emotional sweating involve complex central control. [1]
Autonomic testing (clinical)
- Orthostatic vital signs (fall in SBP ≥20 mmHg or DBP ≥10 mmHg)
- Heart-rate variability with deep breathing (parasympathetic)
- Valsalva ratio
- Sweat tests Perioperatively, a fixed heart rate and orthostatic history beat formal labs for risk flagging. [1]
Exam essay skeleton
Define ANS → compare SNS/PNS table → transmitters → receptors/G-proteins → organ effects → reflexes → drug table → autonomic failure → conclusion linking to induction hypotension and vasopressor choice. [1]
Red flags
- Acetylcholine at all ganglia and postganglionic parasympathetic synapses; noradrenaline postganglionic sympathetic except sweat glands (cholinergic).
- β1 cardiac; β2 bronchodilator/vasodilator; non-selective β-blockers can bronchoconstrict.
- α2 is presynaptic-inhibitory and central — dexmedetomidine reduces sympathetic outflow (sedation, bradycardia).
- Adrenal medulla: ~80% adrenaline, ~20% noradrenaline — hormonal arm of the SNS.
- Autonomic failure (diabetes, ageing) blunts the baroreflex — postural and induction hypotension. [1]
References
- [1]Sanches B, et al. β₂‑Adrenergic Receptor Disruption Exacerbates Cardiac Injury and Fibroblast Activation in a Female Mouse Model of Takotsubo Cardiomyopathy Am J Physiol Cell Physiol, 2026.PMID 42302406
- [2]Gumbo CT, et al. Neurocardiac consequences of traumatic brain injury: integrating neuroimmune, autonomic, and cerebrovascular mechanisms Front Immunol, 2026.PMID 42317349
- [3]Abourayya GA, et al. Formoterol induced mitochondrial biogenesis and PINK1-Parkin mitophagy via activation of β2-adrenergic receptor signaling and downregulation of miR-421/miR-103a in acute kidney injury Chem Biol Interact, 2026.PMID 42173392
- [4]Tyagi A, et al. Sympathetic and Parasympathetic Ganglion Blocks for Treatment of Long COVID-19 Symptoms: A Scoping Review Pain Physician, 2026.PMID 42263302
- [5]Prado Fonseca SJ, et al. Anesthetic Considerations in Geriatric Patients Undergoing Cataract Surgery: A Review of Perioperative Management and Outcomes Cureus, 2026.PMID 42037904
- [6]Unterman K, et al. Tourniquet Use and Anesthesiology Considerations in Patients With Hypermobile Ehlers-Danlos Syndrome: Balancing Orthopedic Needs With Anesthetic Safety Cureus, 2026.PMID 41978595