Anaes · Applied cardiovascular & respiratory physiology
Hepatic physiology & drug metabolism
Also known as Liver blood flow · Hepatic drug metabolism · Phase I Phase II metabolism · Cytochrome P450 · First-pass metabolism · Hepatic extraction ratio
The liver receives a dual blood supply and is the body's principal organ of drug metabolism and plasma protein synthesis, so its function governs the duration of almost every anaesthetic drug. The framework rests on five exam-critical ideas: the liver receives about 25 percent of the cardiac output from a dual supply — the portal vein (about 75 percent, nutrient-rich, deoxygenated) and the hepatic artery (about 25 percent, oxygen-rich) — and their contributions to oxygen are roughly equal; drug metabolism proceeds in two phases — Phase I (cytochrome P450 oxidation, reduction, hydrolysis) and Phase II (conjugation, e.g. glucuronidation and sulfation) — producing a water-soluble metabolite for biliary and renal excretion; first-pass (presystemic) metabolism by the gut wall and liver reduces the oral bioavailability of many drugs; the hepatic extraction ratio (the fraction removed in one pass) classifies drugs as high-extraction (flow-limited, e.g. propranolol, morphine) or low-extraction (capacity-limited, e.g. diazepam); and hepatic dysfunction prolongs drug action (less metabolism), reduces clotting factors and albumin (coagulopathy and altered drug binding), and causes encephalopathy. Built on the itraconazole-CYP3A4 drug-interaction study (Scudamore 2026), the hepatic drug metabolism study (Chujan 2026), the dual-vessel hepatic infarction study (Madani 2026), the hepatic transport pathway study (Chan 2026), the MARS-piperacillin liver-failure study (Monet 2026), and the lumacaftor-advanced-liver-disease study (Lim 2026).
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags

Why this matters to the anaesthetist
Primary: dual blood supply, hepatic functions list, Phase I vs II, extraction ratio and bioavailability, enzyme induction/inhibition. Final: dose adjustments in cirrhosis, volatile choice myths vs reality, coagulopathy of liver disease, and portal hypertension physiology.[1]
One-liner: Portal vein ~75% flow / low O2 + hepatic artery ~25% / high O2; clearance of high-extraction drugs is flow-limited, low-extraction is enzyme/protein-binding-limited; Phase I (CYP) then Phase II (conjugate) make drugs excretable. [1]
Dual blood supply and microanatomy
- Portal vein: ~75% of hepatic blood flow, nutrient-rich, relatively deoxygenated — from splanchnic bed.
- Hepatic artery: ~25% of flow, oxygen-rich — buffers oxygen delivery.
- Mix in sinusoids → hepatic veins → IVC.
- Acinus zones: zone 1 periportal (highest O2) to zone 3 centrilobular (lowest O2, CYP-rich, vulnerable to ischaemia and paracetamol NAPQI injury). [1]
Hepatic blood flow falls with volatile anaesthesia, surgical retraction, hypovolaemia, and α-agonists; rises with hypercapnia and some β-agonists. Portal hypertension shunts portal blood away from hepatocytes → reduced first-pass for oral drugs and variceal risk. [1]
Liver function exam list
- Synthetic: albumin, clotting factors (I, II, V, VII, IX, X, protein C/S, AT), thrombopoietin contribution.
- Metabolic: carbohydrate (glycogen, gluconeogenesis), lipid, protein (urea cycle).
- Detoxification/drug metabolism: Phase I/II, ammonia handling.
- Bile formation: bilirubin excretion, fat/vitamin absorption.
- Immunologic: Kupffer cells.
- Storage: glycogen, vitamins, iron/copper (pathology when overloaded). [1]
Drug metabolism — Phase I and Phase II
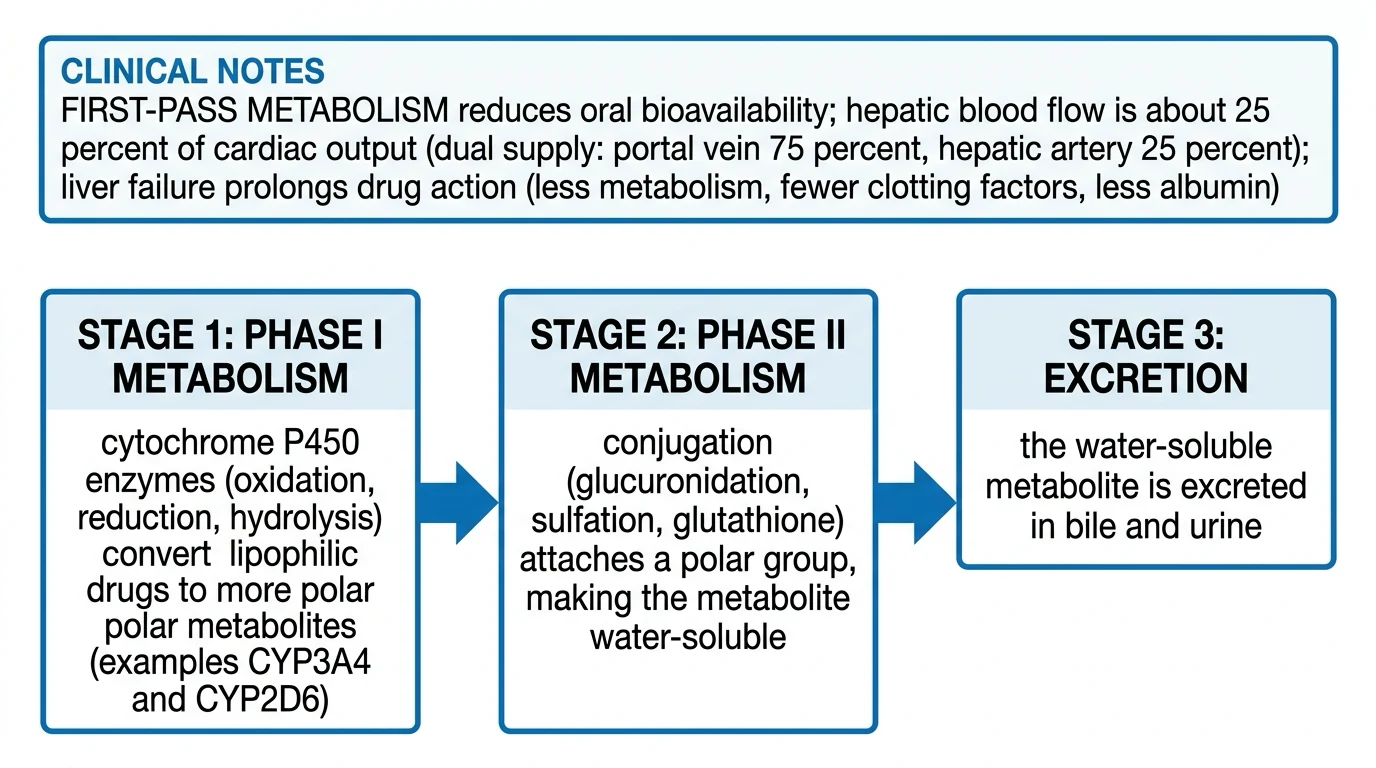
Phase I (functionalisation)
Oxidation, reduction, hydrolysis — predominantly cytochrome P450 isoforms (CYP3A4 is the workhorse for many anaesthetics/opioids/benzodiazepines; CYP2D6, 2C9, 2C19, 1A2 also high-yield for variability). May activate prodrugs or create reactive intermediates (paracetamol → NAPQI). [1]
Phase II (conjugation)
Glucuronidation (UGT), sulfation, acetylation (NAT2 — slow/fast acetylators), glutathione conjugation (detox NAPQI), methylation. Generally increases water solubility for excretion. [1]
Neonates: immature Phase I/II — prolonged drug effect (link neonatal leaf). Elderly: reduced hepatic flow and mass. [1]
Hepatic clearance, extraction ratio, bioavailability
Hepatic clearance (CL_H) conceptually depends on liver blood flow (Q), fraction unbound (fu), and intrinsic clearance (CLint): [1]
For teaching, extraction ratio E = (C_in − C_out)/C_in. [1]
| Extraction | Examples (teaching) | Rate-limited by | Anaesthetic implication |
|---|---|---|---|
| High (E > 0.7) | Propofol, lignocaine, ketamine, morphine (flow-sensitive), many first-pass drugs | Liver blood flow | Low oral bioavailability; clearance falls if Q falls (shock, β-block, volatiles) |
| Low (E < 0.3) | Rocuronium partially complex; warfarin, phenytoin, diazepam classically | Enzyme activity / binding | Sensitive to induction/inhibition and protein binding changes |
| Intermediate | Many drugs | Mixed | Context-dependent |
Oral bioavailability F reduced by incomplete absorption and first-pass hepatic/gut metabolism. High first-pass → large PO vs IV dose difference (e.g. propranolol, morphine oral vs IV). [1]
Restrictively cleared low-E drugs: only unbound drug is metabolised — hypoalbuminaemia raises free fraction transiently; steady-state free concentration often re-equilibrates via clearance (advanced viva — avoid oversimplified “low albumin always toxicity”). [1]
Biliary excretion and enterohepatic recirculation
Some conjugates are excreted in bile, deconjugated by gut flora, and reabsorbed (enterohepatic recirculation) — prolongs effect (e.g. some NSAIDs, digoxin partially, oestrogens). Cholestasis impairs elimination of biliary-dependent drugs. [1]
Enzyme induction and inhibition
| Process | Effect on victim drug | Classic inducers | Classic inhibitors |
|---|---|---|---|
| Induction | ↓ levels / effect (unless prodrug) | Rifampicin, carbamazepine, phenytoin, St John’s wort, chronic ethanol (some CYPs) | — |
| Inhibition | ↑ levels / toxicity | — | Azoles, macrolides, amiodarone, grapefruit (3A4), cimetidine, acute ethanol |
Induction takes days (protein synthesis); inhibition can be immediate. Exam favourite pairs: CYP3A4 inhibitors + midazolam/fentanyl; inducers + failure of drug effect. [1]
Hepatic dysfunction patterns
- Hepatocellular injury: high ALT/AST; synthetic failure late.
- Cholestasis: high ALP/GGT/bilirubin; pruritus; fat-soluble vitamin issues.
- Synthetic failure: high INR, low albumin — true function tests for anaesthesia risk.
- Portal HTN: ascites, varices, encephalopathy, hypersplenism (low platelets).
- PK changes: reduced CLint, reduced Q, altered binding, volume changes from ascites/oedema. [1]
Anaesthetic relevance
- Prefer drugs with organ-independent routes when possible in severe liver disease (cisatracurium Hofmann/ester; remifentanil esterases).
- Reduce dose/titrate high-extraction IV agents when cardiac output/hepatic flow low.
- Coagulopathy: factors + fibrinogen + platelets; vitamin K if deficient; viscoelastic guidance useful.
- Avoid sedatives that precipitate encephalopathy; careful opioids (morphine-6-glucuronide renal issues also).
- Paracetamol: safe at standard doses in stable chronic liver disease usually, but toxic in overdose via NAPQI when glutathione depleted (alcohol, malnutrition).
- Volatiles: modern agents undergo minimal metabolism (desflurane/sevoflurane/isoflurane low %); historical halothane hepatitis is the classic immune/metabolic teaching story. [1]
Numbers board
- Total hepatic blood flow ~1.5 L/min (~25% CO).
- Portal : arterial flow ≈ 3 : 1.
- CYP3A4 metabolises a large fraction of common drugs.
- Factor VII short half-life → INR early marker of synthetic acute change. [1]

High extraction
- Flow-limited clearance
- Large first-pass
- Shock ↓ clearance
- Titrate IV carefully
Low extraction
- Enzyme/binding-limited
- Induction/inhibition matter
- Binding changes complex
- Oral F often higher
Viva scripts
Draw dual supply and state percentages. [1]
Define extraction ratio and give one high and one low E drug with dosing implication. [1]
Phase I vs II with paracetamol as the worked toxin example. [1]
Why oral morphine dose ≫ IV dose — first-pass. [1]
Extended viva dialogue
Examiner: Propofol clearance is high — what does that mean clinically? [1]
Candidate: Clearance depends heavily on hepatic blood flow (and extrahepatic sites contribute). In low-output states clearance falls and accumulation risk rises; titration and context-sensitive half-time still matter for long infusions. [1]
Examiner: How does enzyme inhibition present? [1]
Candidate: A perpetrator drug immediately reduces metabolism of a victim drug — levels rise, sedation or toxicity appears within dosing intervals, especially for narrow therapeutic index agents. [1]
Clinical synthesis: Hepatic physiology for anaesthesia is blood flow + enzymes + synthesis. Name which of the three is broken in the patient in front of you. [1]
Well-stirred model equation (exam form)
CL_H = Q × (f_u × CL_int) / (Q + f_u × CL_int) [1]
- If f_u·CL_int ≫ Q → CL_H ≈ Q (flow-limited, high E).
- If f_u·CL_int ≪ Q → CL_H ≈ f_u·CL_int (capacity-limited, low E). [1]
This single equation unifies extraction ratio teaching. [1]
Paracetamol pathway (toxin map)
Most dose: glucuronidation/sulfation (safe). Minor CYP2E1 path → NAPQI → glutathione conjugation. Overdose: glutathione depletes → NAPQI binds hepatocytes (zone 3). NAC restores glutathione pathways. [1]
Worked SAQ
SAQ: Explain hepatic extraction ratio and give anaesthetic examples (8 marks)
Extraction ratio is the fraction of drug removed from blood in one pass through the liver. High-extraction drugs (propofol, lidocaine, ketamine teaching set) have clearance dominated by hepatic blood flow and large first-pass after oral dosing. Low-extraction drugs have clearance sensitive to enzyme activity and unbound fraction, so induction/inhibition and cirrhosis enzyme loss dominate. Shock that halves liver blood flow halves clearance of high-E drugs. [1]
Primary exam expansion — dense examiner pack
Gross hepatic functions for anaesthesia
- Drug metabolism and first-pass. 2. Synthesis: albumin, clotting factors (except VIII partly extrahepatic), thrombopoietin nuances, bile. 3. Bilirubin handling. 4. Glucose (glycogen/gluconeogenesis). 5. Lactate clearance. 6. Immune (Kupffer). 7. Hormone inactivation. [1]
Dual blood supply and extraction
Portal vein ~75% flow; hepatic artery ~25%; O2 delivery more balanced. Total hepatic blood flow ~25% CO. Hepatic arterial buffer response defends flow when portal falls. Under anaesthesia/surgery: volatiles, hypocapnia, surgical traction, pneumoperitoneum, haemorrhage reduce flow. [1]
Extraction ratio and clearance (must write)
E = (C_in − C_out)/C_in. CL_H = Q × E. Well-stirred: CL_H = Q (fu CLint)/(Q + fu CLint). [1]
| Type | E | Rate-limited by | Examples | Clinical |
|---|---|---|---|---|
| High extraction | >0.7 | Blood flow Q | Propofol, ketamine, morphine, lignocaine, metoprolol | Low CO → ↑ levels |
| Low extraction | under 0.3 | fu × CLint | Warfarin, phenytoin, diazepam, many rocuronium partial | Enzyme induction/inhibition & binding matter |
| Intermediate | 0.3–0.7 | Mixed | Midazolam | Both matter |
Phase I and Phase II metabolism
Phase I: oxidation/reduction/hydrolysis — CYP450 dominant (CYP3A4 biggest share). Phase II: conjugation (glucuronidation, sulfation, acetylation, glutathione) — usually makes more polar renally excreted metabolites. Some metabolites active (morphine-6-G) or toxic (NAPQI). [1]
Enzyme induction and inhibition
Induction (days): rifampicin, carbamazepine, phenytoin, chronic alcohol, St John’s wort → ↑CLint → treatment failure. Inhibition (hours): azoles, macrolides, cimetidine, grapefruit → ↑ victim drug levels → toxicity (midazolam, fentanyl prolonged). Competitive vs mechanism-based inhibition concepts. [1]
First-pass and bioavailability
Oral drugs with high E have low F. Cirrhosis + portosystemic shunts raise F of high-extraction oral drugs → exaggerated effects (oral morphine, midazolam). IV bypasses first-pass. [1]
Liver disease anaesthetic implications
| Problem | Consequence |
|---|---|
| Synthetic failure | Coagulopathy (not fully captured by INR alone for thrombin generation) |
| Hypoalbuminaemia | Binding/fu changes; ascites |
| Portal hypertension | Varices, encephalopathy, hyperdynamic circulation |
| Drug clearance | Prolonged sedatives; prefer short-acting (remifentanil, cisatracurium/ Hofmann) |
| Encephalopathy | Avoid deep residual sedation; ammonia/GI bleed triggers |
| Hepatorenal | Perfusion sensitive |
Child–Pugh / MELD risk stratify — state as scoring systems without inventing operative cut-offs. [1]
Paracetamol NAPQI map
Therapeutic: glucuronidation/sulfation. Overdose: CYP2E1 → NAPQI → glutathione depletes → hepatocyte necrosis. Antidote N-acetylcysteine restores glutathione pathways. Chronic alcohol/enzyme inducers increase risk teaching. [1]
Hofmann elimination / esterases contrast
Atracurium/cisatracurium: Hofmann + ester hydrolysis — organ-independent component useful in hepatic/renal disease (laudanosine historical atracurium concern high doses). Remifentanil tissue esterases. Not hepatic CYP stories — compare explicitly in viva. [1]
SAQ: hepatic extraction ratio with examples (8 marks)
Define E and CL_H (2). High vs low extraction drugs examples (3). Well-stirred limiting cases (2). One clinical CO or cirrhosis implication (1). [1]
Viva
Q: Why does shock raise propofol plasma for same infusion? A: High-E drug clearance falls when hepatic blood flow falls. Q: Why is INR high in liver failure? A: Reduced synthesis of clotting factors (VII short half-life early). Q: Does atracurium need liver? A: Predominantly organ-independent Hofmann/ester — preferred narrative in hepatic failure vs aminosteroid accumulation risk. [1]
High-yield viva battery and numbers lock-in
High versus low extraction drug lists (commit)
High E: propofol, lignocaine, morphine, ketamine, metoprolol, pethidine teaching. Low E: warfarin, phenytoin, diazepam, theophylline, many highly bound capacity-limited drugs. Intermediate: midazolam. [1]
Cirrhosis anaesthetic preference logic
Use drugs with organ-independent elimination when possible (cisatracurium, remifentanil); reduce doses of sedatives; avoid long-acting benzos; careful with opioids (encephalopathy); expect reduced plasma cholinesterase sometimes; correct coagulopathy based on clinical bleeding/viscoelastic not INR alone; manage ascites respiratory effects; prepare for variceal and haemodynamic instability. [1]
Enzyme history questions that matter
"What enzyme-inducing anticonvulsants or rifampicin? Any azole or macrolide? Chronic alcohol? St John's wort? Grapefruit?" — maps to midazolam/fentanyl/volatile minor paths and transplant drug interactions. [1]
Full viva dialogue (additional)
Examiner: Write the well-stirred model and take high-E and low-E limits. [1]
Candidate: CL_H = Q × (fu × CLint) / (Q + fu × CLint). If fu CLint is much greater than Q, CL_H approximates Q — flow-limited high extraction. If fu CLint is much less than Q, CL_H approximates fu × CLint — capacity-limited low extraction. [1]
Examiner: Why might oral bioavailability of morphine rise in cirrhosis? [1]
Candidate: Portosystemic shunting and reduced first-pass extraction allow more drug into the systemic circulation, so the same oral dose produces higher exposure and more sedation or respiratory depression. [1]
Exam traps
- Saying all drugs need dose cuts the same way in liver disease.
- Ignoring flow-limited clearance in shock.
- Assuming atracurium is heavily CYP-dependent.
- Treating INR as a full factor-by-factor map. [1]
References
- [1]Scudamore O, et al. The Effect of Multiple Doses of Itraconazole on the Pharmacokinetics of a Single Oral Dose of Zongertinib in Healthy Male Volunteers Pharmacotherapy, 2026.PMID 42324472
- [2]Chujan S, et al. Effects of 7-hydroxymitragynine on serotonin, amino acid profiles, and ion homeostasis in SH-SY5Y cells Mol Biol Rep, 2026.PMID 42334658
- [3]Madani R, et al. Case Report: Nonoperative management of traumatic dual-vessel hepatic infarction Front Surg, 2026.PMID 42305804
- [4]Chan A, et al. A Comprehensive Rat Model For Assessing Hepatic Transport Pathways Through Simultaneous Lymphatic And Blood Vascular Sampling J Vis Exp, 2026.PMID 42224152
- [5]Monet C, et al. Impact of Molecular Adsorbent Recirculating System Therapy on Piperacillin Concentration in Critically Ill Patients: An Observational Cohort Study Crit Care Med, 2026.PMID 42301229
- [6]Lim AYL, et al. Lumacaftor-Ivacaftor in Pediatric Patients With Cystic Fibrosis and Advanced Liver Disease: A Pilot Study Clin Ther, 2026.PMID 42031572