Anaes · Applied cardiovascular & respiratory physiology
Pharmacokinetics: compartment models
Also known as Pharmacokinetics · Compartment model · Volume of distribution · Clearance · Half-life · Redistribution
Pharmacokinetics describes what the body does to the drug — absorption, distribution, metabolism and excretion — and the compartment model is the mathematical framework that predicts drug concentration over time. The framework rests on five exam-critical ideas: the body is modelled as connected compartments (the central compartment of plasma and well-perfused tissues, a fast peripheral compartment of muscle, and a slow peripheral compartment of fat) between which the drug distributes and redistributes; the volume of distribution (Vd) is the apparent volume that would contain the total drug at the plasma concentration — a large Vd means the drug has left the plasma for the tissues (lipophilic drugs); clearance (CL) is the volume of plasma cleared of drug per unit time, and is the main determinant of the maintenance infusion rate; the elimination half-life (t1/2) is the time for the plasma concentration to fall by 50 percent, determined by Vd and CL (t1/2 equals 0.693 times Vd over CL); and redistribution from the peripheral compartments back to the central compartment is the mechanism by which a single IV bolus of thiopental or propofol wears off — the drug has not been metabolised, it has redistributed to muscle and fat, dropping the brain concentration below the effect threshold. Built on the Marsh-Schnider PK-PD comparison study (Ye 2026), the four-model propofol comparison study (Introna 2026), the paediatric melatonin PK study (de Barros Garioud 2026), the remimazolam PK review (Dong 2025), the LC-MS/MS propofol assay study (Ng 2026), and the body-size PK virtual trial (Marques 2026).
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags
Why this matters to the anaesthetist
Primary PK is compartments, rate constants, Vd, CL, half-lives, and multi-exponential decline. This is the language of TCI (Marsh/Schnider/Minto) and of every “why did this dose last so long?” viva.[1]
One-liner: Body modelled as V1 central + peripheral V2/V3; drug input to V1; intercompartmental rate constants k12/k21 etc.; elimination from V1 as k10; plasma curve is multi-exponential sum. [1]
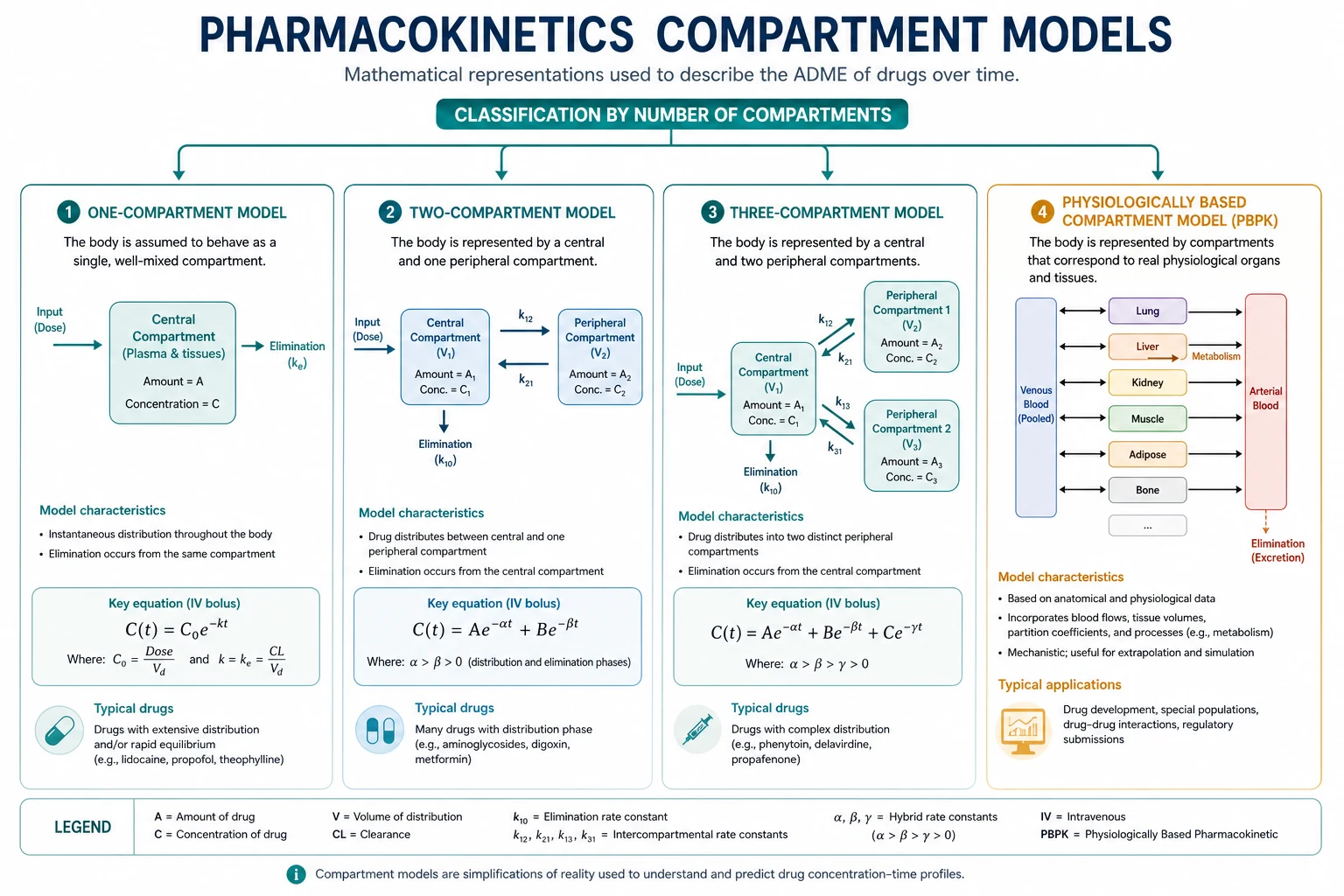
One-compartment model
- Instant mixing in single Vd; elimination first-order.
- C(t) = (Dose/V) e^(−kt); t½ = 0.693/k; CL = kV.
- Useful teaching fiction for some drugs; poor for most anaesthetics after IV bolus (distribution phases obvious). [1]
Two- and three-compartment models
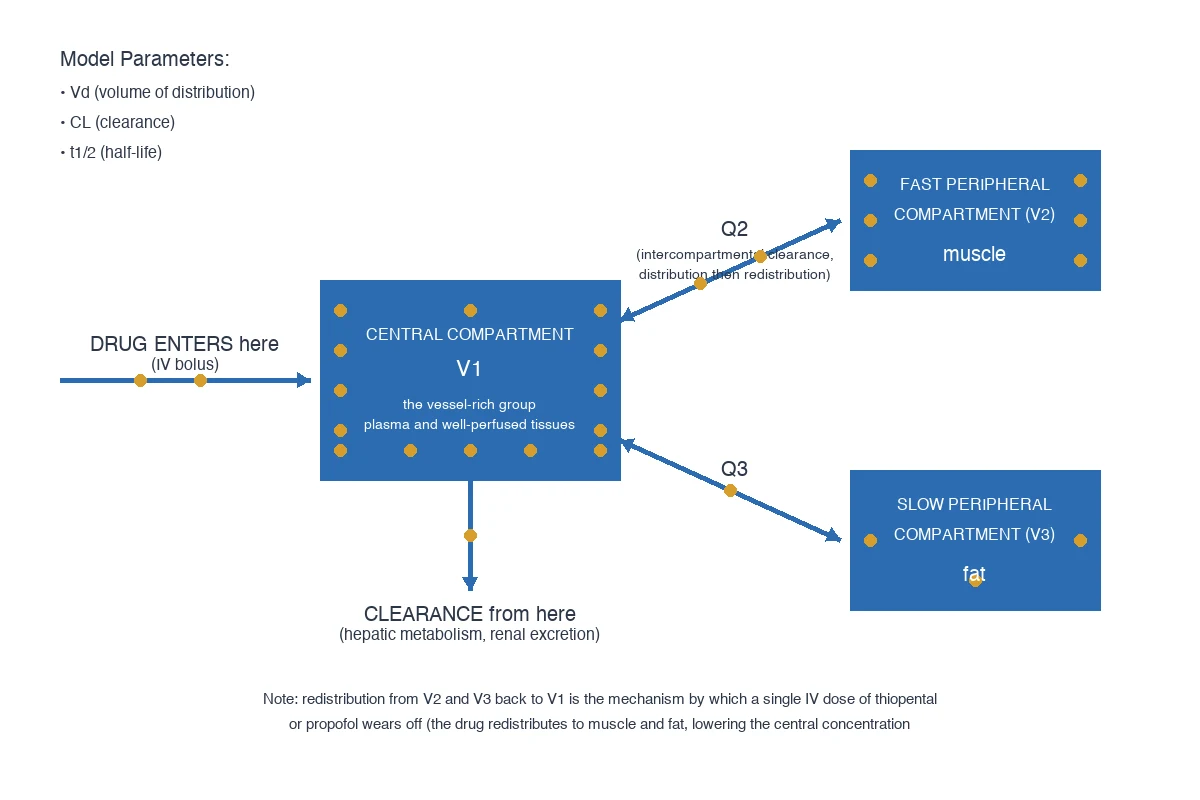
Typical anaesthetic IV model (3-compartment mamillary): [1]
- V1: plasma + highly perfused instantaneous mix (heart, brain, liver, kidney conceptually).
- V2: rapidly equilibrating peripheral (muscle).
- V3: slowly equilibrating (fat) for lipophilic drugs.
- k10: elimination rate constant from V1.
- k12, k21, k13, k31: intercompartmental transfers. [1]
Plasma concentration after bolus: triexponential
C(t) = Ae^(−αt) + Be^(−βt) + Ge^(−γt)
with α ≫ β ≫ γ corresponding to rapid distribution, slower distribution, terminal elimination. [1]
Macro parameters examiners want
| Parameter | Meaning | Relation |
|---|---|---|
| Vd | Apparent volume | Amount/concentration (various Vss, V1…) |
| CL | Clearance | Volume plasma cleared/time; dose rate = CLss × Css |
| t½ | Half-life | 0.693 × V/CL (one-compartment); multi half-lives if multi-compartment |
| ke0 | Effect-site equilibration | Links plasma to effect compartment for TCI |
| F | Bioavailability | Fraction reaching systemic circulation |
Steady state: input rate = elimination rate; time to ss ~3–5 half-lives of the relevant terminal phase (long for huge Vd drugs). [1]
Bolus vs infusion intuition
- Bolus offset of induction agents often distribution, not elimination (thiopental classic).
- Infusion fills peripherals → recovery governed by CSHT (sister leaf).
- Loading dose ≈ Ctarget × V1 (or Vd depending on target); maintenance rate ≈ Ctarget × CL. [1]
Physiological determinants
- CO and regional flows move drug to tissues and liver/kidney.
- Protein binding affects free fraction and sometimes Vd/CL interpretation.
- Extraction ratio (hepatic leaf) decides flow- vs capacity-limited clearance.
- Age, obesity, pregnancy, CPB alter V and CL — models may mis-specify. [1]
TCI link (keep applied)
Target-controlled infusion uses population PK parameters (V1, V2, V3, CLs, ke0) to drive a pump toward plasma or effect-site targets. Marsh vs Schnider (propofol) differ in covariates and V1 — know they are models, not truth, and age/weight matter. Minto for remifentanil. [1]
Linearity and context
First-order linear PK assumed in standard models: double dose → double concentration. Non-linearity appears with saturation (phenytoin), time-varying clearance, or deep hypothermia/CPB extremes. [1]
Numbers / relations board
- CL = rate/Css
- Vss related to distribution into peripherals
- Half-life alone does not determine infusion recovery (see CSHT)
- ke0 larger → faster plasma–effect equilibration (remifentanil fast; fentanyl slower) [1]
Bolus decline
- Distribution phases
- α then β then γ
- Wake may be redistribution
- V1 critical for peak
Infusion behaviour
- Fill V2/V3
- Css = rate/CL
- CSHT rules recovery
- Model drives TCI
Viva scripts
Draw 3-compartment mamillary model and label k’s. [1]
Write triexponential C(t). [1]
Explain why thiopental wake-up is redistribution. [1]
Relate Css to infusion rate and CL. [1]
Extended viva dialogue
Examiner: What is V1? [1]
Candidate: The central compartment volume — the apparent volume that dilutes drug instantly after IV injection to produce the initial concentration. A small V1 means a higher peak concentration for the same bolus. [1]
Examiner: How does clearance determine infusion rate? [1]
Candidate: At steady state, infusion rate equals clearance times target concentration. If clearance falls in shock or liver failure, the same infusion rate produces a higher steady-state concentration. [1]
Clinical synthesis: Compartments are a map for peaks, redistribution, steady state and TCI — speak in V and CL, not only half-life. [1]
Rate constants and half-lives relationship
Macro rate constants α, β, γ are roots of the characteristic equation from micro constants k10, k12, k21… You need not derive in the exam, but must state plasma decline is a sum of exponentials after IV bolus. [1]
Effect compartment
dCe/dt = ke0 (Cp − Ce). Larger ke0 → faster equilibration (remifentanil). Explains hysteresis: peak effect after peak plasma for slower drugs. [1]
Worked SAQ
SAQ: Describe a three-compartment mamillary model for an IV anaesthetic (8 marks)
Drug enters the central compartment V1 (plasma and well-perfused tissues) and distributes to rapid and slow peripheral compartments V2 and V3 via first-order rate constants, with elimination from V1 (k10). After a bolus, concentration falls multi-exponentially as distribution then elimination occur. Infusion rates at steady state equal clearance times target concentration; recovery after long infusions depends on context-sensitive half-time as peripherals empty back into V1. [1]
Primary exam expansion — dense examiner pack
Micro-constants, hybrid constants and parameters you must name
After IV bolus into V1, the system of first-order ODEs yields plasma concentration as a sum of exponentials. Examiners expect: [1]
| Symbol | Meaning | Clinical translation |
|---|---|---|
| k10 | Elimination rate from V1 | Links to clearance: CL = k10 × V1 |
| k12, k21 | V1 ↔ V2 transfer | Fast distribution (muscle-rich) |
| k13, k31 | V1 ↔ V3 transfer | Slow distribution (fat/lipophilic drugs) |
| α, β, γ | Hybrid macro rate constants | Slopes of log-concentration phases |
| A, B, G (or C) | Intercept coefficients | Depend on dose and volumes |
| Vss | Steady-state volume of distribution | V1 + V2 + V3 (mamillary, elimination from V1) |
| MRT | Mean residence time | Vss/CL for IV bolus in linear kinetics |
| ke0 | Effect-site equilibration constant | TCI effect-site targeting |
Do not claim that α equals k12 in multi-compartment drugs — α, β, γ are eigenvalues of the rate matrix, not single micro-constants. [1]
Bolus peak, redistribution and wake-up without metabolism
- IV bolus mixes in V1 → high Cp peak → rapid equilibration with vessel-rich group (including brain for lipophilic agents).
- Drug leaves V1 into V2/V3 → Cp falls even if little drug has been metabolised.
- Effect-site concentration falls below hypnotic threshold → patient wakes (redistribution offset).
- Later, drug returns from fat/muscle while k10 slowly eliminates total body load. [1]
Classic pair: thiopental and propofol after single induction dose. Contrast with recovery after prolonged infusion (context-sensitive half-time leaf). [1]
Loading dose and maintenance — equations examiners want written
- Loading dose (plasma target) ≈ Ctarget × Vd_appropriate. Immediate peak after IV often uses V1. If you load to Vss for a high-Vd drug, initial Cp may be dangerously high while distribution is incomplete.
- Maintenance infusion rate at steady state = Ctarget × CL. Units must match (µg/mL × mL/min = µg/min).
- Time to steady state ≈ 3–5 terminal half-lives for constant infusion without loading — long for drugs with large Vss or low CL. [1]
Multi-compartment half-lives
- t½α (distribution half-life): rapid fall after bolus — redistribution dominated.
- t½β / t½γ: slower phases; terminal half-life reflects the slowest eigenvalue and can be long while clinical recovery after a short exposure is still fast.
- Never use terminal half-life alone to predict emergence from TIVA — that is why CSHT exists. [1]
Bioavailability and extravascular routes
For oral/IM/epidural drugs: F = AUCextravascular / AUCiv (same dose). First-pass hepatic extraction reduces F for high-extraction oral drugs. Epidural fentanyl has complex systemic plus local kinetics — do not treat as a simple IV clone. [1]
TCI models — what differs and why the viva cares
| Model | Drug | Key covariate themes | Pitfall |
|---|---|---|---|
| Marsh | Propofol | Weight-scaled; larger V1 historically | Age effects weaker than Schnider |
| Schnider | Propofol | Age, height, weight, LBM; smaller V1 | Rapid bolus predictions differ |
| Eleveld | Propofol | Broad age continuum including children | Implementation dependent |
| Minto | Remifentanil | Age, LBM | Still titrate to effect |
Population models are typical-patient maps. Obesity, CPB, haemorrhage, hepatic failure and concurrent vasoactives break assumptions. Always close the loop with clinical signs, processed EEG and haemodynamics.[1][2]
Body size, renal impairment and virtual-trial thinking
Renal impairment and body size are major PK covariates; virtual trials show clearance and volume scale non-linearly with size and organ function.[6] Paediatrics is not small-adult per kg — allometric scaling (often CL proportional to weight to the power 0.75) appears in modern models.[3]
Remimazolam and esterase-cleared agents
Ultra-short agents with organ-independent metabolism still need compartment language for onset (V1, ke0) even when offset is esterase-driven and CSHT-flat.[4] Assay work underpins model validation, not routine theatre care.[5]
Graph viva checklist (timed)
- Draw mamillary three-compartment box diagram; arrows k12/k21/k13/k31/k10.
- Sketch log Cp versus time after bolus: steep then shallower phases.
- Write C(t) = A e^(−αt) + B e^(−βt) + G e^(−γt).
- State infusion rate = CL × Css.
- Mention ke0 and hysteresis loop (Cp versus effect).
- Say when recovery is redistribution versus elimination versus CSHT. [1]
Clinical scenarios with model language
Obese patient on propofol TCI: total body weight versus lean body mass inputs change predicted Cp; clinical depth may not match display — titrate. Shock with reduced hepatic blood flow: high-extraction drug clearance falls → higher Css at same infusion rate. Massive blood loss or CPB: V1 and CL change acutely; models lag reality. Paediatric preschool PK: maturation of clearance pathways can dominate weight scaling.[3]
SAQ mark plan — multi-compartment PK (10 marks)
Define compartment and mamillary assumption (2). Label V1/V2/V3 and rate constants (2). Write multi-exponential equation and name phases (2). Link CL and V to half-life and infusion rate (2). Clinical example: bolus offset versus infusion recovery or TCI caveat (2). [1]
Extra viva lines
Q: Why is Vd apparent? A: It is amount divided by concentration referenced to plasma — can exceed body volume if tissue binding concentrates drug. Q: What is clearance if not how fast the drug disappears? A: Volume of plasma completely cleared of drug per unit time — a flow-like parameter, not a pure rate constant. Q: Why might two drugs share terminal half-life but differ clinically? A: Different V1, distribution speeds, ke0, potency and CSHT curves — half-life is one scalar of many. [1]
High-yield viva battery and numbers lock-in
One-page formula sheet
- One-compartment: C(t) = (Dose/V) e^(−kt); t½ = 0.693/k; CL = kV = 0.693 V / t½
- Multi-compartment bolus: C(t) = A e^(−αt) + B e^(−βt) + G e^(−γt)
- Steady-state infusion: Css = Rate / CL; Rate = Css × CL
- Loading dose ≈ Ctarget × V1 (peak control) or carefully chosen Vd
- Bioavailability F = AUCpo/AUCiv × Doseiv/Dosepo
- MRT ≈ Vss/CL (IV bolus linear kinetics)
- Effect site: dCe/dt = ke0 (Cp − Ce) [1]
Redistribution versus elimination — two-sentence contrast
Redistribution is net movement from vessel-rich effect sites into muscle/fat that lowers plasma and effect-site concentrations after a bolus without requiring metabolism. Elimination is irreversible removal from the body (metabolism/excretion) described by clearance acting on plasma concentration, equal to k10 × V1 in the central-elimination mamillary model. [1]
TCI failure modes checklist
Wrong patient covariates; obese weight scalar mismatch; haemorrhage changing V1; low CO changing high-E clearance; syringe empty/disconnect (awareness risk in TIVA); model–drug mismatch (using propofol model for another drug); ignoring residual opioid when interpreting processed EEG. Treat the patient, not the pump number. [1]
Full viva dialogue (additional)
Examiner: Define volume of distribution at steady state. [1]
Candidate: Vss is the apparent volume relating the amount of drug in the body to plasma concentration when distribution equilibrium is reached; in a three-compartment model it is conceptually the sum of compartment volumes. It is not a real anatomical space. [1]
Examiner: A drug has short terminal half-life but long CSHT after infusion — possible? [1]
Candidate: Terminal half-life and CSHT answer different questions. More commonly we see long terminal half-life with short clinical recovery after brief exposure because distribution clears plasma. If CSHT is long after infusion, peripherals have loaded — recovery is slow regardless of how the terminal half-life is marketed. [1]
Examiner: Write the relationship between clearance, concentration and elimination rate. [1]
Candidate: Elimination rate equals CL × Cp (first-order linear kinetics). At steady state this equals the infusion rate. [1]
Exam traps
- Equating half-life with duration of action after IV bolus of lipophilic induction agents.
- Loading to Vss with a rapid bolus for high-Vd drugs (toxic peak).
- Believing TCI displays measured concentrations.
- Forgetting ke0 when discussing time to peak effect.
- Using total body weight indiscriminately in all models. [1]
References
- [1]Ye J, et al. A Prospective Study of Marsh PK-PD Model and Schnider PK-PD Model During Anesthesia Induction for Obese Patients Undergoing Elective Heart Surgery Pharmacol Res Perspect, 2026.PMID 42286797
- [2]Introna M, et al. Target concentrations of propofol predicted by four different pharmacokinetic/pharmacodynamic models to induce loss of consciousness in neurosurgical patients J Anesth Analg Crit Care, 2026.PMID 42231496
- [3]de Barros Garioud AL, et al. Pharmacokinetics of Intravenous Melatonin in Preschool-Aged Pediatric Surgical Patients Paediatr Anaesth, 2026.PMID 42325096
- [4]Dong Y. Remimazolam in anesthesia and sedation: A narrative review J Anesth Transl Med, 2025.PMID 41929379
- [5]Ng MKL, et al. Development and Application of an LC-MS/MS Assay for Plasma Propofol Quantification in Major Noncardiac Surgical Patients to Evaluate Target-Controlled Infusion Algorithms Ther Drug Monit, 2026.PMID 42214089
- [6]Marques L, et al. Model-Based Virtual Clinical Trial Reveals Renal Impairment and Body Size as Key Determinants of Pharmacokinetic Variability and Drug-Drug Interaction Risk in Propranolol Therapy Pharmaceutics, 2026.PMID 42357253