Anaes · Cardiac anaesthesia
Anaesthesia for adult congenital heart disease
Also known as ACHD noncardiac surgery · Fontan anaesthesia adult · Grown-up congenital heart GUCH
Exam-pass ACHD for noncardiac surgery: lesion classification, shunt and PVR goals, Fontan physiology, endocarditis/arrhythmia risks, and centre selection for ANZCA Final.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Why this is examined / the one-line answer
Adults with congenital heart disease (ACHD / GUCH) increasingly appear on general, obstetric, and emergency lists. Maxwell et al. showed higher perioperative morbidity and mortality after major noncardiac surgery versus matched controls — examiners want physiology-driven plans, not sympathy.[1]
One-liner: I map native anatomy and surgical pathway, identify residual shunts, Fontan, or PHT physiology, defend PVR and SVR goals, de-air everything if right-to-left risk exists, and involve ACHD cardiology for moderate–complex disease. [1]
Preoperative assessment
History that changes the plan
- Original diagnosis and operations (arterial switch, tetralogy repair, Fontan stages, Mustard/Senning, Glenn).
- Residual lesions, exercise tolerance, cyanosis at rest or on effort.
- Arrhythmias, pacemakers/ICDs, anticoagulation.
- Pulmonary hypertension, heart failure, previous endocarditis.
- Fontan extras: liver disease, protein-losing enteropathy, plastic bronchitis, thromboembolism.
- Learning disability / transition care — consent complexity. [1]
Investigations
Recent echo/MRI/cath reports (not a decade-old letter alone), ECG, baseline saturations, Hb (secondary erythrocytosis in cyanosis), coagulation, LFTs, renal function. Functional class matters more than calendar age.[3]
Risk framing
ACHD increases adverse perioperative outcomes after major noncardiac surgery; complexity and comorbidities drive risk. Do not trivialise “simple repaired ASD” without confirming no residual lesion — and do not anaesthetise complex Fontan/Eisenmenger electively in a district list without specialist support.[1]
Applied physiology clusters
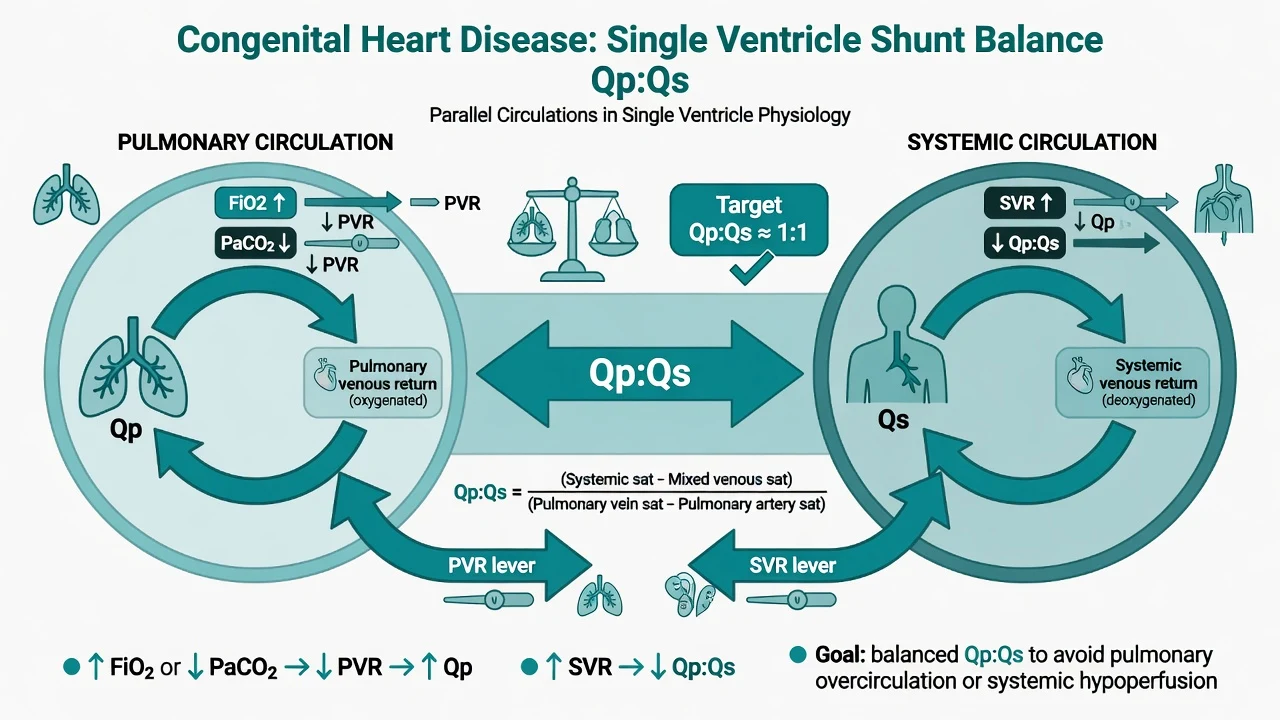
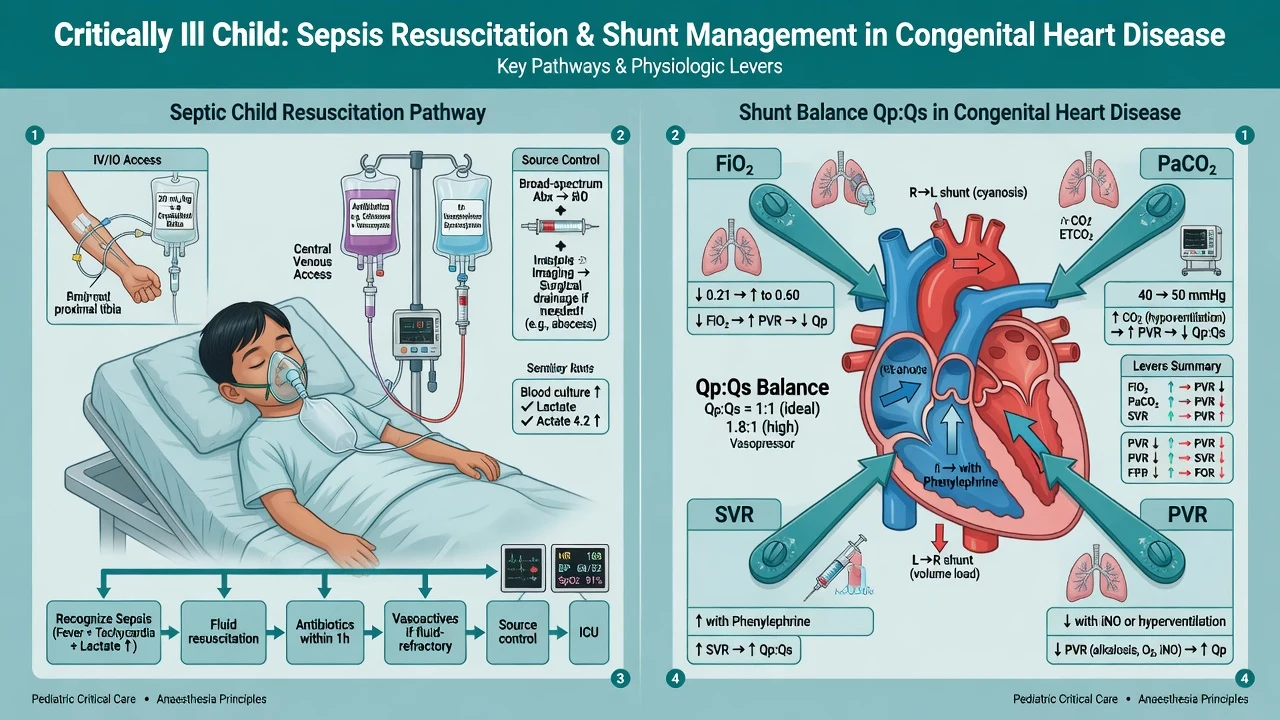
Shunt lesions
| Physiology | Goals | Avoid |
|---|---|---|
| Left-to-right | Balance ventilation; avoid extreme SVR rise if harmful pulmonary overcirculation history | Ignoring residual Qp:Qs |
| Right-to-left / Eisenmenger | Maintain SVR; keep PVR low; de-air lines | Sudden SVR fall; hypoxia/hypercarbia/acidosis; air emboli |
| Balanced shunts | Titrate SVR/PVR to sats and BP | Single-number dogma without clinical context |
Paradoxical embolus: any right-to-left communication (including residual PFO physiology in some contexts) — air filters on IV lines, meticulous de-airing, careful drug reconstitution. [1]
Fontan circulation (single ventricle, passive pulmonary flow)
Systemic venous return enters the pulmonary arteries without a subpulmonary ventricle. Pulmonary blood flow depends on: [1]
- Adequate preload
- Low PVR
- Low mean intrathoracic pressure
- Sinus rhythm (atrial contribution and AV synchrony)
- Competent systemic ventricle [1]
Fontan killers: hypovolaemia, high PEEP/high mean airway pressure, hypoxia/hypercarbia (↑PVR), loss of sinus rhythm, high abdominal pressure (laparoscopy), haemorrhage, positive-pressure ventilation without optimisation.[2]
Obstructive / valvular residua
Residual AS/PS/coarctation gradients — lesion-specific loading goals (e.g. maintain SVR in residual AS). [1]
Cyanotic haematology
Secondary erythrocytosis raises viscosity; baseline “high Hb” may be appropriate. Coagulopathy and bleeding can coexist with thrombosis risk — do not venesect casually on the day of surgery. [1]
Anaesthetic goals
- Understand the circuit — draw it if needed.
- Maintain oxygen delivery (CO × CaO2); cyanotic patients may need higher Hb.
- Control PVR drivers (O2, CO2, pH, lung volumes, pain, temperature).
- Avoid bubbles with shunt risk.
- Specialist help for complex elective major cases. [1]
Technique matrix
Monitoring and equipment
Standard + arterial line for major/complex cases. Central access carefully — know Glenn/Fontan pathways before wires travel unexpected routes. TOE if major surgery or instability. Air filters on IV lines if R-to-L risk. Defibrillator pads. Vasopressors ready; pulmonary vasodilator thinking (oxygen, iNO in specialist centres). Endocarditis prophylaxis only when current guidelines indicate (not automatic for all ACHD forever). [1]
Intraoperative management
Induction: titrate; support SVR if R-to-L physiology (vasopressor ready). [1]
Ventilation: avoid hypoxia/hypercarbia; moderate tidal volumes; titrate PEEP carefully in Fontan — high mean airway pressure cuts pulmonary blood flow.[2]
Fluids: Fontan often preload-dependent, but liver/renal limits exist; use dynamic assessment. [1]
Regional: excellent for analgesia when appropriate; avoid sudden profound SVR loss in Eisenmenger without a plan (cautious titrated epidural or alternative techniques). [1]
Laparoscopy: pneumoperitoneum raises SVR and impairs venous return — lower pressures, careful ventilation, readiness to desufflate. [1]
Arrhythmia readiness: atrial arrhythmias are common and poorly tolerated in Fontan — early cardioversion if unstable. [1]
Crisis pivots
Desaturation in shunt patient
Increase FiO2; treat ↑PVR causes (hypoxia, hypercarbia, acidosis, high airway pressure, pain); raise SVR if R-to-L increasing; exclude tube problems. [1]
Fontan low output
Fluids if empty; reduce mean airway pressure; correct CO2/O2; restore sinus rhythm; inotrope for systemic ventricle; expert help early.[2]
Unstable arrhythmia
DC cardioversion sooner rather than later in Fontan; correct electrolytes; antiarrhythmics with ACHD advice when stable enough. [1]
Bleeding + cyanotic physiology
Balanced resuscitation; remember their baseline Hb is often high — oxygen delivery mathematics differs from the anaemic elderly. [1]
Paradoxical embolus suspicion
Support ABCs; prevent further air; imaging/neurology pathways; prevention is the exam mark. [1]
Postoperative plan
Monitored bed for complex ACHD. Early ACHD cardiology review after major surgery. Thromboprophylaxis balancing polycythaemia and bleeding. Restart anticoagulation carefully. Watch liver/renal function in Fontan. [1]
Special populations
- Pregnancy in ACHD: high-stakes multidisciplinary — separate detailed topic; WHO maternal cardiovascular risk classification thinking.
- Learning disability / transition care: supported decision-making.
- Heart failure / transplant assessment patients: limited reserve.
- Home pulmonary vasodilators: do not stop without a plan.
- Pacemaker/ICD: standard peri-op device management. [1]
SAQ answer scaffold
A 28-year-old Fontan patient needs laparoscopic appendicectomy. Outline anaesthetic management. [1]
- Anatomy map (3): single ventricle, passive PBF, residual issues, baseline sats/Hb.[2]
- Risk (2): ACHD major NCS risk elevation; specialist input.[1]
- Goals (3): preload, low PVR, sinus, careful ventilation/PEEP.
- Technique (3): titrated GA or appropriate regional; low insufflation; air filters if any shunt risk.
- Postop (2): monitored bed, early mobilisation vs VTE risk, cardiology review.
Viva stem bank and model phrases
Stem 1: “Why is ACHD higher risk for noncardiac surgery?”
Model: “Observational data show increased morbidity and mortality after major noncardiac surgery compared with matched controls — complexity and residual physiology drive risk.”[1]
Stem 2: “Fontan and PEEP?”
Model: “High mean airway pressure can reduce pulmonary blood flow because there is no subpulmonary pump — I use the least PEEP that maintains oxygenation and aim for early extubation when feasible.” [1]
Stem 3: “Air bubbles?”
Model: “With right-to-left shunt risk I use filters and meticulous de-airing to reduce paradoxical embolus.” [1]
Stem 4: “Eisenmenger for hip replacement — spinal?”
Model: “Sudden SVR fall can increase right-to-left shunt. If neuraxial is chosen it must be carefully titrated with vasopressor readiness; many prefer carefully managed GA with SVR support — individualise with ACHD team.” [1]
Stem 5: “Draw the Fontan.”
Model: “Systemic veins to PA confluence/connection, lungs, pulmonary veins to systemic ventricle, aorta to body — passive pulmonary flow.” [1]
Stem 6: “Endocarditis prophylaxis?”
Model: “Only when current guideline indications are met for the procedure and lesion — not automatic for every ACHD patient forever.” [1]
Stem 7: “Where should complex elective major surgery occur?”
Model: “In a centre with ACHD cardiology and appropriate intensive care — not as a surprise on a cold orthopaedic list.”[3]
Common traps
- Generic “keep them warm and give fluids” without circuit understanding
- Forgetting air filters
- High PEEP Fontan without thought
- Spinal in Eisenmenger without SVR plan
- No specialist referral for complex elective major surgery
- Treating cyanotic high Hb as automatic transfusion trigger
- Ignoring atrial arrhythmia risk in Fontan [1]
Fontan goals — FLOW
Examiner mental map
- Map anatomy and repair pathway.
- Cluster physiology (shunt / Fontan / PHT / residua).
- PVR/SVR and preload plan.
- Air and arrhythmia risks.
- Fontan specifics (FLOW).
- Centre escalation for complex disease. [1]
Whiteboard physiology beats memorised lesion lists. [1]
References
- [1]Maxwell BG, Wong JK, Kin C, Lobato RL Perioperative outcomes of major noncardiac surgery in adults with congenital heart disease Anesthesiology, 2013.PMID 23907357
- [2]McNamara JR, McMahon A, Griffin M Perioperative Management of the Fontan Patient for Cardiac and Noncardiac Surgery J Cardiothorac Vasc Anesth, 2022.PMID 34023201
- [3]Baehner T, Ellerkmann RK Anesthesia in adults with congenital heart disease Curr Opin Anaesthesiol, 2017.PMID 28306681