Anaes · Paediatric anaesthesia
Paediatric anaesthesia neurotoxicity debate: GAS, MASK, PANDA and counselling
Also known as Anaesthetic neurotoxicity children · GAS trial · PANDA study · MASK study · SmartTots
Exam-exhaustive synthesis of the paediatric anaesthetic neurotoxicity debate: animal apoptosis signal, GAS trial 2- and 5-year outcomes, PANDA and MASK human studies, FDA/SmartTots context, and parent counselling for necessary versus deferrable surgery.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Why this is examined
Parents and surgeons ask about “brain damage from anaesthesia.” Fellowship candidates must separate animal signals from human trials, name GAS, PANDA, and MASK findings accurately, and counsel without false certainty or harmful delay. The topic tests evidence appraisal as much as pharmacology: randomisation versus confounding, primary versus secondary endpoints, and the ethics of necessary surgery in infancy.
[1]Animal evidence and translation limits
Rodent and non-human primate studies show anaesthetic-induced neuroapoptosis and behavioural changes after prolonged or repeated exposures during synaptogenesis windows. Agents implicated in various models include volatile anaesthetics, propofol, ketamine, and benzodiazepines. Mechanisms discussed in the literature include GABA-A potentiation, NMDA antagonism, disrupted neurotrophic signalling, and altered synaptogenesis — but mechanism lectures are not a licence to claim proven human harm at clinical doses.
[4]Translation fails when:
[1]- Doses and durations exceed typical paediatric cases
- Animals lack concurrent surgery, inflammation, pain, and human social environment
- Outcome tests do not map cleanly to human IQ, language, or school performance
- Confounding by underlying disease is absent in healthy animal models
- Developmental windows in rodents do not equal human infancy month-for-month
Human research therefore prioritised observational cohorts and the rare randomised design (GAS).
[1]GAS trial — the only major RCT
Design
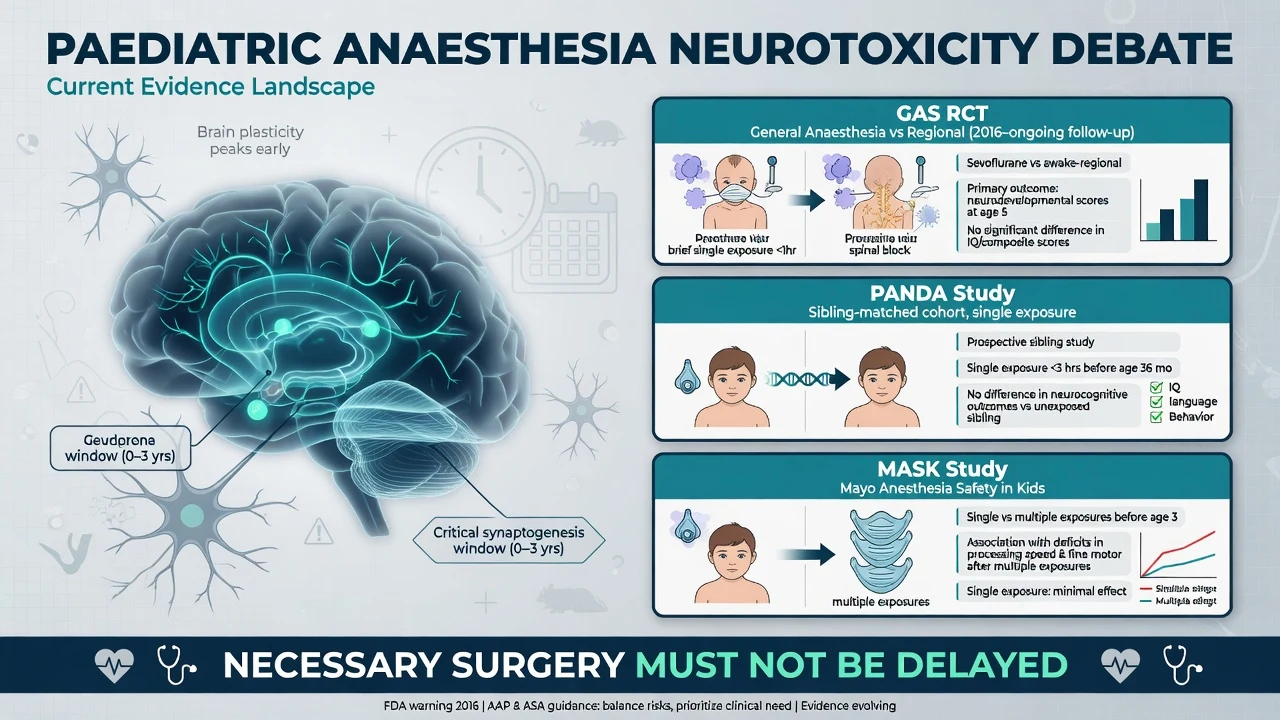
Infants requiring inguinal herniorrhaphy were randomised to awake-regional anaesthesia versus sevoflurane general anaesthesia (brief exposure). The question was whether a short sevoflurane anaesthetic in infancy impairs neurodevelopment compared with a regional technique that largely avoids volatile anaesthetic exposure.
[1]Two-year outcome
No significant difference in the primary cognitive composite (Bayley-III cognitive score) between groups — reassuring for brief sevoflurane versus regional in this setting.[1]
Five-year outcome
No significant difference in full-scale IQ; continued strong reassurance for brief single exposure in infancy for the studied population and endpoint.[2]
Limitations candidates must own
- Single brief procedure in mostly healthy infants
- Not powered for every subtle domain-specific effect in every subgroup
- Regional failures crossed over to general anaesthesia (analyse with intention-to-treat understanding)
- Does not answer prolonged neonatal cardiac surgery, repeated exposures, or critical illness
- Does not prove all agents equal at all doses forever
Exam phrase: “GAS provides the highest-level evidence that a brief sevoflurane anaesthetic for infant hernia repair was developmentally equivalent to awake-regional at two and five years for the primary cognitive endpoints studied.”
[1]PANDA study
Sibling-matched cohort design: children with a single general anaesthesia exposure before age 36 months (often hernia surgery) compared with an unexposed sibling. No significant difference in global cognitive function (IQ) in later childhood for that single-exposure scenario.[3] Strength: partial control for family and genetic background. Limitation: observational; residual confounding; mostly single exposure.
MASK study
Mayo population cohort comparing unexposed, single-exposed, and multiply exposed children before age three. Primary outcome of general intelligence: no deficit associated with anaesthetic exposure. Some secondary signals appeared in fine motor performance and parent-reported behaviour or learning among multiply exposed children — hypothesis-generating and confounded by comorbidity and the need for repeated procedures.[4]
Do not quote MASK as proving that multiple anaesthetics cause learning disorders; quote it as: intelligence preserved overall, secondary domains need cautious interpretation.
[4]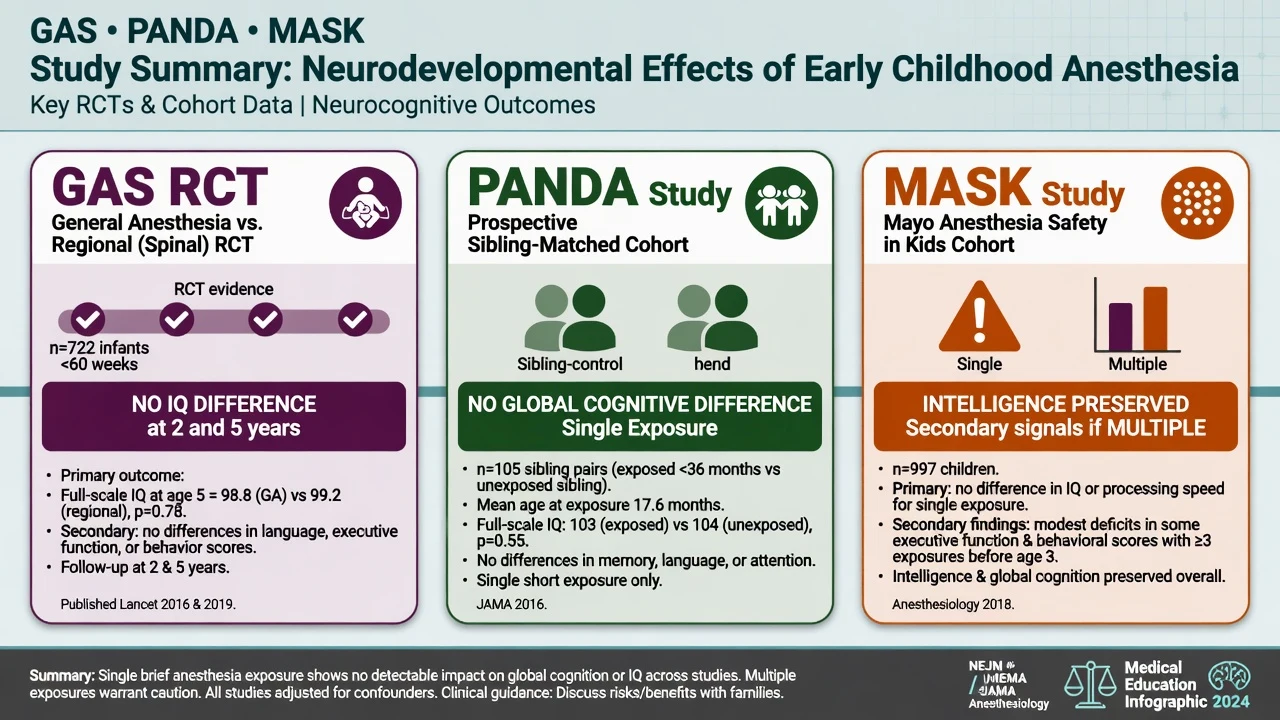
Regulatory and SmartTots context
FDA communications warned about repeated or lengthy use of general anaesthetics and sedation drugs in children under three years and in pregnant women in the third trimester, based largely on animal data plus incomplete human evidence. SmartTots and professional societies promote research and balanced messaging:
[4]- Necessary procedures should proceed without delay driven by fear
- Elective deferrable procedures might wait if clinically safe and surgically agreed
- Research into long and repeated exposures continues
In viva, acknowledge the warning without weaponising it against indicated care.
[1]Counselling framework (viva gold)
- Acknowledge the concern — animal data raised a legitimate scientific question
- State human evidence — GAS, PANDA, and MASK are reassuring for single brief exposures regarding global cognition
- Necessity first — delaying indicated surgery (obstructed hernia, abscess, testicular torsion, congenital lesions with risk) harms more than theoretical neurotoxicity
- Elective timing — if truly deferrable without medical downside, waiting can be reasonable after shared decision with the surgeon
- Uncertainty — prolonged, repeated, or critically ill exposures remain less well defined
- What we do practically — trained paediatric teams; multimodal care; avoid unnecessary long deep anaesthesia; maintain oxygenation, perfusion, glucose, CO2, and temperature
Sample parent script:
[1]“Laboratory studies raised a question about long or repeated anaesthetics in very young animals. The best human studies — including a randomised trial called GAS — are reassuring that a short anaesthetic for common infant surgery was not linked to differences in later IQ compared with spinal or regional techniques. We will not delay surgery your child needs. If a procedure is purely optional and can safely wait, we will discuss timing with the surgeon.”
[1]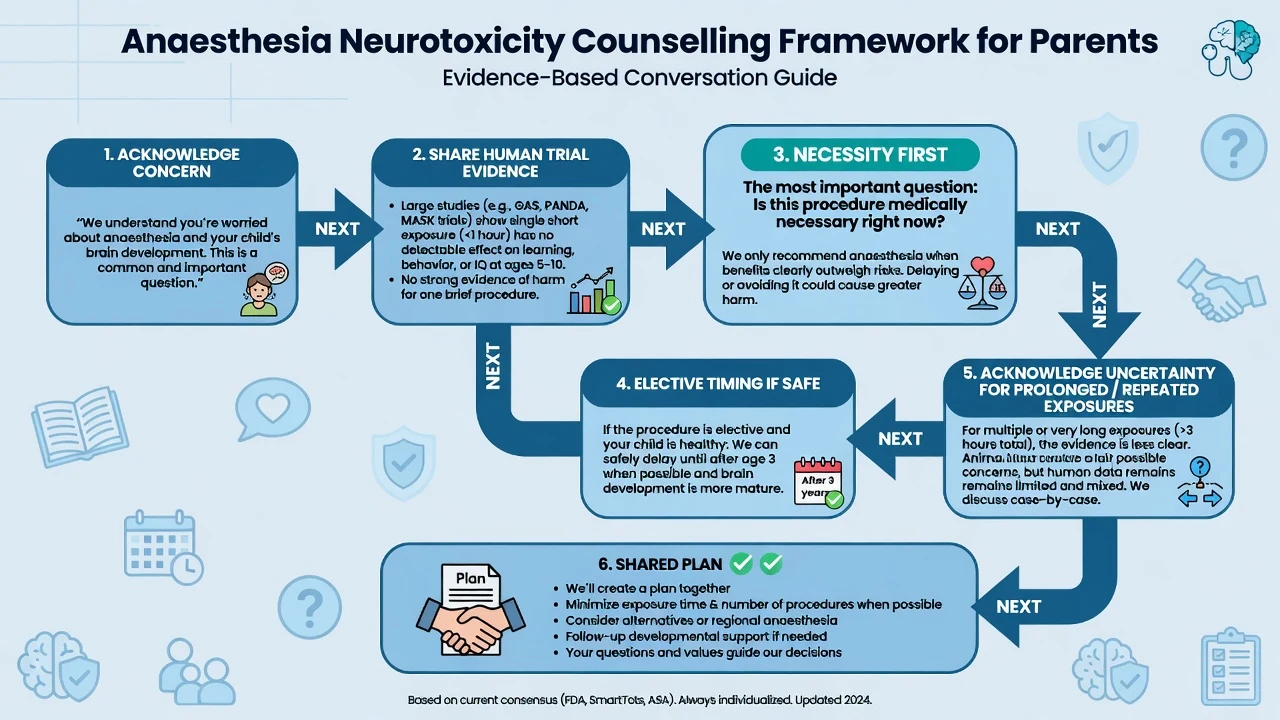
What remains unknown
- Prolonged anaesthesia for major neonatal and infant surgery
- Multiple sequential exposures in complex disease
- Interaction with inflammation, hypoxia, cardiopulmonary bypass, and critical illness
- Domain-specific subtle effects and educational outcomes at population scale
- Whether any specific agent is clearly safer in humans at equipotent clinical doses
- Fetal third-trimester exposure questions overlapping obstetric anaesthesia
Anaesthetic practice implications (not magic protocols)
- Do not invent unproven “brain-safe” TIVA dogma as established human fact
- Maintain physiological homeostasis meticulously — hypoxia and hypotension are not theoretical
- Use regional and multimodal analgesia to reduce needless depth and systemic opioid where appropriate
- Document indication and discussion when parents raise the issue
- Avoid stacking unnecessary premedication and prolonged deep planes “because the list is delayed”
Interaction with other paediatric topics
Emergence delirium is a short-lived recovery phenomenon, not proof of neurotoxicity. GAS does not redefine cardiorespiratory physiology of infants. Apnoea risk in ex-preterms is a monitoring issue, not a neurotoxicity endpoint. When parents conflate thrashing in PACU with “brain damage,” separate PAED-scored emergence delirium from the developmental debate.
[1]SAQ answer scaffold
- Animal signal and limits of translation
- GAS methods and 2- and 5-year results with accurate endpoints
- PANDA and MASK key findings and confounding
- Counselling script for a parent of a six-month-old needing hernia repair
- When you might defer elective imaging under GA
- What you would not claim
Viva stem bank
- “Is sevoflurane toxic to the infant brain?”
- “Summarise GAS in sixty seconds.”
- “How do you answer a parent who read about the FDA warning?”
- “Does TIVA eliminate neurotoxicity risk?”
- “This neonate needs emergency laparotomy — any delay for ‘neuroprotection’?”
Detailed comparison matrix for rapid recall
| Feature | GAS | PANDA | MASK |
|---|---|---|---|
| Design | RCT | Sibling cohort | Population cohort |
| Exposure | Brief sevo vs regional | Single GA | Single vs multiple |
| Primary message | No cognitive/IQ difference at 2 and 5 y | No IQ difference | Intelligence OK; secondary signals if multiple |
| Key limit | Brief healthy hernia population | Observational | Confounding in multi-exposed |
Cite accurately in SAQs.[1][2][3][4]
Parent FAQ bank with model answers
“Will this cause ADHD?”
“Some observational studies looked at behaviour after multiple exposures and results are mixed and confounded. The best evidence for a single short anaesthetic is reassuring for overall intelligence. We will not delay surgery your child needs.”
“Should we wait until age three for hernia repair?”
“Only if the surgeon agrees delay is safe. Incarceration risk and pain matter. Timing is a shared surgical–anaesthetic decision, not an internet rule.”
“Is total intravenous anaesthesia safer for the brain?”
“We do not have human proof that TIVA eliminates theoretical risk. We choose techniques for the whole patient — airway, surgery, recovery — and keep the anaesthetic only as deep and long as needed.”
How SmartTots messaging fits
Supports research and balanced communication: proceed with necessary care; consider deferring truly elective procedures if safe; avoid alarmism. Align your consent language with this balance.
[4]Examiner hostility management
If an examiner pushes “so you admit anaesthetics are toxic,” answer: “Animal data show a signal under certain conditions; human trials of brief single exposures are reassuring for global cognition; uncertainty remains for prolonged repeated exposures; necessity governs timing.”
[3]Common traps
Claiming zero risk forever; delaying orchidopexy or hernia repair for years without surgical input; quoting wrong trial endpoints; saying regional has zero drug exposure (systemic absorption and sedation still occur); ignoring confounding in observational multiple-exposure data; promising a specific agent is proven safer in humans; equating animal apoptosis photos with clinical IQ loss.
[3]Evidence table for rapid revision
How to appraise a new neurotoxicity paper in the exam
Ask: Was exposure single or multiple? How long? What age? What primary endpoint was pre-specified? Was there randomisation or only association? What confounders (syndromes, hypotension, hypoxia, socioeconomic status, repeated illness)? Is the effect size clinically meaningful? Does it change consent for emergency care? This appraisal structure scores marks even when the paper is unfamiliar.
[3]Ethical framing
Non-maleficence includes avoiding both theoretical over-fear and casual unnecessary exposure. Beneficence prioritises treating painful, obstructive, or infectious surgical disease. Justice includes not denying indicated anaesthesia to disadvantaged children because of media-driven fear. Shared decision-making records the discussion without coercing parents into unsafe delay.
[4]Pregnancy and third-trimester overlap
Regulatory language often groups young children with third-trimester fetuses. Obstetric anaesthesia for indicated procedures (cervical cerclage, non-obstetric emergency surgery, caesarean) should not be withheld for theoretical fetal neurotoxicity when maternal or fetal welfare requires intervention. Use the same honesty-plus-necessity framework.
[4]Research horizon (high-level only)
Ongoing work examines longer exposures, advanced neuroimaging correlates, and educational outcomes. Until higher-quality data redefine practice, clinical standards remain: necessary care proceeds; physiology is protected; counselling is balanced; unproven “neuroprotective cocktails” are not sold as certainty.
[3]Extended viva model answers
“Is sevoflurane toxic?”
“In animals at certain doses and durations, apoptotic changes occur. In humans, the best evidence for a brief single exposure — GAS, supported by PANDA and MASK intelligence outcomes — is reassuring. I will not claim universal lifelong safety for all exposures, and I will not delay necessary surgery.”
“Why not always use regional?”
“Regional is excellent when appropriate, but it is not always feasible, sufficient, or safer overall. GAS used awake-regional as a comparator, not as a mandate for every infant. Failed regional, patient factors, and surgical needs still require general anaesthesia.”
“Multiple anaesthetics for oncology care?”
“MASK secondary signals in multiply exposed children may reflect disease burden and repeated procedures as much as anaesthetic molecules. I minimise unnecessary visits under GA, coordinate procedures when safe, maintain physiology, and avoid fear-based denial of indicated treatment.”
Numbers and names to memorise
- GAS 2-year: Bayley cognitive composite — no significant difference sevoflurane vs awake-regional.[1]
- GAS 5-year: full-scale IQ — no significant difference; equivalence framing in the paper’s interpretation.[2]
- PANDA: sibling-matched single exposure before 36 months — no IQ difference.[3]
- MASK: intelligence preserved; secondary behavioural/motor signals with multiple exposures need cautious reading.[4]
Documentation snippet
“Discussed anaesthetic neurotoxicity concerns with parents. Explained animal data limitations and reassuring human evidence for brief single exposure (GAS/PANDA/MASK context). Proceeding with indicated surgery today because delay risks [hernia incarceration / infection / other]. Parents verbalised understanding.”
[3] [3]Fellowship consolidation — neurotoxicity evidence and counselling
[1]The neurotoxicity debate requires accurate trial names, honest uncertainty, and ethical prioritisation of necessary care. Animal models show anaesthetic-associated neuroapoptosis after prolonged or repeated exposures during synaptogenesis, but translation is limited by dose, duration, lack of surgery, and non-equivalent outcome measures.
[1]GAS is the key randomised trial: infants for inguinal herniorrhaphy assigned to awake-regional anaesthesia versus sevoflurane general anaesthesia. At two years, Bayley cognitive outcomes did not differ significantly. At five years, full-scale IQ did not differ significantly. This is the strongest human evidence for brief single early exposure in a relatively healthy surgical population.
[1]PANDA used sibling matching for single general anaesthesia exposure before 36 months and found no significant difference in later global IQ compared with unexposed siblings. MASK, a population cohort, found no primary deficit in general intelligence with exposure, while some secondary behavioural or fine-motor signals appeared among multiply exposed children and remain confounded by disease burden.
[3]Regulatory warnings about lengthy or repeated anaesthetic and sedation drug use in young children and third-trimester pregnancy were driven largely by animal data plus incomplete human evidence. Professional messaging emphasises that necessary procedures should proceed and that truly elective deferrable procedures can wait if surgically safe.
[4]Counselling framework: acknowledge concern, summarise reassuring human evidence for single brief exposures, prioritise necessity, discuss elective timing jointly with surgeons, admit uncertainty for prolonged or repeated critical-illness exposures, and explain practical safety measures including trained teams and physiological homeostasis.
[3]Do not claim lifelong zero risk for all exposures. Do not delay obstructed hernia, torsion, abscess drainage, or other time-critical surgery. Do not assert that TIVA is proven non-neurotoxic in humans. Do not mock parents who read FDA or media summaries.
[1]Practice implications are modest and sensible: avoid unnecessary prolonged deep anaesthesia, combine procedures when safe, maintain oxygenation perfusion glucose and carbon dioxide, use multimodal and regional techniques appropriately, and document discussions. Unproven neuroprotective cocktails should not be sold as certainty.
[1]Emergence delirium is a short recovery phenomenon and is not evidence of long-term neurotoxicity. Coté apnoea risk in ex-preterms is a monitoring issue separate from IQ endpoints. Keep domains distinct in viva answers.
[1]Sixty-second GAS summary for the examiner: randomised infant hernia trial of sevoflurane versus awake-regional; no significant difference in primary cognitive outcome at two years or IQ at five years; brief single exposure population; does not answer prolonged neonatal cardiac surgery or multiple exposures.
[1]Ethical bottom line: non-maleficence includes avoiding both casual unnecessary exposure and fear-driven denial of indicated anaesthesia. Beneficence prioritises treating surgical disease that threatens life, organ function, or development more certainly than theoretical drug toxicity.
[1] [1]Written consent and documentation examples
"Discussed parental concerns regarding anaesthetic effects on the developing brain. Explained that animal studies raised a scientific question after prolonged or repeated exposures, while human evidence from the GAS randomised trial and supporting observational studies (PANDA, MASK) is reassuring for a single brief anaesthetic regarding global cognitive outcomes. Proceeding today because surgery is indicated and delay carries [state risk]. Parents verbalised understanding and agreement."
[3]For elective deferrable imaging under GA: "Shared decision with procedural team to defer non-urgent MRI under GA for three months because no clinical red flags and family preference after discussion of uncertain theoretical risks of elective exposure."
[3]Critical appraisal checklist for any new paper
- Randomised or observational?
- Single or multiple exposures?
- Duration and agent details?
- Age at exposure and at outcome assessment?
- Primary endpoint pre-specified?
- Confounders measured (syndrome, prematurity, socioeconomic status, hypoxia events)?
- Effect size clinically meaningful?
- Does it change emergency consent?
Using this checklist scores marks even when the paper is unfamiliar.
[1]Separation from adjacent paediatric myths
- ED thrashing is not proof of toxicity.
- Brief sevoflurane for hernia repair was developmentally similar to awake-regional in GAS.
- Multiple-exposure signals in MASK may reflect disease as much as drugs.
- Regional anaesthesia still involves systemic drug exposure and is not risk-free.
- Maintaining blood pressure, oxygen, glucose, and carbon dioxide is non-theoretical brain protection.
Timeline of the debate and how to teach it
Early animal work demonstrated that commonly used anaesthetic agents can trigger neuroapoptosis during vulnerable developmental windows, with later behavioural changes in some models. Media coverage and regulatory communication followed, creating parental fear that outpaced human outcome data. The field responded with smarter human studies rather than only more animal dose-finding.
[1]GAS provided randomised evidence for brief sevoflurane versus awake-regional in infant hernia repair and was reassuring at two and five years for primary cognitive endpoints. PANDA and MASK added observational breadth for single and multiple exposures, with MASK's secondary signals in multiply exposed children generating hypotheses rather than definitive proof of causation. SmartTots and professional societies promoted research funding and balanced messaging: necessary care proceeds; elective delay is sometimes reasonable; scare tactics are not.
[1]Teaching juniors should therefore emphasise three competencies. First, accurate citation of what each major study actually randomised or observed. Second, a counselling script that is empathetic and non-alarmist. Third, clinical humility about prolonged neonatal and cardiac anaesthesia where evidence remains incomplete. The candidate who can do all three will pass even if they forget a secondary endpoint detail, because examiners are testing judgement under uncertainty rather than pure memorisation of animal cascade diagrams.
[1] [1]Final synthesis for the night before the exam
Remember three study names and one counselling rule. GAS is the randomised brief sevoflurane versus awake-regional infant hernia trial, reassuring at two and five years for primary cognitive endpoints. PANDA is sibling-matched single exposure without global IQ difference. MASK is population data with preserved intelligence and secondary signals if multiple exposures that remain confounded. The counselling rule is necessity first, honesty about uncertainty for prolonged or repeated exposures, and no delay of indicated surgery. If you can deliver that package calmly under pressure, you have the topic.
[3] [1]One more viva drill
Question: "Would you refuse sevoflurane for all children under three?"
Answer: "No. GAS supports developmental equivalence of brief sevoflurane versus awake-regional for infant hernia repair on primary cognitive endpoints. I individualise technique for airway and surgery, avoid unnecessary prolonged deep anaesthesia, and never refuse indicated care because of theoretical risk alone."
Closing line
Necessary surgery proceeds; brief single exposures are the best-studied and most reassuring scenario; prolonged and repeated exposures remain uncertain; counselling is honest, calm, and free of both denial and panic.
[3] [1]References
- [1]Davidson AJ et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS). Lancet, 2016.PMID 26507180
- [2]McCann ME et al. Neurodevelopmental outcome at 5 years of age after general anaesthesia or awake-regional anaesthesia in infancy (GAS). Lancet, 2019.PMID 30782342
- [3]Sun LS et al. Association Between a Single General Anesthesia Exposure Before Age 36 Months and Neurocognitive Outcomes in Later Childhood (PANDA). JAMA, 2016.PMID 27272582
- [4]Warner DO et al. Neuropsychological and behavioral outcomes after exposure of young children to procedures requiring general anesthesia (MASK). Anesthesiology, 2018.PMID 29672337