Anaes · Cardiac anaesthesia
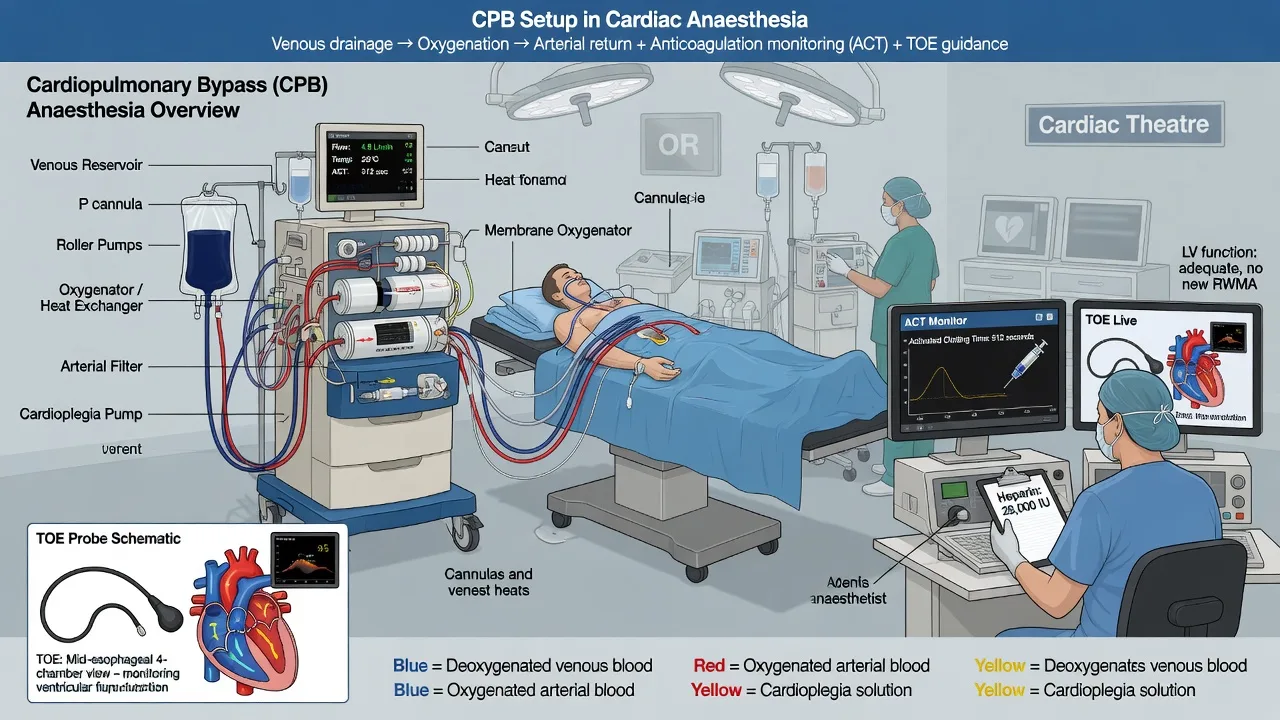
Cardiopulmonary bypass circuit: components, physiology, and anaesthetic priorities
Also known as CPB circuit · Cardiopulmonary bypass anaesthesia · Heart-lung machine
Ordered CPB circuit components, heparin and ACT targets, indexed flows and MAP, alpha-stat versus pH-stat, weaning with rate-rhythm-preload-afterload-contractility, protamine reactions, air embolism, and TRICS III transfusion context for ANZCA Final.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Why this is examined
Cardiopulmonary bypass is core SS_CS material. Examiners ask circuit order (rote pass filter), anticoagulation targets, indexed flows, temperature and blood-gas strategy, and weaning physiology. Classic crises are inability to wean, protamine reaction, and air embolism. TRICS III anchors the transfusion conversation around CPB-related anaemia.[1]
Circuit components in order (must be spoken without hesitation)
Venous to arterial pathway
Accessories examiners expect
- Cardiotomy suction (shed blood to reservoir — activates inflammation/coagulation)
- Cell saver (washed red cells)
- LV vent (prevents distension)
- Cardioplegia delivery line (antegrade/retrograde)
- Sampling manifold (ACT, ABG, electrolytes, Hb)
- Vacuum-assisted venous drainage (where used) — air entrainment risk if lines open
Pump types
Roller pumps are occlusive, deliver fixed stroke volume, and can generate high pressure against obstruction (line rupture/dissection risk if clamped). Centrifugal pumps are afterload-sensitive, less likely to blow lines, may be gentler on blood, but flow depends on preload/afterload and air handling differs. Modern membrane (hollow-fibre) oxygenators have replaced bubble oxygenators.
[1]Anticoagulation and reversal
Heparin before bypass
- Unfractionated heparin 300–400 IU/kg IV (institutional).
- Target ACT ≥400 s before full CPB; many units use ≥480 s.
- Confirm ACT after heparin and before initiating full bypass.
- Heparin resistance: check antithrombin III; may need ATIII concentrate/FFP and more heparin — do not start full CPB on a low ACT.
Protamine
Approximate 1 mg protamine per 100 IU heparin administered (titrate to ACT and bleeding), given slowly, preferably via a peripheral line, with surgical and anaesthetic readiness for reaction.[2]
Protamine reaction spectrum:
[2]- Transient systemic hypotension (histamine, rapid injection)
- Anaphylactoid/anaphylactic reaction
- Catastrophic pulmonary vasoconstriction with right ventricular failure
Management: stop protamine; 100% oxygen; support SVR and RV (inotropes/vasopressors; inhaled pulmonary vasodilators as available); re-heparinise and return to CPB if life-threatening and surgically agreed; treat as anaphylaxis pathway when indicated.
[2]Physiology on bypass
What changes
- Non-pulsatile (or attenuated) flow
- Haemodilution from crystalloid/colloid prime → lower haematocrit and viscosity
- Hypothermia for metabolic protection (degree procedure-dependent)
- Systemic inflammatory response from circuit contact, ischaemia–reperfusion, cardiotomy suction
- Altered drug pharmacokinetics (volume of distribution, sequestration)
Targets (exam numbers)
Flow is indexed to body surface area. MAP targets are individualised (chronic hypertension, carotid disease, age). Monitor urine output, serial ABG, ACT, potassium (cardioplegia), ionised calcium, haematocrit/haemoglobin, glucose, and TOE for de-airing and ventricular function.
[1]Alpha-stat versus pH-stat
- Alpha-stat: blood gases analysed at 37°C without temperature correction; tends to preserve autoregulation; common in adult CPB.
- pH-stat: temperature-corrected targets, often with CO2 addition; more used in deep hypothermic circulatory arrest and many congenital practices for cerebral vasodilation and more homogeneous cooling.
Know which strategy your unit uses for the case type and why.
[1]Myocardial protection (link, not full cardioplegia topic)
Cardioplegia (cold/warm, blood/crystalloid, antegrade/retrograde) achieves diastolic arrest and reduces myocardial oxygen demand. Communication with the surgeon about delivery route and redosing intervals matters when weaning fails from ischaemic injury.
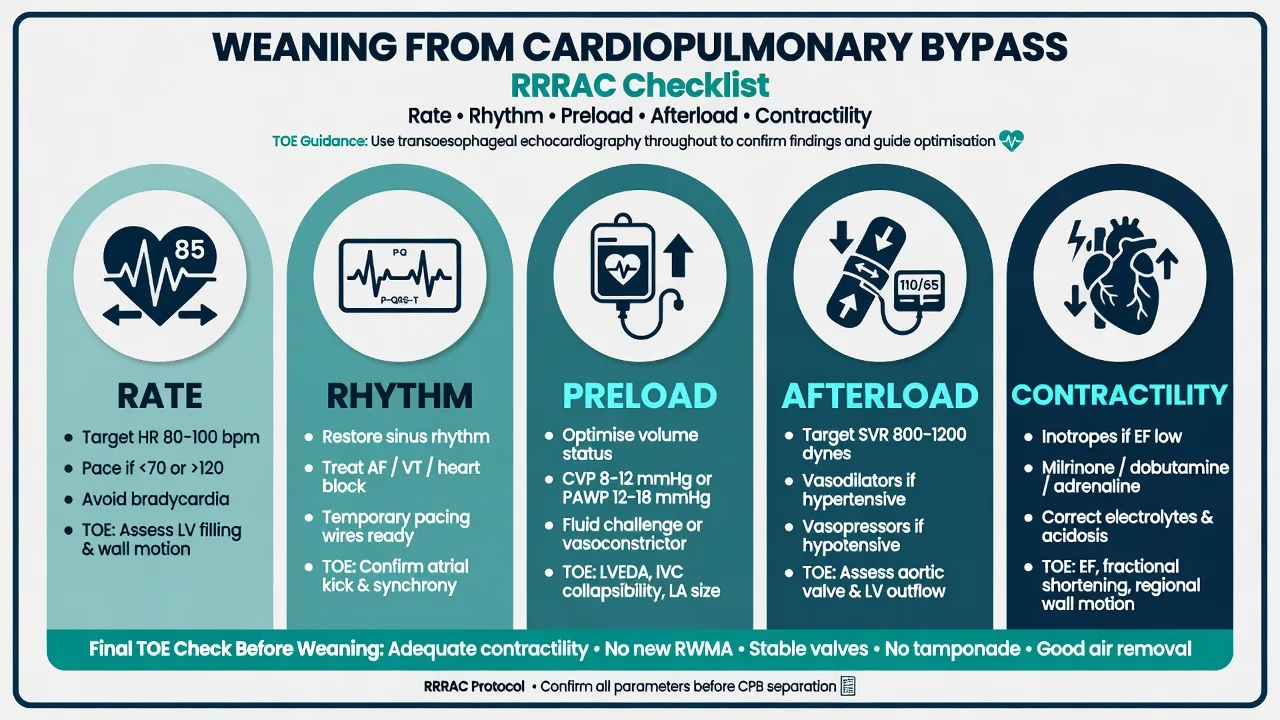
[2]Weaning from bypass — RRRAC
[1]Unable to wean — structured response
- Return to full support; rest the heart.
- Diagnose with TOE + surgical inspection + labs (Hb, K+, Ca2+, ABG, ACT).
- Escalate: inotrope/vasopressor optimisation, IABP, Impella, VA-ECMO as indicated.
- Revisit coronary graft integrity and valve function.
Transfusion on CPB — TRICS III
TRICS III showed a restrictive red-cell transfusion strategy was non-inferior to a liberal strategy for a composite outcome in moderate-to-high-risk adults undergoing cardiac surgery with CPB.[1] Exam phrasing: restrictive thresholds are reasonable in many adults, individualise for active bleeding, ischaemia, and institutional protocol — do not invent a single universal number without context.
Classic crises
Arterial and venous air on CPB
Prevention: de-airing routines, arterial filter, vigilance with open lines, careful cannulation. Management is team-based: stop entrainment, Trendelenburg when cerebral arterial air suspected, possible retrograde cerebral perfusion strategies with surgeon agreement, support and hyperoxia as adjuncts.
[1]Monitoring and TOE role
Standard cardiac: arterial line, central venous access, TOE (cannulation, venting, de-airing, weaning, valve assessment), ACT, urine, temperature (nasopharyngeal/bladder as per protocol), processed EEG/NIRS where used. TOE is the diagnostic spine of weaning failure.
[1]Special populations
- Paediatric/congenital CPB: different priming, temperature strategies, pH-stat more often in DHCA, size-specific cannulae — not adult arithmetic alone.
- Emergency redo sternotomy: massive haemorrhage readiness, external defibrillator pads, surgical femoral access plan.
SAQ answer scaffold
- Circuit order venous → arterial.
- Heparin dose, ACT threshold, protamine ratio and reaction types.[2]
- Indexed flow and MAP band.
- Alpha-stat vs pH-stat one-liners.
- Weaning RRRAC + unable-to-wean escalation.
- TRICS III restrictive non-inferiority one-liner.[1]
Viva stem bank
- “List the CPB circuit from venous cannula to aorta.”
- “ACT is 280 s after 400 IU/kg — what now?”
- “Patient will not wean — your systematic approach?”
- Model phrase: “I will not go on full bypass without a confirmed therapeutic ACT.”
Priming, haemodilution, and haematocrit
The circuit prime dilutes the patient’s blood volume. Paediatric primes are proportionally more significant. Strategies: miniaturised circuits, retrograde autologous priming in adults, colloid/crystalloid mix per perfusion protocol, and transfusion thresholds informed by TRICS III in appropriate adults.[1] On bypass, monitor haematocrit; extreme haemodilution reduces oxygen-carrying capacity and oncotic pressure.
Temperature management
- Mild hypothermia common for many adult CABG/valve cases
- Deeper hypothermia for complex aortic/DHCA work
- Rewarming rate matters (avoid excessive gradient); watch for vasodilation on rewarm
- Hyperthermia after CPB is harmful to the brain — do not overshoot
Conduct checklist (anaesthetist side)
- Pre-CPB: lines, TOE, heparin given, ACT confirmed, pumps ready, alarms set.
- Going on: head down slightly as agreed, ventilation paused when full flow established, inspect face for colour/symmetry (malperfusion clue).
- On CPB: anaesthetic depth via volatile in oxygenator gas or TIVA into circuit, paralysis, MAP/flow targets, urine, gases, ACT redosing with perfusionist.
- Preparing to wean: rewarm, correct labs, de-air, ventilation resumed, pacing available, inotropes running if needed, TOE survey.
- After CPB: protamine plan, bleeding check, ventilation and TOE reassess.
Communication phrases that score marks
- “ACT is therapeutic — happy to go on bypass.”
- “Line pressure is high — pause; exclude dissection/obstruction.”
- “RV is failing on TOE — reduce afterload on PA side, support contractility, consider returning to bypass.”
- “Stopping protamine — treating as reaction.”
Circuit order spoken script
“Venous cannula from the right atrium or bicaval cannulae drain to a venous reservoir, then to a roller or centrifugal pump, then through a membrane oxygenator with heat exchanger, then through an arterial line filter, then back via the arterial cannula usually in the ascending aorta.”
[1]Heparin resistance algorithm
Low ACT after standard heparin 300–400 IU/kg → give additional heparin → if still resistant, consider antithrombin III deficiency pathway (ATIII concentrate or FFP per protocol) → do not initiate full CPB until ACT therapeutic (≥400–480 s institutional target).
[1]Protamine reaction management detail
Stop protamine; 100% oxygen; support BP and RV; pulmonary vasodilators as available for catastrophic pulmonary hypertension; treat anaphylaxis pathway when indicated; discuss return to CPB if arresting; slow peripheral administration next time with test dose strategies per unit.[2]
Alpha-stat vs pH-stat table
| Alpha-stat | pH-stat | |
|---|---|---|
| Analysis | 37°C uncorrected | Temperature-corrected |
| CO2 | Not added to force correction | Often CO2 added |
| Autoregulation | Better preserved (adult teaching) | Cerebral vasodilation |
| Common use | Adult CPB | DHCA / many congenital practices |
Weaning RRRAC expanded
Rate: epicardial pacing if bradycardic.
Rhythm: defibrillate AF/VF as needed; sinus preferred.
Preload: volume from reservoir guided by TOE.
Afterload: vasopressors for vasoplegia; avoid extreme hypertension on suture lines.
Contractility: inotropes; fix Ca2+, K+, pH, ischaemia.
Unable to wean → full support → diagnose with TOE/surgery/labs → IABP/ECMO escalation.
[1]TRICS III one-liner with nuance
Restrictive red-cell transfusion was non-inferior to liberal in moderate-to-high-risk adults having cardiac surgery with CPB for the composite outcome studied; individualise for active bleeding and ischaemia.[1]
Inflammatory and coagulation effects of CPB
Contact activation, cardiotomy suction, ischaemia–reperfusion, hypothermia, and haemodilution drive coagulopathy and vasoplegia. Point-of-care viscoelastic testing guides targeted therapy in many centres. Cell salvage reduces allogeneic transfusion needs.
[1]Anaesthetist–perfusionist communication phrases
“ACT therapeutic — happy to go on.”
“Line pressure high — pause for dissection check.”
“Coming off — ventilation resumed, pacing on, noradrenaline running, TOE shows…”
“Stopping protamine — treating as reaction.”
Full conduct of bypass from the anaesthetic chair
Pre-bypass
Complete monitoring including arterial line and central access; TOE probe after induction when indicated; baseline ACT; antifibrinolytic per protocol; heparin 300–400 IU/kg; confirm ACT ≥400–480 s before full flow; communicate “happy to go on bypass.”
[1]Initiation
Head positioning as agreed; ventilation paused when full flow established; check face for colour symmetry (malperfusion clue); ensure adequate anaesthesia via oxygenator volatile or TIVA into circuit; paralysis; set MAP and flow targets with perfusionist.
Maintenance on CPB
Indexed flows about 2.2–2.5 L/min/m²; MAP commonly 50–80 mmHg individualised; urine output; serial ABG, ACT, K+, Ca2+, Hb/Hct, glucose; temperature strategy; cardioplegia communication; TOE for distension and air.
Separation
Rewarm without overshoot hyperthermia; correct labs; de-air with surgical manoeuvres and TOE; resume ventilation; pacing available; inotropes if needed; RRRAC optimisation; protamine after surgical request when stable, slowly, with reaction readiness.[2]
Pump failure and crisis extras
Massive air entrainment: stop entrainment, circuit management with perfusionist, surgical field control, support, cerebral protection strategies as indicated. Arterial dissection: high line pressure, asymmetric perfusion — immediate surgical emergency. Oxygenator failure: rare, catastrophic — emergency protocols with perfusion.
[1]Vasoplegia after CPB
Low SVR state with high or normal cardiac output after bypass. Treat with noradrenaline, add vasopressin, consider methylene blue or hydroxocobalamin in refractory cases per local protocol. Exclude residual issues (bleeding, tamponade, technical surgical problems) before labelling pure vasoplegia.
[1]Haematocrit and oxygen delivery on CPB
Haemodilution from prime lowers haematocrit; oxygen delivery depends on flow × content. TRICS III supports restrictive transfusion strategies in many adults undergoing CPB surgery without inferior composite outcomes versus liberal transfusion, with individualisation for bleeding and ischaemia.[1]
TOE views that matter on and off bypass
Cannula position concerns, aortic dissection flaps, ventricular filling and function, air in chambers, residual valvular lesions, SAM/LVOTO after mitral repair, tamponade after chest closure. Weaning failure without TOE is incomplete evaluation.
[1]Paediatric CPB differences (high-level)
Proportionally larger prime, temperature strategies including DHCA more often, pH-stat in many congenital DHCA pathways, size-specific cannulae, different haematocrit targets — do not export adult numbers uncritically.
[1]SAQ mark plan
Circuit order (3) · heparin/ACT/protamine (4) · flows/MAP (2) · alpha vs pH stat (2) · weaning RRRAC (3) · TRICS III (1) · crises (3).
[1]Common traps
Mixing venous and arterial ends; forgetting arterial filter; reverse protamine ratio errors; weaning only with inotropes while ignoring rhythm and preload; missing TOE findings; starting protamine as a rapid central bolus.
[2]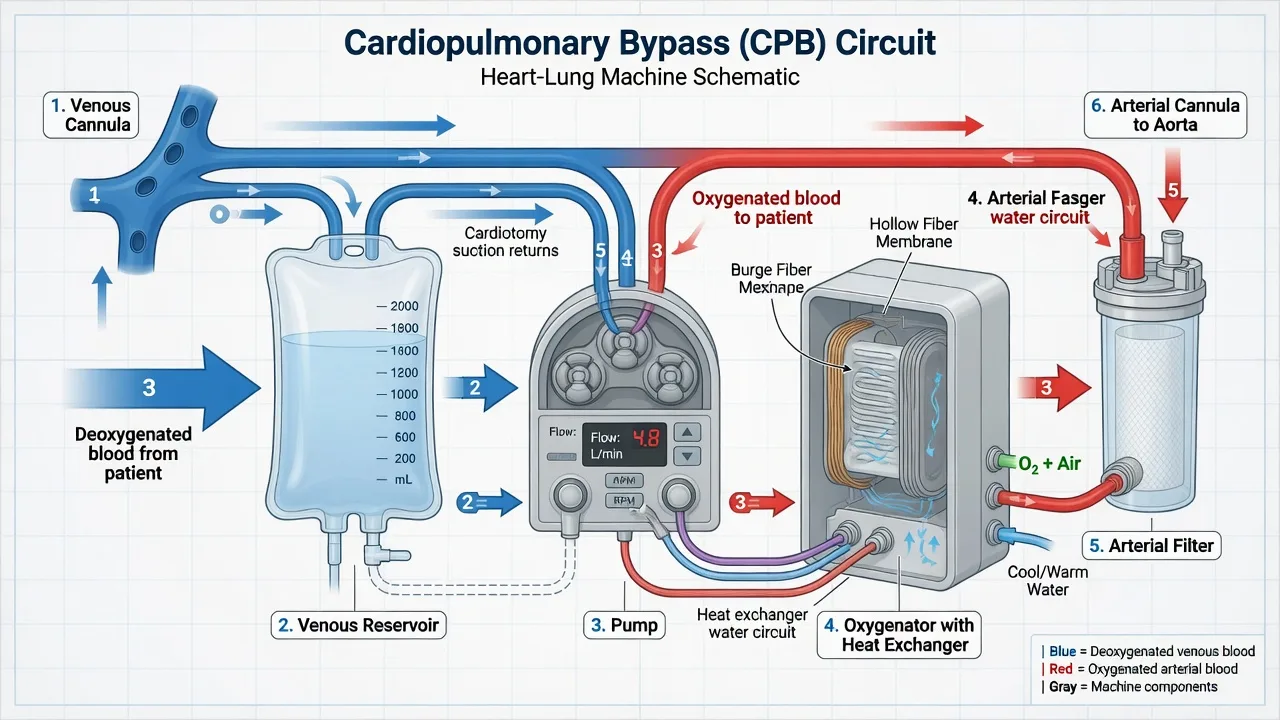
Fellowship consolidation — CPB circuit and conduct
[1]Speak the circuit without hesitation: venous cannula to venous reservoir to pump to oxygenator with heat exchanger to arterial filter to arterial cannula in the ascending aorta. Accessories include cardiotomy suction, cell saver, LV vent, cardioplegia lines, and sampling manifold. Roller pumps are occlusive and can generate high pressures against obstruction; centrifugal pumps are afterload sensitive.
[1]Anticoagulate with unfractionated heparin typically 300 to 400 IU/kg and confirm ACT of at least 400 to 480 seconds before full bypass. Heparin resistance may reflect antithrombin deficiency and needs ATIII concentrate or FFP pathways plus more heparin. Never initiate full CPB on a subtherapeutic ACT.
[1]Protamine dosing approximates 1 mg per 100 IU heparin administered, given slowly with readiness for hypotension, anaphylaxis, or catastrophic pulmonary vasoconstriction with right ventricular failure. Stop protamine, support the circulation and RV, treat anaphylaxis when indicated, and consider return to bypass for refractory collapse.
[2]On bypass, non-pulsatile flow, haemodilution, hypothermia, and inflammatory activation dominate physiology. Indexed flows are commonly about 2.2 to 2.5 L/min/m² with MAP often targeted around 50 to 80 mmHg and individualised for age and cerebrovascular disease. Alpha-stat is common in adult CPB; pH-stat is more often used in deep hypothermic circulatory arrest and many congenital practices.
[2]Wean using rate, rhythm, preload, afterload, and contractility guided by TOE. Unable to wean means return to full support, diagnose with TOE surgical inspection and labs, then escalate mechanical support if needed. TRICS III found restrictive red-cell transfusion non-inferior to liberal strategies for a composite outcome in moderate-to-high-risk adults having cardiac surgery with CPB, with individualisation for bleeding and ischaemia.
[1]Classic crises: air embolism, malperfusion or dissection with high line pressure, vasoplegia treated with noradrenaline and vasopressin, RV failure on weaning, and protamine reaction. Communication phrases that score include declaring therapeutic ACT before going on and stopping protamine immediately if reaction is suspected.
[2]Anaesthetist conduct checklist: lines and TOE ready, heparin given, ACT confirmed, anaesthesia maintained on bypass via oxygenator gas or circuit TIVA, rewarming without hyperthermic overshoot, de-airing, ventilation resumed, pacing available, then protamine after surgical request when stable.
[2] [1]Extended crisis table for revision
Inadequate ACT before bypass. Give more heparin; consider ATIII pathway; do not go on full bypass; recheck ACT.
[1]High arterial line pressure at initiation. Suspect malposition, clamp, or dissection; pause; surgical evaluation immediately; do not push flow against obstruction.
[1]Air in arterial line or heart chambers. Stop entrainment; circuit and field management with perfusion and surgery; TOE assessment; cerebral protection strategies as indicated; support.
[1]Failure to wean. Return to full CPB; optimise RRRAC; correct K+, Ca2+, pH, Hb; TOE for graft, valve, function, air, obstruction; escalate IABP or VA-ECMO.
[1]Protamine reaction. Stop drug; 100 percent oxygen; support SVR and RV; anaphylaxis treatment if indicated; consider reheparinisation and return to bypass if arresting.
[2]Vasoplegia. Noradrenaline, vasopressin, consider methylene blue per protocol after excluding technical and bleeding causes.
[1]Teaching conversation with a primary exam candidate
Primary exams may ask circuit order and basic physiology of non-pulsatile flow and haemodilution. Final exams add ACT numbers, protamine reactions, weaning structure, alpha-stat versus pH-stat, and TRICS III transfusion framing. Learn the circuit first; everything else hangs on that skeleton.
[1] [1]Temperature, prime, and inflammatory burden expanded
Temperature strategy ranges from mild hypothermia for many adult coronary and valve cases to deep hypothermia with circulatory arrest for complex aortic arch work. Rewarming gradients matter; excessive speed and overshoot hyperthermia are harmful to the brain. On bypass, the oxygenator heat exchanger is the temperature engine, but the anaesthetist still owns the decision band with the surgeon and perfusionist.
[1]Prime volume relative to patient blood volume is larger in small adults and massive in paediatrics, driving haemodilution, lower oncotic pressure, and transfusion decisions. Miniaturised circuits and retrograde autologous priming are adult strategies to limit dilution. Cell salvage returns washed red cells and reduces some inflammatory and coagulation load compared with unwashed cardiotomy suction, though both have roles.
[1]The inflammatory burden of CPB arises from blood-circuit contact, ischaemia-reperfusion, cardiotomy suction, and hypothermia. Clinically this appears as vasoplegia, capillary leak, coagulopathy, and multiorgan stress. Antifibrinolytics, gentle suction practices, and targeted blood product therapy using viscoelastic testing are modern mitigations. Understanding this biology explains why weaning is not only about the heart but about the whole inflammatory milieu created by the machine that just saved the patient's life.
[2] [1]Final synthesis and must-speak numbers
- Circuit order: venous cannula, reservoir, pump, oxygenator with heat exchanger, arterial filter, arterial cannula
- Heparin 300 to 400 IU/kg; ACT at least 400 to 480 seconds before full bypass
- Indexed flow about 2.2 to 2.5 L/min/m²; MAP commonly 50 to 80 mmHg individualised
- Protamine about 1 mg per 100 IU heparin, slow, reaction-ready
- Wean by rate, rhythm, preload, afterload, contractility with TOE
- Alpha-stat common in adult CPB; pH-stat more in DHCA and many congenital practices
- TRICS III: restrictive transfusion non-inferior to liberal in studied adult CPB population for the composite outcome
Say the circuit first. Confirm the ACT second. Wean with structure third. That order mirrors safe real-world conduct and safe viva conduct.
[1] [1]Additional viva drills
"ACT is 280 after 400 IU/kg heparin." Give more heparin, consider ATIII deficiency pathway, recheck ACT, and do not initiate full bypass until therapeutic.
[1]"Patient will not wean." Return to full support, optimise rate rhythm preload afterload contractility, correct electrolytes and haemoglobin, use TOE to find technical or functional problems, then escalate mechanical support if needed.
[1]"Protamine given and the right ventricle fails." Stop protamine, support RV and SVR, pulmonary vasodilators as available, treat as reaction, discuss return to bypass.
[2] [1]Closing line for CPB
Know the venous-to-arterial circuit order cold, never go on full bypass without a therapeutic ACT, wean with rate rhythm preload afterload and contractility under TOE guidance, and treat protamine as a drug that can kill as well as reverse heparin. Those four sentences are the spine of safe CPB anaesthesia and of a pass-level viva.
[2] [1]Extra examiner soundbites for CPB
"I will not go on full bypass without a confirmed therapeutic ACT."
"Flow is indexed to body surface area, commonly around 2.2 to 2.5 litres per minute per square metre."
"Protamine is approximately one milligram per one hundred international units of heparin and is given slowly with reaction readiness."
"Weaning uses rate, rhythm, preload, afterload, and contractility guided by TOE."
"TRICS III supports restrictive transfusion strategies in many adults having cardiac surgery with CPB, individualised for bleeding and ischaemia."
References
- [1]Mazer CD, Whitlock RP, Fergusson DA, et al. Restrictive or Liberal Red-Cell Transfusion for Cardiac Surgery (TRICS III). New England Journal of Medicine, 2017.PMID 29130845
- [2]Levy JH, Ghadimi K, Kizhakkedathu JN, Iba T What's fishy about protamine? Clinical use, adverse reactions, and potential alternatives. Journal of Thrombosis and Haemostasis, 2023.PMID 37062523