Anaes · Head & neck / ENT anaesthesia
Jet ventilation techniques: Sanders, HFJV, and barotrauma
Also known as Sanders injector · HFJV anaesthesia · Transtracheal jet ventilation
Manual Sanders and high-frequency jet ventilation for shared airway surgery, TIVA requirement, open expiratory pathway rule, barotrauma recognition, and transtracheal jet hazards.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Why this is examined / the one-line answer
Jet ventilation is classic SS_HN viva material because it fuses physics, shared-airway logistics, and a lethal crisis: barotrauma when high-pressure gas has no exit.[1] Examiners also test why TIVA is mandatory, differences between Sanders and HFJV, and why transtracheal jetting in CICO is dangerous without upper-airway egress (DAS culture).[2][3]
One-line opener: Open egress, TIVA, watch the chest fall — if it does not fall, I stop the jet.
[2]Preoperative assessment and risk stratification
Indications. Microlaryngoscopy, laser laryngeal work with tubeless field, tracheal stenosis interventions, selected shared-airway ENT cases where a standard ETT obstructs surgery.
[2]Contraindications / high-risk features. Complete upper-airway obstruction without planned egress, massive emphysema/bullae, uncontrolled asthma with high barotrauma risk, full stomach (gastric insufflation), inability to deliver TIVA reliably, lack of experienced operator or automatic cut-outs for HFJV, known difficult front-of-neck anatomy if rescue needed.
[2]Setup checklist. Working jet injector or HFJV machine, high-pressure oxygen source with known driving pressure limits, TIVA pumps (propofol ± remifentanil), difficult airway trolley, chest drains available for PTX, arterial line for prolonged cases, suction, surgical communication plan, laser fire precautions if laser used.
[3]Applied physics and physiology
Conventional positive-pressure ventilation delivers tidal volumes above dead space at low frequency. Jet ventilation delivers short high-velocity pulses:
[1]- Bulk flow of entrained and injected gas
- At high frequency: enhanced Taylor dispersion, coaxial flow, and other non-conventional gas exchange mechanisms
- Expiration is passive — the airway and chest wall must empty between pulses
If inspiration is driven but expiration is blocked (instrumentation, tumour, laryngoscope tip, packed glottis, closed cords), mean intrathoracic pressure rises → pneumothorax, pneumomediastinum, subcutaneous emphysema, haemodynamic collapse.[1]
Gastric insufflation occurs when jets are supra-glottic and the oesophagus shares the pressure field — raise the index of suspicion for regurgitation and abdominal distension.
[2]Techniques compared
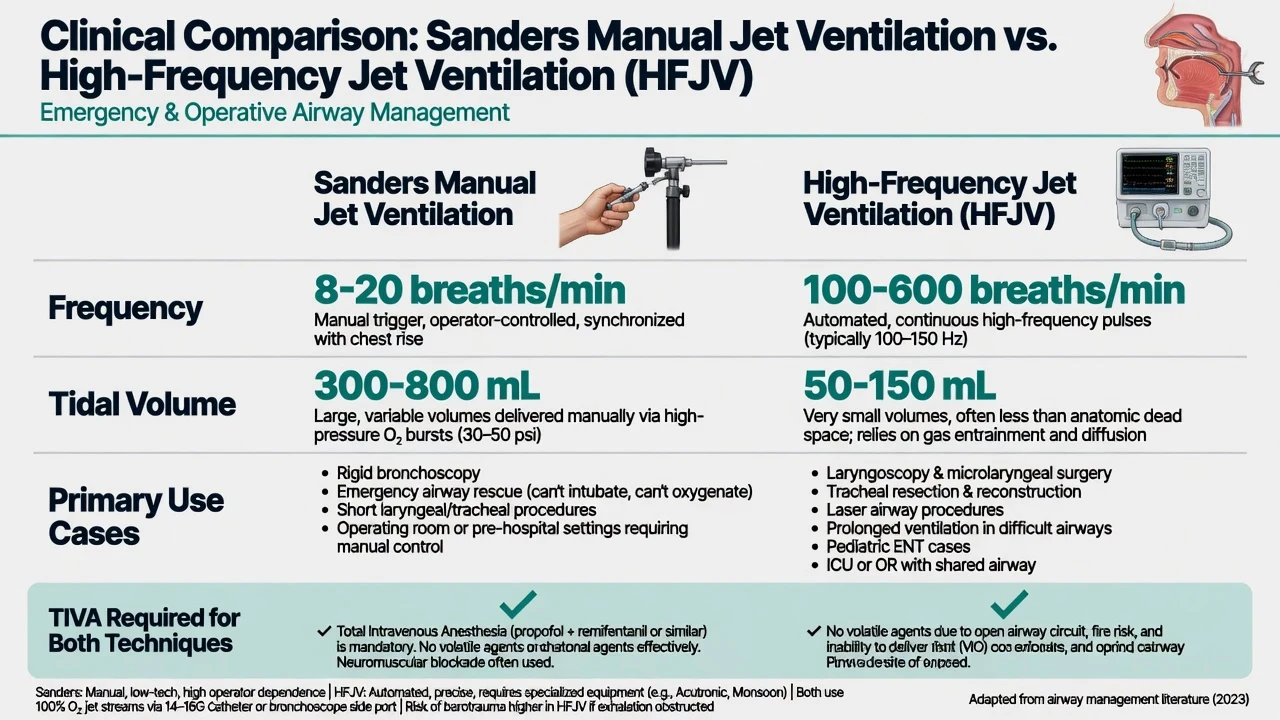
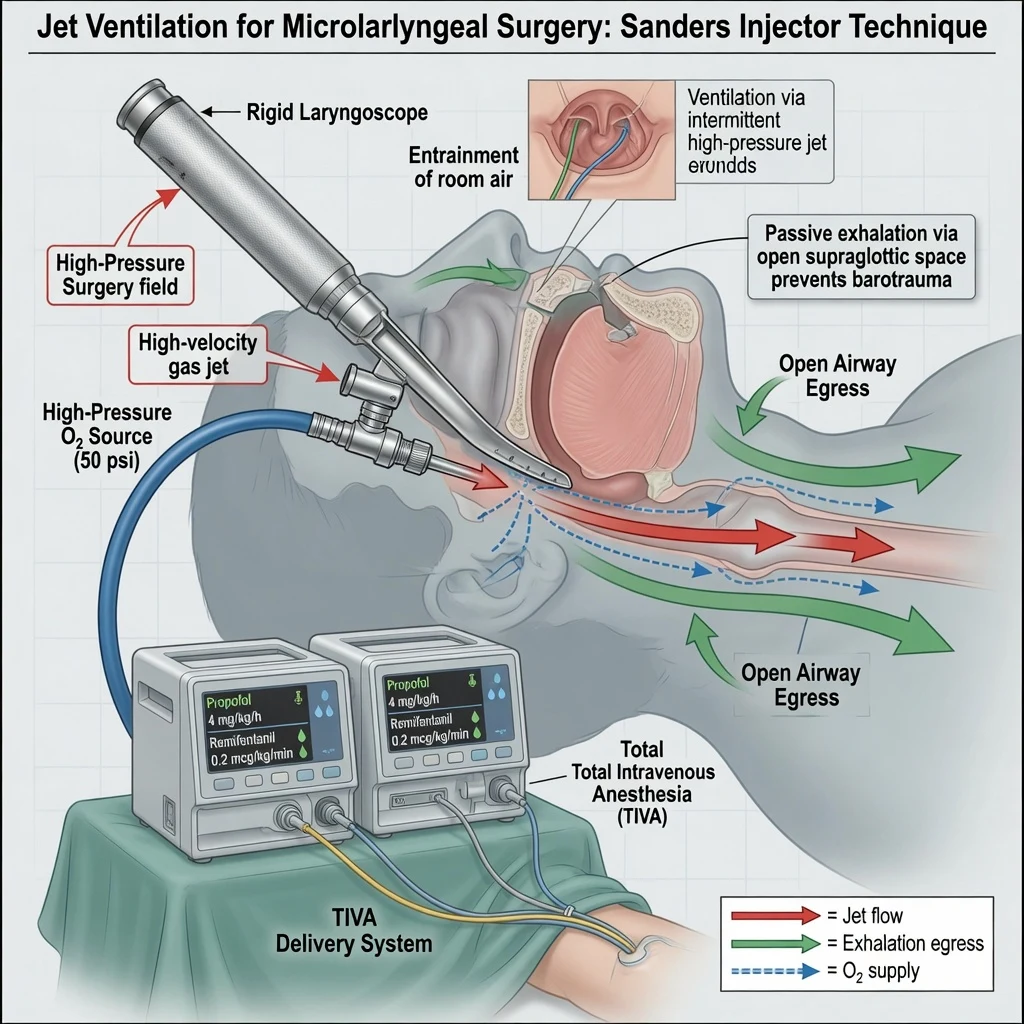
Sanders injector (classic equipment viva)
- High-pressure oxygen (pipeline or cylinder) via a hand-triggered injector
- Jet delivered through a side-port on a rigid laryngoscope or suspension system
- Operator controls rate and duty cycle by hand
- Simple, ubiquitous in ENT theatres, highly dependent on vigilance
HFJV
- Automated delivery at high frequency with set driving pressure, frequency, and inspiratory time percentage
- Better CO2 clearance for longer cases when set correctly
- Requires understanding of alarm systems and automatic shut-off for high airway pressure when available
- Still needs patent expiratory pathway
Transtracheal jet ventilation (TTJV)
Discussed historically for CICO. Modern DAS emphasis prioritises controlled front-of-neck access with a definitive plan for ventilation rather than unsupervised high-pressure jetting into a closed upper airway.[2] If jet is used below the glottis, upper airway must allow egress or a second pathway must exist.
Anaesthetic goals
- Maintain oxygenation and acceptable CO2 without barotrauma.
- Provide immobile surgical field with TIVA (not volatile-via-jet fantasy).
- Continuous two-way communication about airway openness.
- Immediate conversion plan to intubation, rigid bronchoscope ventilation, or surgical airway.
- Laser fire prevention if laser is concurrent (lowest safe oxygen, no N2O).
Rules of safe jetting (memorise)
- Exhalation pathway must be patent — never jet into a closed airway.
- TIVA (propofol–remifentanil typical) — volatiles are not reliably delivered; theatre pollution and awareness risk.
- Start with modest driving pressure; titrate to bilateral chest rise and fall.
- Limit I:E so expiration is adequate; avoid progressive stacking.
- Coordinate with surgeon: throat packs, instruments, and laser can obstruct egress.
- Full monitoring; arterial blood gas if prolonged; watch SpO2, chest excursion, haemodynamics.
- Automatic pressure cut-outs when available — never disable casually.
- Have a stop rule: no chest fall = stop jet.
Drug and technique practicalities
- Induction: standard IV induction with full preoxygenation when possible; for obstructing lesions, senior ENT and difficult airway plan first
- Maintenance TIVA: propofol effect-site or infusion titration; remifentanil for immobility and reflex suppression; consider depth monitoring adjuncts
- Muscle relaxation: often used for microlaryngoscopy; if used, ensure ventilation strategy is solid before paralysis
- Oxygen concentration: balance oxygenation needs against fire risk if laser; air/oxygen mix per setup
- Rescue drugs: adrenaline not first for barotrauma — stop jet and decompress; have muscle relaxant reversal or sugammadex if residual paralysis complicates recovery plans
Monitoring and equipment
- SpO2 continuous (primary early warning of failure)
- ECG, NIBP or arterial line for longer cases
- Capnography may be intermittent or unavailable in open systems — do not falsely reassure
- Visual and tactile chest assessment every few jets at start
- Peak/mean airway pressure displays on HFJV
- Ready needle decompression / chest drain equipment
- Suction for blood and debris that can block egress
Risks and complications
Jet hazards
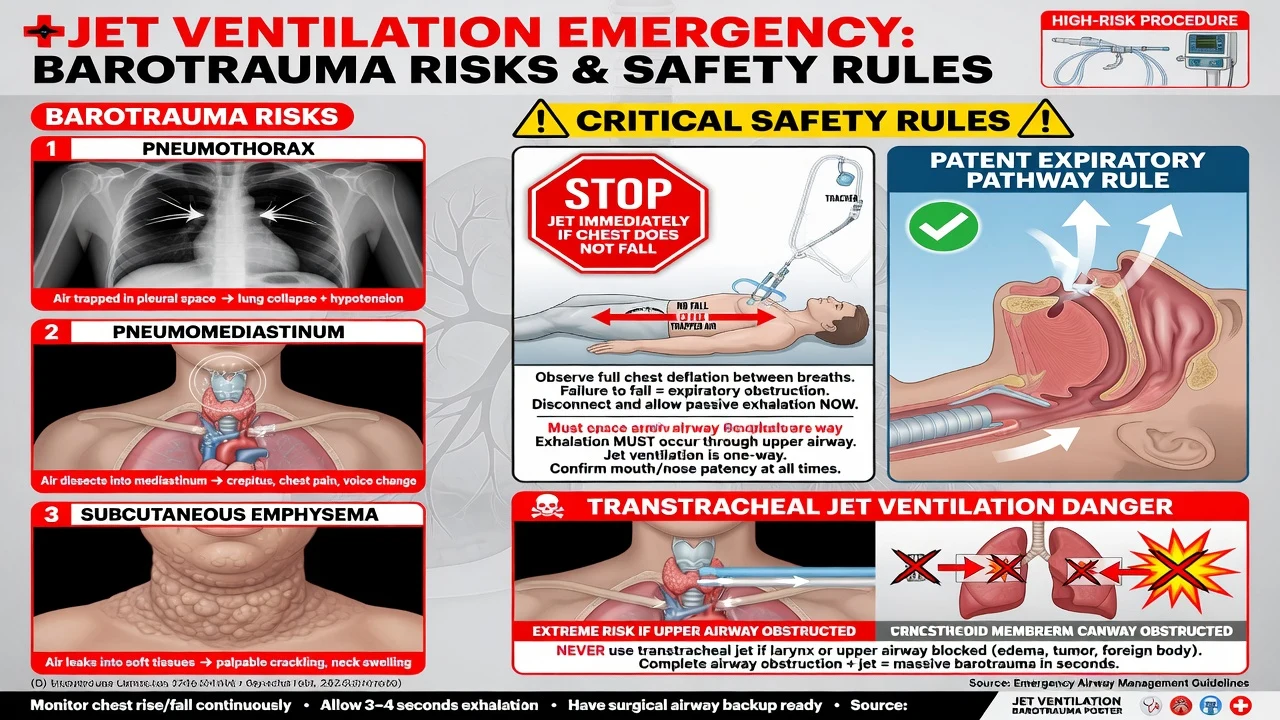
Barotrauma crisis script
- Stop jetting immediately.
- Disconnect high-pressure source; open the airway pathway.
- Assess: unequal chest, rising peak pressures history, surgical emphysema, hypotension, desaturation.
- Needle decompress / intercostal catheter for tension PTX.
- Convert to controlled ventilation strategy (intubation, rigid bronchoscope, surgical airway).
- Support circulation; exclude bilateral PTX if still unstable.
- Postoperative CXR and HDU observation even if stabilised.
Hypercarbia management: improve egress, reduce frequency or inspiratory time, optimise driving pressure carefully, intermittent intubation/ventilation breaks, ABG guidance.
[1]Crisis pivots — what changes the plan
- Chest rises but does not fall: stop, clear obstruction, discuss with surgeon
- Sudden cardiovascular collapse on jet: barotrauma until proven otherwise
- Laser case with jet: apply fire triad rules; oxidiser still present in jet gas
- CICO: prefer planned front-of-neck techniques with controlled ventilation strategy rather than blind high-pressure TTJV into a closed airway.[2]
- Suspected awareness: deepen TIVA, midazolam as indicated, frank postoperative discussion
NAP4 reinforces that head and neck airway crises demand experienced teams, capnography culture when a tube is present, and early definitive strategies.[3]
Postoperative plan
- Observe for delayed pneumothorax and subcutaneous emphysema
- Watch for hypercarbia residual effects (somnolence, hypertension)
- Airway oedema after laryngeal surgery — humidification, steroids per local practice
- PONV risk if gastric insufflation occurred
- Clear handover: jet mode used, any high-pressure alarms, ABG trends, chest findings
Special populations
- Paediatric jetting: smaller airways, faster stacking, specialist equipment and expertise
- Tracheal stenosis: jet may be used carefully distal/proximal to lesion depending on technique — egress still mandatory
- Obesity / restrictive chest: harder expiration, higher mean pressures
- Full stomach: high aspiration risk with supra-glottic jet — avoid if possible
SAQ answer scaffold
- Define jet ventilation and why expiration must be passive and patent.
- Sanders vs HFJV comparison table.
- Why TIVA is mandatory.
- Safe jetting rules and stop criteria.
- Barotrauma recognition and immediate management.[1]
- Transtracheal jet hazards within DAS CICO philosophy.[2]
Viva stem bank and model phrases
- “Explain how gas exchange occurs during HFJV.”
- “The chest is rising but not falling during Sanders ventilation.”
- “Why not use sevoflurane with jet ventilation?”
- “Is transtracheal jet your CICO plan?”
Model phrases:
[2]- “I will not jet without a visible expiratory pathway.”
- “Stopping the jet — this is stacking and barotrauma risk.”
- “TIVA is mandatory because I cannot reliably deliver volatile anaesthetic by jet.”
Common traps
- Jetting with laryngoscope tip obstructing the glottis
- Believing the vaporiser will anaesthetise the patient via jet
- Ignoring rising airway pressure alarms on HFJV
- Casual transtracheal jetting without egress
- Fixating on SpO2 while CO2 climbs for an hour
- No chest drain plan when using high driving pressures
- Laser fire prevention forgotten because “we are on jet, not a tube”
Driving pressure and frequency — practical teaching numbers
Exact machine settings are device-specific, but viva answers should show order-of-magnitude literacy:
[2]- Manual Sanders: short hand bursts watching chest; start conservatively with pipeline oxygen pressure regulated through the injector system rather than unrestricted wall pressure anecdotes
- HFJV frequency: often discussed in ranges from about 60–150 cycles/min or higher depending on device class and indication
- Inspiratory time percentage: keep low enough for expiration (e.g. 30–40% bands as teaching starting points — titrate)
- Driving pressure: start low and titrate to chest movement and gas exchange; never max the dial because SpO2 is 96%
Always defer to the specific HFJV manual on your unit and state that automatic pressure alarms must remain active.
[2]Gas exchange physiology in HFJV
At high frequency, tidal volumes may approach or fall near anatomic dead space; gas exchange relies on bulk flow of a fraction of gas plus enhanced diffusion, pendelluft, and coaxial streaming. Clinical implication: EtCO2 sampling is unreliable; use SpO2, ABG, and clinical chest movement. Rising PaCO2 is common and may be tolerated briefly, but progressive hypercarbia causes hypertension, arrhythmias, and awareness risk if depth is marginal — deepen TIVA and improve ventilation strategy.
[1]Supraglottic versus subglottic catheter jets
Supraglottic jets entrain air and risk gastric insufflation and less efficient delivery. Subglottic catheters improve delivery but can whip, injure mucosa, or obstruct if clotted with blood. Confirm position continuously; stop if surgical bleeding fills the field.
[2]Interaction with laser airway surgery
Jet gas is often oxygen-rich. Laser fire risk remains. Strategies: reduce oxygen fraction in jet gas if the system allows air/oxygen blending, intermittent laser with jet pauses, wet field discipline, and immediate fire algorithm readiness. Barotrauma plus fire is a dual-disaster stem examiners love.
[1]Conversion strategies when jet fails
- Stop jet; 100% oxygen by mask or rigid bronchoscope side-arm if available
- Intubate with microlaryngeal tube or standard ETT if surgery allows
- Surgical tracheostomy if upper airway impossible
- For tension PTX: decompress before endless airway attempts if chest is the cause of arrest
Paediatric and stenosis notes
Children desaturate faster; stacking is easier; only experienced teams should jet. In tracheal stenosis, jetting proximal to a critical stenosis without distal egress is particularly hazardous — discuss with interventional pulmonology/ENT before induction.
[2]Awareness prevention checklist for TIVA jet cases
- Working two pumps or backup syringe
- Visible IV site or central access reliability
- Processed EEG adjunct if available
- Avoid pump silence alarms ignored
- Midazolam co-induction optional per practice
- Postoperative explicit questioning if instability occurred
Equipment viva: Sanders injector components
High-pressure oxygen source → pressure regulator / injector body → hand trigger → delivery needle or side-port connection on the laryngoscope → patient airway. Entrainment of room air occurs around the jet stream (Venturi-like behaviour), so delivered FiO2 may be less than 1.0 even with oxygen pipeline supply — still enough oxidiser for laser fire risk. Never connect an unrestricted high-pressure hose to a tracheal catheter without a purpose-designed system and exhaust path. [1]
HFJV machine parameters to name
- Driving pressure
- Frequency
- Inspiratory time %
- Pause / I:E relationships
- Gas composition (O2/air blender if available)
- Alarm and cut-off for high pressure / obstruction [1]
If the machine alarms high pressure repeatedly: stop, clear airway, do not silence and continue. [1]
Hypercarbia versus hypoxia patterns
Hypoxia: immediate stop-and-fix (obstruction, PTX, circuit failure, severe shunt).
Hypercarbia: may develop gradually; improve egress, reduce frequency or inspiratory fraction, increase driving pressure carefully, intermittent conventional ventilation breaks, check for fatigue of manual operator in long Sanders cases. [1]
Gastric distension management
Suspect when abdomen rises, regurgitation, high airway pressures without chest movement. Stop jet, decompress stomach with OG tube when possible, protect airway from aspiration, convert technique. [1]
CICO and jet — modern framing
DAS 2015 emphasises scalpel–bougie–tube front-of-neck access for CICO in adults as a canonical pathway, with oxygen delivery strategies that do not rely on unsupervised high-pressure jetting into a completely obstructed upper airway.[2] If a narrow-bore cannula technique is used in some regions historically, the examiner wants insight into barotrauma risk and the need for upper airway patency or controlled expiration. NAP4 showed real-world harm when airway rescue is delayed or unstructured.[3]
Combined laser + jet case plan
TIVA; eye protection; lowest safe oxygen in jet gas; wet field; jet pause during laser if needed; fire algorithm posted mentally; chest rise/fall every burst; ABG at 30–60 minutes in long cases; convert to tube if gas exchange or safety fails. [1]
Postoperative imaging
Any suspicion of barotrauma: urgent CXR; assess for PTX, pneumomediastinum, subcutaneous emphysema. Even “resolved” intraoperative emphysema deserves observation. [1]
Teaching analogy
Jet ventilation is like inflating a balloon through a straw: easy to put gas in, disaster if the neck of the balloon is pinched while you keep blowing. [1]
Indications ranked by exam frequency
- Microlaryngoscopy / phonosurgery shared airway
- Laser laryngeal surgery tubeless field
- Selected tracheal interventions
- Historical/limited role in CICO oxygen delivery debates [1]
Contraindications ranked
- Complete airway obstruction without egress
- Untrained operator / missing equipment
- Active severe bullous disease high PTX risk (relative)
- Inability to provide TIVA safely
- Uncontrolled full stomach when supraglottic jet likely (relative) [1]
Monitoring when EtCO2 is unavailable
SpO2, chest wall movement, invasive arterial blood pressure for long cases, serial ABG, surgical field colour, pupil/haemodynamic signs of hypercarbia (hypertension, tachycardia, arrhythmias). Do not pretend open-system jet has reliable continuous capnography. [1]
Manual Sanders fatigue
Long cases tire the operator; irregular jetting worsens hypercarbia. Swap operators, convert to HFJV if available, or place a tube for periods of surgery that allow it. [1]
Barotrauma radiographic and clinical signs
Subcutaneous emphysema of neck/chest, rising airway pressures before collapse, unequal air entry, tracheal deviation late, desaturation, obstructive shock pattern. Treat tension physiology immediately. [1]
Integration with shared airway fire topic
Cross-link mentally: jet cases still obey fire triad if laser is used; TIVA still mandatory; egress still mandatory. Dual-topic stems are common in Final. [1]
Numbers / facts card
| Fact | Answer |
|---|---|
| Anaesthetic | TIVA mandatory |
| Critical safety | Open expiratory path |
| Classic manual system | Sanders |
| Top crisis | Barotrauma / PTX |
| Stop rule | No chest fall |
| CICO philosophy | DAS controlled FONA; caution TTJV |
Final line
“Jet ventilation is safe only when gas can leave as easily as it enters.” [1]
Worked hypercarbia stem
After 40 minutes of Sanders jetting for laser cord surgery, ABG shows PaCO2 75 mmHg, pH 7.18, SpO2 96%. Actions: inform surgeon, improve egress, reduce obstruction from scope, consider lowering frequency/inspiratory time if on HFJV, deepen TIVA to prevent awareness during hypercarbia stress, take ventilation breaks with intubation if surgery allows, rule out PTX if pressures odd, plan shorter remaining surgical time or convert technique. Do not ignore progressive respiratory acidosis because SpO2 looks acceptable. [1]
Entrainment and delivered oxygen
The jet entrains ambient air, so alveolar oxygen fraction is not simply the pipeline oxygen fraction. Still treat laser risk seriously. If air/oxygen blending is available on HFJV, use it to lower oxidiser when laser is active and SpO2 allows. [1]
Training requirements
Only operators familiar with the specific injector/HFJV device should run jet lists. Anaesthetic assistants should know the stop-jet command and PTX drill. New trainees start with short elective microlaryngoscopy under direct supervision. [1]
Cross-reference doses for TIVA immobility
Remifentanil often 0.1–0.5 microg/kg/min with propofol TCI or infusion sufficient for microlaryngoscopy; titrate to movement and haemodynamics. Have a backup propofol syringe. Muscle relaxation if used must not replace the need for patent egress and careful jetting. [1]
One-line physics closer
Expiration is passive; if the chest does not fall, high-pressure gas is accumulating and barotrauma is imminent — stop the jet before cardiovascular collapse declares the diagnosis for you. [1]
[2] [2]References
- [1]Clevenger FW et al. Barotrauma associated with high-frequency jet ventilation for hypoxic salvage Arch Surg, 1990.PMID 2244805
- [2]Frerk C et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults Br J Anaesth, 2015.PMID 26556848
- [3]Cook TM et al. Major complications of airway management in the UK: results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: anaesthesia Br J Anaesth, 2011.PMID 21447488