Anaes · Obstetric anaesthesia
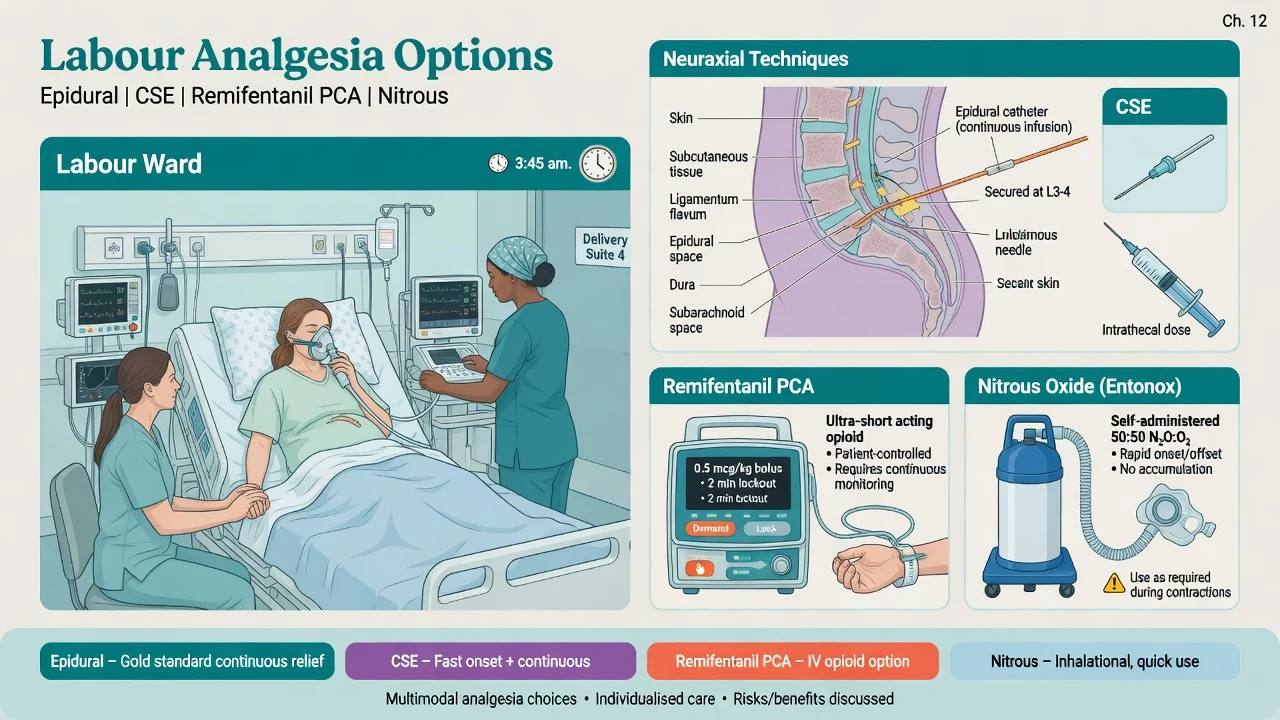
Labour analgesia: epidural, CSE, and non-neuraxial alternatives
Also known as Labour epidural · Combined spinal epidural labour · COMET trial mobile epidural · Remifentanil PCA labour
Fellowship coverage of labour neuraxial analgesia: consent, epidural and CSE technique, low-dose mobile solutions, COMET trial findings, PCEA, breakthrough pain, complications, and alternatives including remifentanil PCA and nitrous oxide.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Why this is examined / the one-line answer
Labour analgesia is the bread-and-butter of obstetric anaesthesia on the ANZCA Final Examination and equivalent boards. The examiner wants a consultant who can consent clearly, place a low-dose mobile epidural or CSE, programme maintenance, troubleshoot breakthrough pain, convert to surgical anaesthesia for caesarean, and manage complications including hypotension, high block, post-dural puncture headache, and local anaesthetic systemic toxicity — then offer a safe non-neuraxial alternative when neuraxial is impossible.
[1]The one-line answer: I offer a low-dose mobile epidural or CSE after excluding contraindications, maintain with dilute local anaesthetic–opioid mixture via PCEA or programmed intermittent bolus, treat breakthrough by examining the catheter not by endless blind boluses, top up only a working epidural for theatre, and if neuraxial is refused I run remifentanil PCA with continuous monitoring or offer nitrous oxide as a lesser alternative.
[1]COMET remains the named trial that moved practice from dense traditional epidurals toward low-dose ambulatory techniques with less instrumental delivery.[1] OAA/DAS sits in the background whenever conversion to general anaesthesia is contemplated.[4]
Consent — what you must say out loud
Benefits: best quality analgesia available for labour; reduced maternal catecholamine surge (relevant in cardiac and hypertensive disease); ability to extend the block for instrumental delivery or caesarean without inducing general anaesthesia; option for patient-controlled boluses.
[2]Risks (frequency framing for viva):
- Failure or partial block (common enough that you promise management, not perfection).
- Hypotension from sympathectomy — treated with position, fluids, vasopressors.
- Post-dural puncture headache after accidental (or intentional CSE) dural puncture — usually self-limiting or treatable with epidural blood patch.
- Temporary motor weakness; modern low-dose mixtures aim for mobility.
- Rare: nerve injury, epidural haematoma, epidural abscess, high or total spinal, LAST.
- Historical association of dense epidurals with instrumental delivery — mitigated by low-dose mobile techniques (COMET).[1]
- Effect on labour duration is modest with modern solutions; second stage may be slightly longer in some series — discuss without scaremongering.
Alternatives: nitrous oxide/oxygen, systemic opioids, remifentanil PCA, non-pharmacological support, no pharmacological analgesia.
[2]Decision capacity: labour pain does not remove capacity, but information must be clear and timely. Antenatal education helps; on-demand consent on the labour ward is still valid if coherent.
[2]Contraindications and pre-procedure checks
Hard (until corrected): patient refusal; uncorrected coagulopathy; infection at the needle site; raised intracranial pressure from mass lesion; uncorrected severe hypovolaemia.
[4]Relative / individualise: progressive neurological disease, some spinal abnormalities or previous spinal surgery, systemic sepsis without treatment and source control, significant aortic stenosis or other lesions where afterload reduction is dangerous (still often use carefully titrated epidural rather than single-shot spinal — lesion-specific), thrombocytopenia thresholds per unit (many units are cautious below 70–80 × 10⁹/L for elective epidural; higher concern in rapidly falling PET/HELLP counts).
[1]Checks before needle: recent platelet count when pre-eclampsia, HELLP, abruption, or idiopathic thrombocytopenic purpura risk exists; anticoagulation timing per ASRA/ANZCA-style regional guidelines used by the unit; intravenous access; blood pressure baseline; CTG review with midwifery/obstetrics; allergy and previous epidural history; airway assessment in case of high block or conversion to GA.
[4]Maternal physiology interface (why low-dose works and why position matters)
Pregnancy engorges epidural veins, reduces lumbar CSF volume, and increases neuraxial sensitivity — a given milligram dose spreads further than in non-pregnant adults. Aortocaval compression worsens after sympathectomy: maintain left lateral tilt or uterine displacement when supine. Rapid desaturation physiology matters if you convert to general anaesthesia for failed block at category-1 caesarean.[4]
Epidural technique for labour — step by step
- Position: sitting (easier midline, better for obesity) or lateral (may reduce orthostatic symptoms).
- Asepsis: full sterile precautions; chlorhexidine carefully dried (neurotoxicity concern if wet into CSF).
- Level: L3/4 or L4/5 common; iliac crest (Tuffier) approximates L4.
- Loss of resistance: saline preferred by many (less pneumocephalus risk than air); air still used by some — know both for viva.
- Catheter: thread 3–5 cm into the epidural space; note depth at skin; secure meticulously (dislodgement is a leading cause of “failed epidural”).
- Aspiration: for blood or CSF; if frank blood, withdraw and resite; if CSF, manage as dural puncture (see complications).
- Test dose culture: units vary. Classic adrenaline-containing lidocaine test dose looks for intravascular tachycardia; many obstetric units use a small fraction of the low-dose mixture with careful observation for high block instead. State your unit practice and the physiological logic.
- Loading dose: dilute local anaesthetic plus lipophilic opioid. Example teaching ranges (always follow local protocol): bupivacaine 0.0625–0.1% or levobupivacaine/ropivacaine dilute mixtures with fentanyl 2 microg/mL (or equivalent), given in fractionated boluses to a total loading volume often 10–20 mL depending on recipe.
- Maintenance: PCEA ± low background infusion, or programmed intermittent epidural bolus (PIEB) plus PCEA — PIEB may improve distribution and reduce local anaesthetic consumption versus continuous infusion alone.
- Review: block height, bilateral sacral coverage, modified Bromage motor score, maternal observations, CTG, and catheter depth after every significant intervention.
CSE for labour
Spinal component (example teaching doses — unit protocol rules): low-dose intrathecal bupivacaine 1–2.5 mg plus fentanyl 10–25 microg (or sufentanil in some systems) for rapid sacral and early labour relief, then epidural catheter for maintenance.
[1]Advantages: fastest onset; excellent sacral block for advanced labour or multiparous women with rapid progress; can reduce initial epidural failure from malpositioned catheters by proving neuraxial access.
[2]Disadvantages / risks: intentional dural puncture (PDPH risk, though small-gauge pencil-point needles keep rates low); high or total spinal if epidural doses are given as if no spinal drug were present or if large volumes are pushed into a catheter that is actually intrathecal; delayed confirmation of epidural catheter function until spinal component recedes; theoretical fetal bradycardia after intrathecal opioid (usually transient).
[1]COMET trial — the named evidence
COMET (Comparative Obstetric Mobile Epidural Trial) compared traditional higher-concentration epidural techniques with low-dose “mobile” techniques (low-dose CSE and low-dose infusion). Low-dose mobile techniques reduced instrumental vaginal delivery compared with traditional epidural, supporting modern dilute ambulatory-style labour analgesia as the default teaching standard.[1] Quote the one-liner in viva; do not invent secondary endpoints you cannot defend.

PCEA and PIEB programming principles
- Demand bolus: patient control improves satisfaction and allows titration to contraction pain.
- Lockout interval: prevents dangerous stacking (typical teaching order 10–20 minutes depending on bolus size — use unit pump card).
- Background infusion vs PIEB: continuous low background is traditional; programmed intermittent boluses may improve spread.
- Hourly maximum: hard stop for safety.
- Audit the button: high demand count means inadequate block, advanced labour, or dystocia — examine the patient and catheter, do not blame the woman.
- Drug choice: dilute long-acting amide plus lipophilic opioid remains standard; avoid dense 0.25–0.5% bupivacaine infusions as routine labour maintenance.
Breakthrough pain algorithm
- Review clinical context: stage of labour, oxytocin use, occiput posterior, full bladder, impending second stage, or obstructed labour.
- Examine the block: sensory level left and right, sacral segments (S2–4), motor score, patchy or unilateral pattern.
- Inspect the catheter: depth at skin versus documented depth; wet dressings; disconnection; pump programming errors.
- Position: lateral to the poorly blocked side; withdraw catheter 0.5–1 cm if unilateral and multi-orifice catheter is deep.
- Manual bolus of low-dose mixture; reassess in 10–15 minutes with continuous maternal observations.
- If primary failure: resite epidural or convert to CSE rather than pouring volume into a wrong space.
- Communicate with obstetrics: breakthrough plus poor progress may signal need for theatre planning, not only more local anaesthetic.

FAILED epidural check
Conversion to anaesthesia for caesarean section
This is where labour epidurals earn their keep — and where they kill time if mismanaged.
[2]Category 2–3 caesarean with a working epidural: top up early with a surgical mixture (examples used in teaching: lidocaine 2% with adrenaline ± bicarbonate and fentanyl, or higher-concentration ropivacaine/levobupivacaine per unit protocol) aiming for bilateral T4 surgical anaesthesia, dense sacral block, and no pain on testing. Fractionate doses; prepare vasopressors; maintain left tilt; convert the labour analgesic into a surgical anaesthetic deliberately.
[1]Category-1 caesarean: if the epidural has not been assessed as dense and bilateral to a surgical level, do not gamble serial top-ups while the fetus is crashing. Prepare for rapid sequence general anaesthesia with OAA/DAS failed intubation planning, or perform a rapid single-shot spinal only if time, coagulation, and airway risk truly favour it and the team agrees.[4] A weak labour epidural is not a secured airway.
Vasopressors: phenylephrine strategies from spinal caesarean evidence inform top-up hypotension management; treat early.[3]
Failed top-up in theatre: declare failure, convert to GA or spinal (with caution if large epidural volumes already given — high block risk) according to urgency and residual block.
[4]Complications — recognition and first actions
| Problem | Immediate actions |
|---|---|
| Hypotension | Left tilt / uterine displacement, IV fluid, phenylephrine or ephedrine, call help if severe |
| High / total spinal | Call help, airway support, intubate if inadequate ventilation or consciousness lost, 100% oxygen, vasopressors/adrenaline as needed, left tilt, deliver if indicated, ICU pathway |
| Accidental dural puncture | Stop, do not inject large LA volume, options: thread intrathecal catheter (unit policy) or resite epidural at another level; counsel re PDPH; label clearly |
| PDPH | Supine comfort, hydration, simple analgesia, caffeine as adjunct; epidural blood patch if disabling (classically 15–20 mL autologous blood, sterile, experienced operator) |
| LAST | Stop injection, ABC, seizure control with benzodiazepine, 20% lipid emulsion (ASRA: 1.5 mL/kg bolus then infusion — know your local card), avoid pure lidocaine for arrhythmias as first thought |
| Epidural haematoma | Rare; evolving motor block after block should be wearing off is a red flag — urgent MRI and surgical decompression pathway |
| Infection / abscess | Fever, back pain, evolving neurology — imaging and neurosurgical review |
| Failure | Early honest recognition; resite or alternative plan |
Non-neuraxial alternatives
Nitrous oxide / oxygen (Entonox 50:50)
Rapid onset and offset; useful early labour or as bridge; incomplete analgesia for many; nausea, drowsiness, environmental exposure concerns; not a substitute for neuraxial when severe pain or operative delivery is likely.
Remifentanil PCA
The principal alternative when neuraxial is contraindicated or refused. Ultra-short-acting mu-agonist; patient-controlled bolus timed to contractions. Mandatory safety system: one-to-one midwifery, continuous pulse oximetry, clear PCA protocol, supplemental oxygen as indicated, readiness to support ventilation, and strict prohibition of proxy bolusing by family. RemiPCA SAFE Network audit data support structured safety systems rather than ad hoc use.[2] Neonatal and maternal respiratory depression remain real — this is monitored care, not a “natural” option.
Systemic opioids
Pethidine, morphine, diamorphine, or fentanyl protocols vary by region. Limited efficacy in late labour; maternal sedation; neonatal respiratory depression and impaired breastfeeding initiation — know your jurisdiction’s preferred agent and why many units have moved away from routine intramuscular pethidine.
Non-pharmacological
Continuous support, water immersion, TENS, positioning — adjuncts that improve experience; rarely sufficient alone for modern nulliparous labour expectations, but respect maternal choice.
Monitoring standards
- Maternal blood pressure, heart rate, and consciousness after every bolus and at protocol intervals.
- Continuous CTG as obstetric protocol (note that fetal heart rate changes after CSE opioid are usually transient but must be communicated).
- Sensory level and modified Bromage motor score.
- For remifentanil: continuous SpO2 and dedicated observation without exception.[2]
- After accidental dural puncture or large top-ups: heightened surveillance for high block.
Special clinical contexts
- Trial of scar / previous caesarean: epidural useful for labour and rapid extension if scar rupture concerns arise — still needs obstetric vigilance.
- Pre-eclampsia: epidural can help blood pressure control by reducing pain; check platelets and coagulation; avoid excess fluid; prepare for higher airway risk if GA needed.
- Cardiac disease: early epidural often preferred to blunt catecholamine surges; titrate carefully; arterial line in severe lesions; multidisciplinary plan.
- Obesity: sitting position, longer needles, ultrasound if available, higher failure risk, harder airway if conversion needed — place early.
- Anticoagulated patients: follow regional anaesthesia timing guidelines; do not improvise.
- Sepsis / chorioamnionitis: individualise; untreated systemic sepsis is a concern for neuraxial infection risk.
Regional notes
ANZ / UK: low-dose mobile epidural or CSE is standard teaching; COMET is expected by name; remifentanil PCA requires formal monitoring protocols; OAA resources widely used.
US / Canada: CSE and dilute PCEA common; lipid emulsion and ASRA LAST checklist standard; institutional obstetric anaesthesia guidelines.
India / resource-variable: same pharmacological principles; Entonox and remifentanil availability vary; denser solutions still appear where pumps and dilute premixes are limited — examiners still prefer the low-dose safety message when asked for ideal practice.
SAQ answer scaffold
- Consent: benefits, risks, alternatives.
- Contraindications and pre-epidural checks (platelets, anticoagulation).
- Low-dose epidural recipe and PCEA/PIEB principles.
- CSE: doses, pros/cons.
- COMET one-liner and practice implication.
- Breakthrough pain algorithm.
- Conversion to caesarean anaesthesia by urgency category.
- Remifentanil PCA safety requirements.
- Management of high spinal and LAST.
Viva stem bank with model outlines
Stem 1: “This primip is 4 cm and requests an epidural — consent her.”
Outline: benefits (best analgesia, theatre extension), risks (failure, hypotension, PDPH, rare serious harm), motor block usually mild with low-dose, COMET context for instrumental delivery, alternatives, answer questions, document.
Stem 2: “Why low-dose mobile techniques?”
Outline: COMET — reduced instrumental delivery vs traditional higher-dose epidural; better mobility; similar or better analgesia with modern PCEA; dense motor block is outdated as default.[1]
Stem 3: “Unilateral block at 8 cm — your steps?”
Outline: examine catheter depth, pull back 1 cm if deep, lateral position to weak side, bolus, reassess; if fails resite or CSE; exclude full bladder and OP position; do not promise perfection.
Stem 4: “Neuraxial refused — run remifentanil PCA safely.”
Outline: protocolised bolus/lockout, 1:1 midwife, continuous SpO2, no proxy boluses, oxygen and airway support ready, convert plan if operative delivery needed.[2]
Stem 5: “Category-1 caesarean, labour epidural in situ, last top-up two hours ago, block patchy to T10.”
Outline: this is not a surgical epidural; prepare GA with OAA/DAS plan; do not waste time on hopeful top-ups unless block rapidly densifies and obstetrician agrees seconds matter less than airway risk — usually GA.[4]
Stem 6: “Immediate headache and clear fluid from the needle.”
Outline: recognise wet tap; options intrathecal catheter vs resite; label; counsel PDPH; if catheter used as spinal, only spinal doses; observe for high block.
Common traps
- Running dense 0.25–0.5% bupivacaine as routine labour maintenance.
- Endless top-ups for category-1 caesarean with a weak epidural.
- Ignoring high PCEA demand counts.
- Remifentanil without continuous oximetry and dedicated observation.
- Forgetting lipid emulsion location when topping up.
- Not labelling an intrathecal catheter after wet tap.
- Promising zero motor block or zero PDPH risk.
Examiner mental map — fifteen dimensions
- Consent completeness.
- Contraindications and platelets/anticoagulation.
- Epidural technical steps and catheter depth.
- Low-dose mixture composition.
- PCEA vs PIEB logic.
- CSE doses and trade-offs.
- COMET named result.
- Breakthrough algorithm.
- Caesarean conversion by category.
- Hypotension and phenylephrine.
- High/total spinal drill.
- PDPH and blood patch.
- LAST and lipid.
- Remifentanil safety system.
- Special populations (PET, cardiac, obesity).
Fellowship consolidation — labour epidural and CSE [1]
Low-dose mobile labour epidurals combine dilute long-acting local anaesthetic with lipophilic opioid to provide analgesia with less motor block than traditional dense local anaesthetic infusions. COMET showed that low-dose mobile techniques reduced instrumental vaginal delivery compared with traditional higher-dose epidural techniques. [1]
Consent covers benefits of best labour analgesia and convertibility for operative delivery, plus risks of failure, hypotension, PDPH, rare haematoma or infection, and motor block. Check contraindications including coagulopathy, infection at site, and uncorrected hypovolaemia. Time anticoagulants using regional anaesthesia society guidance used by the unit. [1]
CSE offers rapid sacral onset via a small intrathecal dose then epidural maintenance, useful in advanced labour, at the cost of intentional dural puncture considerations and the need to prove epidural function before dense surgical top-up. PCEA with optional programmed intermittent boluses improves patient control; frequent demands suggest catheter problems or dystocia. [1]
Breakthrough pain algorithm: assess stage and block, check catheter depth, reposition, withdraw slightly if unilateral, give manual low-dose bolus, resite or CSE if primary failure, and escalate obstetric review for dystocia. For caesarean conversion, top up early for category 2 to 3 cases toward surgical T4 anaesthesia; for category 1 with a weak epidural, prepare GA using OAA/DAS thinking rather than endless top-ups. [1]
Remifentanil PCA is a monitored alternative when neuraxial is refused or contraindicated, requiring one-to-one midwifery, continuous pulse oximetry, strict PCA protocol, and readiness for sedation-related respiratory depression. Nitrous oxide remains a rapid on-off adjunct with incomplete analgesia. [1]
Complications needing instant algorithms include hypotension with tilt and vasopressors, high or total spinal with airway support, LAST with lipid emulsion, and PDPH pathways culminating in blood patch when disabling. Never top up a questionable catheter for category-1 caesarean without block assessment and GA readiness. [1]
[2]Bottom line for the Final Exam
Labour analgesia passes when you sound like the person who runs the labour ward at 03:00: low-dose by default, CSE when speed and sacral block matter, relentless troubleshooting of breakthrough pain, ruthless honesty about conversion for category-1, and a monitored remifentanil pathway when the needle cannot go in. Name COMET, name OAA/DAS for the GA exit, and never top up hope into a category-1 airway disaster.
[2]References
- [1]COMET Study Group UK. Effect of low-dose mobile versus traditional epidural techniques on mode of delivery: a randomised controlled trial Lancet, 2001.PMID 11454372
- [2]Melber AA et al. Remifentanil patient-controlled analgesia in labour: six-year audit of outcome data of the RemiPCA SAFE Network (2010-2015) Int J Obstet Anesth, 2019.PMID 30685299
- [3]Ngan Kee WD et al. Prophylactic phenylephrine infusion for preventing hypotension during spinal anesthesia for cesarean delivery Anesth Analg, 2004.PMID 14980943
- [4]Mushambi MC et al. Obstetric Anaesthetists' Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation in obstetrics Anaesthesia, 2015.PMID 26449292