Anaes · Thoracic anaesthesia
Lung isolation: double-lumen tubes and bronchial blockers
Also known as Double-lumen tube · Bronchial blocker · Lung isolation · Left-sided DLT · Arndt blocker
Fellowship-level lung isolation: exact adult DLT sizing, left versus right DLT margin of safety, bronchial blocker types and indications, fibreoptic confirmation, and crisis management for malposition.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Why this is examined / the one-line answer
Lung isolation is the technical backbone of thoracic anaesthesia on the ANZCA Final Examination and equivalent boards. Examiners do not accept “I put in a double-lumen tube.” They want exact adult starting sizes, why left-sided tubes are preferred, when a right-sided DLT or bronchial blocker is mandatory, fibreoptic landmarks spoken in sequence, and a malposition drill that links to one-lung ventilation hypoxaemia.
[1]The one-line answer: I prefer a left-sided double-lumen tube sized about 35 French in the average adult woman and 37 French in the average adult man, confirm position with a fibreoptic bronchoscope before and after turning, and I choose a bronchial blocker through at least a 7.5 millimetre single-lumen tube when the airway is difficult, a tracheostomy is present, the patient is a child, lobar isolation is needed, or postoperative ventilation without tube exchange is planned.[1]
Malposition is the leading fixable cause of hypoxaemia during one-lung ventilation. Device choice without confirmation is the leading preventable error in the viva.[3]
Goals of lung isolation
- Collapse the operative lung for surgical exposure.
- Protect the dependent lung from contamination (pus, blood, lavage fluid).
- Permit differential ventilation and suction.
- Allow controlled resumption of two-lung ventilation.
- Preserve a pathway to re-secure the airway if the device fails.
Isolation is a means to safe one-lung ventilation, not an end in itself. Protective OLV settings and the hypoxaemia algorithm are covered in the companion OLV topic; this leaf owns the device.
[2]Preoperative assessment that changes the device
- Airway difficulty: predicted difficult intubation, limited mouth opening, radiation, cervical fixation → secure a single-lumen tube first (awake fibreoptic if indicated), then place a blocker.
- Tracheostomy: blockers through the tracheostomy tube or specialised solutions; standard oral DLT may be impossible or unwise.
- Side and extent of surgery: left pneumonectomy or left main bronchial anastomosis may preclude a left endobronchial cuff sitting in the surgical field → right-sided DLT or alternative strategy.
- Need for postoperative ventilation: DLT exchange to single-lumen at the end is a second airway event; a blocker avoids exchange.
- Paediatric size: many children are better served by blockers or age-appropriate small DLTs (26–28 Fr range in larger children) than adult-sized left DLT dogma.
- Imaging: PA chest radiograph or CT tracheal and bronchial diameters refine DLT size; Brodsky’s tracheal-width method is the classic exam citation.[1]
- Infection or massive haemoptysis: plan early isolation and prefer a device that allows large-bore suction of the dirty lung (often DLT).
Consent should mention sore throat, voice change, dental injury, rare airway trauma, failure of isolation, and conversion plans.
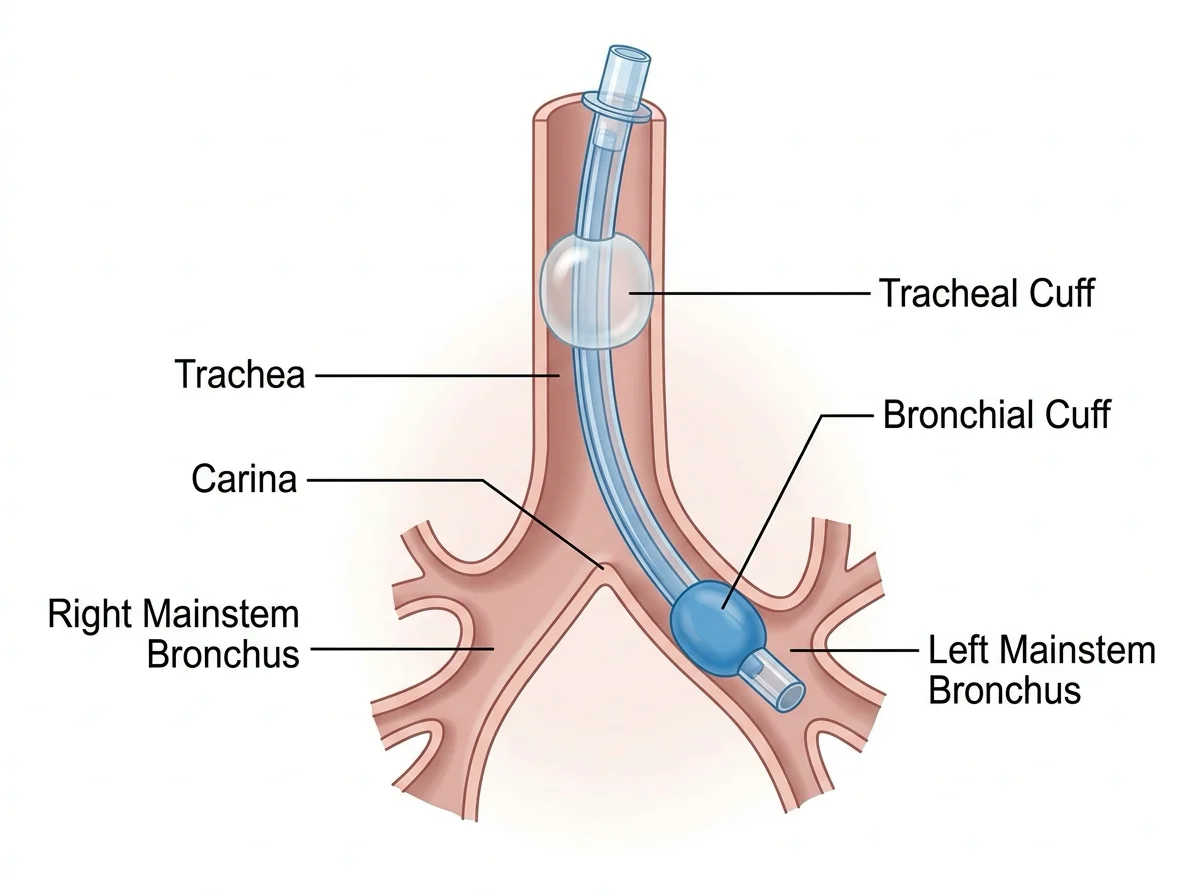
[1]Applied anatomy — the margin of safety argument
The left main bronchus is longer (approximately 4–5 cm) than the right main bronchus (approximately 1.5–2 cm). The right upper lobe bronchus arises early from the right main bronchus. A left-sided DLT therefore has a larger longitudinal window in which the bronchial cuff can sit without obstructing an upper lobe orifice or herniating over the carina. A right-sided DLT must align a side ventilating slot with the right upper lobe orifice under vision — small migrations cause right upper lobe collapse and hypoxaemia.
[1]Exam rule: choose a left-sided DLT for most operations, including many right-sided resections. Reserve right-sided DLT when the left main bronchus is the surgical target (left pneumonectomy, left sleeve resection, left main reconstruction) so the bronchial cuff is not in the operative field.[1]
Exact DLT sizing
Adult double-lumen tubes are sized in French gauge from 26 to 41 Fr. Conventional starting sizes used worldwide in fellowship teaching:
[1]| Patient | Starting left DLT |
|---|---|
| Average adult female | ≈ 35 Fr |
| Average adult male | ≈ 37 Fr |
| Small adult / many Asian body habitus | 32–35 Fr |
| Large male | 39–41 Fr |
Brodsky tracheal-width method (PA chest radiograph tracheal width at the level of the clavicles) guides left DLT selection. Approximate teaching thresholds: wider trachea → larger tube (classically ≥18 mm toward 41 Fr, stepping down through 39, 37, 35 Fr as width decreases).[1] Always have one size up and one size down available. Height alone is a weak predictor; sex plus tracheal width plus clinical fit after insertion matter more.
Paediatric and adolescent sizing is individualised; do not force adult 35/37 Fr into small airways.
[1]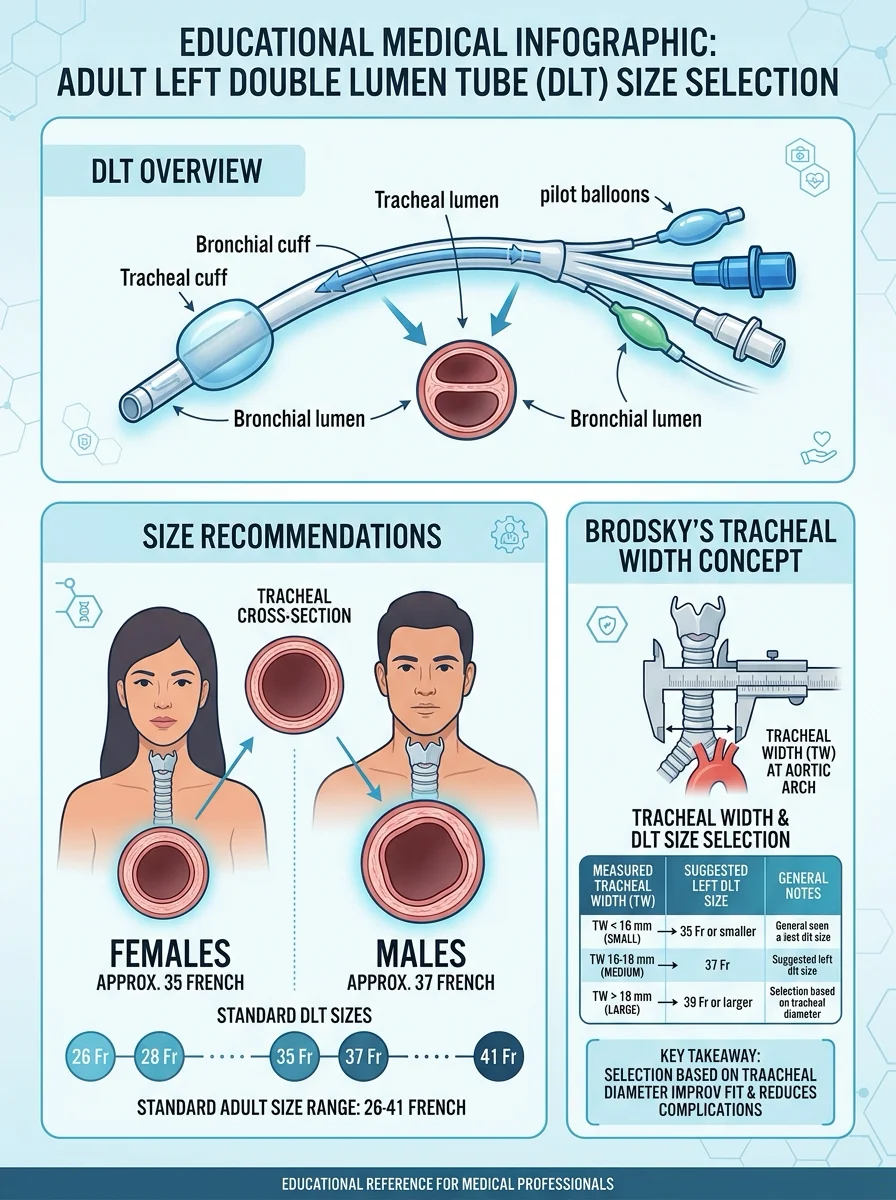
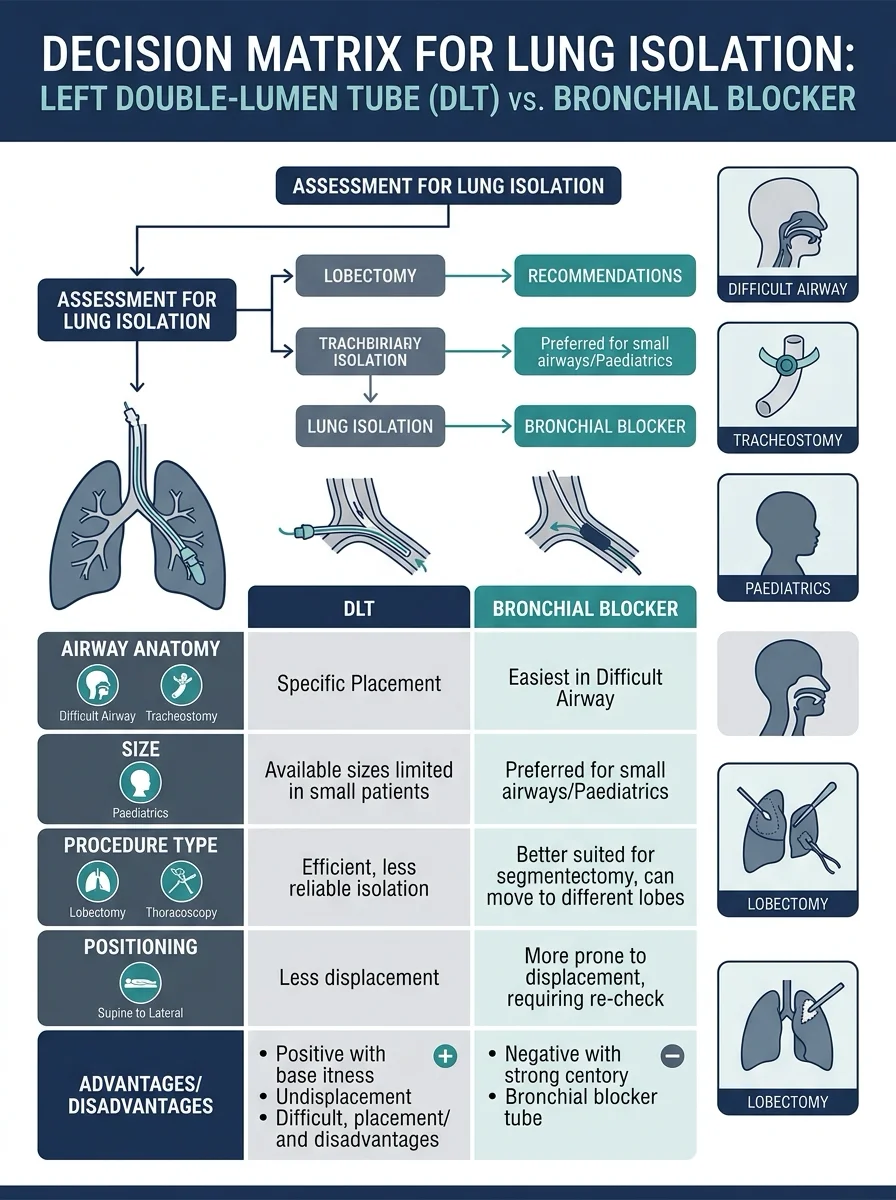
Device decision matrix
Bronchial blockers — types and indications
Common devices:
- Arndt: wire-guided loop snared over a bronchoscope into the target bronchus.
- Cohen: tip-deflecting wheel to steer the tip.
- Fuji Uniblocker: pre-shaped tip, balloon inflation under vision.
- EZ-blocker: bifurcated Y configuration that sits on the carina with a balloon in each main bronchus.
Preferred when:
- Difficult airway (secure single-lumen tube first).
- Existing tracheostomy.
- Paediatrics and small airways.
- Selective lobar isolation (e.g. isolate one lobe rather than whole lung).
- Postoperative ventilation planned without tube exchange.
- Patient already intubated in ICU and needs isolation without re-intubation with a DLT.
Adult carrier tube usually internal diameter ≥7.5 mm to accept the blocker and a fibreoptic scope together.[1] Disadvantages: slower lung collapse sometimes, easier dislodgement with surgical manipulation, poorer suction of massive haemorrhage, and a learning curve for each brand.
Left DLT placement sequence
- Prepare: correct size, spare size, fibreoptic bronchoscope that fits the lumens (often ~3.5–4.0 mm outer diameter), suction catheters, lubricant, syringe for cuffs, clamp, stethoscope as adjunct only.
- Laryngoscopy (direct or video): advance the DLT with the bronchial curvature anterior until the tip passes the vocal cords.
- Rotate 90 degrees toward the left and advance gently.
- Inflate the tracheal cuff; confirm bilateral ventilation and end-tidal CO2.
- Advance until mild resistance or a depth appropriate for the patient (often near 29 cm at the teeth in average-height adults — individualise; never force).
- Inflate the bronchial cuff with minimal air (commonly 1–3 mL); use the least volume that seals.
- Perform isolation tests (clamp/open sequence appropriate to which lung must collapse) while watching peak pressure and EtCO2.
- Mandatory fibreoptic confirmation (see landmarks below).
- Secure meticulously; note depth at teeth.
- Repeat fibreoptic check after lateral positioning — migration is commonest at this moment.[2]
Fibreoptic landmarks (must be sayable)
Via tracheal lumen: carina visible; blue bronchial cuff just inside the left main bronchus without herniating over the carina; no excessive mucosal blanching from overinflation.
[1]Via bronchial lumen: patent left bronchial tree; no obstruction of lobar orifices by the tube tip; mucosa not blanched.
[1]Right DLT: under vision, the side slot must align with the right upper lobe orifice; both middle/lower lobe ventilation via the bronchial lumen and RUL ventilation via the slot must be proven.
[2]Auscultation alone is not fellowship-standard confirmation.[1]
Monitoring and equipment packing list
- Standard anaesthetic monitors plus peak airway pressure alarms.
- Capnography (per lumen awareness when isolating).
- Fibreoptic bronchoscope checked before induction.
- Second isolation strategy immediately available (another DLT size or a blocker kit).
- Suction capable of clearing blood and pus.
- Tube exchanger and video laryngoscope if conversion to single-lumen is planned.
- Arterial line often for major resection; not mandatory for every simple VATS if the patient is fit — individualise.
Intraoperative conduct once isolated
Protective one-lung ventilation (detail in OLV leaf): tidal volume approximately 4–6 mL/kg predicted body weight, peak airway pressure preferably under about 35 cmH2O, titrated FiO2, PEEP to the ventilated lung, and vigilance for hypoxaemia.[2][3] Keep the bronchial cuff inflated only while isolation is required; deflate when two-lung ventilation resumes to limit mucosal injury.
Surgical phases that threaten position: mediastinal retraction, lung traction, patient repositioning, coughing on a light plane, and bronchoscopy by the surgeon. Treat sudden pressure rise or desaturation as malposition until fibreoptically cleared.
[1]Crisis pivots
Malposition
Malposition red flags
Actions: call the problem aloud; increase FiO2; fibreoptic check first; suction; reposition under vision; reinflate cuffs with minimal volume; if isolation cannot be restored, consider device change or intermittent two-lung ventilation while the team regroups.[3]
Hypoxaemia with a correctly placed device
Run the OLV hypoxaemia algorithm: FiO2 to 1.0 → confirm position → suction → PEEP dependent lung → CPAP to operative lung → recruitment → intermittent two-lung ventilation → consider TIVA to spare hypoxic pulmonary vasoconstriction from high volatile concentrations → surgical clamp of pulmonary artery in selected resections as a last intraoperative surgical adjunct.[3]
Airway trauma
Tracheal or bronchial injury from forced advancement or overinflated cuffs presents with subcutaneous emphysema, unexpected air leak, or bloody return. Deflate cuffs, minimise airway pressures, call thoracic surgery, and plan controlled assessment. Prevention: no force, minimal cuff volume, fibreoptic-guided advancement when resistance is felt.
[1]Massive haemoptysis / soiled lung
Isolate early; protect the dependent lung; prefer DLT for large-bore suction; coordinate blood products and definitive surgical or interventional control.
[1]Conversion to single-lumen tube
If postoperative ventilation is needed after a DLT case, exchange under controlled conditions: deep anaesthesia or adequate topicalisation strategy as indicated, video laryngoscopy, airway exchange catheter when appropriate, pre-oxygenation, and a stated failed-exchange plan. Never treat exchange as a casual end-of-list chore after a long thoracic case.[2]
Special populations
- Difficult airway: SLT first, then blocker.
- Paediatrics: blockers or small DLTs; weight-based and age-based size charts; lower trauma threshold.
- Tracheostomy: blocker through tracheostomy tube or custom approaches.
- Obesity: harder laryngoscopy and positioning; fibreoptic skills critical; shorter safe apnoea time.
- ICU transfer already intubated: blocker avoids risky re-intubation with DLT in an oedematous airway.
- Sleeve resections and carinal surgery: highly individualised; often surgical preference and cross-field ventilation — discuss before induction.
Regional notes
ANZ / UK / Europe: left DLT default teaching; fibreoptic confirmation expected; OLV protective ventilation standards shared.
US / Canada: same device principles; institutional preference for certain blocker brands; Brodsky sizing widely taught.[1]
Resource-variable settings: if a fibreoptic scope is unavailable, the examiner still expects you to state that confirmation is suboptimal and to maximise clinical checks while advocating for equipment — do not pretend auscultation equals modern standard.
SAQ answer scaffold
- Goals of isolation and anatomy margin of safety.
- Exact adult starting sizes and Brodsky concept.
- Left versus right versus blocker decision table.
- Stepwise left DLT insertion and fibreoptic landmarks.
- Malposition recognition and first actions.
- Link to OLV hypoxaemia algorithm.
- Conversion plan and special populations.
Viva stem bank with model outlines
Stem 1: “Why left over right for a right upper lobectomy?”
Outline: longer left main bronchus → greater margin of safety; right DLT needs RUL slot alignment; left DLT remains default for most right-sided resections.
Stem 2: “Size this 160 cm woman.”
Outline: start ~35 Fr left DLT; refine with tracheal width if imaging available; have 32 and 37 Fr ready; confirm fibreoptically.[1]
Stem 3: “How do you confirm placement?”
Outline: describe tracheal-view carina and bronchial cuff position, bronchial-view patency, minimal cuff volume, re-check after lateral turn; reject auscultation-only answers.
Stem 4: “When choose a blocker?”
Outline: difficult airway, tracheostomy, child, lobar isolation, postop ventilation without exchange, already intubated ICU patient; SLT ≥7.5 mm ID.
Stem 5: “Peak pressure doubles after turning lateral.”
Outline: malposition until proven otherwise; FiO2 up; fibreoptic immediately; suction; reposition; only then progress down OLV hypoxaemia list.[3]
Stem 6: “Left pneumonectomy — which tube?”
Outline: right-sided DLT or strategy that keeps hardware out of the left main surgical field; discuss with surgeon.
Common traps
- Sizing by height alone without sex or tracheal width.
- Omitting fibreoptic check or skipping re-check after positioning.
- Using a right DLT “for convenience” on routine right-sided surgery.
- Overinflating the bronchial cuff (ischaemia, rare rupture).
- Forcing a DLT against resistance.
- Choosing DLT when a difficult airway demanded SLT-first.
- Forgetting that malposition is the first hypoxaemia fix.
- Casual DLT-to-SLT exchange without a failed-airway plan.
Examiner mental map — fifteen dimensions
- Isolation goals (exposure, protection, suction).
- Left main length vs right RUL anatomy.
- Female ~35 Fr / male ~37 Fr.
- Brodsky tracheal width.
- Left default rule.
- Right DLT indications only.
- Blocker indications list.
- Adult SLT ≥7.5 mm for blockers.
- Insertion rotation sequence.
- Fibreoptic landmarks both lumens.
- Re-check after lateral.
- Minimal bronchial cuff volume.
- Malposition red flags.
- OLV hypoxaemia algorithm link.
- Exchange and special populations.
Troubleshooting atlas in prose
Cannot advance DLT through larynx. Use a bougie or stylet carefully, consider a smaller French size, or abandon to SLT and blocker rather than traumatising the airway.
[1]Isolation incomplete after placement. Fibreoptic check for cuff herniation over carina, endobronchial migration too deep, or underinflated bronchial cuff. Suction and reposition. Do not keep adding large volumes of air to the bronchial cuff.
[1]Sudden desaturation after lateral turn. Re-scope immediately. The tube has often migrated. Re-seat, re-secure, then resume the OLV hypoxaemia ladder if isolation is correct.
[1]Bloody field contaminating both lungs. Prioritise isolation of the bleeding side, aggressive suction of the ventilated lumen, blood products, and surgical control. DLT advantages for suction may dominate blocker convenience.
[1]Postoperative ventilation planned. Prefer blocker from the start or exchange DLT to SLT with an exchange catheter and video laryngoscopy while still paralysed and deeply anaesthetised enough for safety, with a full difficult airway plan ready.
[2]This atlas turns equipment knowledge into crisis behaviour, which is what Final examiners are actually marking.
[1] [1]Final synthesis and must-speak numbers
- Adult DLT range 26 to 41 French
- Start approximately female 35 French, male 37 French
- Left-sided DLT preferred for most cases because longer left main bronchus
- Right-sided DLT mainly for left main bronchial surgery
- Bronchial blocker via single-lumen tube usually at least 7.5 mm internal diameter
- Fibreoptic confirmation after placement and after lateral positioning
- Bronchial cuff usually 1 to 3 mL air for seal
- Protective OLV tidal volume 4 to 6 mL/kg predicted body weight
Device choice algorithm: difficult airway or postop ventilation need favours blocker after secure single-lumen tube; standard resection with easy airway favours left DLT; malposition is the first fixable cause of hypoxaemia and is diagnosed with the fibreoptic scope, not with hope.
[2] [1]Additional placement and confirmation narrative
After the left DLT passes the cords, rotate so the bronchial lumen faces the left, advance until mild resistance or a known depth estimate, inflate the tracheal cuff, confirm bilateral chest rise, then inflate the bronchial cuff with the smallest volume that seals. Fibreoptic inspection via the tracheal lumen must show the carina and a non-herniating bronchial cuff at the left main bronchial origin. Inspection via the bronchial lumen must show a patent left-sided tree. After lateral positioning, repeat both views because flexion and rolling commonly displace the tube. If isolation fails, do not keep ventilating against a malpositioned device; re-scope, suction, and reseat. If the airway was difficult, the safer long-term strategy is often a single-lumen tube with a bronchial blocker rather than repeated traumatic DLT attempts. These habits prevent hypoxaemia far more effectively than late pharmacological improvisation.
[1] [1]Closing line for lung isolation
Left double-lumen tubes sized around 35 French in women and 37 French in men remain the default for most resections because the left main bronchus offers a greater margin of safety. Bronchial blockers via an adequately large single-lumen tube solve difficult airways, tracheostomies, paediatrics, and postoperative ventilation needs. Fibreoptic confirmation after placement and after turning lateral is not optional. When hypoxaemia occurs, assume malposition until the scope proves otherwise, then run the one-lung ventilation algorithm with protective tidal volumes rather than injurious historical settings.
[2] [1]Extra examiner soundbites for lung isolation
"I start with a left-sided double-lumen tube whenever possible: about 35 French in an average adult woman and 37 French in an average adult man."
"I always confirm with fibreoptic bronchoscopy after placement and after turning lateral."
"I choose a bronchial blocker through at least a 7.5 millimetre single-lumen tube for difficult airway, tracheostomy, paediatrics, selective lobar isolation, or planned postoperative ventilation."
"Right-sided double-lumen tubes are reserved mainly for left main bronchial surgery because the right upper lobe orifice arises early and the margin of safety is small."
"Malposition is the leading fixable cause of hypoxaemia during one-lung ventilation and is diagnosed with the scope, not by guesswork."
Final margin note
[1]If forced to give one sentence in a rapid-fire viva, say: left double-lumen tube first for most adults, sized about 35 French in women and 37 French in men, always confirmed fibreoptically before and after turning lateral, with a bronchial blocker reserved for difficult airways and other special indications.
[1] [1]Bottom line for the Final Exam
Lung isolation passes when you sound like the person who can pick the device in thirty seconds, seat it without trauma, prove it with a bronchoscope, and fix it when the peak pressure doubles after the turn. Numbers first, landmarks second, malposition drill third — then hand the physiology of one-lung ventilation to the companion topic without losing the airway.
[2]References
- [1]Brodsky JB et al. Tracheal diameter predicts double-lumen tube size: a method for selecting left double-lumen tubes. Anesthesia and Analgesia, 1996.PMID 8615510
- [2]Brassard CL et al. Step-by-step clinical management of one-lung ventilation: continuing professional development. Canadian Journal of Anesthesia, 2014.PMID 25389025
- [3]Karzai W, Schwarzkopf K. Hypoxemia during one-lung ventilation: prediction, prevention, and treatment. Anesthesiology, 2009.PMID 19417615