Anaes · Obstetric anaesthesia
Non-obstetric surgery in pregnancy: timing, conduct and fetal considerations
Also known as Surgery during pregnancy anaesthesia · Appendicectomy pregnancy · ACOG nonobstetric surgery · Second trimester elective surgery
Exam-exhaustive anaesthesia for non-obstetric surgery in pregnancy: ACOG timing principles, trimester physiology, aspiration and left uterine displacement, haemodynamic and CO2 goals, laparoscopy adaptations, fetal monitoring philosophy, VTE, and crisis pathways for ANZCA Final and secondary fellowship exams.
On this page & tools
Your progress
Saved locally on this device.
3 MCQs with explanations
Target exams
Red flags
Why this is examined / the one-line answer
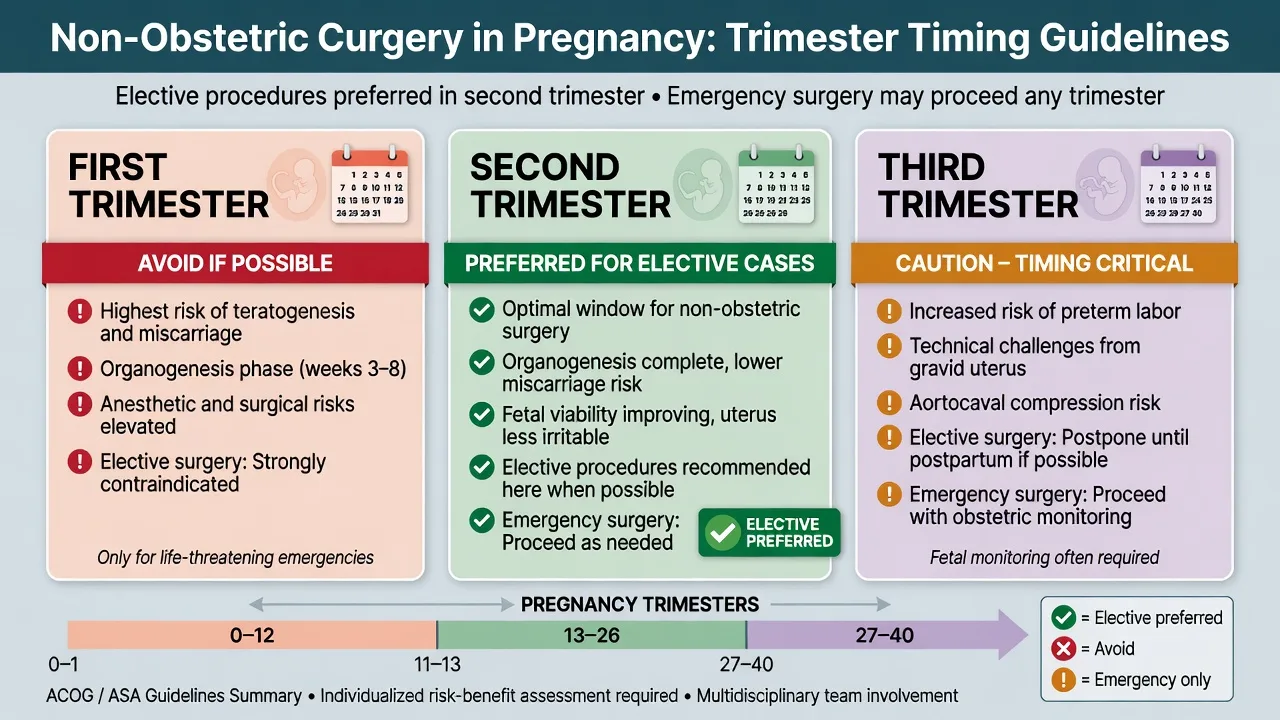
Appendicectomy, cholecystectomy, adnexal torsion, trauma, neurosurgery, and cancer surgery all occur in pregnancy. Fellowship examiners want a decisive opening line: necessary surgery proceeds, timing and technique are adapted to maternal–fetal physiology, and the fetus is protected by protecting the mother. ACOG Committee Opinion 775 states that a pregnant woman should never be denied indicated surgery solely because she is pregnant; elective procedures may be deferred to the second trimester when feasible, but urgency always trumps trimester dogma.[1]
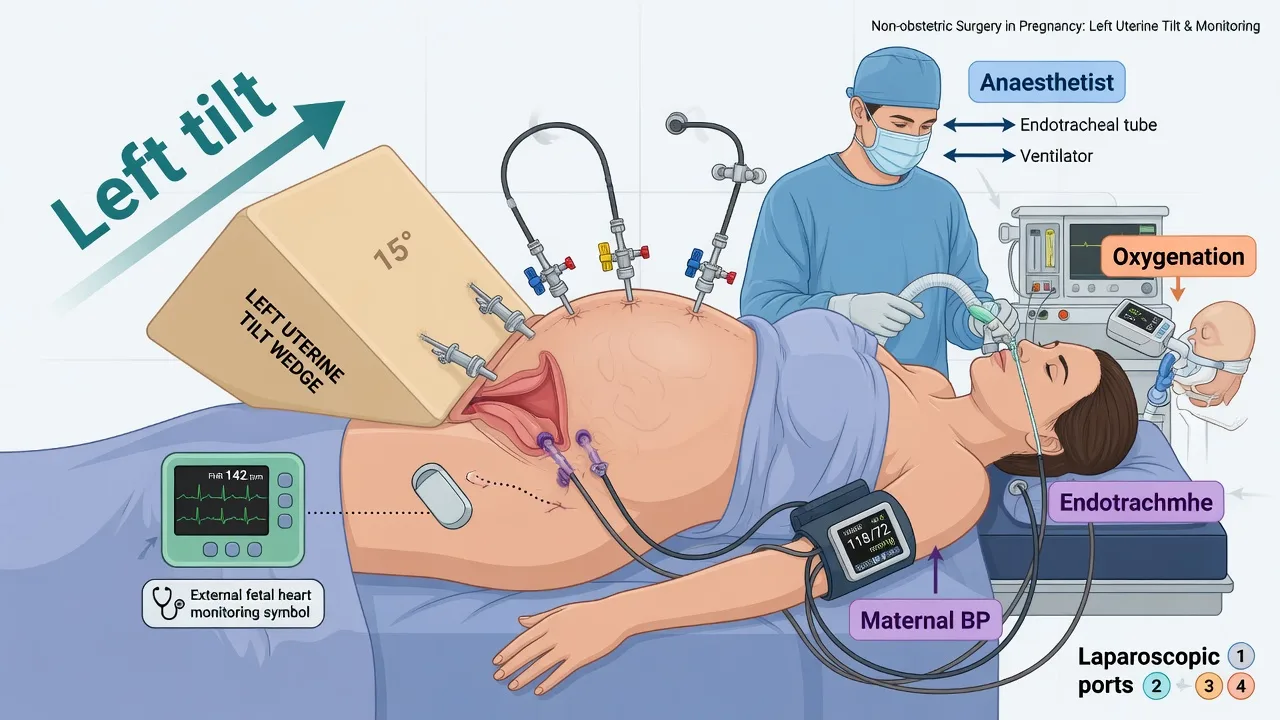
The viva discriminators are not obscure teratology lists. They are the practical checklist: left uterine displacement after about 20 weeks, aspiration readiness and obstetric-style airway thinking in late pregnancy, blood pressure near baseline for uteroplacental perfusion, controlled CO2 rather than aggressive hyperventilation, laparoscopy adaptations, fetal heart monitoring only when it will change management, and VTE prophylaxis because pregnancy is hypercoagulable. Reitman and Flood synthesise the anaesthetic evidence base that examiners still expect candidates to paraphrase.[2]
Preoperative assessment and risk stratification
Obstetric facts first. Confirm gestational age by dates and ultrasound if available, viability, placenta location if relevant to positioning or radiation, multiple pregnancy, and any threatened preterm labour or cervical insufficiency. Speak to obstetrics before elective lists and urgently before emergencies involving a viable fetus. Document the indication and why delay is or is not safe: appendicitis delayed for “the baby” becomes maternal sepsis and fetal loss — a classic fail.[1]
Urgency classification for the team. Emergency (life or organ threat now — trauma laparotomy, ovarian torsion, ruptured appendix with peritonitis), urgent (within hours — symptomatic cholelithiasis with cholangitis), semi-elective (cancer staging windows), or truly elective (can wait until postpartum or second trimester). ACOG supports indicated surgery in any trimester; the second trimester preference applies only when postponement does not increase maternal risk.[1]
Maternal systems review. Airway and Mallampati progression with gestation and oedema; reflux and fasting status; anaemia; gestational hypertension or pre-eclampsia features; diabetes; cardiac disease; VTE history; thrombophilia; anticoagulation; previous obstetric anaesthetic chart; allergies. After about 20 weeks assume aortocaval compression risk in the supine position. In labour or after opioids, gastric emptying is delayed and full-stomach precautions apply more strictly.[2]
Fetal considerations and counselling. Discuss that most modern anaesthetics at clinical doses have not been proven major teratogens when maternal oxygenation and perfusion are maintained; the greater fetal risks are maternal hypoxia, hypotension, severe hypercarbia or hypocarbia, sepsis, and delay of indicated care. Avoid routine prophylactic tocolysis solely because surgery occurs — tocolysis is not an automatic accompaniment of non-obstetric anaesthesia. Radiation, contrast, and laparoscopy require obstetric and surgical shared decisions with fetal dose considerations.[1][2]
Consent structure. Maternal risk, fetal risk, conversion plans, possible preterm delivery contingency if the fetus is viable, postoperative analgesia plan including NSAID limits in late pregnancy, and VTE prophylaxis. If general anaesthesia is planned near term, mention awareness risk and difficult airway pathways in obstetric language.[3]
Applied anatomy, physiology, and pharmacology
Trimester physiology stack
First trimester: organogenesis (highest theoretical teratogenic concern, though modern agents used carefully have not shown consistent major teratogenicity); nausea and aspiration risk; still relatively easy airway compared with term; elective surgery often deferred if safe.[2]
Second trimester: organogenesis complete; uterus not yet maximally impairing FRC and aortocaval return in early second trimester; often the preferred window for semi-elective cases when delay from first trimester is safe.[1]
Third trimester: full obstetric physiology — FRC down, oxygen consumption up, rapid desaturation, engorged airway mucosa, reduced lower oesophageal sphincter tone, aortocaval compression, increased local anaesthetic sensitivity, reduced MAC, and hypercoagulability. Airway and aspiration plans mirror obstetric general anaesthesia thinking.[2][3]
Cardiorespiratory and uteroplacental physiology
Cardiac output and blood volume rise through pregnancy; systemic vascular resistance falls; the gravid uterus compresses the inferior vena cava and aorta in the supine position from about 20 weeks, reducing venous return and placental perfusion. Left lateral tilt of about 15 degrees or manual uterine displacement is mandatory until delivery of a large uterus or completion of surgery with ongoing displacement. Placental perfusion is pressure-dependent without strong autoregulation: maternal hypotension is fetal hypoperfusion. Oxygen delivery depends on maternal SpO2, haemoglobin, and cardiac output — treat anaemia and hypoxia aggressively.[2]
Minute ventilation is already elevated and PaCO2 at term is roughly 4.0 kPa (about 30 mmHg). Extreme hypocapnia causes uterine artery vasoconstriction; extreme hypercapnia and acidosis also harm. Aim near the patient’s pregnant baseline rather than non-pregnant “normal” hyperventilation targets. FRC reduction plus raised oxygen consumption collapses safe apnoea time — preoxygenate meticulously if general anaesthesia is used.[2]
Pharmacology notes examiners want
Most intravenous induction agents, volatiles, opioids, and muscle relaxants are used when indicated; prioritise maternal stability over speculative fetal drug avoidance. Avoid NSAIDs in later pregnancy when possible because of fetal renal effects and ductus arteriosus concerns; prefer paracetamol and carefully titrated opioids, with regional analgesia when suitable. Vasopressors: pure alpha-1 agonists such as phenylephrine restore SVR with a favourable fetal acid-base profile compared with ephedrine in the obstetric spinal literature, and this physiology is commonly extrapolated when treating maternal hypotension under anaesthesia in pregnancy.[4] Suxamethonium remains acceptable for RSI; rocuronium with sugammadex is an alternative when the difficult airway plan requires it.[3]
Anaesthetic goals
- Maternal safety first — oxygenation, ventilation, perfusion, and surgical disease control.
- Left uterine displacement after about 20 weeks until the uterus is no longer compressing vessels.
- Aspiration prophylaxis and airway readiness proportional to gestation and fasting state.
- Maintain blood pressure near baseline; treat hypotension early with phenylephrine or local vasopressor protocols.[4]
- Keep CO2 near pregnant baseline; avoid prolonged extremes.
- Prefer regional anaesthesia when the surgery and coagulation allow, to avoid airway instrumentation.
- Agree fetal monitoring strategy and obstetric call-out before induction.
- Plan postoperative VTE prophylaxis and multimodal analgesia safe for gestation and breastfeeding intent.[1]
Technique options and decision matrix
Regional versus general
Regional anaesthesia reduces airway manipulation and fetal drug exposure and provides excellent analgesia, but still requires left tilt, vasopressor readiness, and attention to local anaesthetic dosing (reduced requirements in pregnancy). General anaesthesia is indicated for many upper abdominal, laparoscopic, neurosurgical, and emergency cases, for coagulopathy, and when the patient refuses regional. Near term, treat the airway as an obstetric airway: preoxygenate to high end-tidal oxygen, have video laryngoscopy and second-generation SGA ready, and know the failed intubation pathway.[3]
Laparoscopy in pregnancy
Laparoscopy is widely used for appendicectomy and cholecystectomy when teams are experienced. Principles: open entry or carefully chosen access to avoid uterine injury; modest pneumoperitoneum pressures; reverse Trendelenburg only as needed and with attention to venous return; ETCO2 control with adequate minute ventilation; left tilt maintained; low threshold to convert to open if ventilation or haemodynamics fail. Fetal CO2 depends on maternal PaCO2 — do not allow progressive hypercarbia.[2]
Fetal monitoring philosophy
Before viability, document fetal heart rate before and after anaesthesia when practical. After viability, continuous intraoperative fetal heart rate monitoring is used only if: (1) it is technically feasible given the surgical field, (2) a clinician who can interpret it is present, and (3) an abnormal trace would change management (for example prompt delivery). Many abdominal cases use intermittent pre- and post-procedure checks rather than continuous monitoring that cannot alter care. The obstetric team must know the case is occurring and have a delivery plan if the fetus is viable.[1]
Monitoring and equipment
Standard AAGBI/ANZCA monitoring; left lateral tilt devices or wedges; large-bore intravenous access for major cases; phenylephrine or metaraminol drawn; difficult airway trolley for general anaesthesia in later pregnancy; fetal Doppler or CTG machine as agreed; obstetric contact numbers confirmed; blood available if haemorrhage risk; thromboprophylaxis plan charted. Arterial line for unstable trauma, major haemorrhage, or significant cardiac disease. Capnography is mandatory for general anaesthesia and useful to track CO2 during laparoscopy.[2][3]
Intraoperative management
Position with left uterine displacement after about 20 weeks. For neuraxial cases, co-load or preload crystalloid per local practice and treat any significant blood pressure fall immediately with phenylephrine (typical obstetric bolus ranges 50–100 microg IV, titrated), remembering fetal acid-base advantages of pure alpha support over ephedrine-heavy regimens in spinal literature.[4] For general anaesthesia: antacid prophylaxis (non-particulate sodium citrate when time-critical; H2-blocker or PPI if earlier opportunity), head-up preoxygenation, RSI when full stomach or late pregnancy risk is high, confirm tube with waveform capnography, ventilate to near-baseline ETCO2, maintain MAP near baseline, and keep the surgical team efficient. Avoid prolonged deep volatile relative overdose without monitoring depth context; TIVA is acceptable when preferred. Temperature maintenance and glucose control matter for maternal recovery and fetal wellbeing.[2]
Document times of induction, any hypotensive episodes, and fetal checks. If the uterus is large and cardiac arrest occurs, follow maternal ALS with continuous left uterine displacement and prepare for resuscitative hysterotomy by four minutes of arrest when the uterus impairs resuscitation — maternal survival is the primary goal.[3]
Crisis pivots — what changes the plan
Maternal hypoxia or failed intubation: declare early, limit trauma, second-generation SGA, OAA/DAS obstetric pathway if late pregnancy, and remember the fetus is resuscitated by resuscitating the mother.[3]
Severe maternal hypotension: increase tilt/manual displacement, fluids if hypovolaemic, phenylephrine or other vasopressors, treat haemorrhage and sepsis at source, and check aortocaval compression first before attributing everything to anaesthetic depth.[4]
Suspected preterm labour after surgery: obstetric review; tocolysis only on obstetric advice, not as routine anaesthetic co-therapy.[1]
Trauma with viable fetus: prioritise maternal ATLS; continuous fetal monitoring when feasible after primary survey; early obstetric involvement; perimortem caesarean pathway if maternal arrest.[2]
Massive obstetric-scale haemorrhage during non-obstetric surgery: activate major haemorrhage protocol, correct coagulopathy, consider tranexamic acid when bleeding trauma or PPH-like physiology coexists per local obstetric/trauma protocols, and maintain tilt and uterine perfusion pressure.
[2]Postoperative / ICU / PACU plan
Recover in left lateral or semi-recumbent with tilt if still pregnant. Multimodal analgesia: paracetamol first-line; opioids as needed; avoid NSAIDs in later pregnancy when possible; regional catheters or single-shot blocks when helpful. Early mobilisation. VTE prophylaxis is essential — pregnancy is a hypercoagulable state and surgery multiplies risk; use mechanical methods plus pharmacological prophylaxis timed to neuraxial catheters per ASRA-style intervals when relevant. Obstetric review before discharge from recovery for viable pregnancies; fetal heart documentation; counselling about warning signs of preterm labour. Critical care if major trauma, sepsis, or significant comorbidity.[1][2]
Special populations and comorbidities
Pre-eclampsia complicating non-obstetric surgery: BP control, magnesium if indicated for PET, fluid caution, airway oedema, and coagulopathy/platelet checks before neuraxial. Cardiac disease: pregnancy heart team principles apply even for appendicectomy. Obesity: ramp, video laryngoscope, VTE, and dosing by lean body weight where appropriate. Multiple gestation: worse aortocaval compression. Substance use or unbooked pregnancy: assume full stomach and limited history. Cancer surgery in pregnancy: MDT timing; chemotherapy and radiotherapy decisions are obstetric-oncology led; anaesthesia focuses on maternal optimisation and fetal monitoring philosophy.[1]
SAQ answer scaffold
A 15-mark stem: A 28-year-old at 24 weeks needs laparoscopic appendicectomy for suspected appendicitis.
[3]- Principle (2): do not delay indicated surgery because of pregnancy; cite ACOG-style guidance.[1]
- Preop (3): gestation, obstetric contact, airway/aspiration, tilt plan, fetal monitoring decision, VTE.
- Conduct (5): left displacement, GA vs regional rationale, RSI elements if GA, CO2 and BP targets, phenylephrine for hypotension, laparoscopy pressure/position notes.[2][4]
- Airway crisis (3): obstetric failed intubation mindset if advanced gestation.[3]
- Postop (2): analgesia without late-pregnancy NSAIDs if avoidable, VTE, obstetric review.
Viva stem bank and model phrases
Stem: “She is 18 weeks pregnant with acute cholecystitis. Surgeons want to wait until after delivery.”
Model: “If this is indicated now, ACOG-type guidance is that pregnancy is not a reason to deny surgery; I will optimise and proceed with obstetric input rather than accept maternal sepsis.”[1]
Stem: “What is your one-line anaesthetic plan at 32 weeks for open appendicectomy?”
Model: “Left tilt, aspiration prophylaxis and RSI readiness, maintain BP and oxygenation for the placenta, control CO2 near her pregnant baseline, and have obstetrics aware with a fetal plan.”[2]
Stem: “How do you treat hypotension under spinal for ankle ORIF at 30 weeks?”
Model: “Increase left displacement, give phenylephrine titrated boluses, restore circulating volume if needed, and remember uteroplacental flow is pressure-dependent.”[4]
Deep dive: common procedures and anaesthetic modifiers
Appendicectomy. Presentation overlaps with pregnancy discomfort; imaging may use ultrasound or carefully justified MRI/CT. Laparoscopic appendicectomy is standard in many centres with the positioning and pneumoperitoneum caveats already described. If peritonitis and sepsis dominate, resuscitate with oxygen, fluids, early antibiotics, and source control — fetal survival tracks maternal recovery, not delay. Neuraxial anaesthesia is rarely suitable for laparoscopy; general anaesthesia with left tilt and controlled ventilation is usual.[1][2]
Cholecystectomy. Biliary colic and cholecystitis are common. Laparoscopic cholecystectomy follows the same laparoscopy rules: open entry consideration, modest pressures, reverse Trendelenburg cautiously because it worsens venous return when combined with pneumoperitoneum and a gravid uterus. Convert early if ventilation fails or surgical access is unsafe.[2]
Adnexal torsion and ectopic pregnancy. These are obstetric–gynaecological emergencies that still obey non-obstetric surgical urgency logic: operate to save ovary or treat rupture. Haemorrhage from ruptured ectopic can be massive — large-bore access, blood products, left tilt if a coexisting intrauterine pregnancy is advanced, and avoid delaying for non-essential tests.[1]
Trauma laparotomy and orthopaedic fixation. Apply ATLS to the mother. Cervical spine precautions, pelvic binders, and haemorrhage control come before detailed fetal counselling. After viability, continuous fetal monitoring is considered once the mother is stabilised if it will change management. Fracture fixation timing balances maternal mobility (VTE reduction) against fetal physiology and radiation; the orthopaedic and obstetric teams share decisions, while anaesthesia delivers maternal optimisation and VTE planning.[2]
Neurosurgery and cardiac surgery in pregnancy. Rare high-stakes intersections: maintain CPP and oxygenation for neurosurgical disease while respecting aortocaval displacement; cardiac surgery with cardiopulmonary bypass requires specialised maternal–fetal centres. Principles still hold — do not deny indicated maternal life-saving surgery.[1]
Deep dive: drug myths versus evidence-minded practice
Examiners punish laundry lists of “banned drugs” that are not grounded in maternal priority. What matters is avoiding maternal hypoxia, hypotension, and uncontrolled hypercarbia. Benzodiazepines historically carried cleft lip concerns from older literature; single perioperative doses for clear indications are often still used judiciously. Nitrous oxide is variably avoided in early pregnancy by some clinicians because of methionine synthase inhibition concerns, though practice varies — many simply omit it because air/oxygen and volatiles or TIVA suffice. NSAIDs in the third trimester risk fetal renal impairment and premature ductus closure — prefer alternatives late in pregnancy. ACE inhibitors and ARBs are contraindicated for ongoing therapy in pregnancy but that is medical therapy context more than a single anaesthetic moment. Always check the latest local obstetric pharmacology resources for breastfeeding plans after delivery if the pregnancy ends perioperatively.[2]
Vasopressor choice deserves repetition because it is high-yield: ephedrine was historically preferred on the false belief that pure alpha agonists reduced uteroplacental flow; quantitative reviews of spinal anaesthesia for caesarean delivery showed phenylephrine produces better fetal acid-base status than ephedrine. When the pregnant patient under non-obstetric anaesthesia becomes hypotensive from sympathectomy or anaesthetic vasodilation, phenylephrine is a rational first-line agent unless bradycardia or other context dictates otherwise.[4]
Deep dive: human factors and communication
State the plan aloud: gestation, tilt, airway strategy, fetal monitoring decision, and who to call if the fetal heart becomes non-reassuring. Night-time appendicectomy with a junior team is a classic setup for omitted obstetric notification. If delivery might be required (viable fetus, unstable mother, or surgery that precipitates labour), ensure neonatal resuscitation capability exists in the hospital. Document gestational age, indication for not delaying, and counselling in the anaesthetic record — medicolegal and handover value are high.[1]
Extended viva model answers
“Is general anaesthesia teratogenic?”
“At clinical doses used for surgery, with maintained maternal physiology, modern anaesthetics have not been shown to be major teratogens in the way examiners fear; the dominant fetal risks are maternal hypoxia, hypotension, severe CO2 disturbance, sepsis, and delayed indicated surgery. I still prefer the second trimester for elective work when safe, per ACOG-type guidance.”[1][2]
“Do you give prophylactic tocolysis?”
“Not routinely. Surgery itself is not an automatic indication for tocolysis; I involve obstetrics if there are contractions or other obstetric concerns.”[1]
“How do you ventilate in laparoscopy at 28 weeks?”
“Left tilt, modest pneumoperitoneum, increase minute ventilation to keep ETCO2 near her pregnant baseline, watch peak pressures and venous return, and convert to open if I cannot ventilate or maintain blood pressure safely.”[2]
Extended SAQ worked example
Stem: A 31-year-old G2P1 at 26 weeks presents with peritonism and imaging consistent with appendicitis. She last ate 4 hours ago. Blood pressure is 95/55 mmHg sitting.
[3]Opening statement: indicated surgery proceeds; pregnancy does not justify delay of appendicectomy with peritonitis risk. I will notify obstetrics, prepare left uterine displacement, treat hypotension, and plan general anaesthesia with full-stomach precautions.[1]
Preoperative: large-bore IV, bloods including group and hold, antacid, fetal heart rate documentation, discuss laparoscopy versus open with surgeons, confirm neonatal and obstetric availability. Resuscitate blood pressure toward baseline with fluids if hypovolaemic and phenylephrine as needed before induction so uteroplacental perfusion is restored.[4]
Intraoperative: left tilt, preoxygenation, RSI, video laryngoscope available, ventilate to near-baseline ETCO2, maintain MAP, communicate fetal plan, avoid prolonged deep Trendelenburg. If septic shock develops, use culture-guided antibiotics, source control, and ICU — not tocolysis as the primary answer.[2]
Postoperative: multimodal analgesia without third-trimester NSAIDs if avoidable, VTE prophylaxis, obstetric review, fetal heart check, early mobilisation, sepsis pathway if indicated.[1]
Common traps
Delaying emergency appendicectomy “for the baby”; operating flat supine after 20 weeks without tilt; aggressive hyperventilation to non-pregnant low ETCO2; omitting obstetric notification for a viable fetus; forgetting VTE prophylaxis; using late-pregnancy NSAIDs casually; debating teratogenicity while the mother desaturates; continuous fetal monitoring that cannot change management and distracts from maternal care.
[3]
PREG SURG checklist
References
- [1]ACOG ACOG Committee Opinion No. 775: Nonobstetric Surgery During Pregnancy Obstet Gynecol, 2019.PMID 30913200
- [2]Reitman E, Flood P Anaesthetic considerations for non-obstetric surgery during pregnancy Br J Anaesth, 2011.PMID 22156272
- [3]Mushambi MC, Kinsella SM, Popat M, et al. Obstetric Anaesthetists' Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation in obstetrics Anaesthesia, 2015.PMID 26449292
- [4]Lee A, Ngan Kee WD, Gin T A quantitative, systematic review of randomized controlled trials of ephedrine versus phenylephrine for the management of hypotension during spinal anesthesia for cesarean delivery Anesth Analg, 2002.PMID 11916798