Anaes · Thoracic anaesthesia
One-lung ventilation physiology and the hypoxaemia management algorithm
Also known as OLV hypoxaemia · One-lung ventilation algorithm · Double-lumen tube hypoxaemia
OLV shunt physiology, hypoxic pulmonary vasoconstriction, DLT versus bronchial blocker principles, lung-protective OLV settings, and the stepwise hypoxaemia algorithm for fellowship exams.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Why this is examined
Hypoxaemia during one-lung ventilation is the canonical thoracic crisis. Examiners expect physiology (shunt and HPV), equipment (DLT versus blocker), protective ventilation settings, and a memorised stepwise algorithm that starts with fibreoptic confirmation rather than exotic pharmacology.[1] Curriculum code cluster: SS_TS.
Physiology of OLV
Lateral decubitus distribution
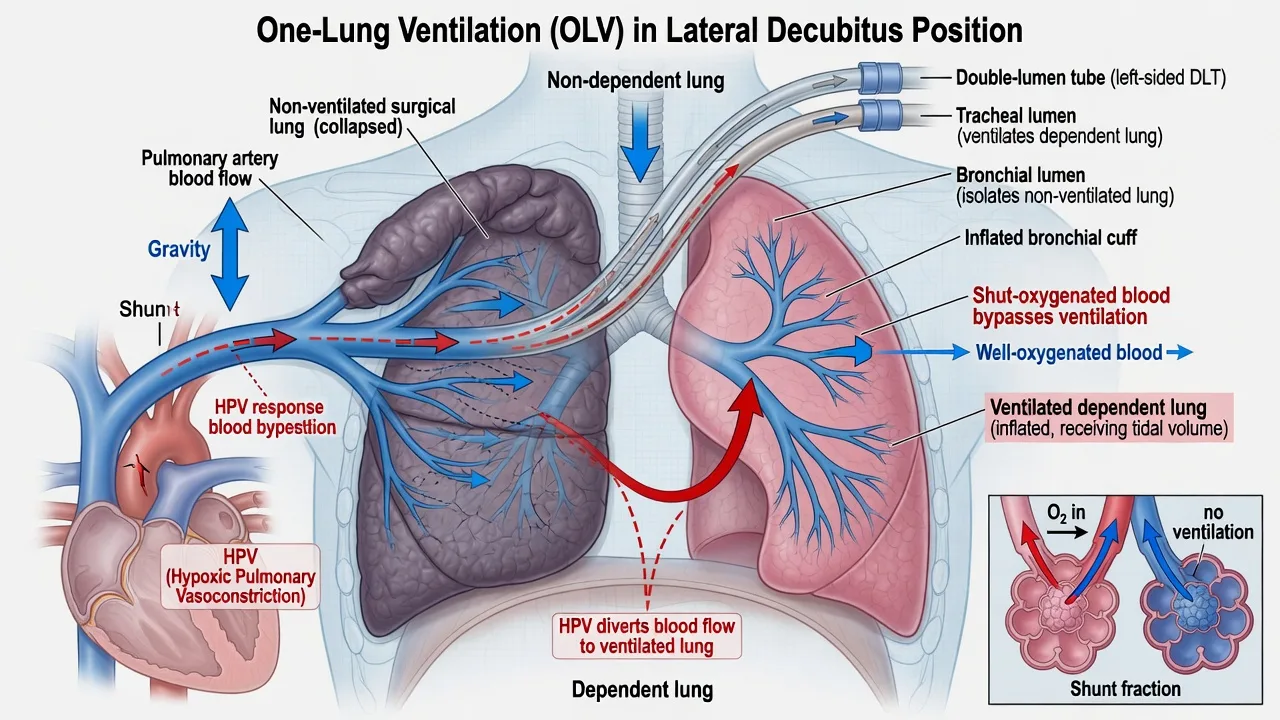
In the awake lateral position, gravity prefers perfusion of the dependent lung. Under anaesthesia and paralysis, the non-dependent lung becomes more compliant and preferentially ventilated if both lungs are open — until isolation. When OLV begins, the non-dependent (surgical) lung is excluded from ventilation but still receives blood flow → true shunt.
[1]Approximate starting perfusion shares (teaching figures): dependent lung ~60%, non-dependent ~40% before HPV fully acts. HPV and surgical manipulation then reduce non-dependent flow.
[1]Hypoxic pulmonary vasoconstriction (HPV)
HPV is the physiological response of pulmonary arterial smooth muscle to low alveolar PO2, diverting blood from hypoxic to better-oxygenated lung regions. During OLV it is the main innate defence against shunt.[1]
Time course (exam): onset within minutes; early peak often described around 15–30 minutes, with a slower second phase over hours in experimental models. Do not expect instant perfection the second you clamp.
[1]Inhibitors of HPV (high-yield list):
[1]- Volatile anaesthetics (dose-dependent; all volatiles to some degree)
- Direct pulmonary vasodilators (nitroprusside, GTN, high-dose calcium antagonists, some PDE inhibitors)
- Infection/inflammation in the non-ventilated lung (pneumonia blunts HPV)
- Extreme hypocapnia / alkalosis patterns
- Very high mixed venous PO2 patterns and some haemodilution states
Preserved/relatively spared: total intravenous anaesthesia (propofol-based) is preferred when HPV must be maximised for refractory hypoxaemia; surgical retraction that mechanically reduces non-ventilated lung blood flow also helps oxygenation (at surgical cost).
[1]Other determinants of OLV PaO2
- Cardiac output (low CO can lower mixed venous O2 and worsen arterial hypoxaemia for a given shunt fraction)
- Haemoglobin (content)
- Dependent-lung atelectasis
- Malposition of DLT/blocker (most common fixable cause)
- Secretions, blood, pneumothorax of dependent lung
Remember oxygen delivery is content times flow — treat anaemia and low cardiac output as part of refractory hypoxaemia, not only FiO2 tricks.
[1]Lung isolation tools
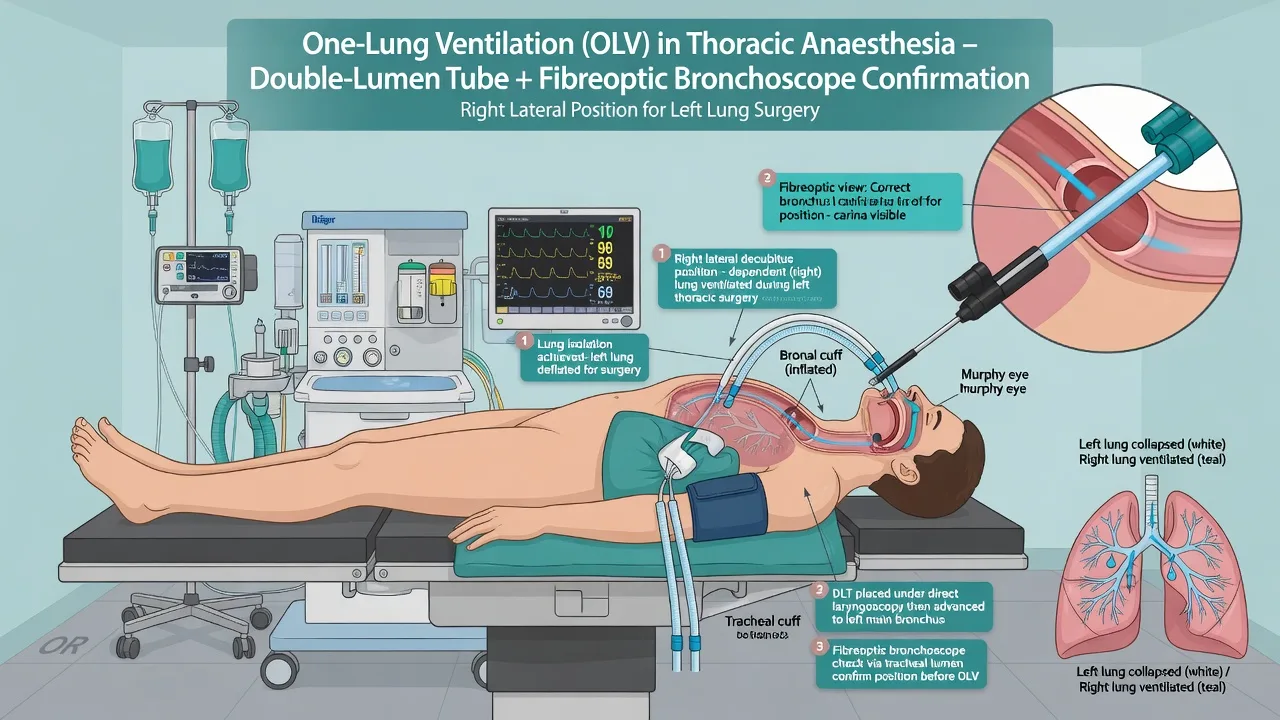
Left-sided DLT is the default for most operations because the left main bronchus is longer, giving a greater margin before the tube migrates into or out of position. Always confirm with fibreoptic bronchoscopy after intubation and after turning lateral.
[1]Protective OLV settings
- Tidal volume 4–6 mL/kg predicted body weight
- Moderate PEEP to the ventilated lung (individualise; avoid over-distension that diverts blood to the non-ventilated lung)
- FiO2 high at onset of OLV, then titrate if stable
- Rate adjusted for CO2; accept permissive hypercapnia when needed for protection
- Peak airway pressure preferably under about 35 cmH2O
- Recruitment manoeuvres of the ventilated lung after isolation or after desaturation recovery
- Avoid routine large 10 mL/kg one-lung volumes (historical practice, injurious)
Hypoxaemia algorithm (memorise in order)
OLV hypoxaemia ladder
Differential of refractory hypoxaemia
- Tube/blocker malposition (still number one)
- Secretions or blood
- Dependent-lung pneumothorax or mainstem issues
- Severe HPV failure (pneumonia, vasodilators, high-dose volatiles)
- Low cardiac output / anaemia
- Circuit disconnect, low FiO2 delivery failure
- Wrong diagnosis: anterior mediastinal mass airway collapse is not “fix with more OLV tricks”
Anaesthetic technique notes
- Thoracic epidural or paravertebral analgesia for open thoracotomy pain (separate skill set).
- Inhalational maintenance is common; switch toward TIVA if HPV-critical hypoxaemia persists.[1]
- Paediatric OLV physiology is the same shunt/HPV story at smaller scale; isolation tools differ (blockers, endobronchial intubation).
SAQ answer scaffold
- Define OLV shunt and role of HPV with time course.[1]
- List HPV inhibitors including volatiles.
- Protective settings 4–6 mL/kg PBW.
- Full hypoxaemia ladder in order.
- CPAP vs PEEP roles and surgical communication.
Viva stem bank
- “SpO2 is 86% five minutes after OLV — your steps?”
- “Why might isoflurane 1.5 MAC worsen oxygenation on OLV?”
- “PEEP or CPAP — which lung, and why?”
- Model phrase: “Fibreoptic confirmation before exotic pharmacology — most OLV hypoxaemia is malposition or secretions.”
Worked hypoxaemia viva script (45 seconds)
“FiO2 to 1.0. Tell the surgeon. Fibreoptic check of the DLT — look for herniation, endobronchial migration, and secretions. Suction. Apply moderate PEEP to the dependent lung. If still hypoxic, apply low-level CPAP or oxygen insufflation to the operative lung with surgical agreement. Recruit the ventilated lung. If critical, resume two-lung ventilation intermittently. Switch toward TIVA to spare HPV. Check blood pressure and haemoglobin. Rule out pneumothorax of the dependent side.”
[1]That script is more valuable than a paragraph of unsorted tips.
[1]DLT placement confirmation landmarks (left-sided)
Fibreoptic view via tracheal lumen: carina visible; blue bronchial cuff just inside left main bronchus without herniating over carina. Via bronchial lumen: patent left bronchial tree. After lateral positioning, re-confirm — most malpositions declare after turning.
[1]HPV pharmacology depth
Volatiles inhibit HPV in a dose-dependent manner; modern agents at 1 MAC or less are often clinically acceptable, but when SpO2 is marginal, reducing volatile and converting to propofol TIVA is a standard lever.[1] Intravenous vasodilators used for deliberate hypotension or graft spasm can worsen shunt. Acid–base: aim near normocapnia; extreme hypocapnia is not a free optimisation tool.
Lung injury prevention after OLV
Protective tidal volumes, limited plateau pressures, judicious fluids, and early extubation pathways when appropriate reduce postoperative pulmonary complications. OLV is not an excuse for 10 mL/kg forever “because the other lung is down.”
[1]Shunt fraction intuition
When one lung is excluded from ventilation but still perfused, that blood flow is true shunt. HPV and surgical compression reduce non-ventilated lung blood flow over minutes. Approximate pre-HPV perfusion shares in lateral position are often taught as ~60% dependent / ~40% non-dependent before HPV fully acts — use as teaching figures, not universal constants.[1]
HPV time course and inhibitors (list to memorise)
Onset within minutes; early maximum often described around 15–30 minutes, with slower phases thereafter. Inhibitors: volatiles (dose-dependent), many systemic pulmonary vasodilators, infected lung, extreme alkalosis/hypocapnia patterns, and some haemodilution states. TIVA relatively spares HPV compared with high-dose volatile.
[1]Protective OLV settings panel
- VT 4–6 mL/kg predicted body weight
- Peak airway pressure preferably under ~35 cmH2O
- Moderate PEEP to ventilated lung (individualise)
- FiO2 high at OLV onset then titrate
- Permissive hypercapnia when needed for protection
- Recruitment after isolation or desaturation recovery
Hypoxaemia algorithm with surgical communication lines
- FiO2 1.0 — “I’m treating desaturation.”
- Fibreoptic position check — “Confirming isolation device.”
- Suction
- PEEP to dependent lung
- CPAP/O2 to operative lung — “May partially inflate surgical field.”
- Recruitment of ventilated lung
- Intermittent two-lung ventilation if critical
- TIVA conversion; optimise CO and Hb; exclude pneumothorax
CPAP vs PEEP — get the side right
PEEP → ventilated dependent lung (FRC). Excess PEEP can divert blood to non-ventilated lung.
CPAP → non-ventilated operative lung (oxygenates shunt flow) but disturbs surgery.
Dependent-lung pneumothorax
Refractory hypoxaemia and rising pressures after central line attempts or surgical breach: consider pneumothorax of the ventilated lung — not solved by more OLV tricks alone.
[1]Analgesia interaction
Thoracic epidural/paravertebral for thoracotomy improves breathing postoperatively but intraoperative hypotension from epidural can lower mixed venous oxygen and worsen arterial hypoxaemia for a given shunt — support BP.
[1]Paediatric OLV note
Same shunt/HPV physiology; isolation often via blockers or endobronchial intubation rather than adult DLTs.
[1]Two-compartment mental model
Compartment A: ventilated dependent lung — aim for open alveoli without overdistension.
Compartment B: non-ventilated non-dependent lung — obligatory shunt pathway moderated by HPV and surgical compression.
Arterial oxygenation is the flow-weighted mix of content from A and B. Interventions either improve A, reduce flow through B, or oxygenate blood traversing B (CPAP/O2).
Cardiac output and mixed venous oxygen
Low cardiac output lowers mixed venous oxygen saturation; for any given shunt fraction, arterial hypoxaemia worsens. Support BP and output; treat bleeding; avoid profound hypovolaemia and overdose of negative inotropes. Anaemia reduces content — transfuse when clinically indicated.
[1]Volatile dose and TIVA conversion practicality
At modest volatile doses many patients oxygenate acceptably on OLV. When SpO2 is marginal after mechanical steps, reduce volatile and convert to propofol-based TIVA to spare HPV.[1] Do not climb volatile to “deepen” a hypoxic patient as the first response.
Lateral position logistics
Axillary roll, neck neutrality, eye/ear protection, invasive lines on accessible side, double check isolation after turning — most malpositions declare then. Surgeon flexion of the table can migrate tubes.
[1]When to abandon OLV temporarily
Critical SpO2 despite algorithm, myocardial ischaemia, right-heart strain, or surgical pause allowing reinflation — resume two-lung ventilation, recruit, then re-isolate when safe. Communicate clearly so the surgeon protects the field.
[1]Postoperative pulmonary complications link
Protective tidal volumes, limited pressures, fluid discipline, and good analgesia reduce PPC risk. OLV is a risk factor for lung injury if conducted with historical large tidal volumes — do not use 10 mL/kg “because one lung is down.”
[1]60-second algorithm recitation (memorise)
“FiO2 one hundred percent. Fibreoptic check. Suction. PEEP to the ventilated lung. CPAP or oxygen to the operative lung with surgical agreement. Recruit the ventilated lung. Intermittent two-lung ventilation if needed. Convert toward TIVA. Optimise cardiac output and haemoglobin. Exclude pneumothorax and equipment failure.”
[1]Common traps
Treating hypoxaemia with ever-higher volatile concentrations; forgetting fibreoptic check; applying CPAP to the wrong lung; using 10 mL/kg tidal volumes on one lung; missing that HPV takes time after isolation; ignoring low cardiac output.
[1]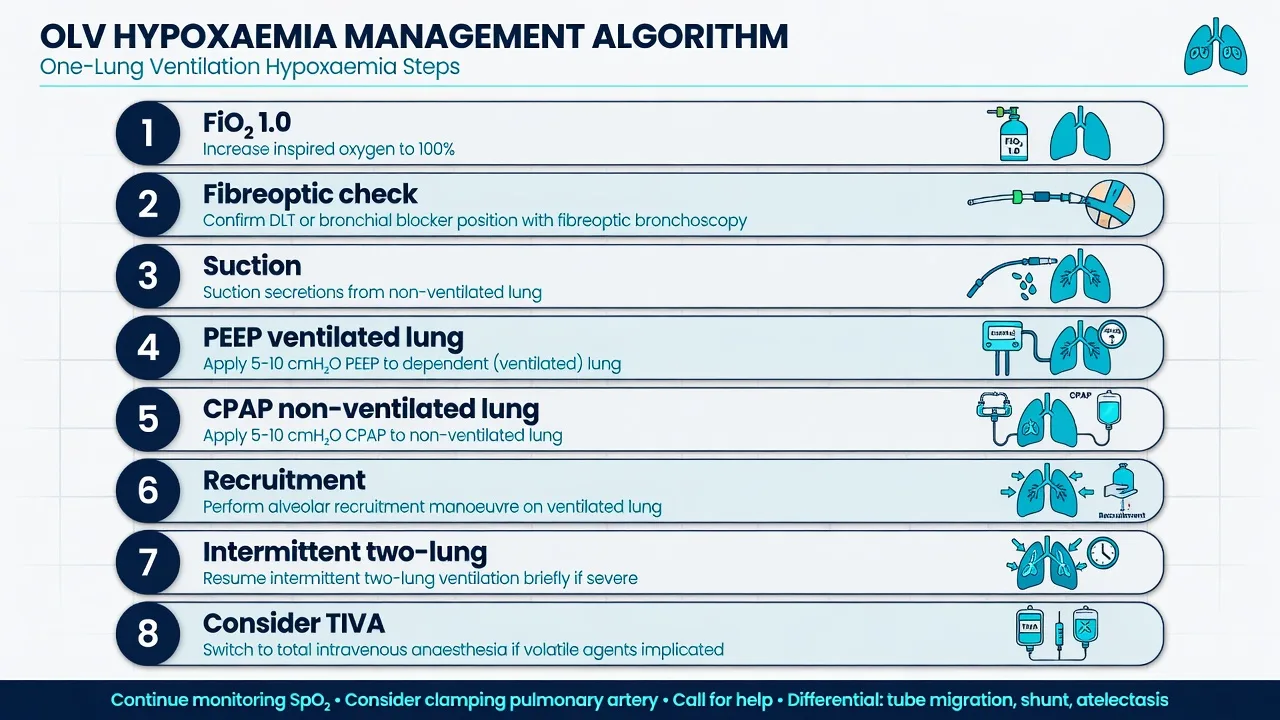
Fellowship consolidation — OLV physiology and hypoxaemia algorithm
[1]One-lung ventilation creates an obligatory true shunt through the non-ventilated lung. In the lateral position under anaesthesia, the non-dependent surgical lung is excluded from ventilation while still receiving blood flow until hypoxic pulmonary vasoconstriction and surgical manipulation reduce that flow.
[1]HPV is the pulmonary arterial response to low alveolar oxygen tension that diverts blood toward better oxygenated lung. Onset occurs within minutes with an early peak often described around 15 to 30 minutes. Volatile anaesthetics inhibit HPV in a dose-dependent fashion; many systemic pulmonary vasodilators also inhibit it; infected lung blunts it. Propofol-based TIVA relatively spares HPV and is a standard lever in refractory hypoxaemia.
[1]Other determinants of arterial oxygenation during OLV include cardiac output and mixed venous oxygen, haemoglobin concentration, dependent-lung atelectasis, secretions or blood, device malposition, and rare dependent pneumothorax. Low cardiac output worsens arterial hypoxaemia for any given shunt fraction.
[1]Protective OLV ventilation uses tidal volumes of 4 to 6 mL/kg predicted body weight, moderate PEEP to the ventilated lung individualised to avoid overdistension, high FiO2 at the onset of OLV then titration, rate adjusted for carbon dioxide with permissive hypercapnia when needed, and peak airway pressures preferably under about 35 cmH2O. Historical 10 mL/kg one-lung volumes are injurious and obsolete as routine practice.
[1]Hypoxaemia algorithm in order: raise FiO2 to 1.0; fibreoptic confirmation of DLT or blocker position; suction secretions or blood; apply PEEP to the ventilated lung; apply CPAP or oxygen insufflation to the non-ventilated lung with surgical agreement; recruit the ventilated lung; resume intermittent two-lung ventilation if critical; convert toward TIVA to spare HPV; optimise cardiac output and haemoglobin; exclude pneumothorax and equipment failure.
[1]PEEP acts on the ventilated dependent lung to improve FRC but excess PEEP can raise vascular resistance there and divert blood to the non-ventilated lung. CPAP acts on the non-ventilated operative lung to oxygenate shunted blood but may inflate the surgical field. Getting the side right is a pure pass-fail viva point.
[1]Left-sided DLT is usually preferred for isolation because of margin of safety; fibreoptic confirmation after turning lateral catches most malpositions. Anterior mediastinal mass collapse is a different crisis and should not be mismanaged as routine OLV hypoxaemia.
[1]A forty-five second viva script: FiO2 to one hundred percent, tell the surgeon, fibreoptic check, suction, moderate PEEP to the dependent lung, low-level CPAP to the operative lung if needed, recruit, intermittent two-lung ventilation if critical, switch toward TIVA, check blood pressure and haemoglobin, rule out dependent pneumothorax.
[1] [1]Physiology-to-action mapping table in prose
High shunt fraction from non-ventilated lung → reduce its blood flow with HPV and surgical compression, or oxygenate that blood with CPAP.
Dependent lung atelectasis → PEEP and recruitment of the ventilated lung.
Malposition → fibreoptic correction first.
Volatile inhibition of HPV → reduce volatile, convert to TIVA.
Low mixed venous oxygen from low cardiac output → support blood pressure and output.
Anaemia → consider transfusion.
Wrong diagnosis such as pneumothorax or mediastinal mass collapse → expand differential rather than stacking tidal volume.
Protective ventilation culture
OLV is not an excuse for injurious volumes. Use predicted body weight for tidal volume calculations, watch plateau and peak pressures, coordinate fluid therapy to avoid soggy dependent lungs, and plan analgesia that allows postoperative deep breathing. The same candidate who recites the hypoxaemia ladder should also refuse 10 mL/kg one-lung ventilation as routine.
[1]Integration with thoracic list planning
Discuss isolation device choice in the team brief, state expected difficult desaturation patients such as those with low preoperative SpO2 or significant contralateral disease, and ensure the fibreoptic scope works before induction. Hypoxaemia management is mostly preparation and algorithm discipline, not improvisation.
[1] [1]Full algorithm annotations with timing and communication
Step one, FiO2 to 1.0, is immediate and non-negotiable while you think. Tell the surgeon you are treating desaturation so surgical manipulation can pause if needed. Step two, fibreoptic check, is the discriminating move that separates protocolised care from panic pharmacology. Look for herniation, depth errors, and secretions. Step three, suction, clears reversible shunt and obstruction. Step four, PEEP to the ventilated lung, restores dependent FRC but should not be escalated blindly into overdistension. Step five, CPAP or oxygen to the operative lung, often dramatically raises SpO2 at the cost of a partially inflated surgical field — negotiate explicitly. Step six, recruitment of the ventilated lung, reverses atelectasis after isolation or after recovery from desaturation. Step seven, intermittent two-lung ventilation, is the safety valve when the patient is in danger. Step eight, TIVA conversion and optimisation of cardiac output and haemoglobin, addresses HPV inhibition and oxygen content and delivery. Throughout, keep peak pressures protective and remember that HPV takes minutes to mature after isolation, so very early desaturation is often position or device until proven otherwise.
[1]Annotating the algorithm this way in a viva sounds consultant-level because it pairs sequence with rationale and team communication rather than reciting a bare list.
[1] [1]Final synthesis and must-speak algorithm
OLV creates true shunt through the non-ventilated lung moderated by HPV over minutes. Protective settings are 4 to 6 mL/kg predicted body weight with preferably less than about 35 cmH2O peak pressure. Hypoxaemia ladder: FiO2 1.0, fibreoptic check, suction, PEEP to ventilated lung, CPAP or oxygen to non-ventilated lung, recruitment, intermittent two-lung ventilation, TIVA to spare HPV, optimise cardiac output and haemoglobin, exclude pneumothorax and equipment failure. PEEP is for the dependent ventilated lung; CPAP is for the operative non-ventilated lung. Fibreoptic confirmation is step two every time. That package is the entire topic distilled for the Final examiner.
[1] [1]Additional physiology vignettes
Vignette one: SpO2 falls to 88 percent two minutes after OLV begins. HPV has not fully matured and malposition is still likely. FiO2 to 1.0 and fibreoptic check beat starting multiple vasodilator discussions.
[1]Vignette two: SpO2 is 90 percent after thirty minutes of OLV with confirmed position. Dependent atelectasis and volatile HPV inhibition are plausible. Apply moderate PEEP, recruit, reduce volatile toward TIVA, and consider operative-lung CPAP with the surgeon.
[1]Vignette three: SpO2 collapses with rising peak pressure after central line attempt on the dependent side. Think pneumothorax of the ventilated lung and treat that differential rather than only climbing the standard OLV ladder.
[1]These vignettes keep the algorithm alive as clinical reasoning instead of a memorised shopping list.
[1] [1]Closing line for OLV hypoxaemia
Shunt through the non-ventilated lung is the central problem; HPV is the central defence; device position is the central fixable failure; and the stepwise ladder from FiO2 and fibreoptic check through PEEP, CPAP, recruitment, two-lung rescue, and TIVA is the central exam answer. Recite it in order every time and you will sound safe under pressure.
[1] [1]Extra examiner soundbites for OLV
"One-lung ventilation creates true shunt through the non-ventilated lung, moderated by hypoxic pulmonary vasoconstriction over minutes."
"Protective tidal volumes are 4 to 6 millilitres per kilogram predicted body weight."
"My hypoxaemia order is FiO2 to 1.0, fibreoptic check, suction, PEEP to the ventilated lung, CPAP to the non-ventilated lung, recruitment, intermittent two-lung ventilation if needed, then TIVA to spare HPV."
"PEEP belongs on the dependent ventilated lung; CPAP belongs on the operative non-ventilated lung."
"Volatiles inhibit HPV dose-dependently; when oxygenation is marginal I reduce volatile and convert toward propofol TIVA."
References
- [1]Licker M, Hagerman A, Jeleff A, Schorer R, Ellenberger C The hypoxic pulmonary vasoconstriction: From physiology to clinical application in thoracic surgery. Saudi Journal of Anaesthesia, 2021.PMID 34764832