Anaes · Paediatric anaesthesia
Paediatric emergence delirium and postoperative nausea and vomiting
Also known as Emergence agitation children · PAED score · Paediatric PONV · Dexmedetomidine emergence delirium
Fellowship-level coverage of paediatric emergence delirium versus pain, the PAED score, prevention (dexmedetomidine, propofol, TIVA), PACU management, and paediatric PONV risk, prophylaxis, and rescue with weight-based doses for ANZCA Final and allied exams.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Why this is examined / the one-line answer
Emergence delirium (ED) and paediatric postoperative nausea and vomiting (PONV) fill PACU bays, delay day-case discharge, frighten parents, and generate high-yield fellowship questions. The examiner is testing whether you can name the PAED items, separate ED from pain, give prevention doses, and build a paediatric PONV plan that does not simply copy adult Apfel habits or repeat the same antiemetic class at rescue.
[2]The one-line answer: I score thrashing children with PAED and a pain scale, treat pain first when FLACC is high, prevent high-risk sevoflurane preschool ENT cases with dexmedetomidine about 0.5 microg/kg or a propofol/TIVA strategy, and for PONV I risk-stratify, use multimodal receptor targets, and rescue with a different class.[1][3]
Keep ED conceptually separate from the neurotoxicity debate. The GAS trial is reassuring about neurodevelopment after brief infantile anaesthesia; it does not mean sevoflurane never causes emergence delirium in preschoolers.[4]
Definitions and differential diagnosis
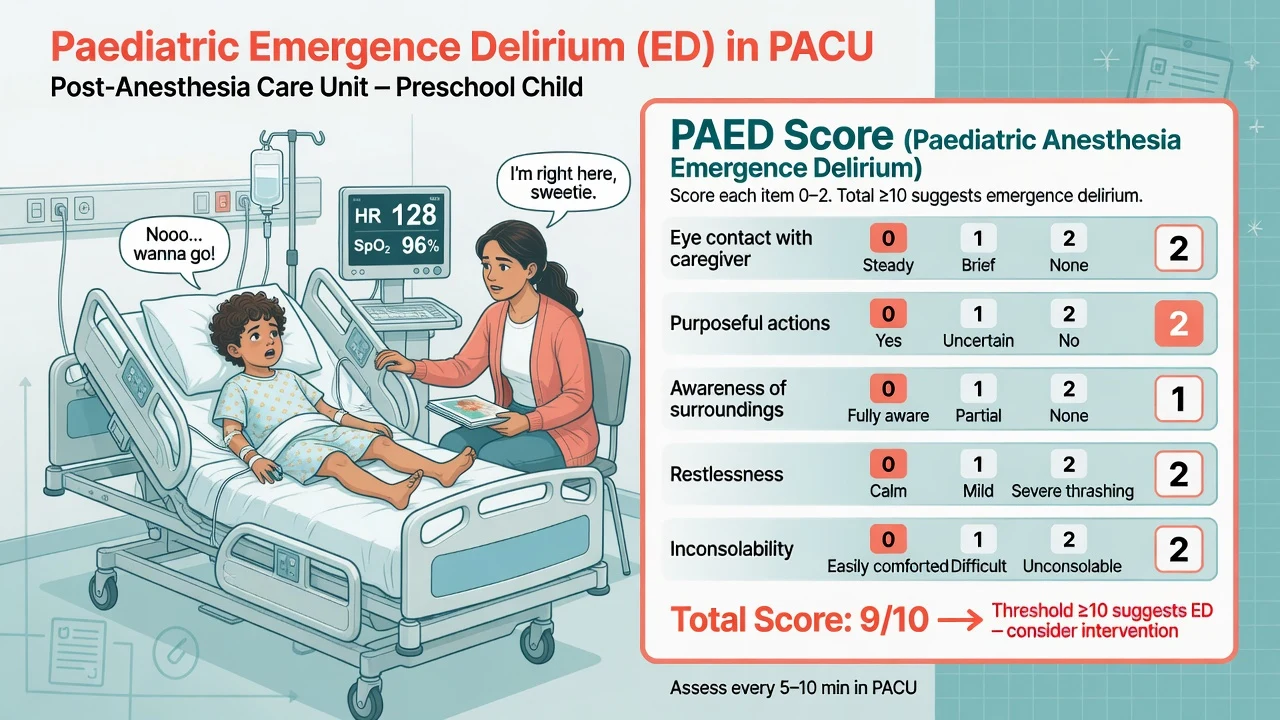
Emergence delirium is a disturbance of a child’s awareness of and attention to their environment, with disorientation and perceptual alterations, including hypersensitivity to stimuli and hyperactive motor behaviour in the immediate post-anaesthesia period.[1] Episodes are often brief (minutes to under thirty minutes) but can cause self-injury, intravenous line loss, surgical site disruption, and parental belief that “something is wrong with the brain.”
Differential of the thrashing child:
[1]| Pattern | Clues | First move |
|---|---|---|
| Pain | Localised guarding, high FLACC, improves with analgesia | Analgesia, examine site |
| ED | Non-purposeful thrashing, poor eye contact, inconsolable, modest FLACC | Calm bay, PAED score, small propofol/dex as protocol |
| Hypoxia / hypercarbia | Low SpO2, poor respiratory effort, obstruction | Airway manoeuvres, oxygen, support ventilation |
| Residual neuromuscular block | Weak grip, inadequate head lift, train-of-four | Reverse, support ventilation |
| Full bladder | Suprapubic mass, recent fluids, no void | Bladder empty |
| Hypoglycaemia | Infants, prolonged fasting, diabetes | Check glucose, treat |
| Seizure / neuro event | Asymmetry, prolonged, post-ictal | ABC, anticonvulsant pathway |
| Full-stomach retching / aspiration risk | Recent emergency, soiling | Lateral, suction, protect airway |
Never label all thrashing as delirium. Never treat all thrashing with more opioid.
[1]PAED score — exact components
The Pediatric Anesthesia Emergence Delirium (PAED) scale of Sikich and Lerman has five items, each scored 0–2 (higher = more abnormal):[1]
- Eye contact with the caregiver
- Purposeful actions
- Awareness of surroundings
- Restlessness
- Inconsolability
Total range 0–10. A score ≥10 suggests emergence delirium.
[1]Document the score when ED is suspected, treat, and rescore. PAED was developed as a research instrument with strong internal consistency; clinically it structures observation so that “agitated” becomes measurable. Use carers as the behavioural baseline in children with neurodevelopmental disorders.
[2]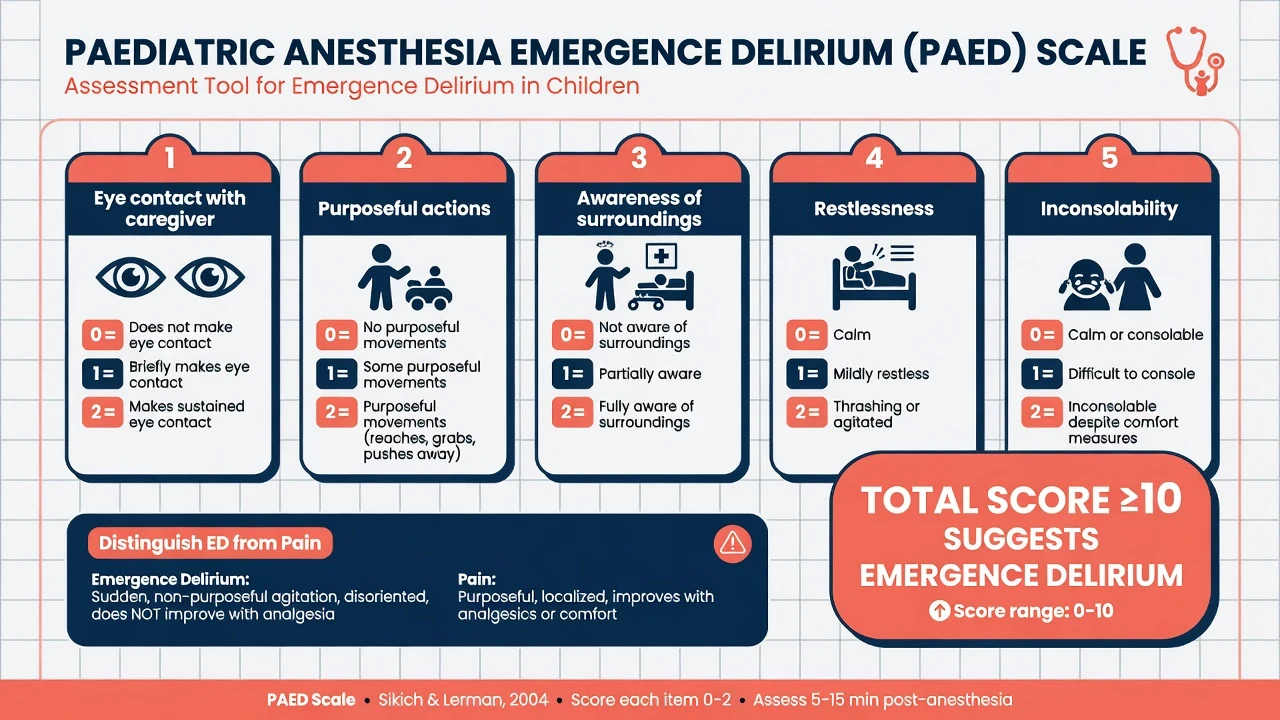
Risk factors for emergence delirium
Classic high-risk cluster:
[1]- Preschool age (about 2–5 years)
- Sevoflurane or desflurane maintenance (rapid recovery profile)
- ENT, ophthalmology, and short painful procedures
- Preoperative child or parental anxiety
- Previous ED
- Rapid emergence without analgesia or sedative bridge
- Possibly male sex and certain temperaments (weaker, less examinable)
IV induction and propofol TIVA are associated with lower ED rates than pure sevoflurane techniques. Regional analgesia and good multimodal pain control reduce the pain confounder. Premedication policies vary; avoid oversedating children with obstructive sleep apnoea.
[1]Pathophysiology sketch (viva depth, not speculation)
ED associates with rapid emergence from low-solubility volatiles, immature prefrontal control networks in preschoolers, anxiety, and pain. ENT and eye surgery combine sensory stimulation with volatile techniques and the preschool demographic. Propofol and alpha-2 agonists alter recovery trajectory and anxiolysis. Exact cellular mechanisms remain incompletely mapped — examiners prefer risk factors, scores, and management over speculative neurochemistry.[1]
Prevention strategies
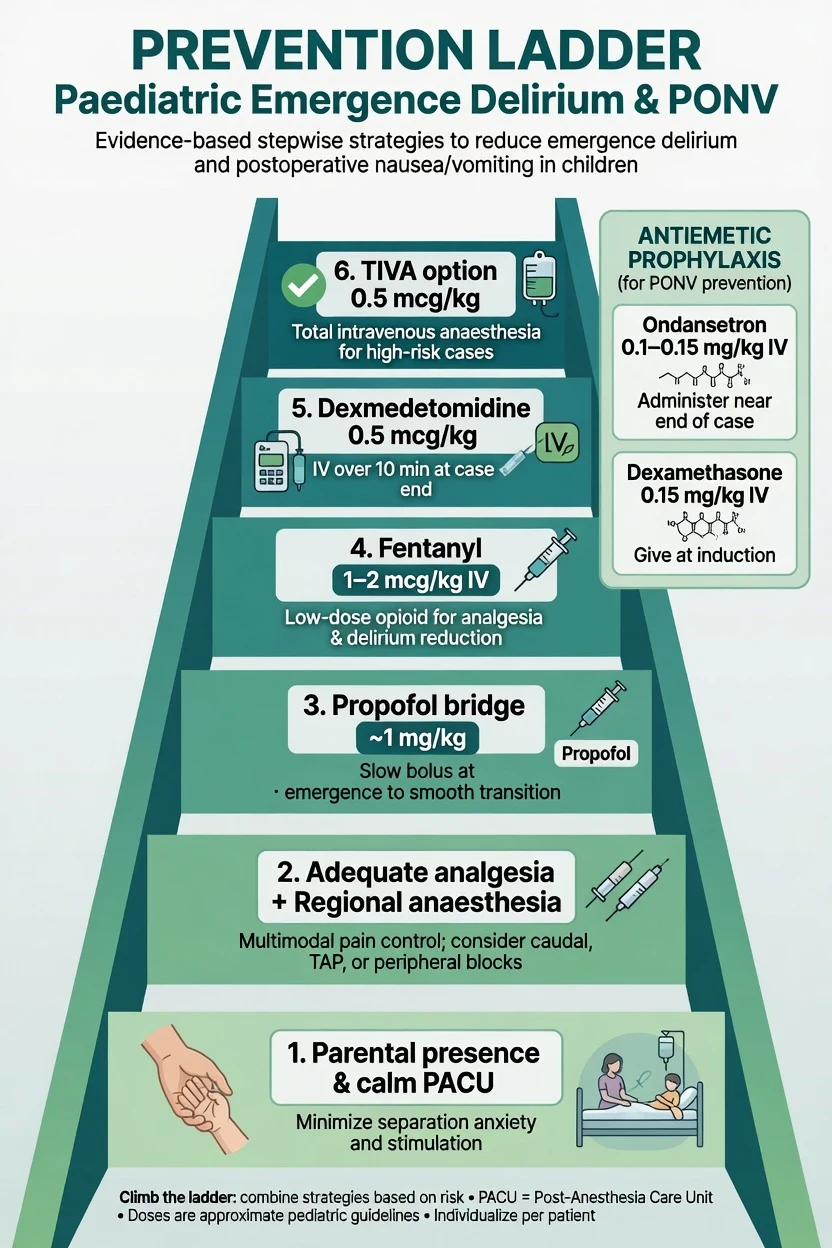
[1]Evidence synthesis supports intraoperative dexmedetomidine around 0.5 microg/kg IV (often after induction, given slowly) reducing ED with an acceptable recovery profile when dosed thoughtfully.[3] Avoid large rapid boluses in hypovolaemic or significant cardiac disease. Combine with analgesia — dexmedetomidine is not a substitute for a blocked caudal that has worn off.
Propofol bridge: after sevoflurane maintenance, ~1 mg/kg near the end can reduce ED at the cost of slightly longer wake-up. Useful when dexmedetomidine is undesirable. Watch airway obstruction in OSA and post-tonsillectomy patients.
[3]Management of established ED
- Protect the airway, oxygen saturation, and intravenous access; prevent falls and self-injury.
- Exclude hypoxia, hypercarbia, hypoglycaemia, full bladder, residual neuromuscular block, and surgical complication.
- Score PAED and pain (FLACC/FACES as age-appropriate).
- Treat pain first if pain is plausible.
- If pure ED (PAED ≥10, pain controlled): calm environment, parental presence when safe, small propofol boluses (0.5–1 mg/kg) or unit-protocol dexmedetomidine under monitoring.
- Avoid stacking sedatives in OSA without extended observation.
- Document duration and response; counsel parents that ED is usually self-limiting and distinct from long-term neurodevelopmental injury questions answered by GAS for brief exposures.[4]
Paediatric PONV
Risk thinking
Adult Apfel simplified score (female sex, non-smoker, history of PONV or motion sickness, postoperative opioids) remains the conceptual skeleton for receptor-based thinking.[2] Paediatric modelling differs: age (infants often lower risk than school-age for some contexts), strabismus, adenotonsillectomy, middle ear surgery, long laparoscopy, volatile agents, opioids, motion sickness history, hydration, and duration. Do not give identical triple prophylaxis to every hernia repair.
High-risk paediatric surgeries: strabismus, adenotonsillectomy, middle ear, long laparoscopic procedures, opioid-heavy techniques.
[2]Prophylaxis principles
- Risk-stratify.
- Reduce baseline risk: TIVA where suitable, multimodal opioid-sparing analgesia, adequate hydration, gentle suction of gastric air after mask ventilation when appropriate.
- Multimodal receptors when risk is high.
- Rescue with a different class from prophylaxis.
Exam-ready doses
| Drug | Typical paediatric teaching dose | Notes |
|---|---|---|
| Ondansetron | 0.1–0.15 mg/kg IV (max often 4 mg) | 5-HT3 antagonist |
| Dexamethasone | 0.15 mg/kg IV (max often 4–8 mg by indication) | Also analgesic adjunct in tonsillectomy pathways |
| Droperidol | 10–15 microg/kg IV | QT caution; institutional use varies |
| Dexmedetomidine (ED) | 0.5 microg/kg IV | Not primarily an antiemetic |
| Propofol rescue (ED) | 0.5–1 mg/kg IV | Monitoring required |
NK1 antagonists appear in some high-risk adult and selected paediatric pathways where available. Metoclopramide has limited paediatric popularity for routine prophylaxis compared with ondansetron/dexamethasone combinations.
[1]Classic trap: giving ondansetron for prophylaxis and again for rescue. Switch class (for example add droperidol or dexamethasone if not already given, per local formulary and contraindications).[2]
Integrated day-case ENT pathway
- Identify preschool + sevoflurane + ENT risk for ED and high PONV risk.
- Multimodal analgesia; avoid codeine after tonsillectomy (see analgesia topic).
- Dual antiemetic prophylaxis common (ondansetron + dexamethasone) when risk high.
- Consider dexmedetomidine 0.5 microg/kg or propofol strategy for ED prevention.
- PACU: quiet bay, parental presence early when safe.
- Score FLACC and PAED.
- Treat pain first if indicated; pure ED gets small propofol.
- Antiemetic rescue with new class if vomiting.
- Discharge only when alert or at baseline, pain controlled, no active vomiting, SpO2 stable on air (or baseline oxygen), parents understand ED may briefly recur on transfer.
Special populations
- OSA after tonsillectomy: ED + PONV + obstruction triangle — minimise sedative stacking; longer observation.
- Neurodevelopmental disorders: baseline behaviours confuse scoring — use carers; quiet environment.
- Strabismus: very high PONV risk — dual or triple prophylaxis common.
- MRI under GA: low pain, volatile still may cause ED — TIVA attractive.
- Emergency full stomach: ED management remains secondary to aspiration risk and airway protection.
- Cardiac children: titrate dexmedetomidine cautiously (bradycardia, systemic vascular resistance changes).
Parental counselling language
“Some preschool children wake confused and thrashing after anaesthetic gases. It usually lasts minutes. We score it, treat pain if present, and may give a short-acting medicine to calm the phase. It is not the same question as long-term development after brief anaesthesia, which studies like GAS have been reassuring about.”[4]
Written discharge advice: when to give next analgesics, maximum daily paracetamol, red flags (sedation, snoring pauses, persistent vomiting, bleeding after tonsillectomy), and who to call.
[2]Monitoring and disposition
- Continuous SpO2 until awake and settled.
- Document PAED and pain scores when thrashing occurs.
- Record antiemetics given and plan the rescue class in advance.
- Unplanned admission criteria: unresolved ED with safety risk, persistent vomiting with dehydration risk, hypoxia, bleeding, or inadequate pain control.
- Handover must mention both ED risk and PONV prophylaxis already given so the ward does not repeat ondansetron blindly.
Quality improvement hooks
Track ED rates by case mix and volatile versus TIVA; percentage of thrashing children with documented PAED/FLACC; antiemetic rescue class concordance; unplanned admissions for vomiting; parental complaint themes. Simulation of thrashing-child differentials for rotating trainees prevents opioid-only habits.
[2]Regional notes
ANZ / UK: PAED score expected by name; dexmedetomidine widely available; APAGBI-aligned paediatric practice.
US / Canada: similar pharmacology; institutional ED protocols common; Apfel still taught as adult skeleton.
India / resource-variable: same scores and differentials; drug availability for NK1 or dexmedetomidine varies — propofol bridge and multimodal analgesia remain universal tools.
SAQ answer scaffold
- Define ED and list differentials including pain and hypoxia.
- Reproduce PAED five items and ≥10 threshold.
- List risk factors and prevention with exact doses.
- PACU management algorithm.
- Paediatric PONV risk factors versus adult Apfel.
- Prophylaxis doses and class-switched rescue.
- Special notes for tonsillectomy/OSA and strabismus.
Viva stem bank with model outlines
Stem 1: “This 3-year-old is thrashing after sevoflurane ENT — differential?”
Outline: pain vs ED vs hypoxia vs residual paralysis vs bladder vs hypoglycaemia; score FLACC and PAED; ABC first.
Stem 2: “Score this child with PAED.”
Outline: name five items, each 0–2, total ≥10 suggests ED.[1]
Stem 3: “Would you give dexmedetomidine? Dose and side effects?”
Outline: ~0.5 microg/kg IV slow after induction for prevention; bradycardia, hypotension, possible longer recovery; not instead of analgesia.[3]
Stem 4: “How does your PONV plan differ from an adult Apfel-4 patient?”
Outline: paediatric surgical risks (strabismus, tonsils), weight-based doses, still multimodal receptors, still different-class rescue; Apfel skeleton for thinking not verbatim scoring.[2]
Stem 5: “Prophylactic ondansetron given — now vomiting in PACU.”
Outline: do not repeat ondansetron as sole rescue; add different class; check opioids, hydration, surgical cause.
Stem 6: “Parents ask if the thrashing means brain damage.”
Outline: usually brief ED; distinct from neurotoxicity literature; GAS reassuring for brief infant exposure neurodevelopment; document and comfort.[4]
Common traps
- Calling all agitation ED without scoring pain.
- Forgetting the five PAED items or the ≥10 threshold.
- Repeating ondansetron for rescue after ondansetron prophylaxis.
- Over-sedating OSA children to “treat ED.”
- Promising zero ED risk with any single drug.
- Confusing ED prevention with the neurotoxicity debate.
- Discharging while still thrashing or actively vomiting.
- Using adult fixed antiemetic doses without mg/kg thinking.
Examiner mental map — fifteen dimensions
- ED definition.
- Differential of thrashing.
- PAED five items.
- Threshold ≥10.
- Risk cluster (preschool, sevo, ENT).
- Dexmedetomidine 0.5 microg/kg.
- Propofol bridge ~1 mg/kg.
- TIVA vs volatile.
- Pain-first rule.
- Established ED algorithm.
- Paediatric PONV risk modifiers.
- Ondansetron and dexamethasone mg/kg.
- Different-class rescue.
- OSA/tonsillectomy cautions.
- GAS vs ED conceptual split.
Pathophysiology, scoring psychometrics, and service design
Emergence delirium clusters where rapid recovery from low-solubility volatiles meets immature cortical control networks in preschool children, often after stimulating ENT or eye surgery. Preoperative anxiety in child and parent raises risk. Pain amplifies agitation and confounds diagnosis, which is why simultaneous FLACC and PAED scoring is more than bureaucracy. The original PAED psychometric work demonstrated strong internal consistency and provided a shared language for research and clinical communication; the operational threshold of 10 or more remains the number examiners expect.
[1]Service design reduces ED without exotic pharmacology alone. Quiet induction and recovery spaces, parental presence policies that are child-centred rather than dogmatic, adequate local anaesthesia by surgeons, and avoiding abrupt volatile cessation without an analgesic or sedative bridge all matter. Units that audit ED rates in preschool sevoflurane ENT lists and feed results back to trainees improve faster than units that treat thrashing as inevitable personality.
[4]PONV service design is equally structured. Risk-stratify rather than give identical triple prophylaxis to every child. Prefer multimodal receptor coverage in high-risk strabismus and adenotonsillectomy pathways. Ensure rescue algorithms specify a different class. Track unplanned admissions for vomiting and rescue class errors. Pair antiemetic planning with opioid-sparing multimodal analgesia because postoperative opioids are a major modifiable risk factor.
[2]Finally, separate three parental fears that often arrive together: thrashing on wake-up, vomiting, and brain damage from anaesthetic. Answer each on its own evidence: ED is usually brief and scored; PONV is preventable and treatable with receptor logic; neurodevelopment after brief single exposure is addressed by GAS-context reassurance and is not the same phenomenon as PACU agitation.
[4] [1]Comprehensive exam revision sheet — ED and PONV
Exact numbers and scores
- PAED: five items, each 0 to 2, total 0 to 10, threshold greater than or equal to 10 suggests ED
- FLACC: Face Legs Activity Cry Consolability, each 0 to 2, total 0 to 10 for pain
- Dexmedetomidine prevention: about 0.5 micrograms per kilogram IV
- Propofol bridge or rescue: 0.5 to 1 mg/kg IV
- Fentanyl: 1 to 2 micrograms per kilogram IV
- Ondansetron: 0.1 to 0.15 mg/kg IV, maximum often 4 mg
- Dexamethasone: 0.15 mg/kg IV, maximum often 4 to 8 mg depending on indication
- Droperidol: 10 to 15 micrograms per kilogram IV with QT caution where used
Differential of thrashing in one minute
Hypoxia, hypercarbia, pain, ED, full bladder, residual neuromuscular blockade, hypoglycaemia, seizure, uncomfortable cast or dressing, full stomach retching. Airway and oxygen first. Score pain and ED second. Treat the dominant diagnosis third.
Prevention sentence for the examiner
"For a high-risk preschool ENT case under sevoflurane I would ensure adequate analgesia and local techniques, consider dexmedetomidine 0.5 micrograms per kilogram after induction or a propofol bridge at the end, plan dual antiemetic prophylaxis if PONV risk is high, and recover in a calm bay with parental presence when safe."
Rescue sentence for the examiner
"If PAED is 10 or more and pain scores are low I protect the airway, calm the environment, and give propofol 0.5 to 1 mg/kg under monitoring rather than stacking opioids. If vomiting follows ondansetron and dexamethasone prophylaxis I rescue with a different receptor class and reassess hydration and surgical causes."
[2]What not to say
Do not call all thrashing ED without scoring. Do not promise zero ED risk with any single drug. Do not discharge an actively vomiting or hypoxic child. Do not equate PACU thrashing with long-term neurotoxicity. Do not repeat the same antiemetic class for rescue after it already failed as prophylaxis.
Cross-links
See paediatric analgesia for FLACC detail and codeine contraindications after tonsillectomy. See neurotoxicity topic for GAS-context parental questions that often arise while the child is thrashing in PACU. See induction techniques for volatile versus TIVA choices that change baseline ED risk.
Final synthesis
ED and PONV are high-frequency PACU problems with high-yield exam numbers. Master PAED, a short prevention list with doses, a pain-versus-ED algorithm, and receptor-based PONV prophylaxis with class-switched rescue. That package passes almost every stem built on the thrashing or vomiting child.
[1]Additional worked PACU dialogues
Parent: "Is my child brain damaged?"
Answer: "What you are seeing is usually emergence delirium, a short-lived confused wake-up that we score and treat. It is different from the long-term development question. For a brief anaesthetic, the best human studies are reassuring about later intelligence. Right now our job is oxygen, comfort, and calm recovery."
Surgeon: "Can we discharge?"
Answer: "Not while thrashing, hypoxic, or actively vomiting. Once behaviour is near baseline, pain is controlled, and SpO2 is stable, day-case discharge can proceed with written analgesia and antiemetic advice."
Nurse: "Shall I give more morphine? FLACC is 2 but the child is screaming."
Answer: "Score PAED as well. If this is pure ED, a small propofol dose under monitoring is more appropriate than stacking opioid into a low pain score, especially after tonsillectomy with OSA risk."
These dialogues convert scores and doses into communication behaviours examiners love.
[1] [1]Closing clinical pearls for ED and PONV mastery
Treat every thrashing child as a structured diagnostic problem rather than a single drug opportunity. Protect the airway, measure SpO2, score FLACC and PAED, and only then choose analgesia versus sedative rescue. In high-risk preschool sevoflurane ENT surgery, prevent with dexmedetomidine or a propofol bridge and plan antiemetics as deliberately as you plan the airway. In PACU, class-switch antiemetic rescue and never discharge unresolved agitation or active vomiting. Parents need plain language that distinguishes brief emergence delirium from long-term neurodevelopmental questions. If you can do those things fluently, this topic is under control for ANZCA Final and allied fellowship exams.
[3]Bottom line for the Final Exam
Paediatric recovery passes when you sound like the PACU consultant: score before you sedate, treat pain before you label delirium, prevent the preschool sevoflurane ENT storm with a plan rather than hope, and never rescue PONV with the same receptor you already blocked. PAED ≥10, dexmedetomidine 0.5 microg/kg, ondansetron 0.1–0.15 mg/kg, different-class rescue — those numbers, spoken cleanly, carry the viva.
[3]References
- [1]Sikich N, Lerman J. Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology, 2004.PMID 15114210
- [2]Apfel CC et al. A simplified risk score for predicting postoperative nausea and vomiting. Anesthesiology, 1999.PMID 10485781
- [3]Manning AN et al. Dexmedetomidine dosing to prevent pediatric emergence delirium. AANA Journal, 2020.PMID 32990204
- [4]Davidson AJ et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS): an international multicentre, randomised controlled trial. Lancet, 2016.PMID 26507180