Anaes · Paediatric anaesthesia
Paediatric fluids, fasting, and glucose: Holliday-Segar and safe maintenance
Also known as Holliday-Segar · Paediatric maintenance fluids · Paediatric fasting guidelines
Exact Holliday-Segar 4-2-1 maintenance, AAP isotonic maintenance guidance, perioperative fasting including liberalised clear fluids, glucose monitoring in infants, and prevention of hospital-acquired hyponatraemia for fellowship exams.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Why this is examined
Fluid calculation errors harm children. Examiners demand the exact Holliday-Segar formula, the modern isotonic maintenance message (AAP 2018), and contemporary fasting times including liberalised clear fluids in many paediatric centres.[1][2] SAQs almost always want arithmetic shown.
Holliday-Segar maintenance — exact formula
4-2-1 hourly maintenance
Daily equivalent (original framing): 100 mL/kg/day first 10 kg + 50 mL/kg/day next 10 kg + 20 mL/kg/day thereafter.[1]
Worked examples (memorise the pattern)
| Weight | Hourly calculation | Rate |
|---|---|---|
| 5 kg | 5 × 4 | 20 mL/h |
| 10 kg | 10 × 4 | 40 mL/h |
| 15 kg | 40 + (5 × 2) | 50 mL/h |
| 20 kg | 40 + 20 | 60 mL/h |
| 30 kg | 40 + 20 + 10 | 70 mL/h |
| 40 kg | 40 + 20 + 20 | 80 mL/h |
Show the working in SAQs; bare numbers without arithmetic lose marks.
[2]What Holliday-Segar is — and is not
It estimates maintenance free-water need related to metabolic rate. It is not a resuscitation formula, not a blood-loss replacement formula, and not a licence to give hypotonic saline. Composition of the fluid is a separate decision from volume rate.
[1]Which fluid? Isotonic maintenance
Why hypotonic fluids became dangerous perioperatively
Non-osmotic ADH release (pain, stress, nausea, volume stimuli, pulmonary/CNS disease) impairs free-water excretion. Hypotonic maintenance then dilutes plasma sodium → hospital-acquired hyponatraemia → encephalopathy and seizures. Classic wrong fluid: 0.18% saline with dextrose as “routine maintenance.”
[2]Practical perioperative choices (ANZ-friendly phrasing)
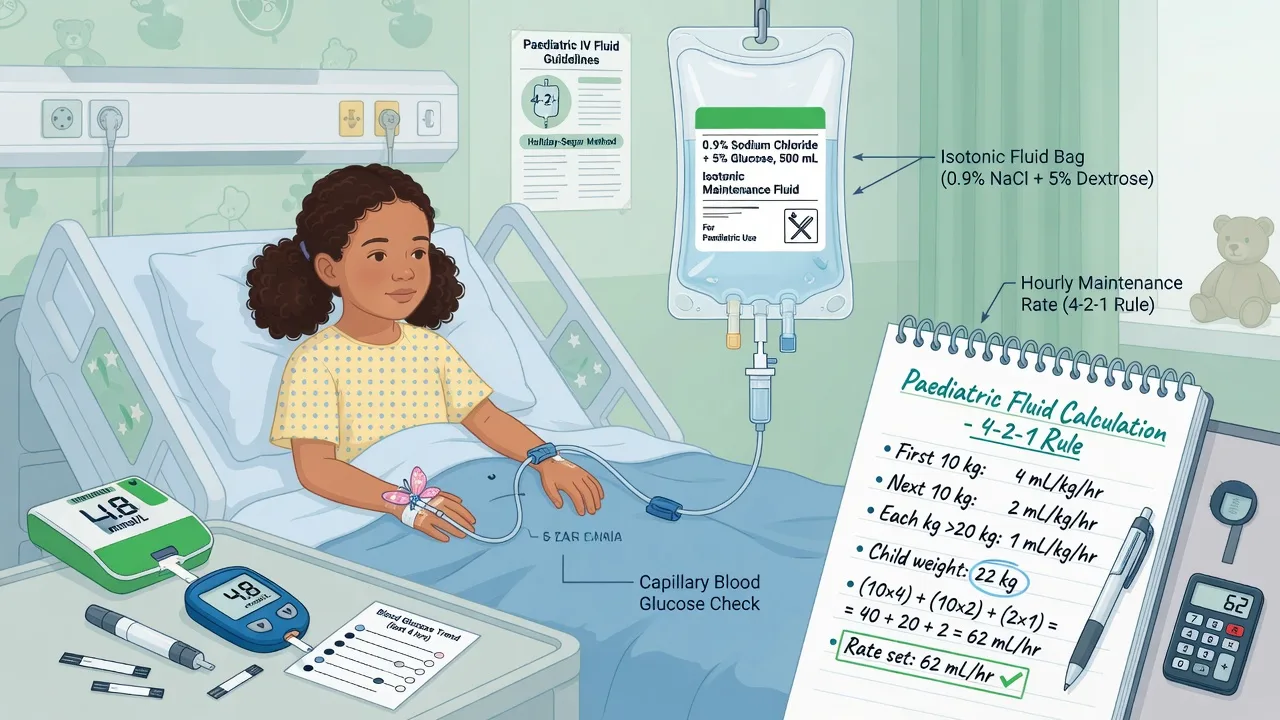
- Maintenance: isotonic balanced crystalloid (e.g. Plasma-Lyte 148) or 0.9% sodium chloride, with glucose added when indicated (especially neonates/infants), and potassium once urine output confirmed and local protocol allows.
- Resuscitation boluses: isotonic crystalloid 10–20 mL/kg, reassess; blood products when haemorrhage is the problem.
- Ongoing losses: replace like-for-like thinking (e.g. gastric losses) under specialist guidance.
- Exceptions needing specialist fluid recipes: renal disease, severe cardiac disease, neurosurgical hyponatraemia risk patterns, diabetic ketoacidosis protocols, NICU-specific recipes — do not force a single bag type on every neonate without unit advice.
Deficit, maintenance, and replacement structure
- Resuscitate shock with isotonic boluses.
- Estimate deficit (clinical dehydration grade × weight) and replace over a protocolised period with isotonic fluid (classic teaching often over 24–48 h depending on severity — follow local paediatric guidelines).
- Add maintenance at Holliday-Segar rate (may reduce if overloaded or SIADH risk).
- Replace ongoing losses separately.
- Monitor sodium, potassium, glucose, fluid balance, weight.
Perioperative “deficit from fasting” is often modest if clear fluids were allowed recently; do not automatically dump large “NPO deficit” volumes into every well child for a short case.
[2]Fasting guidelines
Many paediatric societies and centres now allow clear fluids up to one or two hours pre-op to reduce dehydration, ketosis, irritability, and hypotension at induction while maintaining safety. Confirm local APAGBI / institutional guidance — quote the principle and the need to follow local protocol in the viva. Do not extend clear-fluid fasting accidentally on emergency lists when sips of water would be allowed.
[2]Glucose
Neonates and small infants have limited glycogen. Prolonged fasting or surgical stress causes hypoglycaemia (jitteriness, lethargy, seizures, or subtle tone changes) or stress hyperglycaemia. Check glucose perioperatively in:
[3]- neonates and young infants
- prolonged cases / prolonged fasting
- liver disease, inborn errors (specialist)
- critically ill children
- mothers with diabetes (neonates)
Include dextrose in maintenance when indicated; treat confirmed hypoglycaemia with protocolised glucose boluses (e.g. 2–5 mL/kg of 10% dextrose depending on age/protocol — use local paediatric emergency dosing) and recheck.
[2]Scenario matrix
[2]Apnoea risk after anaesthesia in ex-preterms is not a fluid formula issue, but the same patients need glucose attention and monitoring plans.[3] Developmental outcome trials such as GAS sit in the same age band but do not dictate fluid composition.[4]
SAQ answer scaffold
- Write 4-2-1 with a worked example for the stem weight.[1]
- Specify isotonic maintenance and why (ADH, hyponatraemia; AAP).[2]
- State bolus volume for shock and reassessment.
- List fasting times including liberalised clears.
- State glucose monitoring plan for infants.
Viva stem bank
- “Calculate maintenance for an 18 kg child.”
- “Why not 0.18% saline postoperatively?”
- “What is your fasting advice for clear fluids in a 4-year-old?”
- Model phrase: “Volume by Holliday-Segar; composition isotonic with glucose as indicated; never hypotonic maintenance by default.”
Deficit arithmetic (classic exam structure)
For a dehydrated child, many paediatric protocols still teach:
[2]- Estimate % dehydration clinically (mild/moderate/severe).
- Deficit (mL) ≈ % dehydration × weight (kg) × 10.
- Resuscitate shock first with isotonic boluses.
- Replace remaining deficit over a protocolised period with isotonic fluid.
- Add Holliday-Segar maintenance.
- Add ongoing losses.
Example structure (illustrative): 12 kg child, 5% dehydrated → deficit ~600 mL. After any boluses already given, replace residual deficit plus maintenance (~44 mL/h by 4-2-1) per local timing rules. Always recheck sodium if hyponatraemia or hypernatraemia is present — replacement rate changes in sodium disorders.
[2]Perioperative fluid plan for a typical list
Short ear tube case, 18 kg, clear fluids 90 minutes ago: often no large deficit; consider free IV or maintenance only if delayed; avoid routine large “NPO catch-up.”
[2]Infant inguinal hernia, 5 kg, breast milk 5 hours ago: start isotonic fluid with glucose, check glucose, keep case short, plan postoperative feeding early if appropriate.
[3]Perforated appendicitis, 30 kg, septic: 10–20 mL/kg isotonic boluses with reassessment, antibiotics, maintenance isotonic, monitor lactate and urine, consider blood if bleeding/anaemia.
[1]Regional guideline framing
- AAP 2018 (US): isotonic maintenance 28 days–18 years.[2]
- ANZ / RCH-style practice: isotonic balanced solutions common (Plasma-Lyte); local fluid monographs rule.
- UK / NICE and paediatric society fasting updates: many centres liberalise clear fluids to 1 hour — quote local policy in the exam.
Never present one country’s protocol as universal without naming it.
[2]Hyponatraemia crisis recognition
Headache, nausea, seizures, reduced consciousness postoperatively after hypotonic fluids = emergency. Stop free water, call for help, ABC, check sodium, treat per paediatric hyponatraemic encephalopathy protocols (hypertonic saline pathways under senior guidance). Prevention is better than treatment: isotonic maintenance.
[2]Holliday-Segar mastery — more worked examples
Hourly 4-2-1 method:[1]
- 8 kg: 8 × 4 = 32 mL/h
- 12 kg: 40 + (2 × 2) = 44 mL/h
- 18 kg: 40 + (8 × 2) = 56 mL/h
- 22 kg: 40 + 20 + 2 = 62 mL/h
- 35 kg: 40 + 20 + 15 = 75 mL/h
Daily method cross-check for 18 kg: 1000 mL (first 10 kg) + 400 mL (next 8 kg) = 1400 mL/day ≈ 58 mL/h (rounding differences are acceptable if method is shown).
[2]Always show working in SAQs. State explicitly that Holliday-Segar is maintenance, not resuscitation.
[2]Isotonic maintenance — physiology of the recommendation
The AAP 2018 guideline recommends isotonic maintenance fluids with appropriate potassium and dextrose for children 28 days to 18 years needing IV maintenance, to reduce hospital-acquired hyponatraemia.[2] Perioperative ADH release from stress, pain, nausea, volume stimuli, and pulmonary or CNS disease impairs free-water excretion. Hypotonic fluids (historically 0.18% saline with dextrose) then generate hyponatraemia that can cause encephalopathy and seizures. Exam phrase: “Volume by Holliday-Segar; composition isotonic; glucose as indicated.”
Resuscitation versus maintenance versus deficit
| Purpose | Fluid type | Typical approach |
|---|---|---|
| Shock resuscitation | Isotonic crystalloid | 10–20 mL/kg boluses with reassessment |
| Maintenance | Isotonic + glucose when needed | 4-2-1 rate (may reduce if SIADH risk) |
| Deficit replacement | Isotonic | Estimate % dehydration × weight × 10 mL; replace per protocol after shock fixed |
| Ongoing losses | Match losses | NG, drains, third space — specialist recipes when complex |
| Blood loss | Blood products | Do not replace haemorrhage with free water |
Deficit arithmetic worked example
Child 14 kg, clinically 5% dehydrated:
[2]- Deficit ≈ 5 × 14 × 10 = 700 mL
- Maintenance ≈ 40 + 8 = 48 mL/h by 4-2-1
- If shocked, give isotonic boluses first; subtract boluses from remaining deficit plan
- Recheck sodium if hyper- or hyponatraemic — replacement rate changes in sodium disorders
Fasting guidelines — liberal clear fluids
Many paediatric centres allow clear fluids up to one or two hours preoperatively to reduce dehydration, ketosis, hypotension at induction, and distress. Typical teaching times:
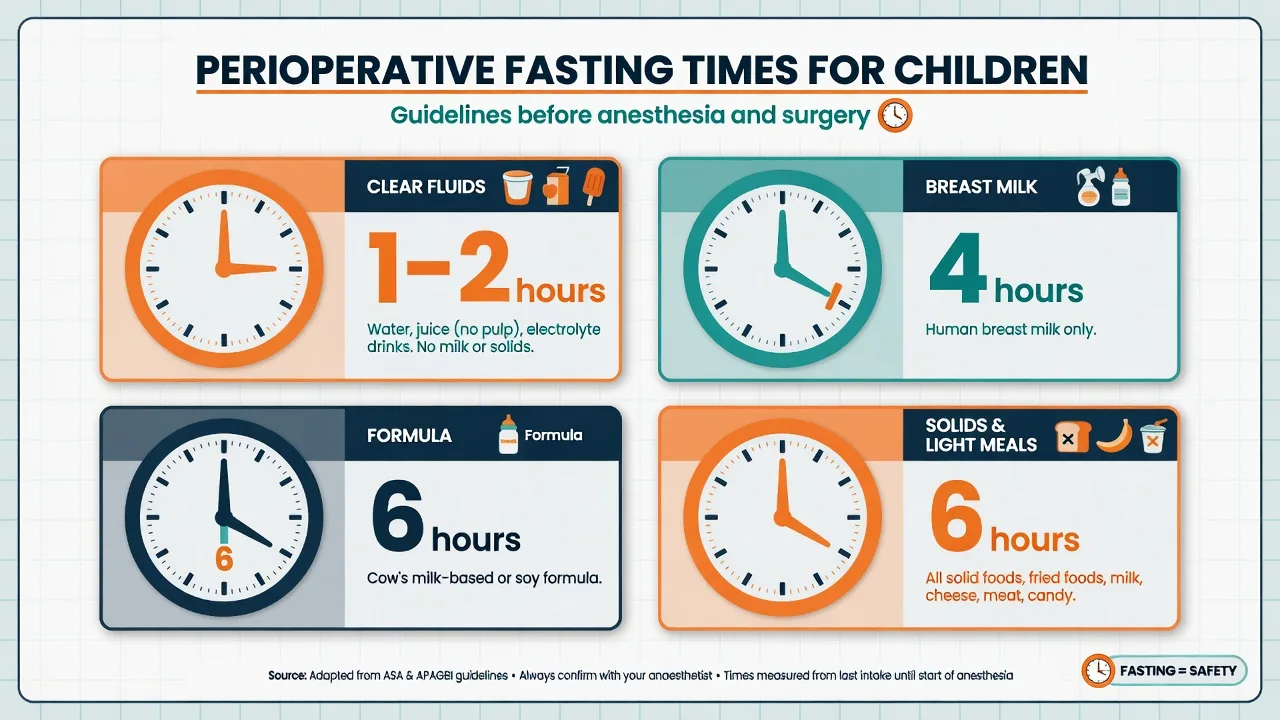
[2]- Clear fluids: 1–2 h (local policy)
- Breast milk: 4 h
- Formula / light meal: 6 h
- Heavy/fatty solids: 6–8 h
In viva, name the principle and commit to local APAGBI/institutional policy rather than fighting the examiner over a single international number. Do not accidentally impose six-hour clear-fluid starvation on a delayed list when sips of water are allowed.
[2]Glucose — recognition and treatment
Neonates and small infants have limited glycogen. Hypoglycaemia may present with jitteriness, lethargy, seizures, apnoea, or subtle tone changes — or be silent until checked. Check glucose in neonates, prolonged fasts, liver disease, critically ill children, and infants of diabetic mothers. Treat with protocolised dextrose (commonly 2–5 mL/kg of 10% dextrose depending on age/protocol) and recheck. Include dextrose in maintenance when indicated rather than running plain saline for hours in a neonate.
[2]Scenario playbooks
Well child, short myringotomy, clear fluids 90 minutes ago: minimal deficit; avoid automatic large NPO catch-up volumes.
Infant hernia, prolonged wait: isotonic fluid with glucose; check glucose; keep opioid-sparing.
Pyloric stenosis: correct dehydration and electrolytes before elective GA; chloride and base deficit matter; specialist fluid recipes.
DKA: follow DKA protocol — not routine Holliday-Segar alone.
Raised ICP risk: avoid hypotonic free water.
Cardiac failure: restricted fluids, specialist titration.
Ex-preterm: glucose plus apnoea monitoring plan coexist.[3]
Hyponatraemic encephalopathy emergency
Postoperative seizure or reduced consciousness after hypotonic fluids is an emergency. Stop free water sources, ABC, check sodium urgently, call for senior help, and treat per paediatric hyponatraemic encephalopathy protocols (hypertonic saline pathways under specialist guidance). Prevention with isotonic maintenance is the fellowship standard.
[2]Potassium and additives
Add potassium to maintenance only after urine output is established and local protocol allows, carefully in renal impairment. Never bolus concentrated potassium. Glucose concentrations in neonatal fluids are unit-specific — collaborate with NICU recipes for true neonates rather than forcing adult ward bags.
[2]Monitoring fluid therapy
Weight, fluid balance charts, sodium, potassium, glucose, urea/creatinine, clinical oedema or dehydration signs, and in sick children lactate and haemodynamics. Postoperative ADH physiology means “full maintenance plus large deficit catch-up plus hypotonic fluid” is a triple error.
[1]Linking to neurodevelopmental consent topics
Fluid composition does not change GAS trial messages; keep domains separate when parents ask about anaesthesia safety.[4] The practical safety wins for small children on the day of surgery are glucose, sodium, and temperature.
SAQ arithmetic station simulation
Stem: “Calculate maintenance for a 16 kg child and prescribe a safe perioperative fluid.”
Answer: 40 + (6 × 2) = 52 mL/h isotonic balanced crystalloid with glucose if indicated; boluses 10–20 mL/kg for shock with reassessment; no 0.18% saline; show working.
Extended viva model answers
Why not 0.18% saline postoperatively?
“Non-osmotic ADH release impairs free-water excretion. Hypotonic maintenance causes hospital-acquired hyponatraemia and can lead to encephalopathy. AAP 2018 recommends isotonic maintenance for children needing IV maintenance fluids.”
Calculate maintenance for 27 kg.
“40 mL/h for first 10 kg, 20 mL/h for next 10 kg, 7 mL/h for remaining 7 kg → 67 mL/h isotonic fluid with glucose if indicated.”
Clear fluids on a delayed list?
“If local policy allows clear fluids to one or two hours, I will not extend starvation accidentally. I will coordinate with nursing to offer approved clear fluids and reduce ketosis and irritability.”
Pyloric stenosis fluid pearl (high-yield stem)
Infants with pyloric stenosis classically develop hypochloraemic hypokalaemic metabolic alkalosis with dehydration. Resuscitate and correct electrolytes before elective GA; empty the stomach before induction; aspiration risk is real. Fluid recipes are specialist — do not treat as a simple 4-2-1 only problem.
[1]Perioperative hypoglycaemia drill
Check → treat with protocolised 10% dextrose bolus → recheck in 15–30 minutes → adjust maintenance dextrose rate → look for sepsis or metabolic disease if unexpected and recurrent.
[2]Composition choices in ANZ practice language
Balanced isotonic crystalloids such as Plasma-Lyte 148 are commonly used for perioperative maintenance and boluses in many Australian and New Zealand paediatric centres, with glucose added for neonates and long-fasting infants. 0.9% sodium chloride remains acceptable isotonic fluid but large volumes can contribute to hyperchloraemic acidosis. The exam point is isotonic versus hypotonic, not brand loyalty. Follow local monographs for potassium-containing maintenance bags.
[2]What “appropriate glucose” means
Neonates often need glucose in maintenance fluids to prevent hypoglycaemia. Older children on short lists may not need dextrose if recently fed clear fluids and the case is brief. Critically ill children may show stress hyperglycaemia — treat extreme values per ICU protocols rather than reflexively stopping all glucose in an infant who still risks rebound hypoglycaemia.
[2]Blood product thinking (brief, linked)
Replace blood loss with blood products, not free water. In massive haemorrhage, use paediatric massive transfusion thinking with senior help. Calcium, temperature, and coagulopathy matter alongside volume.
[1]SIADH-risk states after surgery
Pain, nausea, morphine, pulmonary disease, and CNS surgery increase ADH effect. In these settings, even isotonic fluids can be associated with falling sodium if water intake is high and output low — monitor sodium rather than assuming isotonic fluids make hyponatraemia impossible. Still, isotonic is far safer than hypotonic maintenance as a default.[2]
Emergency department to theatre handover fluids
Ask what boluses were already given, current sodium/glucose, and whether the child is still shocked. Do not blindly repeat 60 mL/kg without reassessment. Abdominal sepsis can look underfilled then suddenly leak into the peritoneum — serial examination beats formula worship.
[2]Teaching list for the night before the exam
- Write 4-2-1 from memory for 5, 10, 15, 20, 30, 40 kg
- State AAP isotonic maintenance message
- List fasting times including liberal clears
- State 10–20 mL/kg bolus with reassessment
- Explain ADH and hypotonic harm
- Describe glucose check triggers in infants
Common traps
Using 0.18% saline maintenance; adult 125 mL/h orders in toddlers; six-hour clear-fluid starvation by default in centres with 1-hour clear policies; forgetting glucose in neonates; confusing resuscitation volume with maintenance rate; replacing blood loss with free water.
[1]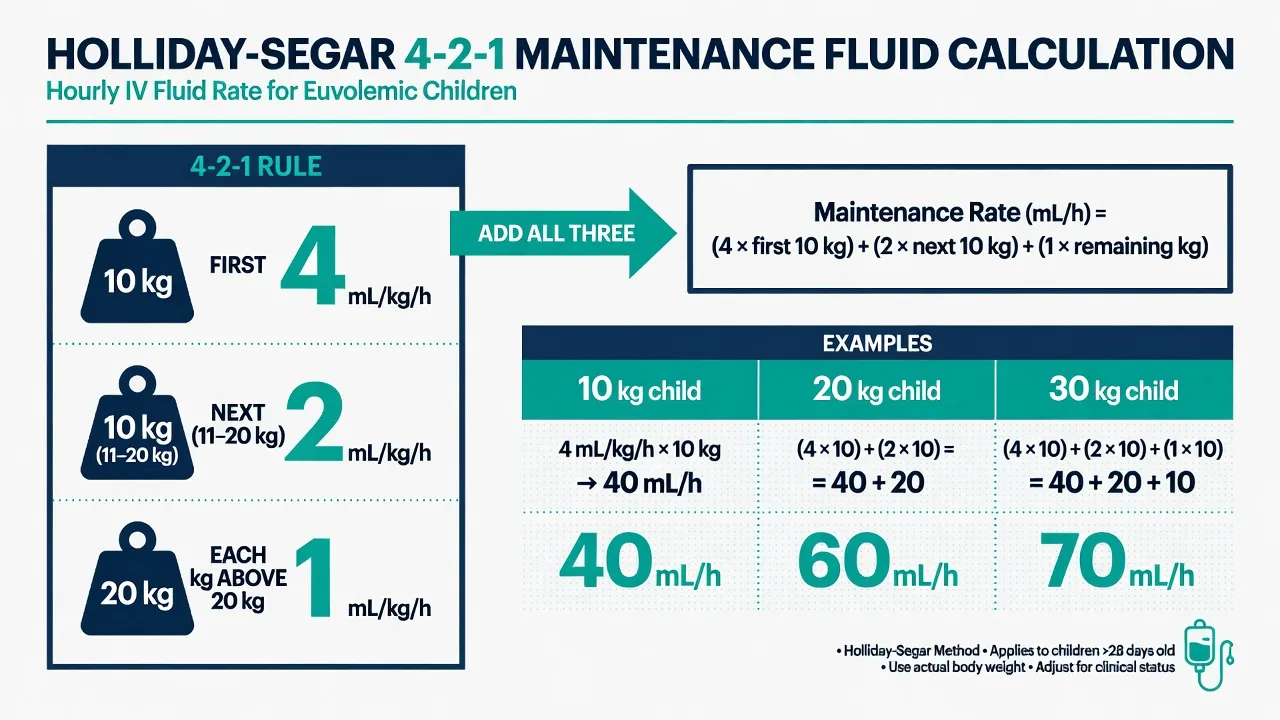
Fellowship consolidation — paediatric fluids, fasting, and glucose
[2]Holliday-Segar maintenance is calculated hourly as 4 mL/kg for the first 10 kg, 2 mL/kg for the next 10 kg, and 1 mL/kg for every kilogram above 20 kg. The daily form is 100, 50, and 20 mL/kg/day for the same weight bands. Show the arithmetic in every SAQ.
[2]Worked anchors: 5 kg equals 20 mL/h; 10 kg equals 40 mL/h; 15 kg equals 50 mL/h; 20 kg equals 60 mL/h; 30 kg equals 70 mL/h; 40 kg equals 80 mL/h. For 17 kg: 40 plus 14 equals 54 mL/h. For 26 kg: 40 plus 20 plus 6 equals 66 mL/h.
[2]Holliday-Segar estimates maintenance water need related to metabolic rate. It is not a shock bolus formula, not a blood-loss formula, and not permission to prescribe hypotonic saline. Composition is a separate decision from rate.
[1]AAP 2018 recommends isotonic maintenance fluids with appropriate potassium and dextrose for children aged 28 days to 18 years who need IV maintenance, because isotonic fluids reduce hospital-acquired hyponatraemia. Perioperative non-osmotic ADH release from pain, stress, nausea, and volume stimuli impairs free-water excretion; hypotonic maintenance then dilutes plasma sodium.
[2]Resuscitate shock with isotonic crystalloid boluses of 10 to 20 mL/kg and reassess for overload after each bolus. Replace deficits with isotonic fluid after shock is treated. Add maintenance at 4-2-1, reduced if SIADH risk or fluid overload. Replace ongoing losses separately. Monitor sodium, potassium, glucose, balance, and weight.
[1]Modern fasting practice often allows clear fluids until one or two hours preoperatively per local policy, breast milk around four hours, and formula or light meals around six hours. Liberal clear fluids reduce dehydration, ketosis, and distress. Do not impose accidental six-hour clear-fluid starvation on delayed elective lists when sips are allowed.
[2]Glucose monitoring is mandatory thinking for neonates, young infants, prolonged fasting, liver disease, critical illness, and infants of diabetic mothers. Include dextrose in maintenance when indicated. Treat hypoglycaemia with protocolised 10 percent dextrose boluses and recheck.
[3]Pyloric stenosis is a specialist fluid and electrolyte problem with hypochloraemic metabolic alkalosis — correct before elective GA. Raised intracranial pressure pathways avoid free water. Cardiac and renal failure need restricted specialist regimens. Ex-preterm infants need glucose attention plus separate apnoea monitoring plans.
[1]Hyponatraemic encephalopathy after hypotonic fluids presents with headache, nausea, seizures, or reduced consciousness. Stop free water, support ABC, check sodium urgently, and treat under senior paediatric guidance with hypertonic saline pathways as indicated. Prevention with isotonic maintenance is the standard.
[2]Exam phrase to memorise: volume by Holliday-Segar, composition isotonic with glucose as indicated, boluses 10 to 20 mL/kg with reassessment, never hypotonic maintenance by default, show the working.
[2] [2]Perioperative fluid case scripts for SAQ practice
Script 1 — 9 kg infant, delayed hernia list, last breast milk 5 hours ago.
Calculate maintenance as 36 mL/h by 4-2-1. Start isotonic fluid containing glucose, check bedside glucose at induction, keep the case short, plan early postoperative feeding if appropriate, and avoid large theoretical NPO deficit dumping. Disposition still respects any apnoea monitoring needs if the infant is an ex-preterm.
Script 2 — 22 kg child with perforated appendicitis and signs of shock.
Give isotonic crystalloid 10 to 20 mL/kg, reassess perfusion and lung fields, repeat as needed, start antibiotics, calculate maintenance 62 mL/h isotonic, check glucose and electrolytes, and prepare for theatre with ongoing resuscitation rather than pausing fluids for a neat anaesthetic chart.
Script 3 — 16 kg child after hypotonic maintenance overnight with postoperative seizure.
This is hyponatraemic encephalopathy until proven otherwise. Support airway and breathing, check sodium urgently, stop free water sources, call senior help, and treat per paediatric hypertonic saline protocols. Then redesign maintenance as isotonic and audit how the hypotonic bag was chosen.
These scripts train the same principles: correct arithmetic, isotonic composition, glucose vigilance, and crisis recognition.
[2] [2]References
- [1]Holliday MA, Segar WE The maintenance need for water in parenteral fluid therapy. Pediatrics, 1957.PMID 13431307
- [2]Feld LG, Neuspiel DR, Foster BA, et al. Clinical Practice Guideline: Maintenance Intravenous Fluids in Children. Pediatrics, 2018.PMID 30478247
- [3]Coté CJ, Zaslavsky A, Downes JJ, et al. Postoperative apnea in former preterm infants after inguinal herniorrhaphy. A combined analysis. Anesthesiology, 1995.PMID 7717551
- [4]Davidson AJ, Disma N, de Graaff JC, et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS). Lancet, 2016.PMID 26507180
- [5]Sikich N, Lerman J Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology, 2004.PMID 15114210