Anaes · Paediatric anaesthesia
Paediatric induction techniques: inhalational versus intravenous, premedication, and the sick child
Also known as Paediatric inhalational induction · Paediatric RSI · Sevoflurane induction children
Exam-exhaustive paediatric induction: sevoflurane inhalational technique, IV induction doses, premedication, parental presence, modified RSI, full-stomach and sick-child pathways, laryngospasm prevention, GAS trial neurotoxicity counselling, and crisis pivots for ANZCA Final and cross-exam equivalents.
On this page & tools
Your progress
Saved locally on this device.
8 MCQs with explanations
Target exams
Red flags

Why this is examined / the one-line answer
Induction is where paediatric anaesthesia most often declares its crises: laryngospasm, bradycardia, lost IV access, failed mask ventilation, and cardiovascular collapse in the septic or hypovolaemic child. Examiners want a reasoned choice between inhalational and intravenous techniques, exact sevoflurane conduct, premedication options, modified RSI, and a safe plan for the sick child. The GAS trial enters when parents ask about neurotoxicity after brief sevoflurane exposure in infancy.[1][2]
One-line opener: I match the induction technique to the child — sevoflurane inhalational for the well child without IV access, intravenous when access or full-stomach or instability demands it — and I never instrument a light paediatric airway. [1]
Preoperative assessment and risk stratification
History: fasting status (clear fluids 1 to 2 hours per modern liberalised guidance where adopted; breast milk 3 to 4 hours; formula and light meal 6 hours — follow local APAGBI/institutional rules); recent upper respiratory tract infection (URTI multiplies laryngospasm risk, odds ratio about 2); passive smoke exposure; asthma/croup history; snoring and obstructive sleep apnoea; congenital syndromes and previous difficult airway letters; cardiac lesions and shunts; reflux and full-stomach risk (trauma, bowel obstruction, bleeding, opioids); previous emergence delirium or postoperative nausea; allergies; current medications and steroid dependence. [1]
Examination: weight (measured, not guessed when possible); airway features; work of breathing; hydration; fever; heart murmur context; developmental stage and anxiety. [1]
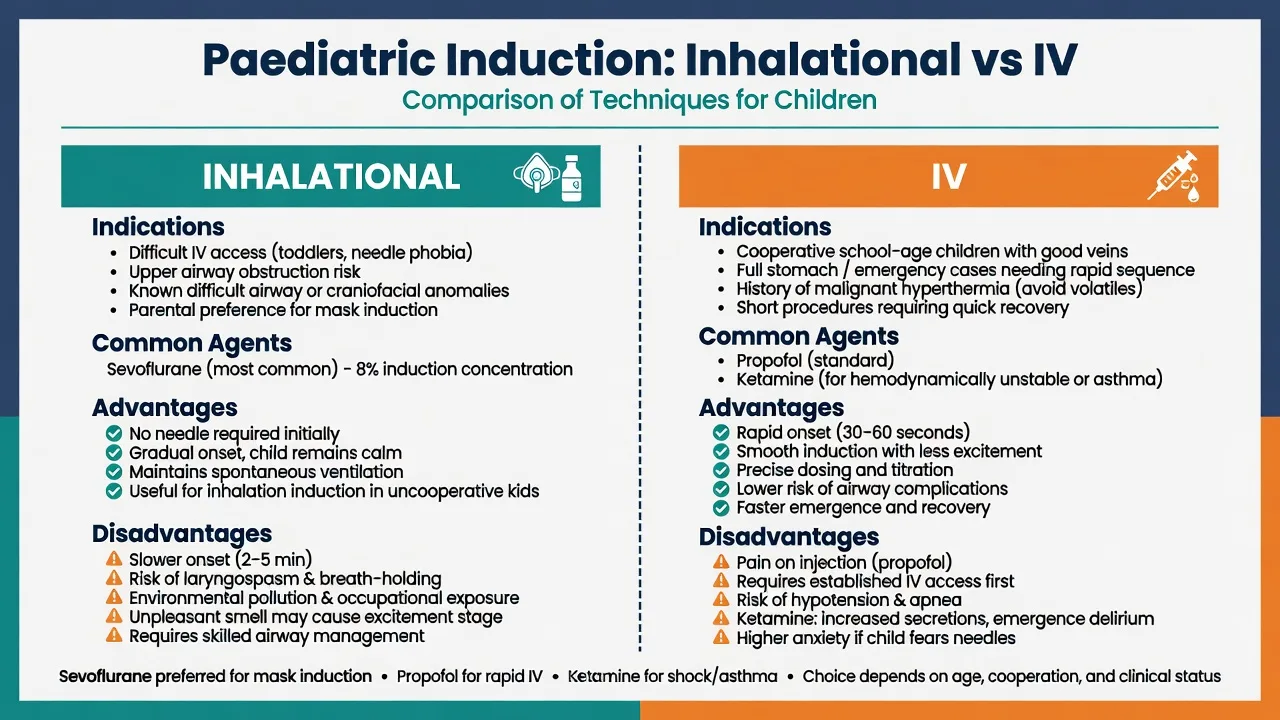
Risk triage for induction method:
- Well elective day-case child, no IV: inhalational sevoflurane is standard in many centres.
- Existing cannula or EMLA already effective: IV induction often smoother and faster.
- Full stomach / bowel obstruction / major trauma: secure IV first (IO if needed); modified RSI.
- Septic, cardiogenic, or hypovolaemic shock: IV access before induction; haemodynamically gentle agents; senior help.
- Predicted difficult airway: preserve spontaneous ventilation strategy (see syndromic airway topic); ENT present when indicated.
- Active significant URTI for elective surgery: consider postponement when feasible.[3]
Applied physiology and pharmacology
Why children desaturate fast: oxygen consumption approximately 6 mL/kg/min in infants (about twice adult), small FRC, closing capacity near FRC, high closing volume — apnoea after induction is measured in tens of seconds in neonates and young infants. Cardiac output is heart-rate dependent; hypoxia causes bradycardia quickly via vagal pathways. Atropine 20 microg/kg IV (or 20 to 40 microg/kg IM) treats or prevents bradycardia in high-risk settings; many draw it before infant induction. [1]
Sevoflurane: low blood-gas partition coefficient enables rapid induction and emergence; non-pungent compared with isoflurane/desflurane — preferred inhalational induction agent. MAC is higher in infants (sevoflurane MAC roughly 3 percent in infants, falling toward 2 percent in older children and adults). Induction concentrations of 6 to 8 percent in oxygen (with or without nitrous oxide 50 to 70 percent) are common. Dose-dependent respiratory depression, hypotension from vasodilation and reduced SVR, and epileptiform EEG patterns at high concentrations in some children are examinable caveats. Compound A and low-flow concerns are less dominant with modern circuits and CO2 absorbents but appear in primary/final physics crossovers. [1]
Nitrous oxide: speeds induction (second gas effect) but limits FiO2; avoid in bowel obstruction, pneumothorax, and some ENT middle-ear contexts; environmental and PONV considerations. [1]
Propofol: 2 to 4 mg/kg IV for induction in well children; reduce in hypovolaemia; pain on injection mitigated by lidocaine co-administration (0.5 to 1 mg/kg mixed) or larger forearm veins. Causes apnoea and hypotension. [1]
Ketamine: 1 to 2 mg/kg IV or 5 to 10 mg/kg IM; preserves respiratory drive relatively and supports blood pressure via sympathetic stimulation — first-line in many shocked children; secretions and emergence phenomena possible; consider atropine or glycopyrrolate for secretions in some protocols. [1]
Thiopental: 4 to 6 mg/kg IV historically; still examinable; less used where propofol dominates. [1]
Opioids: fentanyl 1 to 2 microg/kg IV blunts airway reflexes and reduces induction agent dose; risk of chest wall rigidity with rapid large fentanyl boluses in infants; remifentanil infusions for intubation without relaxant in skilled hands. [1]
Neuromuscular blockers: suxamethonium 1.5 to 2 mg/kg IV (2 to 4 mg/kg IM if no access) for RSI and laryngospasm rescue; bradycardia risk — atropine ready; avoid in malignant hyperthermia susceptibility, muscular dystrophy risk (hyperkalaemia), and after denervation injuries. Rocuronium 0.6 to 1.2 mg/kg IV (higher end for RSI) with sugammadex available (2 mg/kg moderate block; 4 mg/kg deep; 16 mg/kg immediate reverse after high-dose RSI in cannot-intubate pathways). [1]
Premedication pharmacokinetics: oral midazolam 0.5 mg/kg (typical max 15 to 20 mg) onset 20 to 30 minutes; nasal midazolam or dexmedetomidine in unit protocols; clonidine 2 to 4 microg/kg oral for anxiolysis and possible emergence delirium reduction. [1]
Anaesthetic goals at induction
- Safety first: monitoring on before drugs when cooperative; minimum SpO2 and ECG as soon as feasible in the uncooperative child.
- Maintain oxygenation throughout — continuous oxygen, early CPAP, short apnoeic intervals.
- Adequate depth before IV cannulation or airway instrumentation.
- Plan B equipment on the trolley (SGA, different blade, smaller tubes, suction, drugs drawn).
- Parental role defined; assistant dedicated to airway, not to distraction alone.
- Anticipate laryngospasm and bradycardia. [1]
Technique options and decision matrix
Inhalational induction — conduct
- Prepare: suction, face masks, oropharyngeal airways, SGAs, laryngoscopes (Miller for infants), cuffed tubes sized by Cole formula with half-size either side, drugs drawn (propofol or sevoflurane vaporiser filled, atropine, suxamethonium, adrenaline per local emergency doses).[5]
- Parental presence if helpful; calm environment; scented mask optional.
- Monitoring as tolerated — pulse oximeter often first.
- 100 percent oxygen or oxygen/nitrous mix; introduce sevoflurane progressively or as a single breath high-concentration technique in cooperative children.
- Maintain spontaneous ventilation; apply gentle CPAP; avoid forceful positive pressure that inflates the stomach.
- Watch for excitement stage: hold the mask, do not instrument, do not cannulate yet.
- At adequate depth (see KeyFact), place IV cannula; then deepen further for airway instrumentation if needed; give adjuncts (opioid, relaxant) as planned.
- Secure airway: SGA for many elective cases; tracheal tube when indicated (full stomach, shared airway, prone, laparoscopy, predicted long case).
Intravenous induction — conduct
When a working cannula exists: preoxygenate as able; propofol 2 to 4 mg/kg (or ketamine 1 to 2 mg/kg if unstable); optional opioid; airway support with mask then SGA or tube; neuromuscular blockade if intubating. Confirm IV patency before injecting (extravasation of induction agents causes failure and pain). [1]
Parental presence and behavioural strategies
Parental presence at induction reduces child anxiety for many families but can increase parental anxiety and, rarely, disrupt the team if the parent panics. Brief the parent: stand at the child’s side, comfort without leaning on the airway, leave promptly when asked. Child life specialists, video distraction, and play therapy are adjuncts. Do not force parental presence when the clinical situation is critical. [1]
Premedication options
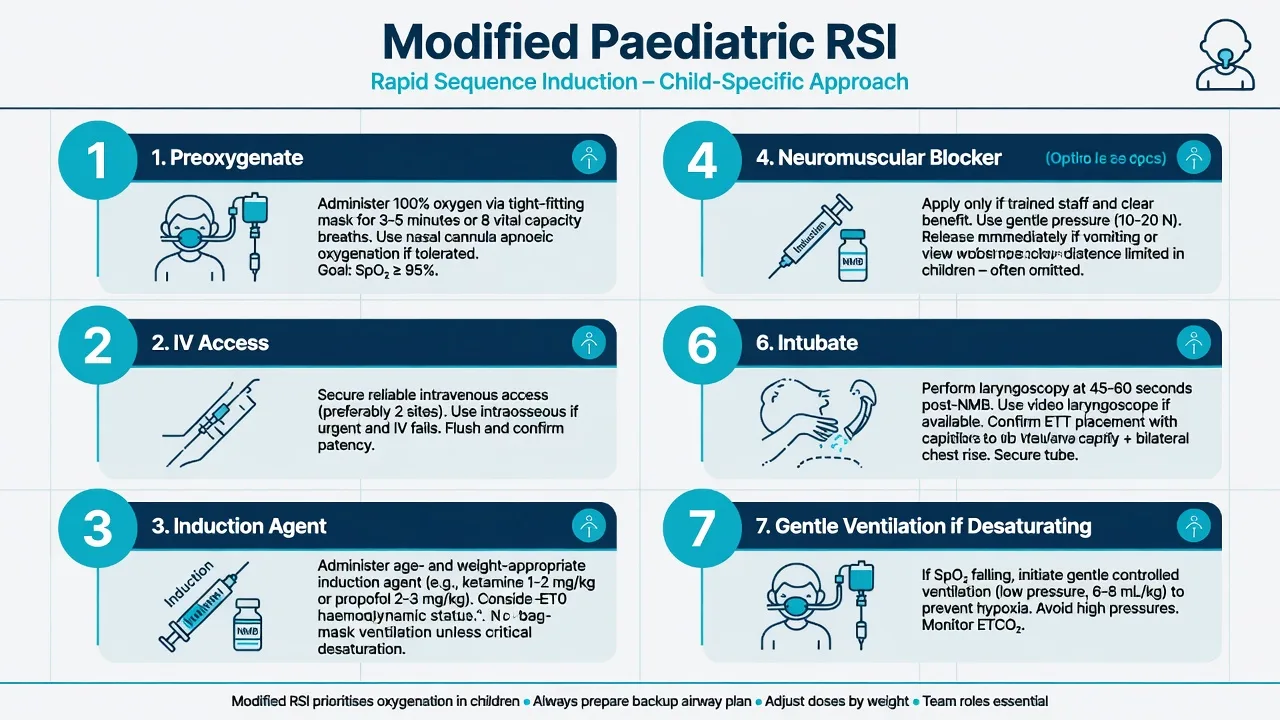
[1]Modified RSI in children
True adult classic RSI (no ventilation, mandatory cricoid) is modified because children desaturate rapidly and may need gentle ventilation. [1]
Steps:
- Prepare suction, help, difficult airway kit, and correctly sized tubes.[5]
- Preoxygenate as cooperation allows; high-flow nasal oxygen if available.
- Working IV mandatory (IO in emergency: proximal tibia, 3 to 15 kg use appropriate needle).
- Induction agent + neuromuscular blocker: suxamethonium 1.5 to 2 mg/kg IV or rocuronium 1 mg/kg (up to 1.2 mg/kg) with sugammadex available.
- Cricoid force is optional/controversial in paediatrics — if used, it must not impair ventilation or intubation; release immediately if it does.
- Gentle mask ventilation with low pressure is acceptable and often safer than prolonged apnoea.
- Intubate promptly; video laryngoscopy if skilled; confirm capnography.
- If desaturating: oxygenate first — abandon the look, mask ventilate, then reattempt with a plan change.
The sick child
Prefer IV (or IO) access before induction. Use ketamine 1 to 2 mg/kg IV or carefully titrated propofol; expect reduced drug requirements in shock; start fluid bolus 10 to 20 mL/kg isotonic crystalloid as indicated; have adrenaline 1 microg/kg IV boluses for refractory hypotension (or infusion); atropine ready. Inhalational induction of a septic or obstructed cardiac child can produce profound collapse as SVR falls and spontaneous catecholamine drive is lost. In duct-dependent congenital heart disease, maintain prostaglandin infusion and target balanced systemic and pulmonary circulations with senior cardiac anaesthesia input. [1]
Monitoring and equipment at induction
Minimum: SpO2, ECG, NIBP cycling, capnography from first airway device, temperature soon after. Stethoscope. Emergency drug calculator or Broselow/PAWPER weight estimate if weight unknown: weight (kg) approximately (age + 4) × 2 for 1 to 10 years as a rough check. Defibrillator available in theatre complex. Suction always on. [1]
Intraoperative transition
After airway secure: check bilateral air entry, secure tube at depth ID × 3 cm at lips/teeth for oral tubes, monitor cuff pressure if cuffed (below 20 to 25 cmH2O), start maintenance (sevoflurane or TIVA), multimodal analgesia, antiemesis, temperature conservation. Plan emergence deliberately — light wet extubation in a high-risk airway is a laryngospasm trap.[3]
Crisis pivots during induction
Laryngospasm: remove stimulus, 100 percent oxygen with CPAP, Larson manoeuvre, deepen with propofol 0.5 to 1 mg/kg IV, suxamethonium 0.1 to 0.2 mg/kg IV or 4 mg/kg IM, atropine 20 microg/kg for bradycardia.[3] Lidocaine IV or topical reduces laryngospasm risk in meta-analysis (risk ratio approximately 0.39).[4]
Bradycardia: treat hypoxia first; atropine; adrenaline if arrest pathway. [1]
Cannot cannulate during stormy gas induction: deepen safely, use IO, or place SGA and cannulate at depth — do not persist with light-plane needling. [1]
Failed intubation after relaxant: APAGBI/DAS paediatric algorithm — call for help, oxygenate, SGA, limit attempts, age-appropriate CICO pathway. [1]
Anaphylaxis at induction: adrenaline 1 to 10 microg/kg IV per local paediatric dosing card, remove triggers, fluids, call for help. [1]
Malignant hyperthermia suspicion (masseter spasm after suxamethonium): call for help, discontinue triggers, dantrolene pathway, supportive care. [1]
Postoperative / PACU plan
Observe for post-obstructive pulmonary oedema after laryngospasm; emergence delirium versus pain using PAED score (five items 0 to 2; total 10 or more suggests emergence delirium).[6] Analgesia, parental reunification, discharge criteria for day-case. After modified RSI for full stomach, ensure full recovery of airway reflexes before discharge from PACU.
Special populations
Neonate / ex-preterm: extreme desaturation risk; apnoea monitoring post-op if PMA under local threshold (often about 60 weeks); glucose and temperature critical. URI: defer elective when appropriate; if proceed, consider IV induction, avoid airway instrumentation when possible, deep extubation strategies in selected cases.[3] Full stomach trauma: IV/IO RSI pathway. Syndromic airway: spontaneous ventilation preserved strategy. Parental neurotoxicity anxiety: GAS showed equivalence of brief sevoflurane versus awake-regional for cognitive outcomes at 2 years and full-scale IQ at 5 years after infant hernia repair — communicate honestly; data do not cover prolonged repeated exposures.[1][2]
SAQ answer scaffold
- Compare inhalational versus IV induction with indications for each.
- Describe sevoflurane induction steps and signs of adequate depth.
- Write modified paediatric RSI with drug doses.
- Outline management of laryngospasm at induction with doses.[3]
- Counsel parents using GAS trial findings.[1][2]
Viva stem bank and model phrases
Stem: “Three-year-old for elective dental extraction, no IV, terrified.”
Model: “I offer oral midazolam 0.5 mg/kg if time, parental presence, sevoflurane inhalational induction in oxygen with or without nitrous, IV at depth, then shared airway plan with the dentist.” [1]
Stem: “Why not classic adult RSI?”
Model: “Children desaturate within seconds; gentle ventilation is often safer; cricoid may worsen the view and is not mandatory if it harms oxygenation.” [1]
Stem: “Parents fear brain damage from gas.”
Model: “The GAS trial found no neurodevelopmental difference at 2 and 5 years after about one hour of sevoflurane versus awake-regional in infancy for hernia repair; we still avoid unnecessary anaesthesia and keep haemodynamics and ventilation optimal.”[1][2]
Common traps
- Instrumenting or cannulating at a light plane
- No plan for lost IV during gas induction
- Adult RSI dogma without gentle ventilation rescue
- Omitting atropine readiness in infants
- Forcing parental presence when the parent increases chaos
- Using uncuffed tube exchange chaos without knowing cuffed evidence[5]
- Ignoring URTI risk factors for laryngospasm
- Forgetting IO as emergency access
Induction safety checklist
ANZCA Final candidates should link induction choices to SS_PA outcomes, name sevoflurane as the induction volatile of choice, and be ready to discuss GAS when neurotoxicity is raised in the communication viva station.
Inhalational induction — stage-by-stage examiner detail
Preparation room versus theatre induction: many centres induce in theatre for high-risk airways; day-case well children may induce in an anaesthetic room if local practice allows and the transfer is short with monitoring. Always have oxygen and a self-inflating bag for transfer. [1]
Single-breath versus incremental sevoflurane: cooperative older children may take a vital capacity breath of high-concentration sevoflurane in nitrous oxide/oxygen for faster loss of consciousness; toddlers usually need incremental or continuous high-concentration mask induction with distraction. The excitement stage features irregular breathing, vocalisation, and movement — hold the mask, protect the IV site if already present, do not instrument. [1]
Nitrous oxide role: second gas effect speeds induction; limits FiO2; omit when high oxygen reserve is critical (anticipated difficult airway, significant lung disease, vitamin B12 deficiency pathways, middle-ear surgery preferences). [1]
When inhalational induction fails or storms: convert to IM ketamine 5 to 10 mg/kg if no IV; or place IO; or deepen carefully with continued sevoflurane and insert SGA at depth to buy a route to cannulation. Do not persist with trauma at light planes.[3]
Intravenous induction — pharmacology table for the viva
| Agent | Typical induction dose | Notes | | Propofol | 2–4 mg/kg IV | Pain on injection; apnoea; reduce in shock | | Ketamine | 1–2 mg/kg IV; 5–10 mg/kg IM | Haemodynamically friendlier; secretions | | Thiopental | 4–6 mg/kg IV | Historical RSI agent; myocardial depression | | Fentanyl | 1–2 microg/kg IV | Blunts airway reflexes; rigidity if rapid large dose in infants | | Suxamethonium | 1.5–2 mg/kg IV; 2–4 mg/kg IM | RSI and laryngospasm; bradycardia risk | | Rocuronium | 0.6–1.2 mg/kg IV | RSI at high dose; sugammadex reverse | | Atropine | 20 microg/kg IV | Bradycardia; dry secretions somewhat | | Midazolam oral | 0.5 mg/kg | Premed 20–30 min prior | [1]
(Markdown tables can break MDX — use prose doses already in StatRow; this section restates in sentences.) Propofol 2 to 4 mg/kg IV remains the default well-child IV induction. Ketamine 1 to 2 mg/kg IV is preferred in shock. Suxamethonium 1.5 to 2 mg/kg IV or rocuronium 1 to 1.2 mg/kg IV for RSI. Atropine 20 microg/kg IV for infant bradycardia risk. Oral midazolam 0.5 mg/kg for premedication. [1]
Full-stomach scenarios in children
Indications for modified RSI: acute abdomen, bowel obstruction, bleeding tonsil, major trauma, poorly controlled reflux with recent meal, opioid-treated labouring adolescent, and any child with genuine aspiration risk. Emptying the stomach with a nasogastric tube before induction is appropriate in bowel obstruction when time allows — aspirate free fluid, leave free drainage. Cricoid force, if used, is applied by a trained assistant and released if it worsens the view. Have two suction devices for the bleeding tonsil (shared airway with blood). Head-up or lateral head-down for regurgitation events. [1]
Emergence and extubation planning starts at induction
Choose deep versus awake extubation based on risk. High laryngospasm risk (URI, airway surgery, reactive airway) may favour deep extubation by experienced hands or fully awake extubation with meticulous suction — both are defensible if deliberate. Light, wet, stimulated extubation is the trap.[3] Plan analgesia so pain does not mimic emergence delirium; use PAED when needed.[6]
Consent and neurotoxicity communication script
“Animal studies raised concern that anaesthetic drugs can affect the developing brain. The best human randomised evidence is the GAS trial, which compared about one hour of sevoflurane general anaesthesia with awake-regional anaesthesia for infant hernia repair and found no difference in cognitive scores at two years or IQ at five years. We still use the lightest effective anaesthetic, keep blood pressure and oxygen normal, and avoid unnecessary procedures — but we should not delay needed surgery because of fear of a brief anaesthetic.”[1][2]
Extended crisis algorithms at induction
Anaphylaxis: stop suspected trigger (antibiotic, muscle relaxant, latex), call for help, adrenaline per paediatric dosing card (commonly 1 to 10 microg/kg IV titrated or IM 10 microg/kg of 1:1000 in some protocols — know your local card), fluids 20 mL/kg boluses, airway support, tryptase sampling when stable. [1]
Malignant hyperthermia masseter spasm: discontinue triggers, call for help, convert to non-triggering technique, dantrolene 2.5 mg/kg IV repeated as needed, cool, treat hyperkalaemia, ICU. [1]
Aspiration: head-down lateral, suction, secure airway, oxygenate, do not routine bronchoalveolar lavage, chest radiograph, antibiotics only if infected material suspected later, observe for pneumonitis. [1]
Exam integration notes
This topic is examined across MCQ, SAQ, anaesthesia viva, and hot-case surfaces. Lead with the one-line algorithm, then expand into physiology, exact doses, and decision tables. Name the landmark guideline or trial early. Close with human factors: call for help, declare the problem, limit harmful persistence, and document. Cross-link maternal or paediatric physiology rather than treating the crisis as a pure checklist. In the ANZCA Final, discriminating marks come from absolute doses, absolute contraindications, and the structured decision when two reasonable options exist (wake versus proceed; deep versus awake extubation; proceed versus cancel). [1]
Worked scenarios (model answers)
Scenario A — 4-year-old dental, needle-phobic, well, starved. Parental presence, optional oral midazolam 0.5 mg/kg thirty minutes prior, sevoflurane in oxygen with or without nitrous oxide, IV at depth, nasal tube or shared airway plan with the dentist, throat pack vigilance, smooth emergence, day-case discharge when criteria met. [1]
Scenario B — 2-year-old bowel obstruction, bilious vomiting. IV or IO first; modified RSI with suction ×2; atropine drawn; suxamethonium 2 mg/kg IV or rocuronium 1 mg/kg with sugammadex available; gentle ventilation if desaturating; nasogastric aspiration before or after airway secure per surgical plan; expect rapid desaturation. [1]
Scenario C — 6-month-old septic for laparotomy. IO if no IV; ketamine 1 to 2 mg/kg; fluid 10 to 20 mL/kg isotonic boluses; adrenaline infusion ready; senior help; avoid pure inhalational induction; invasive monitoring early; postoperative ICU. [1]
Scenario D — Ex-preterm 50 weeks PMA for hernia. Discuss regional versus GA; apnoea monitoring overnight; glucose and temperature; brief sevoflurane if GA chosen; GAS trial context for parental questions about development after brief exposure. [1]
Theatre teamwork at paediatric induction
Assign roles: airway clinician, drug clinician, parent liaison, runner. Closed-loop drug doses by weight. Cognitive aid for emergency drugs on the wall. If induction is stormy, the team leader stops additional stimuli (surgeons, noise) until the airway is stable. Production pressure to start the list on time is not a reason to instrument a light child. [1]
References
- [1]Davidson AJ, Disma N, de Graaff JC, et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS): an international multicentre, randomised controlled trial Lancet, 2016.PMID 26507180
- [2]McCann ME, de Graaff JC, Dorris L, et al. Neurodevelopmental outcome at 5 years of age after general anaesthesia or awake-regional anaesthesia in infancy (GAS): an international, multicentre, randomised, controlled equivalence trial Lancet, 2019.PMID 30782342
- [3]Flick RP, Wilder RT, Pieper SF, et al. Risk factors for laryngospasm in children during general anesthesia Paediatr Anaesth, 2008.PMID 18315633
- [4]Mihara T, Uchimoto K, Morita S, Goto T The efficacy of lidocaine to prevent laryngospasm in children: a systematic review and meta-analysis Anaesthesia, 2014.PMID 24992191
- [5]Shi F, Xiao Y, Xiong W, Zhou Q, Huang X Cuffed versus uncuffed endotracheal tubes in children: a meta-analysis J Anesth, 2016.PMID 26296534
- [6]Sikich N, Lerman J Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale Anesthesiology, 2004.PMID 15114210