Anaes · Paediatric anaesthesia
Paediatric regional anaesthesia: caudal block dosing and safety
Also known as Armitage caudal dosing · Paediatric caudal block · Infant regional anaesthesia
Caudal anatomy and landmark versus ultrasound technique, exact Armitage volume dosing by block height, local anaesthetic mg/kg limits, test-dose limitations, LAST recognition and lipid therapy, and GAS trial context for infant regional anaesthesia.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Why this is examined
Caudal analgesia is the workhorse paediatric regional technique for sub-umbilical surgery. Examiners want Armitage volumes, safe local anaesthetic dosing arithmetic, ultrasound versus landmark technique, and LAST readiness. The GAS trial keeps infant regional anaesthesia in the curriculum for developmental outcomes after awake-regional versus sevoflurane.[1][2]
Applied anatomy
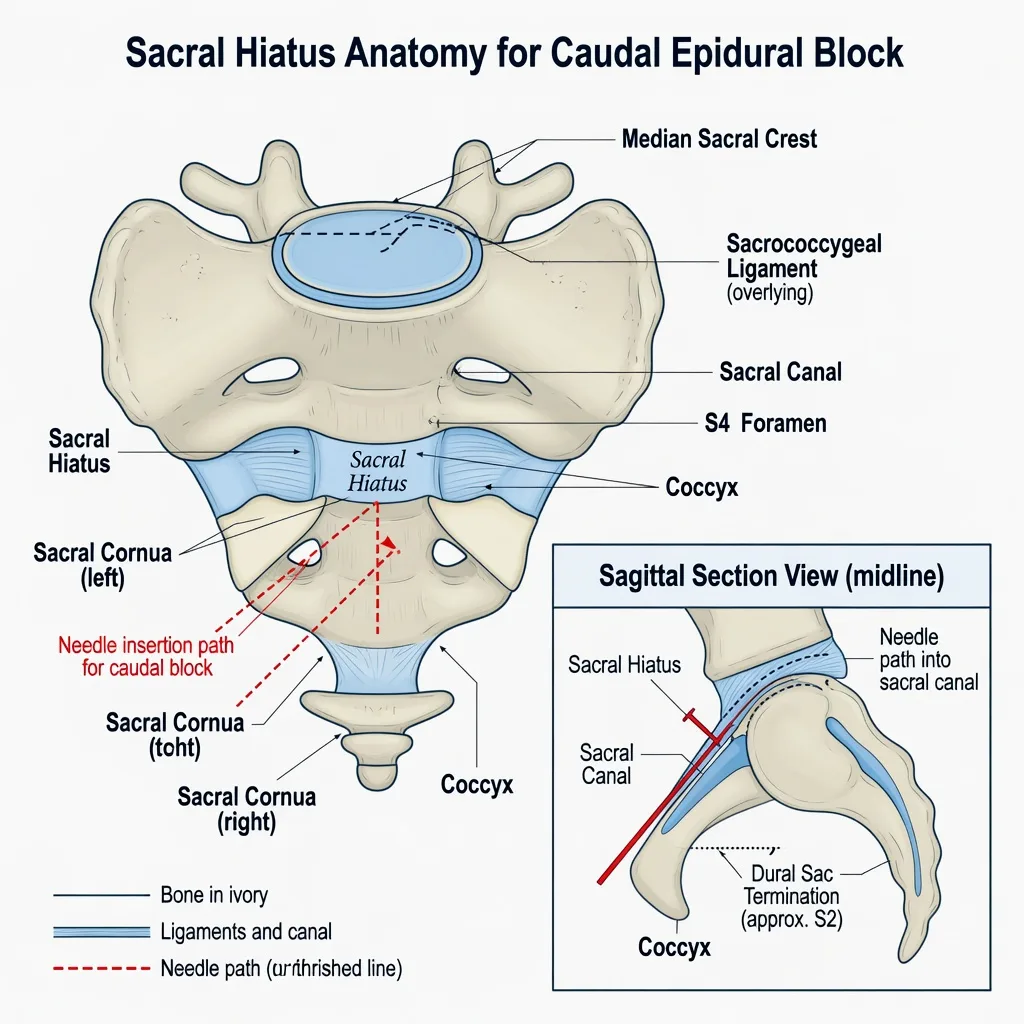
The sacral hiatus lies between the sacral cornua, covered by the sacrococcygeal ligament, continuous with the epidural space. In infants the dural sac ends lower (often near S3–S4 at birth, ascending with growth), so the risk of dural puncture and total spinal is higher than casual adult thinking suggests. Sacral anomalies (e.g. sacral dimple with tethered cord suspicion) are a stop-and-image moment — do not blindly caudal through uninvestigated sacral stigmata.
[3]Technique — landmark and ultrasound
Positioning and landmark approach
Lateral (Sims) or prone. Identify sacral cornua and hiatus. Asepsis. Short-bevel needle or cannula; advance through sacrococcygeal ligament until a characteristic give (or loss of resistance). Aspirate for blood and CSF. Inject slowly and incrementally while monitoring ECG and SpO2.
[1]Ultrasound advantages
Ultrasound improves first-pass success, visualises the sacrococcygeal membrane and sacral canal, reduces bone contact, and can show injectate spread in infants. It does not remove the need for dose calculation or aspiration.
[3]Confirmation and safety behaviours
- Aspirate before and during injection (intermittently).
- Inject in fractions; watch for resistance, subcutaneous swelling (wrong plane), or haemodynamic/ECG change.
- Test doses with adrenaline are less reliable in anaesthetised children; still useful as a behaviour of fractional injection and monitoring, not as a perfect intravascular detector.
- Have lipid emulsion available before high-dose blocks.
Armitage volume dosing — exact
Dose limits and the 10 kg worked example
Order-of-magnitude fellowship figures (confirm with local formulary):
[1]- Plain bupivacaine / levobupivacaine maximum commonly 2–2.5 mg/kg
- Ropivacaine maximum commonly around 2–3 mg/kg depending on source and context
- Adrenaline-containing mixtures may alter some published maxima but add complexity; many paediatric caudals use plain dilute agents
Worked example examiners love
For a 10 kg child, max bupivacaine 2.5 mg/kg = 25 mg total.
0.25% bupivacaine = 2.5 mg/mL → 10 mL = 25 mg.
Armitage 1.0 mL/kg = 10 mL.
So 10 mL of 0.25% is exactly at a 2.5 mg/kg ceiling for a T10-oriented volume — there is no free margin. Many clinicians use 0.2% or 0.19% (diluted) to create safety margin, or accept slightly lower volume.
For 1.25 mL/kg at 0.25% in 10 kg = 12.5 mL = 31.25 mg = 3.125 mg/kg — over many maxima. That is why dilute solutions are mandatory for higher volumes.
[1]LAST — recognition and management
Caudal safety checks
Presentation: perioral tingling and tinnitus are not available under GA; look for ECG change, arrhythmia, haemodynamic instability, seizures on emergence, cardiovascular collapse.
[4]Management (AAGBI/ASRA-aligned checklist thinking):
[1]- Stop injectate; call for help; note time.
- Airway, 100% oxygen, ventilate; abort seizures with benzodiazepines (e.g. midazolam titrated).
- Intravenous lipid emulsion 20%: bolus commonly 1.5 mL/kg lean body weight over 2–3 minutes, then infusion (commonly 0.25 mL/kg/min, increase if unstable) per current checklist — know where the kit is.
- ACLS with modifications: avoid local anaesthetic progression; reduce adrenaline doses in some LAST algorithms; consider CPB/ECMO for refractory arrest.
- Prolonged resuscitation may be required — do not declare futility early.
Context: GAS and multimodal analgesia
Awake-regional techniques in infancy were a GAS trial arm; neurodevelopmental outcomes at 2 and 5 years were similar to brief sevoflurane GA for the studied infant surgery class.[1][2] Caudals combine with paracetamol and NSAIDs when appropriate. Avoid codeine in children after tonsillectomy/adenoidectomy because of CYP2D6 ultra-rapid metabolism risk and regulatory contraindications.
Emergence behaviour may still occur after GA even with good caudal analgesia; PAED scoring is the research tool for emergence delirium, not a caudal endpoint.[4] Airway reactivity remains a separate risk domain.[5]
Contraindications and cautions
- Local infection, sacral anomalies without imaging clearance, coagulopathy beyond institutional thresholds, parental refusal, lack of resuscitation readiness.
- High volumes in small infants: watch for motor block, urinary retention expectations, and rare total spinal.
- Never combine multiple large regional doses without cumulative mg accounting.
SAQ answer scaffold
- Landmarks / ultrasound steps and safety checks.
- Armitage volumes exact.
- Max mg/kg and the 10 kg arithmetic link.
- LAST management including lipid 1.5 mL/kg of 20%.
- GAS one-liner (developmental equivalence in studied cohort).
Viva stem bank
- “Give me Armitage volumes.”
- “Your 8 kg infant needs a high block — how do you stay under 2.5 mg/kg?”
- “Test dose — how good is it in an anaesthetised child?”
- Model phrase: “I calculate milligrams first, then see if Armitage volume fits at a dilute concentration.”
Adjuncts and duration extension
Single-shot caudal duration is limited. Strategies:
[3]- Optimal concentration/volume within mg limits
- Adjuncts used in some practices: clonidine (e.g. 1–2 micrograms/kg caudally — local protocol), preservative-free opioids in specialist settings (respiratory depression risk, monitoring)
- Continuous caudal/epidural catheters in selected infants for major abdominal surgery
- Wound infiltration and systemic multimodal analgesia to spare needing huge caudal volumes
Do not stack adjuncts and high-concentration LA until total toxicity risk is recalculated.
[5]Ultrasound-era updates to Armitage thinking
Armitage remains the exam volume skeleton. Ultrasound and imaging studies show that cranial spread is imperfectly predicted by weight alone and high volumes may still fail to reach high thoracic levels consistently in every child.[3] Clinical implication: for upper abdominal targets, consider epidural/paravertebral/ESP alternatives rather than forcing 1.25 mL/kg if the mg ceiling is already tight.
Total spinal and intravascular injection
Total spinal: sudden apnoea, fixed pupils, cardiovascular collapse after caudal — support airway and circulation; may need prolonged ventilation until block recedes. Higher infant dural sac makes this more than a theoretical risk.
[3]Intravascular: ECG changes, LAST pathway. Incremental injection is the practical defence when test-dose sensitivity is limited under GA.
[1]Documentation and consent
Discuss motor block expectations, urinary retention possibility, rare serious nerve/epidural complications, and LAST risk in age-appropriate consent with parents. Document concentration, volume, total mg, and mg/kg.
[3]Armitage volumes — memorisation and clinical limits
Exact Armitage teaching volumes:
[1]- 0.5 mL/kg — sacral / low lumbar (e.g. circumcision, low perineal)
- 1.0 mL/kg — thoracolumbar around T10 (lower abdominal)
- 1.25 mL/kg — higher thoracic targets
Volume drives cranial spread; concentration and total milligrams drive density and toxicity risk. Fluoroscopic and imaging studies with modern agents support weight-based volume thinking while showing imperfect prediction of exact dermatomes in every child.[3] For high abdominal targets, consider alternative regional techniques when milligram ceilings are tight rather than forcing toxic volumes.
The milligram-first algorithm (non-negotiable)
- Weigh the child (or best estimate).
- Choose maximum mg/kg for the agent (e.g. bupivacaine 2–2.5 mg/kg teaching ceiling).
- Calculate maximum milligrams.
- Choose desired Armitage volume for surgical height.
- Solve for maximum allowable concentration: max mg ÷ volume mL = mg/mL → convert to percent.
- If the desired volume at a convenient concentration exceeds max mg, redesign — lower volume, dilute further, lower target, or different block.
Worked examples
10 kg, target 1.0 mL/kg, bupivacaine max 2.5 mg/kg: max 25 mg; volume 10 mL → max 2.5 mg/mL = 0.25%. Exactly at ceiling — many clinicians choose 0.2% for margin.
[1]8 kg, target 1.25 mL/kg with 0.25%: volume 10 mL; 25 mg = 3.125 mg/kg — over ceiling. Use 0.2% (20 mg = 2.5 mg/kg) or reduce volume.
[1]16 kg, target 0.5 mL/kg with 0.25%: volume 8 mL = 20 mg = 1.25 mg/kg — comfortable margin.
[1]Anatomy risks unique to infants
The dural sac ends lower in neonates (near S3–S4 at birth), ascending with growth. This raises total spinal risk if the needle is advanced too far or large volumes track cranially under pressure. Sacral anomalies and sacral dimples with possible tethered cord require imaging clearance — do not caudal through uninvestigated stigmata.
[3]Landmark versus ultrasound technique expanded
Landmark: lateral or prone; identify cornua and hiatus; asepsis; short-bevel needle; sacrococcygeal ligament give; aspirate; incremental inject.
Ultrasound: visualise membrane and canal; improve first-pass success; see spread; still calculate dose and aspirate. Ultrasound does not make LAST impossible.
Test doses with adrenaline are less reliable under general anaesthesia because heart-rate responses are blunted and specificity/sensitivity are imperfect. Fractional injection plus monitoring remains mandatory.
[1]LAST under anaesthesia — recognition without subjective symptoms
Under GA you will not hear “my tongue is tingling.” Watch for ECG changes, arrhythmias, haemodynamic instability, and later seizures on emergence. Management:
[1]- Stop injectate; call for help
- Airway, 100% oxygen
- Benzodiazepines for seizures
- 20% lipid emulsion bolus commonly 1.5 mL/kg then infusion per current checklist
- Modified ACLS; prolonged resuscitation; ECMO/CPB in refractory arrest where available
- Do not declare futility early
Know the physical location of lipid before performing the block.
[1]Adjuncts and duration
Single-shot caudal duration is limited to hours. Adjuncts used in some practices include clonidine 1–2 microg/kg caudally (local protocol) and, in specialist settings, preservative-free opioids with mandatory monitoring for respiratory depression. Continuous catheters serve major abdominal surgery in infants in specialist centres. Wound infiltration and systemic multimodal analgesia reduce the need for heroic caudal volumes.
[3]GAS trial context for infant regional
GAS randomised infants for hernia repair to awake-regional versus sevoflurane and found similar neurodevelopmental outcomes at 2 and 5 years for primary cognitive endpoints.[1][2] Use this to counsel parents, not to claim regional abolishes all risk or that every infant must have awake-regional regardless of feasibility.
Failure modes and troubleshooting
- Subcutaneous swelling: wrong plane — stop, reassess landmarks/ultrasound
- No block: wrong plane, inadequate volume, intravascular injection, or too little time
- Unilateral block: less common than epidural but reposition and assess
- Dense motor block unexpectedly high: monitor ventilation
- Total spinal: apnoea, cardiovascular collapse — support ABC until recession
Consent points for parents
Expected numbness/weakness of legs for hours, possible urinary retention, rare serious complications (infection, haematoma, nerve injury, LAST), and conversion plan if block fails. Document concentration, volume, total mg, and mg/kg.
[3]Integration with analgesia and ED
Good caudal analgesia reduces pain-driven PACU distress but does not eliminate emergence delirium after sevoflurane; use PAED when thrashing persists despite low pain scores.[4] Airway reactivity remains a separate risk domain in paediatric anaesthesia.[5]
Extended viva model answers
Give Armitage volumes.
“0.5 mL/kg for sacral–low lumbar, 1.0 mL/kg for thoracolumbar about T10, 1.25 mL/kg for higher thoracic targets of dilute local anaesthetic.”
Test dose reliability?
“Less reliable under general anaesthesia. I still aspirate and inject incrementally with ECG monitoring. I do not trust a negative test dose as proof of extravascular placement.”
Lipid dose?
“Intravenous lipid emulsion 20 percent at about 1.5 mL/kg bolus lean body weight, then infusion per the current LAST checklist, alongside airway support and seizure control.”
Block height versus surgery matching
Circumcision/low urology → 0.5 mL/kg often sufficient.
Inguinal hernia/orchidopexy → commonly 1.0 mL/kg.
Upper abdominal → caudal may be the wrong tool; consider epidural/other planes rather than toxic 1.25 mL/kg at high concentration.
Combined caudal plus GA safety
Most paediatric caudals are performed after induction. That improves immobility but removes early subjective LAST symptoms and reduces test-dose sensitivity — hence milligram discipline and incremental injection matter more, not less.
[1]Step-by-step caudal performance checklist
- Consent and indication confirmed; contraindications absent
- Weight recorded; max mg calculated and written
- Desired Armitage volume chosen for surgical height
- Concentration selected so volume × concentration ≤ max mg
- Lipid emulsion location confirmed
- Asepsis; positioning; landmark or ultrasound
- Needle through sacrococcygeal ligament; aspirate
- Incremental injection with monitoring
- Observe for wrong-plane swelling or ECG change
- Document mg, mg/kg, volume, concentration, time
Compare caudal with other paediatric regional options
| Technique | Best for | Limits |
|---|---|---|
| Caudal single shot | Sub-umbilical surgery | Duration; high thoracic unreliable/toxic volume |
| Caudal/epidural catheter | Major abdominal in infants | Infection/care complexity |
| Ilioinguinal/US groin blocks | Hernia | Surgeon infiltration overlap |
| Penile block | Circumcision | Needs correct planes |
| ESP/paravertebral | Thoracic/abdominal alternatives | Skill dependent |
LAST kit contents awareness
20% lipid emulsion, dosing card, airway equipment, benzodiazepine, CPR drugs, and a plan for prolonged resuscitation. Assign who fetches lipid before the block starts in remote locations.
[3]Exam arithmetic speed drills
Do five rapid calculations the night before: 6 kg at 1.0 mL/kg with max 2.5 mg/kg; 12 kg at 0.5 mL/kg with 0.25%; 9 kg at 1.25 mL/kg — show when 0.25% is illegal. Speed plus accuracy wins SAQs.
[1]Common traps
Volume without mg calculation; caudal through sacral stigmata; no lipid available; expecting adrenaline test dose to be perfectly sensitive under GA; using 0.5% bupivacaine for large paediatric volumes; forgetting lower dural sac in infants.
[3]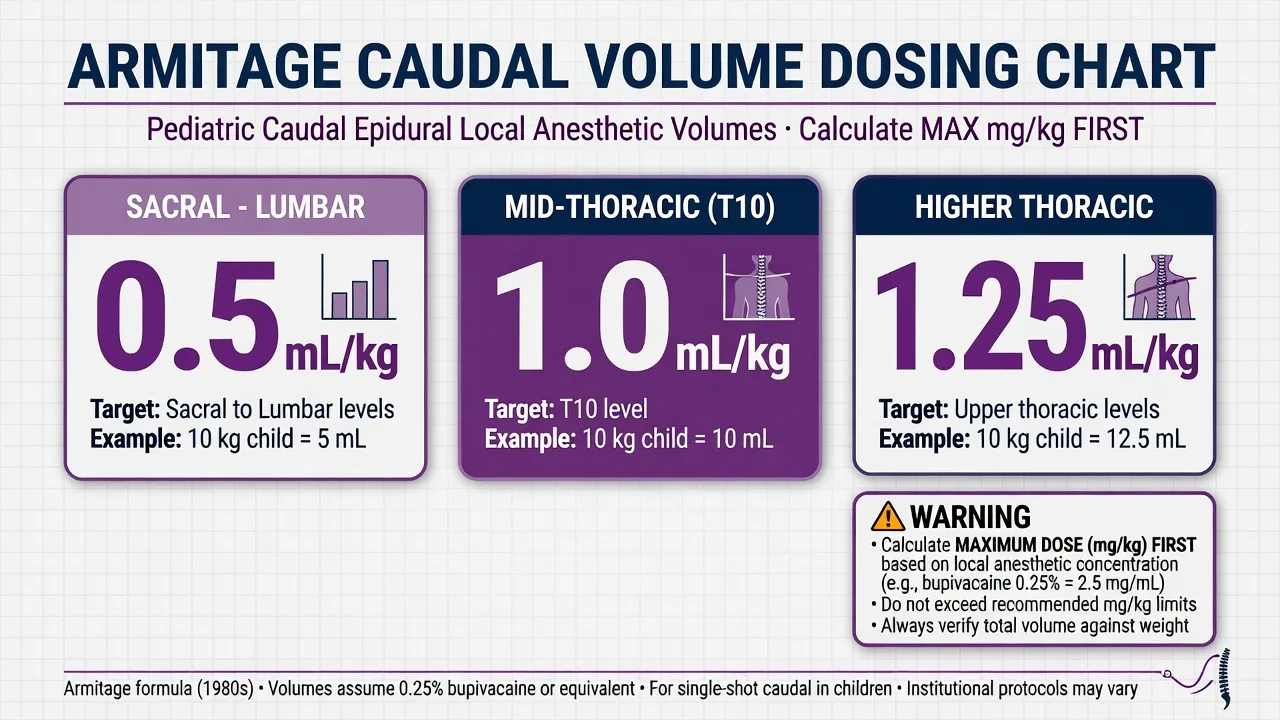
Fellowship consolidation — caudal dosing and LAST safety
[3]Caudal blockade remains the workhorse paediatric regional technique for sub-umbilical surgery. Examiners want Armitage volumes, milligram-first arithmetic, ultrasound versus landmark technique, and LAST readiness including lipid emulsion dosing.
[3]Armitage volumes: 0.5 mL/kg for sacral and low lumbar targets, 1.0 mL/kg for thoracolumbar targets around T10, and 1.25 mL/kg for higher thoracic targets. Volume primarily sets height; concentration and total milligrams set density and toxicity risk.
[5]Typical local anaesthetic ceilings in fellowship teaching are about 2 to 2.5 mg/kg for plain bupivacaine or levobupivacaine and around 2 to 3 mg/kg for ropivacaine depending on source and context. Confirm with local formulary, but never skip the calculation.
[3]Classic 10 kg example: maximum bupivacaine 2.5 mg/kg equals 25 mg. Using 0.25 percent bupivacaine at 2.5 mg/mL, 10 mL equals 25 mg. Armitage 1.0 mL/kg also equals 10 mL, so the plan sits exactly at ceiling with no margin. Many clinicians dilute to about 0.2 percent to create safety margin.
[1]If Armitage 1.25 mL/kg at 0.25 percent in a 10 kg child yields 12.5 mL and 31.25 mg equalling 3.125 mg/kg, the plan exceeds common maxima and must be redesigned. Dilute, reduce volume, lower target height, or choose another technique.
[1]Infant dural sac ends lower, often near S3 to S4 at birth, so total spinal risk is real. Sacral dimples and stigmata of dysraphism require imaging clearance before blind caudal injection. Ultrasound improves first-pass success and can show spread but does not remove dose discipline.
[3]Safety behaviours: asepsis, aspiration for blood and CSF, incremental injection, ECG and SpO2 monitoring, and lipid emulsion immediately available. Adrenaline test doses are less reliable under general anaesthesia; fractional injection remains essential.
[1]LAST under anaesthesia lacks early subjective warning symptoms. Watch ECG and haemodynamics. Management: stop injectate, call for help, 100 percent oxygen, benzodiazepines for seizures, 20 percent lipid emulsion commonly 1.5 mL/kg bolus then infusion per checklist, modified ACLS, and prolonged resuscitation readiness including ECMO where available.
[1]GAS trial context: awake-regional versus sevoflurane in infant hernia repair showed similar neurodevelopmental outcomes at two and five years for primary cognitive endpoints. Use this for counselling, not as a claim that regional abolishes all risk or is always feasible.
[1]Document concentration, volume, total milligrams, and milligrams per kilogram. Consent for motor block, urinary retention possibility, rare serious complications, and failure with conversion to systemic analgesia.
[3] [1]Full SAQ worked answer (model)
Question: Describe how you would provide caudal analgesia for a 12 kg child undergoing bilateral orchidopexy, including dose calculation and safety measures.
[3]Model structure:
[1]- Indication and consent. Sub-umbilical surgery suitable for caudal. Discuss benefits, motor block, rare serious risks, and LAST. Confirm no sacral anomalies or coagulopathy concerns.
- Milligram ceiling first. Using bupivacaine maximum 2.5 mg/kg, maximum total is 30 mg.
- Volume by Armitage. Target about T10 with 1.0 mL/kg equals 12 mL.
- Concentration check. 30 mg in 12 mL equals 2.5 mg/mL equals 0.25 percent exactly at ceiling. Prefer 0.2 percent (24 mg equals 2.0 mg/kg) for margin, accepting slightly less dense block and relying on systemic multimodal analgesia.
- Technique. After GA induction, lateral position, asepsis, landmark or ultrasound identification of sacral hiatus, needle through sacrococcygeal ligament, aspirate, incremental injection with ECG monitoring, observe for subcutaneous swelling.
- Rescue readiness. Lipid emulsion 20 percent available; know 1.5 mL/kg bolus pathway; airway support plan.
- Postoperative. Expect temporary leg weakness; combine with paracetamol and NSAID if appropriate; document mg and mg/kg.
This answer hits anatomy, Armitage, arithmetic, and LAST without fluff.
[1] [1]Adjuncts, catheters, and failure management in depth
Single-shot caudal duration is typically a few hours depending on agent, concentration, and adjuncts. When longer analgesia is required after major abdominal surgery in infants, continuous caudal or epidural catheters may be used in specialist centres with strict asepsis, tunnelling preferences per unit, and monitoring for local anaesthetic accumulation. Adjunct clonidine at about 1 to 2 micrograms per kilogram caudally is used in some protocols to prolong analgesia; preservative-free neuraxial opioids appear only in specialist pathways because of respiratory depression risk and the need for monitored beds.
[3]Failure management is systematic. If the block is patchy or absent, reassess whether injectate went subcutaneous, whether volume was adequate for surgical height, and whether surgery extended above the blocked segments. Do not repeatedly inject more local anaesthetic without recalculating cumulative milligrams. Convert to systemic multimodal analgesia or consider an alternative regional technique rather than chasing a failed caudal into the toxic range.
[3]Urinary retention and temporary motor weakness should be anticipated and explained. Dense unexpected high block with apnoea suggests total spinal physiology — support airway and circulation until recession. Intravascular injection leads into the LAST pathway already described. Infection is rare but catastrophic if epidural abscess develops; fever, back pain, and neurological change need urgent imaging pathways.
[3]For the fellowship candidate, the discriminating skills are not needle heroics but arithmetic honesty: milligrams first, Armitage second, redesign when they conflict, lipid ready before injection, and clear documentation of what was given.
[1] [1]References
- [1]Davidson AJ, Disma N, de Graaff JC, et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS). Lancet, 2016.PMID 26507180
- [2]McCann ME, de Graaff JC, Dorris L, et al. Neurodevelopmental outcome at 5 years of age after general anaesthesia or awake-regional anaesthesia in infancy (GAS). Lancet, 2019.PMID 30782342
- [3]Koo BN, Hong JY, Kim JE, Kil HK Spread of ropivacaine by a weight-based formula in a pediatric caudal block: a fluoroscopic examination. Yonsei Medical Journal, 2010.PMID 20236099
- [4]Sikich N, Lerman J Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale. Anesthesiology, 2004.PMID 15114210
- [5]Flick RP, Wilder RT, Pieper SF, et al. Risk factors for laryngospasm in children during general anesthesia. Paediatric Anaesthesia, 2008.PMID 18315633