Anaes · Paediatric anaesthesia
Paediatric respiratory and cardiovascular physiology for the anaesthetist
Also known as Infant cardiovascular physiology · Paediatric FRC oxygen consumption · Neonatal transitional circulation anaesthesia
Infant oxygen consumption, FRC and closing capacity, compliant chest wall, heart-rate-dependent cardiac output, transitional circulation residues, thermoregulation, and the anaesthetic implications that explain rapid desaturation and hypoxic bradycardia for ANZCA Primary and Final.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Why this is examined
Applied infant physiology is the reason paediatric crises run on a shorter clock than adult ones. Primary examiners want the numbers (VO2, FRC–closing capacity relationship, HR dependence of CO). Final examiners want the same numbers linked to airway time pressure, bradycardia pathways, fluid and drug choices, and the ex-preterm monitoring decision.[3][4] Curriculum anchors sit in SS_PA and basic science respiratory/cardiovascular domains shared across ANZCA, FRCA, EDAIC, ABA APPLIED, and FCAI.
Respiratory physiology — the numbers that matter
Oxygen consumption and FRC
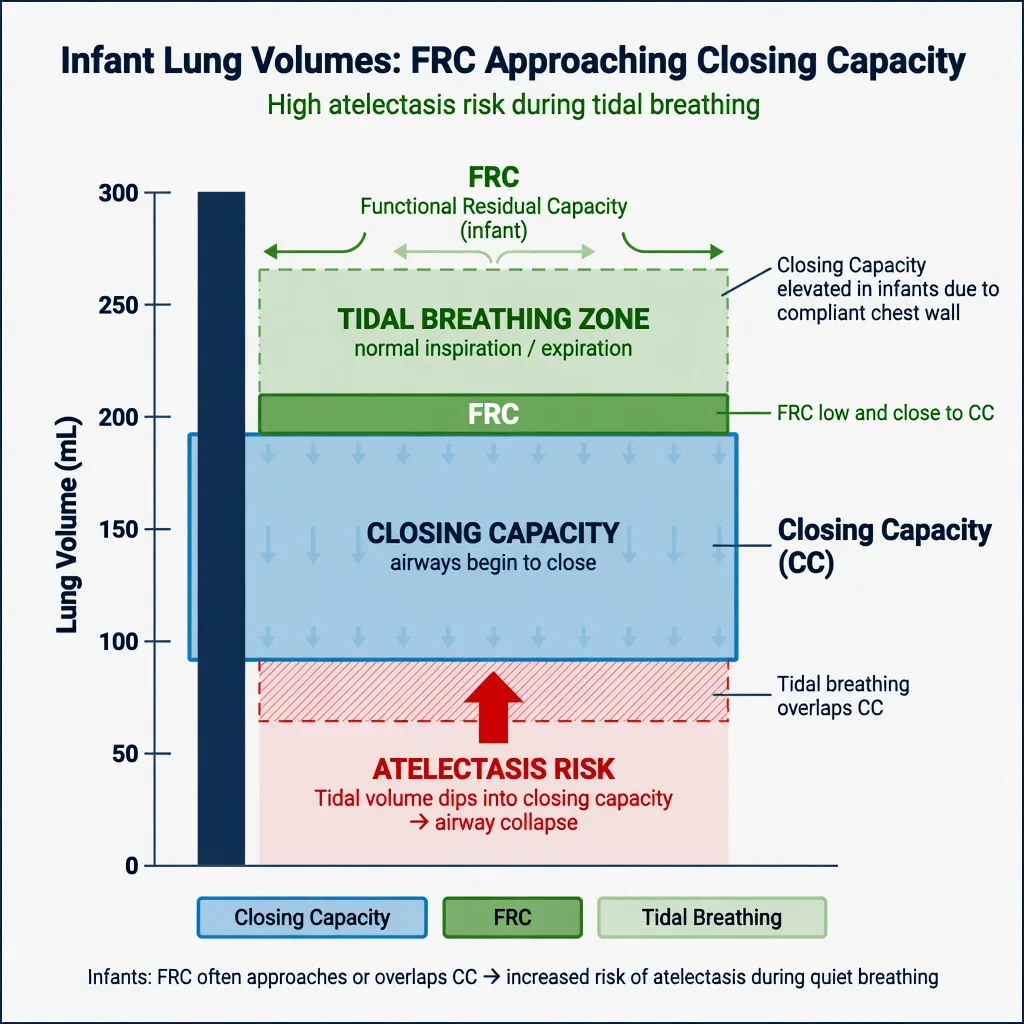
Weight-indexed oxygen consumption in the infant is roughly double the adult value. Coupled with a small absolute functional residual capacity (FRC) and a closing capacity that encroaches on or exceeds FRC during tidal breathing, the result is early airway closure, intrapulmonary shunt, and rapid fall in SpO2 once apnoea begins. Preoxygenation is therefore not optional; it is the only buffer between induction and desaturation.
[1]Chest wall, ribs, and the diaphragm
The infant chest wall is highly compliant and the ribs are more horizontal. Inspiration is largely diaphragmatic. Anything that impairs diaphragmatic excursion — gastric insufflation, abdominal surgery, pneumoperitoneum, abdominal distension from ileus — immediately reduces tidal volume. Preferential nasal breathing in neonates means nasal obstruction (secretions, NG tubes, choanal issues) can tip a marginal airway into obstruction.
[1]Closing capacity and the desaturation cascade
When closing capacity exceeds FRC, dependent airways close during tidal breathing. Under anaesthesia, FRC falls further (loss of tone, cranial diaphragm, absorption atelectasis on high FiO2). The cascade is: low FRC → airway closure → shunt → hypoxaemia → bradycardia → low cardiac output → arrest. That is why laryngospasm and difficult mask ventilation are not “airway only” problems — they are oxygen-delivery emergencies within minutes.[3]
Oxygen transport and haemoglobin
Fetal haemoglobin (HbF) has higher oxygen affinity (left-shifted oxyhaemoglobin dissociation curve), which favours placental oxygen uptake but unloads less readily at tissue PO2. As HbF declines over the first months of life, the curve normalises. Anaemia is poorly tolerated because stroke-volume reserve is limited: oxygen delivery (DO2 = CO × CaO2) falls mainly through content or rate, not through a large SV increase. Maintain haemoglobin thresholds consistent with neonatal/paediatric critical-care guidance in the sick neonate, and treat anaemia before elective major surgery when feasible.
[1]Cardiovascular physiology
[1]Why hypoxia causes bradycardia
Hypoxaemia and acidosis stimulate intense vagal outflow and depress sinoatrial automaticity. The infant has limited ability to increase stroke volume, so the physiological response that adults use (tachycardia then later bradycardia) is truncated. Practically: airway and oxygen first, then atropine (commonly 20 micrograms/kg IV, minimum practical dose often discussed as 100 micrograms in older teaching — follow current PALS/APLS dosing charts), then chest compressions at institutional arrest thresholds.
[1]Transitional circulation residues
The foramen ovale and ductus arteriosus may be only functionally closed. Hypoxia, hypercarbia, and acidosis raise pulmonary vascular resistance (PVR) and can reopen right-to-left shunt, producing cyanosis out of proportion to lung disease — persistent pulmonary hypertension of the newborn (PPHN) physiology. Anaesthetic implications: avoid those triggers; optimise oxygenation and ventilation; consider inhaled nitric oxide and advanced support in the true PPHN crisis (NICU context).
[1]Autonomic and vascular features
Baseline SVR is lower than in older children. Baroreflexes are immature. Volume responsiveness exists but over-transfusion and fluid overload are poorly tolerated in duct-dependent or failing hearts. Inotrope and vasopressor choices must be weight-based and indication-specific (e.g. milrinone in low-output states with high SVR after cardiac surgery; noradrenaline for vasodilated septic shock — senior paediatric ICU input).
[3]Thermoregulation
Large surface-area-to-mass ratio, thin skin, limited subcutaneous fat, brown-fat dependence in neonates, and impaired shivering under anaesthesia produce rapid heat loss. Hypothermia increases oxygen consumption in the awake or lightly anaesthetised infant, worsens coagulopathy, depresses respiration, and prolongs drug effects. Forced-air warming, warm operating-room temperature, covered head and extremities, and warmed fluids are mandatory — not optional comfort measures.
[1]Anaesthetic implications (link physiology to plan)
Induction and maintenance choices through a physiology lens
Inhalational induction with sevoflurane remains common because IV access may be delayed, but the apnoeic window after deep induction is short. Maintain spontaneous ventilation until the airway is secured if the airway is difficult. Once instrumented, controlled ventilation must avoid excessive peak pressures that inflate the stomach. The GAS trial informs the developmental-neurotoxicity debate for brief early anaesthesia but does not redefine the cardiorespiratory physiology above; developmental outcomes at 2 and 5 years were similar for awake-regional versus sevoflurane in the studied infant hernia population.[1][2]
Monitoring priorities
Standard: SpO2, ECG (rate and rhythm are primary CO surrogates), NIBP with appropriate cuff, EtCO2 (waveform quality matters — small tidal volumes leak easily), temperature. Extended: invasive arterial pressure for major or unstable cases, blood gas and glucose, near-infrared spectroscopy in cardiac/neonatal pathways where available. Alarm limits must be age-adjusted; adult bradycardia thresholds will alarm too late.
[1]Special populations and cross-links
- Ex-preterm: apnoea risk after anaesthesia tracks post-menstrual age; Coté combined analysis remains the classic quantitative reference for hernia populations.[4]
- Congenital heart disease: balance PVR/SVR carefully; air filters; de-air lines meticulously.
- Upper respiratory infection: multiplies laryngospasm risk; physiology makes the event more dangerous even if the incidence only doubles.[3]
SAQ answer scaffold
- State the two respiratory numbers: VO2 ~6 mL/kg/min; closing capacity near FRC.
- Explain desaturation: high consumption + low oxygen store + shunt from airway closure.
- State CO ≈ HR × limited SV and why hypoxia → bradycardia.
- List anaesthetic actions: preoxygenate, minimise apnoea, treat bradycardia with oxygen then atropine, active warming, avoid PVR triggers.
- Mention transitional circulation residues in neonates.
Viva stem bank and model phrases
- “Why does an infant desaturate faster than an adult after the same preoxygenation?”
- “Why is bradycardia more dangerous in a six-week-old than in a teenager?”
- “What happens to FRC under anaesthesia, and how does that interact with closing capacity?”
- Model phrase: “Cardiac output is largely rate-dependent; hypoxic bradycardia is an oxygen-delivery emergency, not a pure vagal curiosity.”
Drug and dose implications of the physiology
Weight-based dosing is not optional. Common exam figures:
[1]- Atropine for bradycardia: typically 20 micrograms/kg IV (follow current PALS/APLS chart; ensure adequate minimum practical dose per local protocol).
- Adrenaline for arrest: 10 micrograms/kg IV/IO per resuscitation algorithm.
- Fluid bolus: 10–20 mL/kg isotonic crystalloid with reassessment.
- Induction agents: reduce doses in the critically ill; expect faster desaturation during IV or inhalational induction.
- Suxamethonium: higher paediatric dose historically (~2 mg/kg IV in infants) with bradycardia risk — atropine readiness; many now prefer high-dose rocuronium with sugammadex available where the airway is not predicted difficult.
MAC of volatiles is higher in infants than adults for many agents; sevoflurane remains the workhorse inhalational agent. Residual volatile and opioid effect after short cases still matter when FRC is small and VO2 is high.
[4]Linking numbers to crisis timelines
A viva-quality synthesis:
[1]- Preoxygenation buys limited time because oxygen store (FRC × FAO2) is small and consumption is high.
- Airway obstruction or apnoea → SpO2 falls in tens of seconds to a few minutes depending on age and preoxygenation quality.
- Hypoxaemia → bradycardia → cardiac output collapse → arrest.
- Therefore every paediatric airway plan is also a cardiac output plan.
This is why the same laryngospasm that is annoying in an adult is a near-arrest pathway in an infant, and why concurrent URI multiplies risk in a population that already desaturates fast.
[3]Primary science SAQ numbers checklist
- VO2 infant ~6 mL/kg/min; adult ~3 mL/kg/min
- Closing capacity near FRC in infants
- CO heart-rate dependent
- HbF left-shifted dissociation curve
- BSA:mass high → heat loss
- PVR rises with hypoxia/hypercarbia/acidosis
Deep dive: oxygen stores and apnoea mathematics
The safe apnoea time after preoxygenation is conceptually the usable oxygen store divided by oxygen consumption. In the adult, FRC is large and VO2 is about 3 mL/kg/min. In the infant, FRC is small in absolute terms, closing capacity encroaches on FRC so the effective oxygen store is further reduced by early airway closure and shunt, and VO2 is about 6 mL/kg/min. The result is not a minor difference — it is an order-of-magnitude change in how long the anaesthetist can safely look away from the airway.
[1]Teaching numbers candidates should be ready to state:
[1]- Infant VO2 approximately 6 mL/kg/min (about twice adult weight-indexed values)
- Adult VO2 approximately 3 mL/kg/min
- Infant closing capacity near or above FRC during tidal breathing, especially under anaesthesia
- Preoxygenation remains mandatory even though the bought time is short
- Desaturation after apnoea often occurs in tens of seconds to a few minutes depending on age, residual FRC oxygen fraction, haemoglobin, and cardiac output
A viva-quality synthesis: “I preoxygenate meticulously, minimise apnoea, and treat any airway obstruction as an oxygen-delivery emergency because consumption is high and stores are low.”
[1]Chest wall mechanics and ventilator strategy
The highly compliant chest wall means applied positive pressure preferentially moves the chest wall outward and can also insufflate the stomach if peak pressures are high and the airway is partially obstructed. Gastric insufflation elevates the diaphragm, reduces FRC further, and creates a vicious cycle of worse ventilation. Practical rules:
[1]- Use appropriate mask seal and early advanced airway when mask ventilation is difficult
- Decompress the stomach with an orogastric tube when gastric distension limits ventilation
- Prefer controlled gentle ventilation once the airway is secured rather than heroic high-pressure mask breaths
- In neonates, high mean airway pressure can also impede venous return in parallel with the respiratory story
Horizontal ribs reduce the bucket-handle contribution of the rib cage; diaphragmatic descent does most of the inspiratory work. Anything that splints the diaphragm — abdominal compartment, laparoscopic insufflation, bowel obstruction — is therefore a ventilatory emergency in infants more than in older children.
[3]Haemoglobin, CaO2, and anaemia tolerance
Arterial oxygen content is approximately (1.34 × Hb × SaO2) + (0.003 × PaO2). With limited stroke-volume reserve, the infant cannot compensate for anaemia by large increases in stroke volume the way a healthy adolescent athlete might. Fetal haemoglobin’s higher oxygen affinity favours placental uptake but unloads less readily at tissue PO2; as HbF declines over the first months, unloading improves. Practical implications:
[1]- Treat significant anaemia before major elective surgery when feasible
- In cyanotic congenital heart disease, a higher haematocrit may be required for adequate oxygen delivery — individualise with cardiology
- During crisis, raise FiO2 and restore heart rate first; content still matters if Hb is critically low
Cardiovascular reflexes under anaesthesia
Hypoxia-induced bradycardia is the dominant dangerous reflex. Additional bradycardic stimuli include:
[1]- Laryngoscopy and airway suction (vagal)
- Suxamethonium (especially second dose, and in infants)
- High-dose opioids (especially remifentanil boluses)
- Oculocardiac reflex in strabismus surgery
- Peritoneal traction and extreme surgical stimulation at light planes
Atropine readiness (commonly 20 micrograms/kg IV per PALS/APLS charting, with local minimum practical dose rules) does not replace oxygenation. Chest compressions follow institutional arrest thresholds when output is inadequate despite airway manoeuvres.
[1]Pulmonary vascular resistance levers
PVR rises with hypoxia, hypercarbia, acidosis, high mean airway pressure, atelectasis, and cold. PVR falls with oxygen, normocapnia or mild hypocapnia depending on context, alkalosis, and recruitment of lung units. In neonates with transitional circulation residues or known PPHN risk, anaesthetic plans explicitly avoid PVR crises: gentle ventilation, temperature control, adequate anaesthesia depth, and early ICU involvement if pulmonary hypertensive crisis develops. Inhaled nitric oxide and advanced therapies sit in the NICU/PICU toolkit rather than every routine list.
[1]Thermoregulation mechanisms and theatre conduct
Neonates rely on non-shivering thermogenesis via brown fat; anaesthesia impairs thermoregulatory responses. Heat loss pathways: radiation to cold rooms, convection from airflow, evaporation from wet skin and open cavities, and conduction to cold tables. A practical bundle:
[1]- Warm the room before the neonate arrives
- Forced-air warming from induction
- Cover head and extremities
- Warm fluids and, for major cases, blood products
- Minimise exposure time during line placement
- Continuous temperature monitoring for all but the shortest cases
Hypothermia worsens coagulopathy, drug duration, respiratory drive, and oxygen consumption during recovery — it is a safety issue, not a comfort preference.
[1]Linking physiology to induction technique choice
Inhalational induction remains common when IV access is delayed, but the apnoeic window after deep sevoflurane induction is short. IV induction with carefully titrated agents requires prior access and still demands preoxygenation. For the critically ill child, the physiology of heart-rate-dependent cardiac output argues against high-dose propofol boluses without vasopressor readiness. Modified RSI in children balances aspiration risk against rapid desaturation — gentle ventilation is often preferred over prolonged apnoea.
[3]Primary examination number drill
Candidates sitting primary-level physiology vivas should be able to reproduce without hesitation:
[1]- VO2 infant versus adult
- Closing capacity versus FRC relationship
- CO approximately HR × limited SV
- Hypoxia causes bradycardia in infants
- HbF left-shifted dissociation curve
- High surface-area-to-mass ratio → heat loss
- PVR triggers: hypoxia, hypercarbia, acidosis
- Approximate infant respiratory rate and heart-rate norms by age band (quote local PALS card)
Clinical scenarios that bind the physiology
Scenario A — two-month-old for pyloric stenosis: dehydration and electrolyte issues dominate fluids topics, but respiratory physiology still demands preoxygenation, careful aspiration risk management, and temperature care.
[3]Scenario B — ex-preterm for hernia: same cardiorespiratory fragility plus Coté-informed apnoea monitoring by post-menstrual age.
[1]Scenario C — infant with viral URI for elective ENT: laryngospasm risk multiplied; desaturation cascade faster than adult; consider deferral when appropriate.
[3]Scenario D — neonate with congenital diaphragmatic hernia: FRC and pulmonary hypoplasia physiology; avoid gastric distension; PVR awareness.
[1]Monitoring set-points and alarm literacy
Adult default bradycardia alarms are too low for neonates and infants. Set age-appropriate HR and BP alarms before induction. Capnography may show small waveforms with leaks around uncuffed tubes — interpret trends carefully. Pre- and post-ductal SpO2 probes matter when ductal shunting is possible. Near-infrared spectroscopy appears in cardiac and neonatal pathways as a regional oxygenation adjunct, not a replacement for the basic monitors.
[4]Fluid bolus physiology interaction
A 10–20 mL/kg isotonic bolus can restore preload, but the non-compliant ventricle and ductal physiology mean overload is poorly tolerated in some cardiac lesions. Reassess after every bolus: liver edge, SpO2, airway pressures, and lactate. Physiology forbids “automatic three boluses” without examination.
[1]Drug dosing anchors tied to physiology
- Atropine ~20 microg/kg IV for bradycardia pathways
- Adrenaline 10 microg/kg IV/IO for arrest
- Fluid 10–20 mL/kg isotonic with reassessment
- Suxamethonium historically higher mg/kg in infants with bradycardia risk — many prefer rocuronium when airway not predicted difficult
- MAC of sevoflurane higher in infants than adults for many contexts — yet haemodynamic sensitivity in the sick infant still requires titration
Synthesis paragraph for SAQ endings
Infants live close to the edge of oxygen supply and demand. High consumption, small effective stores, airway closure near FRC, and heart-rate-dependent cardiac output create a short crisis timeline from obstruction to hypoxic bradycardia to arrest. Every anaesthetic plan that prioritises preoxygenation, airway excellence, heart-rate protection, temperature, and avoidance of PVR triggers is simply applied physiology.
[4]Extended viva model answers
Why does the infant desaturate faster?
“Weight-indexed oxygen consumption is about 6 mL/kg/min, roughly double adult values, while absolute FRC is small and closing capacity encroaches on FRC. Under anaesthesia FRC falls further, promoting airway closure and shunt. The usable oxygen store is therefore small and consumption is high, so SpO2 falls within tens of seconds to a few minutes despite preoxygenation.”
Why is bradycardia more dangerous at six weeks than at sixteen years?
“Stroke volume reserve is limited; cardiac output is largely heart-rate dependent. Hypoxic bradycardia therefore collapses oxygen delivery immediately. In older children and adults, tachycardia often appears first and stroke volume can increase.”
How do you set your monitors differently?
“Age-adjusted HR and BP alarms, meticulous SpO2 and EtCO2, continuous temperature for all but the shortest cases, and readiness for atropine and airway rescue. I treat bradycardia as an oxygen-delivery emergency.”
Exam day one-page checklist
- Quote VO2 ~6 mL/kg/min
- Quote closing capacity near FRC
- State CO ≈ HR × limited SV
- Preoxygenate; minimise apnoea
- Warm actively
- Avoid PVR triggers in neonates
- Atropine ready; oxygen first
- Link URI to faster crisis, not only higher incidence
Cross-links without duplication
Airway sizing, ex-preterm apnoea monitoring, fluids/glucose, and CHD shunt balance are separate leaves — use physiology language as the shared foundation rather than repeating full topics.
[1]Age-band cardiorespiratory norms (exam utility)
While exact centiles vary by source, candidates should know the direction of change with age: neonates have the highest heart rates and respiratory rates, with progressive decline toward adult values through childhood. Blood pressure rises with age. Always set monitor alarms to age-appropriate limits before induction rather than accepting adult defaults. Quote a PALS/APLS card in the exam if asked for precise bands rather than inventing false precision.
[1]Work of breathing and fatigue
Infant respiratory muscles fatigue faster; high closing capacity and compliant chest wall increase the work of maintaining FRC. Under anaesthesia, loss of tone reduces FRC; in recovery, residual volatile and opioid effects on a high-VO2 infant can produce hypoventilation and desaturation. That is why PACU monitoring intensity must match age and comorbidities, not only surgical magnitude.
[1]Putting the desaturation cascade in one diagram of words
High VO2 + small O2 store → rapid fall in SpO2 with apnoea → hypoxia-induced bradycardia → fall in cardiac output → further fall in oxygen delivery → cardiac arrest. Interventions map onto the cascade: preoxygenation and airway open the top; atropine and CPR address the bottom; both ends matter.
[1]Common traps
Treating infant bradycardia as pure vagal without oxygenating; applying adult desaturation timelines; ignoring temperature under drapes; over-ventilating and causing gastric distension that further impairs lungs; quoting HbF without linking to oxygen unloading; confusing chronological age with post-menstrual age when discussing apnoea risk.
[1]

References
- [1]Davidson AJ, Disma N, de Graaff JC, et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS): an international multicentre, randomised controlled trial Lancet, 2016.PMID 26507180
- [2]McCann ME, de Graaff JC, Dorris L, et al. Neurodevelopmental outcome at 5 years of age after general anaesthesia or awake-regional anaesthesia in infancy (GAS): an international, multicentre, randomised, controlled equivalence trial Lancet, 2019.PMID 30782342
- [3]Flick RP, Wilder RT, Pieper SF, et al. Risk factors for laryngospasm in children during general anesthesia Paediatr Anaesth, 2008.PMID 18315633
- [4]Coté CJ, Zaslavsky A, Downes JJ, et al. Postoperative apnea in former preterm infants after inguinal herniorrhaphy. A combined analysis Anesthesiology, 1995.PMID 7717551
- [5]Sikich N, Lerman J Development and psychometric evaluation of the pediatric anesthesia emergence delirium scale Anesthesiology, 2004.PMID 15114210