Anaes · Paediatric anaesthesia
The sick child: sepsis, resuscitation, and congenital heart disease for anaesthesia
Also known as Paediatric septic shock anaesthesia · Congenital heart disease anaesthesia · Balanced circulation shunt · Sick child induction
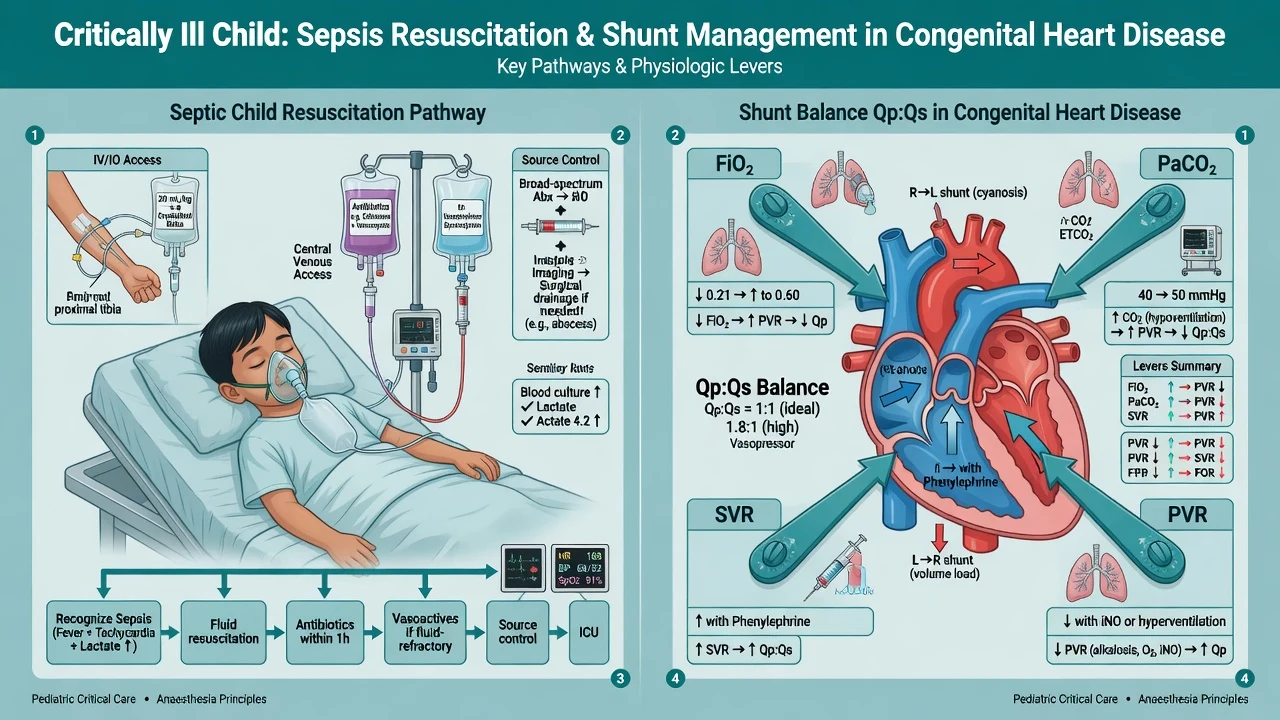
Anaesthesia for the critically ill child covering septic shock resuscitation (Surviving Sepsis Campaign paediatrics), induction of the septic child, and congenital heart disease principles including shunt balance, air precautions, and NAP7 high-risk context.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Why this is examined
The sick child is where paediatric anaesthesia becomes resuscitation. Examiners probe recognition of decompensation, SSC-guided sepsis care, induction without collapse, and lesion-specific CHD goals. NAP7 highlighted infants and congenital heart disease as highest-risk groups for perioperative cardiac arrest — expect that framing.
[1]Recognition of the critically ill child
Look for work of breathing, conscious level, mottling, prolonged CRT, tachycardia then bradycardia (preterminal), hypotension (late in children), oliguria, lactate rise, and fever or hypothermia. Use local paediatric early warning scores. Do not wait for hypotension to declare shock.
[1]Septic shock — resuscitation before aesthetics
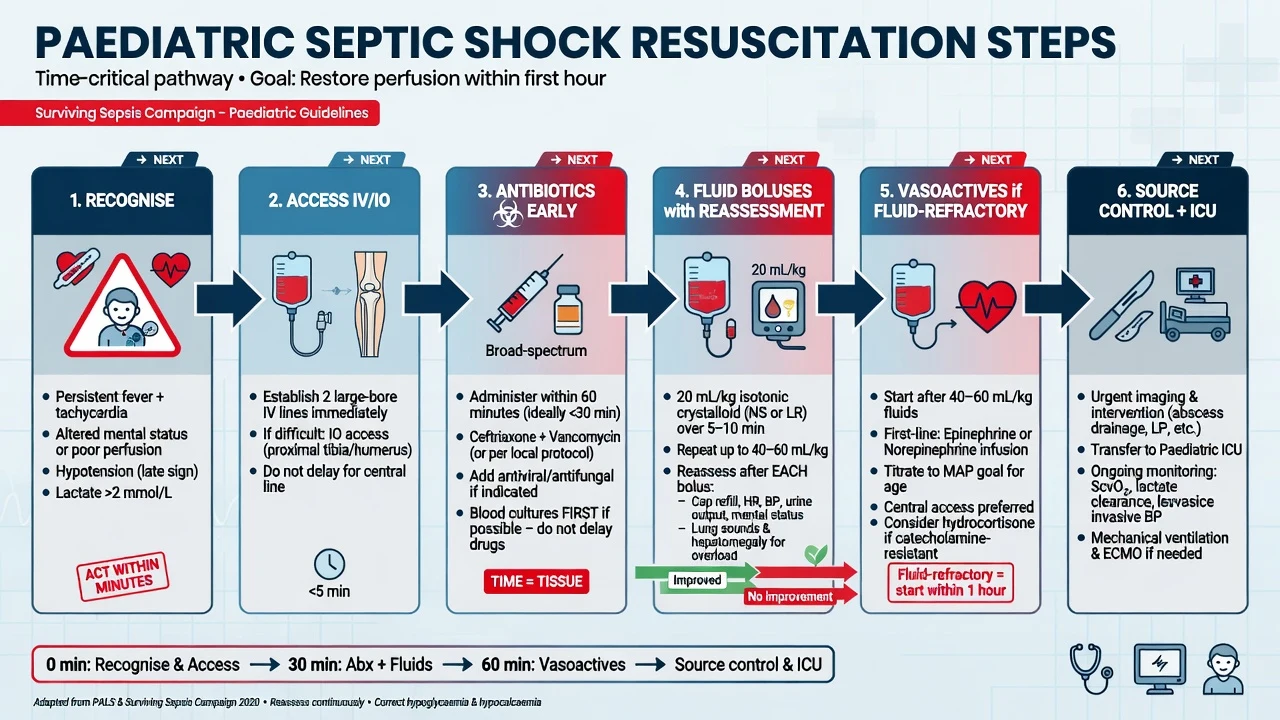
Paediatric Surviving Sepsis Campaign guidance emphasises early recognition, timely antimicrobials, source control, fluid resuscitation with reassessment, and vasoactive support when fluid-refractory.[1][2]
Practical theatre-adjacent algorithm
- ABC with high-flow oxygen; early senior help and ICU
- IV/IO access — do not delay for perfect veins
- Cultures if they do not delay therapy; antibiotics within the first hour of recognition when shock is present
- Fluid boluses of balanced crystalloid (commonly 10–20 mL/kg aliquots) with reassessment after each for overload (hepatomegaly, crackles, rising CVP pattern)
- Vasoactive infusion early if fluid-refractory — adrenaline or noradrenaline commonly used as first-line depending on phenotype (cold vs warm shock patterns) and unit protocol; dopamine still appears in some pathways but is not the modern default everywhere
- Source control — theatre may be the therapy (appendiceal abscess, necrotising soft tissue, obstructed urinary sepsis)
- Glucose and calcium — correct hypoglycaemia and ionised hypocalcaemia
- Steroids — consider for catecholamine-resistant shock or known adrenal risk (protocolised)
Anaesthetic induction of the septic child
Goals: maintain coronary and cerebral perfusion pressure, secure airway without hypoxia/bradycardia cascade, continue resuscitation.
[1]- Prefer IV/IO access first when feasible
- Ketamine 1–2 mg/kg IV often preferred for haemodynamic stability (still can cause collapse if extreme hypovolaemia)
- Carefully titrated propofol only with vasopressors running if used
- Avoid high-concentration sevoflurane induction in profound shock
- RSI / modified RSI for full stomach; have atropine ready for bradycardia
- Invasive arterial line early if shock; central access for vasoactives
- Ventilate gently — high PEEP/pressure can drop venous return in underfilled children
Congenital heart disease — exam framework
Classify lesions by physiology, not only by name:
[1]| Category | Examples | Anaesthetic focus |
|---|---|---|
| Left-to-right shunt | VSD, PDA, ASD | Avoid excessive SVR drop and high FiO2 if pulmonary overcirculation |
| Right-to-left shunt | Tetralogy, Eisenmenger physiology | Maintain SVR; avoid increased PVR (hypoxia, hypercarbia, acidosis) |
| Mixing / parallel | TGA (before switch), truncus | Balance systemic and pulmonary flow |
| Single ventricle / staged | Norwood, Glenn, Fontan | Understand passive pulmonary flow stages; careful ventilation and preload |
| Obstructive | AS, coarctation, HLHS variants | Coronary/systemic perfusion pressure critical |
Balanced circulation (Qp:Qs)
For duct-dependent or parallel circulations, systemic oxygen delivery depends on balancing pulmonary (Qp) and systemic (Qs) blood flow. Excess oxygen and low PVR can steal flow to lungs and underperfuse the body; high PVR can cause cyanosis. Manipulate FiO2, CO2, pH, and SVR thoughtfully with cardiology/ICU.
[1]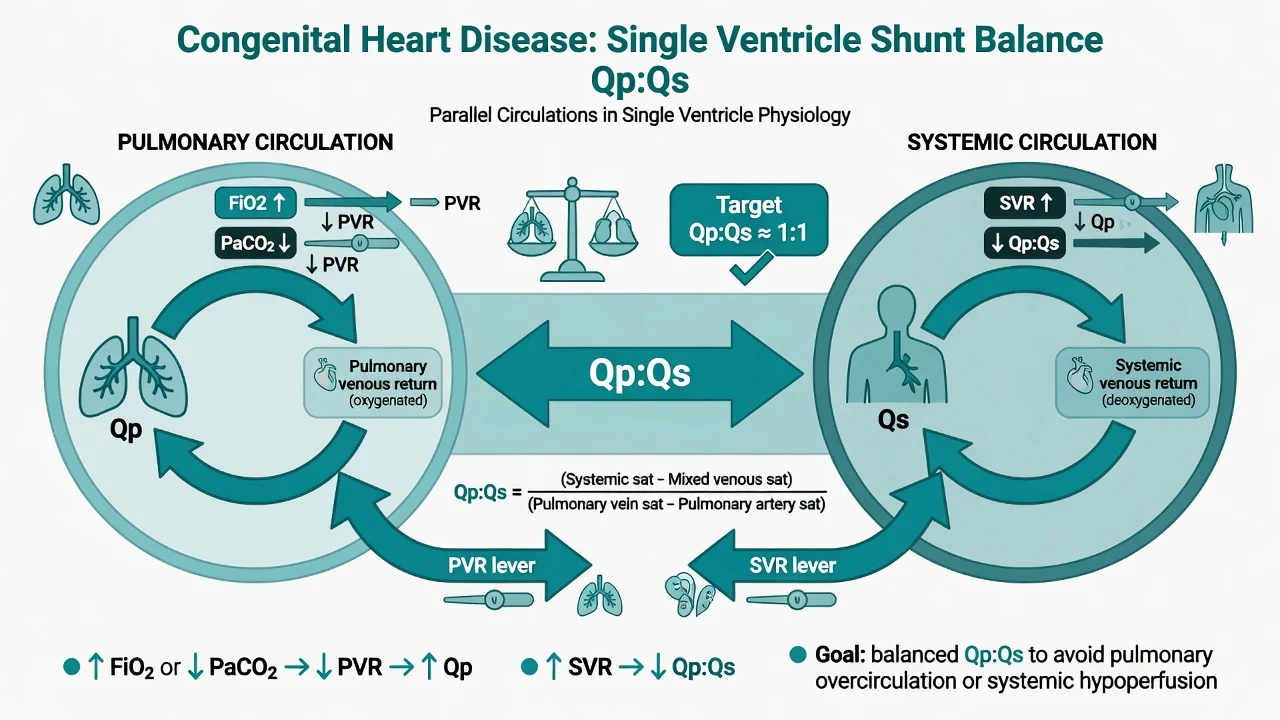
Air and endocarditis
- De-air all lines; use filters where policy dictates for right-to-left shunt risk
- Antibiotic prophylaxis only when guidelines indicate (not for every CHD patient every time)
- Endocarditis risk discussion is lesion- and procedure-specific
Monitoring and equipment
- Preinduction monitors when possible; SpO2 on both pre- and post-ductal sites if relevant
- Arterial line, central venous access, urine output, serial lactate/ABG
- Defibrillator, age-appropriate airway kit, emergency drugs drawn (adrenaline 10 microg/kg IV for arrest dosing context; dilute infusions per unit)
- ECMO/cardiac centre pathways for selected CHD and refractory shock
Intraoperative management pearls
- Continue antibiotics and vasoactives; never stop the infusion for a "neat" anaesthetic
- Match ventilation to lesion (Fontan: avoid high mean airway pressure that impedes passive PBF)
- Transfusion thresholds individualised; cyanotic children may need higher haematocrit for oxygen delivery
- Temperature control — sick children cool fast
Crisis pivots
- Hypotension on induction: fluids, reduce volatile/propofol, start/increase adrenaline or noradrenaline, rule out tension pneumothorax/equipment
- Tet spell: knee-chest/compress femoral vessels, oxygen, volume, deepen anaesthesia, phenylephrine to raise SVR, beta-blockade per unit practice, surgical readiness
- Bradycardia with hypoxia: treat airway first — paediatric arrest is usually hypoxic
Postoperative / ICU
Most septic and complex CHD children need HDU/ICU. Hand over goals: BP/SpO2 targets, vasoactive plan, antibiotic timing, glucose, surgical drains, and what constitutes deterioration.
[1]Special populations
- Neonates with duct-dependent lesions: prostaglandin infusion continuity is non-negotiable
- Fontan: sinus rhythm, preload, low PVR, early extubation when appropriate
- Pulmonary hypertension: avoid hypoxia/hypercarbia/acidosis/pain; have nitric oxide pathway available in specialist centres
SAQ answer scaffold
- Recognise and resuscitate septic shock (SSC pillars)
- Induction agents and monitoring for the septic child
- CHD classification and Qp:Qs balance
- Air precautions and crisis (tet spell / induction collapse)
- Disposition and communication
Viva stem bank
- "2-year-old with purpura and BP 70/40 needs source control — your anaesthetic plan?"
- "How does Surviving Sepsis Campaign change your first 15 minutes?"
- "This neonate is on prostaglandin — what must not stop?"
- "Explain balanced circulation for a single-ventricle infant."
Paediatric sepsis — first-hour detail
Surviving Sepsis Campaign paediatric guidance emphasises recognition, antimicrobial timing, fluid with reassessment, and vasoactives for fluid-refractory shock.[1][2] In theatre-adjacent practice:
- Call for senior paediatric ICU help early
- High-flow oxygen; support work of breathing; intubate if exhaustion or collapse with a haemodynamically thoughtful induction
- IV or IO access — IO is not failure, it is resuscitation
- Antibiotics after cultures only if cultures do not delay therapy
- Balanced crystalloid boluses 10–20 mL/kg, reassess liver edge, crackles, SpO2, lactate, and mentation after each
- Start adrenaline or noradrenaline infusions per phenotype and unit protocol when fluid-refractory
- Correct glucose and ionised calcium
- Source control timing negotiated with surgeons — theatre is part of resuscitation, not an alternative to it
Cold versus warm shock thinking
Classic teaching labels cold shock (low CO, high SVR) versus warm shock (vasodilated). Real children mix phenotypes over time. Adrenaline often supports CO in cold patterns; noradrenaline supports SVR in warm patterns; many units start a single agent and add a second based on response. Say “I will follow PICU protocol and titrate to perfusion, not to a single label.”
[1]Induction of the septic child — pharmacology
- Ketamine 1–2 mg/kg IV: usually most haemodynamically stable induction agent; still dangerous if empty venous reservoir
- Fentanyl small titrated doses: blunts response but can bradycardia
- Propofol: avoid large boluses in shock without vasopressors running
- Sevoflurane: slow careful titration only if IV access impossible — not for profound shock
- Rocuronium high dose for RSI when indicated; have sugammadex available where used
- Atropine ready for hypoxic bradycardia
Positive-pressure ventilation reduces venous return — start lower pressures and fill the tank.
[1]CHD classification for anaesthetists (physiology language)
Examiners reward physiology words: shunt direction, mixing, obstruction, single ventricle stage, pulmonary blood flow dependence.
[1]Left-to-right shunts (VSD, PDA, ASD)
Risk of pulmonary overcirculation with high FiO2 and low PVR. Avoid extreme vasodilation that drops diastolic coronary perfusion in some lesions. Air precautions still matter if any right-to-left possibility exists transiently.
[1]Right-to-left shunts (tetralogy, Eisenmenger physiology)
Maintain SVR; avoid rises in PVR (hypoxia, hypercarbia, acidosis, pain, high airway pressures). Tet spell algorithm: increase SVR (phenylephrine), oxygen, knee-chest/compress femorals, volume, deepen anaesthesia, beta-blockade per unit, surgical readiness.
[3]Mixing and parallel circulations
Balance Qp:Qs with FiO2, CO2 targets, and SVR/PVR manipulation with cardiology/ICU. Excess pulmonary flow steals from systemic perfusion — pink but acidotic is a classic trap.
[1]Single ventricle stages
- Norwood/shunt dependent: balanced circulation critical; prostaglandin continuity pre-repair
- Glenn: pulmonary flow partly passive from upper body veins — high PEEP and high mean airway pressure hurt
- Fontan: fully passive PBF depends on driving pressure from CVP to LA; sinus rhythm, preload, low PVR, early extubation when appropriate
Obstructive lesions
Critical AS, coarctation, HLHS variants: coronary or systemic perfusion pressure is everything; avoid tachycardia and vasodilation that empty the coronary gradient.
[1]Air embolism precautions
Right-to-left shunt pathways allow paradoxical emboli. De-air syringes and lines; use filters where policy dictates; never leave stopcocks open; careful when pressurising bags. This is a pure pass/fail safety behaviour in CHD viva stems.
[1]NAP7 high-risk framing
Infants under one year and children with congenital heart disease are highlighted among highest-risk groups for perioperative cardiac arrest — plan senior operators, full monitoring, and early rescue. Hypoxaemia remains a dominant pathway in small children.
[1]Emergency drug card thinking
- Adrenaline arrest dose 10 microg/kg IV/IO
- Fluid boluses 10–20 mL/kg with reassessment
- Atropine 20 microg/kg IV for bradycardia pathways per PALS/APLS charts
- Infusion dilutions per unit — do not invent exotic concentrations under stress
When neurotoxicity questions arise before septic surgery
Necessary source control and resuscitation dominate; brief necessary anaesthesia should not be delayed for theoretical neurotoxicity concerns; GAS-context reassurance applies to a different population but the ethical priority is the same: treat life-threatening disease first.[3]
Handover template to PICU
Diagnosis and source · antibiotics given and time · vasoactive infusions and concentrations · airway device and difficulties · ventilation settings · latest gas/lactate/glucose/Hb · surgical drains and bleeding · hemodynamic targets (BP, SpO2 for cyanotic lesions) · lines and access sites · parental awareness.
[1]Haemodynamic drug anchors (exam)
- Adrenaline arrest: 10 microg/kg IV/IO
- Fluid bolus: 10–20 mL/kg isotonic with reassessment
- Ketamine induction: 1–2 mg/kg IV
- Atropine: 20 microg/kg IV for bradycardia pathways
- Phenylephrine for tet spells: titrated IV boluses/infusion per unit to raise SVR
Always defer to current PALS/APLS and local PICU infusion charts for dilutions.
[1]Ventilation strategies by lesion class
Overcirculation L→R: avoid excessive oxygen and low PVR if systemic steal is an issue pre-repair.
R→L cyanotic: avoid PVR rises; support SVR.
Fontan/Glenn: minimise mean airway pressure; facilitate early spontaneous breathing when appropriate.
Pulmonary hypertension: prevent hypoxia/hypercarbia/acidosis/pain; iNO pathway in specialist centres.
Source control examples for theatre
Perforated appendicitis with septic shock, necrotising soft tissue infection, obstructed pyonephrosis, empyema drainage — antibiotics and resuscitation run in parallel with surgical urgency. Do not withhold antibiotics “until after induction.”
[1]Monitoring montage for the sick child
Preinduction SpO2/ECG/NIBP when possible; arterial line early in shock or complex CHD; central access for vasoactives; urine output; serial lactate/ABG/glucose/Hb; temperature; pre- and post-ductal SpO2 when relevant; defibrillator pads in high-risk CHD.
[1]Crisis resource management
Call for help early; use closed-loop communication; assign airway, drugs, and scribe roles; keep PICU informed; if cardiac arrest occurs, follow PALS with reversible cause search (Hs and Ts) including hypoxia first in children.
[1]Common traps
Pure sevoflurane induction of septic shock; flooding with oxygen in overcirculated shunt physiology; ignoring air in lines; treating hypotension with more volatile; delaying antibiotics for "theatre first."
[1] [1]Fellowship consolidation — sick child sepsis and congenital heart
[1]The sick child converts paediatric anaesthesia into resuscitation. NAP7-context teaching places infants and children with congenital heart disease among the highest-risk groups for perioperative cardiac arrest. Senior help, calculated emergency drugs, and full monitoring are non-negotiable.
[1]Recognise shock before hypotension: work of breathing, mottling, prolonged capillary refill, tachycardia progressing to bradycardia, altered consciousness, oliguria, and lactate rise. Hypotension is late. Use local paediatric early warning tools and call PICU early.
[1]Paediatric Surviving Sepsis Campaign pillars: early recognition, timely antimicrobials, source control, fluid resuscitation with reassessment, and vasoactive drugs for fluid-refractory shock. Antibiotics should not wait for theatre if shock is present. Cultures are taken only if they do not delay therapy.
[1]Fluid boluses of balanced crystalloid commonly 10 to 20 mL/kg with reassessment after each for hepatomegaly, crackles, worsening oxygenation, or rising venous pressures. Start adrenaline or noradrenaline infusions per unit phenotype pathways when fluid-refractory. Correct hypoglycaemia and ionised hypocalcaemia. Consider steroids for catecholamine-resistant shock or known adrenal risk.
[1]Induction of the septic child: secure IV or IO access first when feasible, prefer ketamine 1 to 2 mg/kg IV with vasopressors ready, avoid large propofol boluses in empty patients, ready atropine for bradycardia, use modified RSI when full stomach risk exists, and ventilate gently because high intrathoracic pressure drops venous return.
[1]Congenital heart disease is managed by physiology class: left-to-right shunt, right-to-left shunt, mixing or parallel circulations, single-ventricle staged physiology, and obstructive lesions. Balance Qp to Qs using FiO2, carbon dioxide, pH, SVR, and PVR with cardiology and ICU partnership.
[1]Right-to-left shunt and mixing lesions demand meticulous de-airing of lines because paradoxical emboli are possible. Maintain prostaglandin infusions for duct-dependent lesions without interruption. Cyanotic children may need higher haematocrit targets for oxygen delivery.
[1]Tet spell algorithm: 100 percent oxygen, knee-chest or femoral compression to raise SVR, volume, deepen anaesthesia, phenylephrine to raise SVR, beta-blockade per unit practice, correct acidosis, and surgical readiness if refractory.
[3]Fontan and Glenn circulations depend on passive or partially passive pulmonary blood flow. High mean airway pressure, hypovolaemia, and loss of sinus rhythm are poorly tolerated. Early extubation strategies are often preferred when otherwise appropriate.
[1]Handover to PICU must include antibiotic times, vasoactive concentrations, SpO2 and blood pressure targets for the lesion, latest gas and lactate, airway details, and what deterioration looks like for this child. Necessary emergency surgery is not delayed for theoretical neurotoxicity debates.
[1] [1]Dual-path viva stems with model openers
Stem 1: "A 2-year-old with purpura fulminans needs source control in theatre. BP is 70/40."
Opener: "This is septic shock. I will call for senior and PICU help, give oxygen, obtain IV or IO access, give antibiotics immediately, give isotonic fluid boluses of 10 to 20 mL/kg with reassessment, start vasoactives if fluid-refractory, correct glucose and calcium, and induce with ketamine and full monitoring only when resuscitation is underway."
Stem 2: "Neonate on prostaglandin for duct-dependent systemic flow needs emergency laparotomy."
Opener: "I will continue prostaglandin without interruption, understand Qp to Qs balance, avoid extreme oxygen and ventilation changes without a plan, de-air all lines, use senior cardiac-capable help, and match SpO2 targets to cardiology advice rather than forcing 100 percent saturation."
Stem 3: "Child with repaired tetralogy becomes deeply cyanosed and hypotensive during emergence stimulation."
Opener: "I will treat this as a spell physiology: 100 percent oxygen, raise SVR with phenylephrine, volume, deepen anaesthesia if still under care, knee-chest positioning principles, and call for help while protecting the airway."
Equipment and drug preparation list
Weight-based emergency card on the machine; adrenaline 10 microg/kg arrest dose calculated; atropine 20 microg/kg calculated; fluid boluses prepared; ketamine drawn; airway kit with correct ETT sizes; defibrillator; arterial line kit; central access kit; blood products if indicated; PICU bed confirmed. For CHD cases add air filters per policy and clear SpO2 target bands written on the board.
[1]What good looks like in a crisis
Closed-loop communication, early call for help, simultaneous rather than sequential resuscitation tasks, refusal to perform pure inhalational induction in profound shock, and clear handover that preserves antibiotic timing and vasoactive continuity.
[1] [1]Balanced circulation arithmetic and practical theatre examples
In parallel circulations and many duct-dependent lesions, systemic oxygen delivery depends on the balance between pulmonary blood flow (Qp) and systemic blood flow (Qs). If Qp is excessively high because pulmonary vascular resistance is low and FiO2 is high, the child may look pink while becoming acidotic from systemic hypoperfusion. If Qp is too low because pulmonary vascular resistance is high, cyanosis and inadequate pulmonary blood flow dominate. The anaesthetic levers are FiO2, carbon dioxide and pH targets, mean airway pressure, temperature, depth of anaesthesia, and vasoactive drugs that change SVR and PVR. None of these levers should be manipulated without a lesion-specific plan agreed with cardiology and intensive care.
[3]Practical theatre example: a neonate with hypoplastic left heart physiology awaiting stage palliation who needs emergency non-cardiac surgery. Continue prostaglandin. Avoid automatic 100 percent oxygen. Agree SpO2 target bands. De-air lines. Prepare for haemodynamic collapse at induction with ketamine, calcium availability, and adrenaline infusion readiness. Ventilate enough to avoid hypercarbia-induced PVR spikes but not so aggressively that pulmonary overcirculation steals systemic flow.
[1]Practical theatre example: septic child with previously repaired congenital heart disease and residual pulmonary hypertension. Sepsis lowers SVR and may destabilise right ventricular function. Resuscitate sepsis first, maintain coronary perfusion pressure, avoid hypoxia and hypercarbia, and have pulmonary vasodilator pathways available in specialist centres. Induction is a shared resuscitation event, not a separate aesthetic phase.
[1]These examples show why the sick-child topic is not two disconnected essays. Sepsis resuscitation principles and congenital heart physiology meet whenever a complex child becomes critically ill, and the viva rewards candidates who can switch languages fluidly between SSC pillars and shunt physiology without losing the airway and blood pressure plot.
[1] [1]Final synthesis and rapid numbers card
- Fluid boluses 10 to 20 mL/kg isotonic with reassessment
- Antibiotics early in shock, not after the knife comes down
- Ketamine induction 1 to 2 mg/kg IV when access exists
- Adrenaline arrest dose 10 micrograms per kilogram IV or IO
- Atropine 20 micrograms per kilogram IV for bradycardia pathways
- Continue prostaglandin in duct-dependent lesions
- De-air lines for right-to-left shunt risk
- Match SpO2 targets to lesion physiology
- Call senior help early for infants and complex CHD
The viva pass phrase: resuscitate first, induce gently, balance the circulation, and never stop the drugs that are keeping the child alive for the sake of a tidy anaesthetic sequence.
[1]References
- [1]Weiss SL et al. Surviving Sepsis Campaign International Guidelines for the Management of Septic Shock and Sepsis-Associated Organ Dysfunction in Children. Pediatric Critical Care Medicine, 2020.PMID 32032273
- [2]Weiss SL et al. Surviving Sepsis Campaign International Guidelines for the Management of Sepsis and Septic Shock in Children 2026. Pediatric Critical Care Medicine, 2026.PMID 41869844
- [3]Davidson AJ et al. Neurodevelopmental outcome at 2 years of age after general anaesthesia and awake-regional anaesthesia in infancy (GAS): an international multicentre, randomised controlled trial. Lancet, 2016.PMID 26507180