EM · Toxicology and environmental emergencies
Bites and stings
Also known as Mammalian bite · Dog bite · Cat bite · Human bite · Clenched-fist injury · Insect sting · Bee sting · Wasp sting · Stingray injury · Marine puncture wound · Snake bite · Elapid envenomation · Pressure immobilisation bandage · Redback spider bite · Funnel-web spider bite · Latrodectism · Box jellyfish sting · Blue-ringed octopus bite · Stonefish sting · Venom-induced consumption coagulopathy
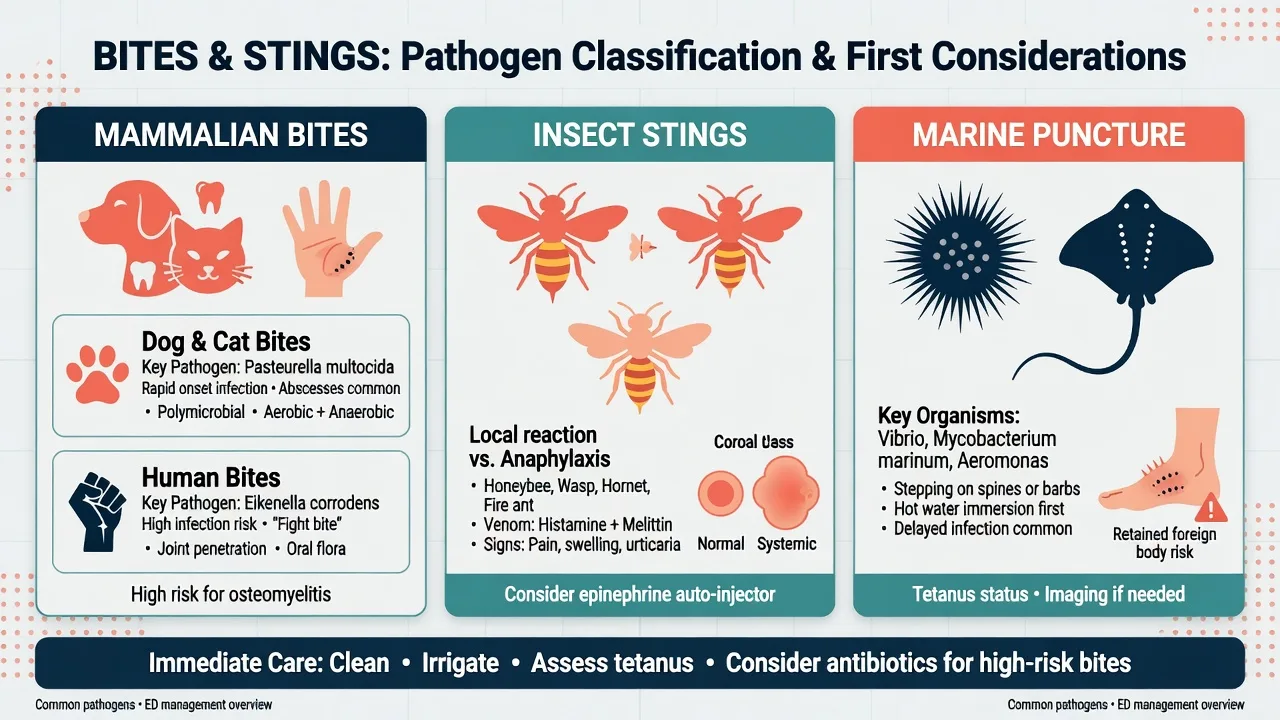
Bites and stings common to the Australasian emergency department — mammalian bites (dog, cat, human), insect stings (bee and wasp), and stingray puncture injuries. Cat and dog bites seed Pasteurella multocida, which establishes infection within 12 hours; human bites seed Eikenella corrodens, and the clenched-fist injury is an orthopaedic emergency because it penetrates the metacarpophalangeal joint. The single antibiotic covering the full bite-flora spectrum is amoxicillin-clavulanate 875/125 mg orally twice daily for five to seven days; flucloxacillin and cephalexin alone miss Pasteurella and Eikenella. Stingray venom is heat-labile — immerse the limb in water at 45 °C for 30 to 90 minutes, then explore every wound for a retained barb fragment and the integumentary sheath. Bee and wasp stings cause local reactions managed with antihistamines and cold packs, and systemic anaphylaxis managed with intramuscular adrenaline. Tetanus prophylaxis is addressed on every bite; rabies post-exposure prophylaxis is considered for bat bites anywhere and for dog bites sustained overseas.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Bites and stings are bread-and-butter emergency medicine, and the Fellowship examiner probes them in the SCQ/MCQ and OSCE more often than the SAQ. The candidate must hold three microbiology patterns (mammalian oral flora, heat-labile marine venom, and Hymenoptera hypersensitivity), one universal antibiotic (amoxicillin-clavulanate), and two prophylaxis obligations (tetanus on every bite, rabies for the overseas dog or any bat exposure). This topic also carries the antivenom-requiring envenomations — elapid and viper snakebite, funnel-web and redback spider, and the marine triumvirate of box jellyfish, blue-ringed octopus, and stonefish — because each turns on a single first-aid or antivenom fact the candidate must reproduce verbatim.[13]
Definition and classification
Bites and stings fall into three groups by mechanism and microbiology. Mammalian bites — dog, cat, human, and occasionally monkey or other species — are polymicrobial wounds seeded with the oral flora of the biter. Arthropod stings — overwhelmingly bee, wasp and (covered separately) ant — deliver venom through a stinger and produce local toxic reactions and, in the sensitised, IgE-mediated anaphylaxis. Marine puncture injuries — stingray, sea urchin, and other spine-bearing animals — drive a physical wound and a heat-labile venom.[3]
The clinical distinction that matters most is the hand bite, which carries the highest morbidity of any mammalian bite because the teeth penetrate joint, tendon sheath and bone. Within the hand bites, the clenched-fist (fight-bite) injury — a human tooth wound over the metacarpophalangeal joint sustained in a punch — is the archetypal orthopaedic emergency.[2]
Epidemiology and microbiology
Dog bites are the commonest mammalian bite overall; cat bites are the most likely to become infected (infection rates up to 50 percent versus 15 percent for dogs), because cat teeth are long, thin needles that deposit flora deep into tendon and joint. Human bites carry the highest morbidity per wound, overwhelmingly because of the clenched-fist mechanism.[2][3]
The microbiology is polymicrobial, mixing aerobic and anaerobic oral flora. The single organism the candidate must name for each source:[2]
The signature organism by bite source
Anaerobes (Bacteroides, Prevotella, Fusobacterium) and streptococci co-infect most wounds; Staphylococcus aureus and group A streptococci are also common, particularly in established infection.[2]
Pathophysiology — why bites behave the way they do
Three mechanisms determine severity. Crush versus puncture — dog bites crush and lacerate, producing devitalised tissue that is easy to see and to clean; cat and human bites puncture, driving deep contamination through a small visible wound that closes over, leaving infection to establish out of sight. Pasteurella virulence — Pasteurella multocida is non-motile but replicates rapidly, producing cellulitis and lymphangitis within 12 hours, far faster than typical staphylococcal cellulitis. Joint and tendon sheath penetration — at the hand, the extensor tendons over the metacarpophalangeal joints lie millimetres beneath the skin; a tooth that penetrates at the moment of fist closure seeds the joint space and the tendon sheath, leading to septic arthritis and pyogenic flexor tenosynovitis.[2][3]
[5]Clinical presentation
A mammalian bite presents at one of three stages. The fresh bite (within hours) shows tooth-mark lacerations or punctures, variable bleeding, and local pain without spreading redness. The early infected bite (12 to 48 hours, classically a cat bite) shows throbbing pain, spreading cellulitis, purulent discharge, and regional lymphadenopathy and lymphangitis — the rapidity is the clue to Pasteurella. The late or neglected bite presents with established abscess, septic arthritis of the hand, pyogenic tenosynovitis (Kanavel signs — fusiform swelling, flexed posture, tenderness along the tendon sheath, pain on passive extension), or systemic sepsis, particularly in the asplenic patient with Capnocytophaga.[3]
A stingray injury presents with immediate, severe, radiating pain at a puncture or laceration, typically on the foot or ankle (waders) or the hand (handling the animal). The wound may show a retained barb fragment. Systemic features — diaphoresis, nausea, dyspnoea, hypotension — can occur with large envenomations but are uncommon.[4]
A bee or wasp sting presents with immediate local pain, a central punctum, and a local wheal-and-flare. The bee leaves its barbed stinger and venom sac in the skin; the wasp can sting repeatedly and retains its stinger. The dangerous presentation is systemic anaphylaxis within minutes — urticaria, angioedema, stridor, wheeze, hypotension, abdominal cramping, collapse.[16]
Differential diagnosis
The differential splits by presentation: the rapidly progressive cellulitis and the collapsed patient after a sting.[9]
Pasteurella cellulitis (cat/dog bite)
- Onset 12 to 24 hours after the bite — faster than staphylococcal cellulitis
- Purulent discharge, lymphangitis, regional adenopathy; puncture wound often small
- Amoxicillin-clavulanate 875/125 mg PO BD; flucloxacillin alone fails
Septic arthritis / tenosynovitis (clenched-fist)
- Pain, swelling, and reduced movement at a metacarpophalangeal joint after a punch
- Kanavel signs if flexor sheath involved; joint held in flexion
- Surgical washout plus intravenous antibiotics; never close; refer to hand surgery
Necrotising soft tissue infection
- Pain out of proportion, rapid spread, systemic toxicity, skin necrosis or crepitus
- Can follow any contaminated bite, especially in diabetes or immunocompromise
- Surgical emergency — broad-spectrum antibiotics plus urgent debridement
Capnocytophaga sepsis (asplenic)
- Overwhelming sepsis with purpura fulminans 1 to 7 days after a dog bite
- Asplenia, alcoholism, or immunocompromise
- Blood cultures; broad-spectrum IV antibiotics covering the organism; intensive care
Anaphylaxis (insect sting)
- Urticaria, angioedema, stridor, wheeze, hypotension within minutes of a sting
- No spreading cellulitis; biphasic reactions can recur 6 to 12 hours later
- Adrenaline 0.5 mg IM to the anterolateral thigh; fluid; observation for 6 to 12 hours
Bedside assessment
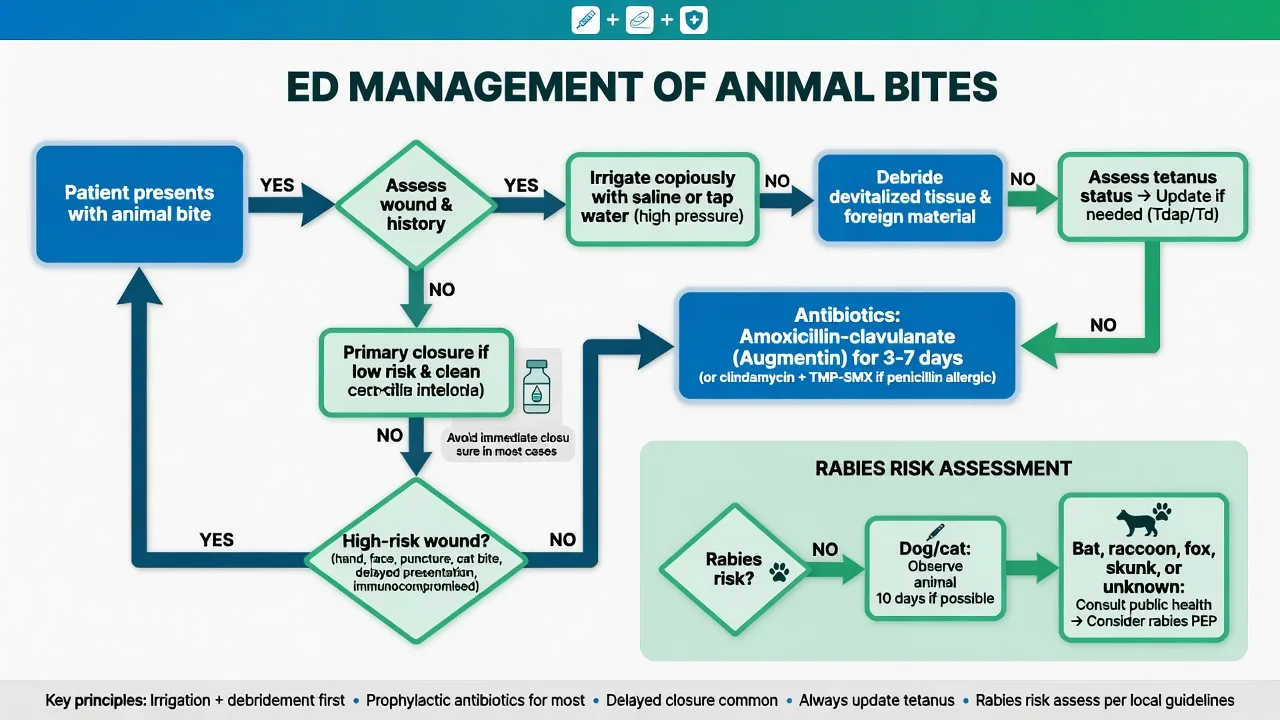
The history establishes the biter, the site, the time, the mechanism (did the patient punch the biter, or were they bitten), the immune status (asplenia, diabetes, immunosuppression, liver disease), the tetanus status, and the geography (overseas dog or monkey, bat exposure). The examination documents the wound depth, the presence of purulence, the range of movement at any involved joint, the neurovascular status distally, the regional lymph nodes, and the Kanavel signs at the hand. Every bite to the hand is examined for tendon and joint involvement — gently explore with a sterile probe; do not probe aggressively in the numbed hand without proper local anaesthesia and a bloodless field. For stingray injury, examine for a retained barb before applying hot water (though hot water is started immediately for pain regardless).[3]
Investigations
Most mammalian bites are managed clinically. Send a wound swab for microscopy and culture only if the wound is clinically infected (purulence, cellulitis) — routine swabbing of uninfected bites is not useful and colonises the result with oral flora. An X-ray of the bitten hand or any deep puncture looks for a retained tooth fragment, air within a joint, or periosteal reaction suggesting osteomyelitis. Bloods (full blood count, electrolytes, inflammatory markers, blood cultures) are reserved for the systemically unwell, the septic, and the immunocompromised. For stingray injury, X-ray or ultrasound the wound for a retained barb fragment — the barb is radiopaque.[2]
Wound management and antibiotic prophylaxis
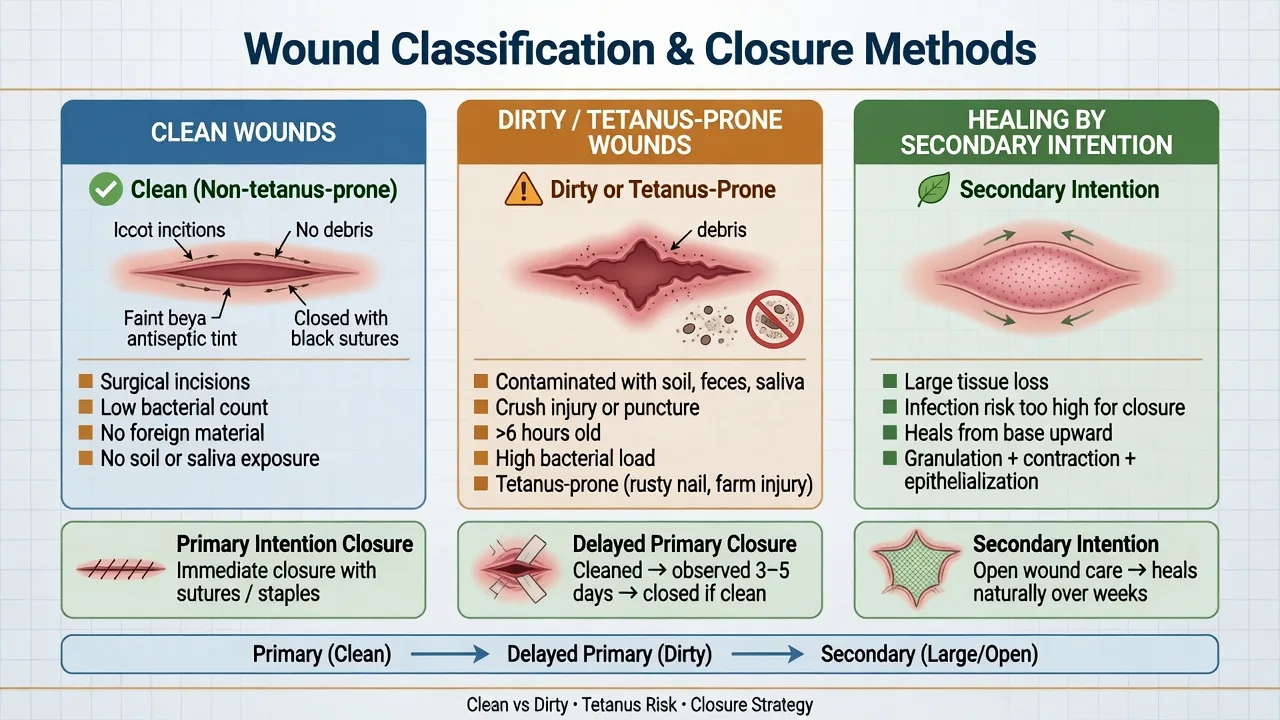
Wound care follows the principles of any contaminated wound: copious irrigation with normal saline, debridement of devitalised tissue, and removal of any foreign body. Most mammalian bites are left open or closed loosely — bites to the face may be primarily closed for cosmetic reasons after thorough irrigation, but bites to the hand, foot, or puncture wounds are not closed primarily.[1][3]
Antibiotic prophylaxis is given to all cat bites, all human bites, all hand bites, all deep puncture wounds, all wounds in the immunocompromised, and any wound more than 24 hours old. The single agent of choice that covers the full bite-flora spectrum — Pasteurella, Eikenella, streptococci, staphylococci, and anaerobes — is amoxicillin-clavulanate 875/125 mg orally twice daily for five to seven days (prophylaxis for three to five days is also cited for clean fresh bites; treat established infection for seven to ten days).[1][3]
In the penicillin-allergic or pregnant patient in whom doxycycline is unsuitable, seek microbiology advice. Practical oral alternatives covering Pasteurella and Eikenella include doxycycline 100 mg twice daily plus metronidazole 400 mg twice daily, or moxifloxacin 400 mg once daily. Cephalexin and flucloxacillin alone do not cover Pasteurella or Eikenella and must not be used as monotherapy for a bite.
Stingray and marine puncture injuries
Immediate first aid is hot-water immersion at 45 °C for 30 to 90 minutes — water hot but not scalding, tested against an unaffected limb; the patient is re-immersed if pain returns on removal. The limb is then removed, and every wound is explored for a retained barb fragment and the barb's integumentary sheath, which frequently separates and remains in the wound; ultrasound or X-ray confirms removal.[4][5] Irrigate, debride, and leave open. The stingray barb can carry seawater organisms — Vibrio species among them — so give prophylactic antibiotics for deep wounds, retained fragments, or immunocompromise (amoxicillin-clavulanate, or a fluoroquinolone with anaerobic cover if seawater exposure). Regional anaesthesia (a wrist or ankle block) is a useful adjunct for wound exploration and pain when hot water alone is insufficient. Address tetanus.
Insect stings — bee and wasp
A simple local reaction needs stinger removal (scrape sideways with a fingernail or the edge of a card; do not squeeze the venom sac with tweezers), cold pack, oral antihistamine (cetirizine 10 mg or promethazine), and simple analgesia. Large local reactions (swelling over 10 cm) additionally benefit from a short course of oral prednisolone.[1]
Systemic anaphylaxis is managed with adrenaline 0.5 mg (0.5 mL of 1:1000) intramuscularly to the anterolateral thigh, repeated every five minutes as needed, plus oxygen, intravenous fluid, and an H1 plus H2 antihistamine. Observe for six to twelve hours because biphasic reactions occur. Discharge the patient with an adrenaline autoinjector and a referral to an allergy specialist for venom immunotherapy, which is highly effective at preventing recurrence in those with confirmed Hymenoptera allergy.[16]
[16]Rabies post-exposure risk
Rabies is universally fatal once symptomatic, so post-exposure prophylaxis is guided entirely by the exposure risk. Consider rabies for any bat bite anywhere in the world (including ANZ, where Australian bat lyssavirus is endemic), and for any dog, cat, monkey or other mammal bite sustained overseas in a rabies-endemic country (most of Asia, Africa, and parts of the Americas).[6]
Wound management for a possible rabies exposure is vigorous washing and irrigation with soap and water or povidone-iodine for 15 minutes — this alone substantially reduces rabies transmission. Do not suture the wound if rabies is a possibility. Seek public-health or infectious-disease advice on the need for rabies vaccine (days 0, 3, 7, 14) and rabies immunoglobulin infiltrated into and around the wound (for previously unvaccinated patients with high-risk exposures). Australian bat lyssavirus is managed with the same protocol.[6]
Tetanus prophylaxis
Assess tetanus status on every bite and sting wound. Puncture wounds, contaminated wounds, and wounds more than six hours old are tetanus-prone. Give a tetanus toxoid booster (0.5 mL IM) if the patient has not had one within five years for a tetanus-prone wound, or within ten years for a clean wound. Give tetanus immunoglobulin 250 IU intramuscularly (500 IU for heavily contaminated or delayed-presentation wounds) to patients with fewer than three prior doses, an uncertain history, or HIV or other immunocompromise with a high-risk wound — in a separate limb and from a separate syringe.[17]
Snake envenomation
Although detailed snakebite management belongs to the dedicated snake-envenomation topic, the Fellowship candidate must hold a working schema because snakebites present to every Australasian ED. Snakes divide by venom action into two families that determine first aid, syndrome, and antivenom: elapids (the Australian and global front-fanged but short-fanged family — brown snakes, tiger, taipan, death adder, black, and the global cobras, mambas, kraits) are neurotoxic and coagulopathic, while vipers (the Old World and Asian family — Russell's viper, saw-scaled viper, puff adder) are haemotoxic and cytotoxic.[7]
The single most important Australasian rule: most locally important snakes are elapids, so apply a pressure immobilisation bandage (PIB) and keep the patient still — do not wash, cut, suck, tourniquet, or capture the snake. PIB retards lymphatic flow of venom to the circulation; it works for elapids whose venom travels lymphatically, and it is the reason movement is restricted. The bite site is left undisturbed so a venom-detection swab can be taken.[7]
Elapid (neurotoxic)
- Australian: brown, tiger, taipan, death adder, red-bellied black; global: cobra, mamba, krait
- Presynaptic and postsynaptic neurotoxins — ptosis, ophthalmoplegia, bulbar palsy, limb weakness, respiratory failure
- Coagulopathy: VICC (venom-induced consumption coagulopathy) with INR > 5, unrecordable fibrinogen, positive D-dimer; brown snake causes defibrination
- First aid: pressure immobilisation bandage + immobilise; do not remove
- Antivenom: monovalent if species known (e.g. brown snake), polyvalent if unknown or multiple species possible
Viper (haemotoxic)
- Russell's viper, saw-scaled viper, puff adder — acquired overseas
- Procoagulant venoms cause consumption coagulopathy and bleeding; cytotoxins cause local blistering, necrosis, compartment syndrome
- AKI is common (Russell's viper), and saw-scaled viper causes life-threatening haemorrhage
- First aid: pressure immobilisation is reasonable but evidence weaker; avoid incisions and tourniquets
- Antivenom: species-specific antivenom where available; supportive care — fluids, transfusion, renal support
Sea snake (hydrophid)
- Myotoxic and neurotoxic — rhabdomyolysis with myoglobinuria and rising CK, plus flaccid paralysis
- Marine exposure is the clue; bites may be painless
- First aid: pressure immobilisation bandage
- Antivenom: sea snake antivenom ( CSL ); polyvalent may help
- Watch for hyperkalaemia and renal failure from rhabdomyolysis
Diagnosis and the venom-induced consumption coagulopathy
A snakebite is not confirmed until there is laboratory or clinical evidence of envenomation — many bites are dry. The minimum panel on arrival (after PIB removal is NOT performed) is a full blood count, coagulation profile (INR, APTT, fibrinogen, D-dimer), urea and electrolytes, creatine kinase, and a urinalysis for blood/myoglobin, repeated at one and two hours if normal. VICC — INR off-scale, fibrinogen unrecordable, D-dimer markedly elevated — is the hallmark of brown, tiger and taipan envenomation and resolves over days to weeks as the liver resynthesises clotting factors (do not expect immediate correction after antivenom). Neurotoxic signs (ptosis is the earliest and most easily missed) and myotoxicity (rising CK, muscle pain, dark urine) round out the syndromes.[14]
[14]Antivenom
Antivenom is given for clinical or laboratory envenomation, not for every bite. Use a monovalent antivenom when the species is known or confidently identified by venom-detection swab; use polyvalent snake antivenom (a mixture covering brown, tiger, taipan, death adder, and black snakes) when the snake is unidentified or the syndrome unclear — polyvalent is the pragmatic choice in the undifferentiated Australasian case. Dose and premedication are unit/manufacturer specific; give via intravenous infusion in a monitored area with adrenaline drawn up because antivenom is heterologous equine protein and anaphylaxis and serum sickness can follow. A venom-detection swab from the bite site (taken over the bandage) guides monovalent choice.[7]
ED management of suspected snakebite
Call for help and notify the toxicology / national poisons centre. Keep the patient still and supine.
Leave the pressure immobilisation bandage IN PLACE until assessed and antivenom is ready; do not remove it to "look". Movement releases venom.
Take a venom-detection swab from the bite site through/over the bandage; do not wash the bite.
Draw bloods: FBC, coagulation (INR, APTT, fibrinogen, D-dimer), U&E, CK, LFT, group and hold, urinalysis.
Assess for neurotoxicity (ptosis, ophthalmoplegia, bulbar signs, respiratory effort) and bleeding.
If envenomed: give monovalent antivenom (species known) or polyvalent antivenom (unknown) IV with monitoring; have adrenaline ready.
Repeat coagulation and CK at 1, 2, 6, 12 hours; titrate further antivenom to clinical and laboratory response.
Observe the asymptomatic patient with normal bloods for at least 12 hours before declaring a dry bite.
Address tetanus. Counsel about serum sickness at 5–14 days.
Red-bellied black snake antivenom (RBB-001)
Multicentre randomised controlled trial with prospective observational cohort
Key finding
In this randomised controlled trial and prospective cohort of red-bellied black snake envenomation, antivenom did not hasten recovery of the characteristic myotoxic and anticoagulant effects; most patients recovered with supportive care alone. The study supports selective, rather than routine, antivenom use for this species, and underscores that minor elapid envenomations may be managed conservatively under observation.
Spider envenomation
Australasia is home to two medically significant spiders with dedicated antivenoms: the redback (Latrodectus hasselti) — a widow spider carrying the neurotoxic α-latrotoxin — and the Sydney funnel-web (Atrax and Hadronyche species) — carrying δ-hexatoxins (atraxotoxin). The two are clinical opposites in every respect: redback envenomation is painful but rarely life-threatening; funnel-web envenomation is the only spider bite that regularly kills.[8][12]
Redback spider bite causes immediate local pain, then over 30–60 minutes a tightening, burning pain that radiates up the limb, with sweating, piloerection, regional lymphadenopathy, and (in severe cases) hypertension, headache, nausea, and priapism. The syndrome is latrodectism: the toxin opens presynaptic calcium channels causing massive neurotransmitter release. First aid is cold compress and analgesia — not a pressure immobilisation bandage, which worsens pain. Most cases resolve with simple analgesia and observation; redback spider antivenom (CSL, equine F(ab')2) is reserved for pain unresponsive to opioids, and is given by the intravenous route in current Australasian practice (the RAVE trial found intramuscular antivenom no better than placebo and is no longer recommended).[13]
Funnel-web spider bite is a true emergency. The venom is a neurotoxin causing autonomic storm and neuromuscular excitation — paraesthesia around the mouth, lacrimation, salivation, sweating, pilomotor erection, muscle fasciculation, hypertension, tachyarrhythmia, then (in severe cases) pulmonary oedema, convulsions, and respiratory failure. First aid is a pressure immobilisation bandage, exactly as for elapid snakebite, because the venom is lymphatically transported. Funnel-web spider antivenom (CSL) is dramatically effective and should be given at the first sign of systemic envenomation.[8]
Redback (Latrodectus)
- α-latrotoxin — presynaptic Ca²⁺ channel activation, massive transmitter release
- Latrodectism: severe local + radiating pain, sweating, piloerection, hypertension; rarely life-threatening
- First aid: cold pack and oral analgesia — NOT a pressure immobilisation bandage
- Antivenom: redback spider antivenom IV for opioid-resistant pain (IM route abandoned after RAVE)
- No deaths in Australia since antivenom introduction in 1956
Funnel-web (Atrax/Hadronyche)
- δ-hexatoxins (atraxotoxin) — neuroexcitation, autonomic storm
- Perioral tingling, lacrimation, salivation, fasciculation, pulmonary oedema, respiratory failure — can kill within hours
- First aid: pressure immobilisation bandage + immobilise (elapid-style)
- Antivenom: funnel-web spider antivenom IV at first sign of systemic envenomation — highly effective
- Most dangerous spider globally; only paediatric deaths now if presentation delayed
Other spiders
- White-tail and huntsman: local pain only, no necrotic arachnidism syndrome supported by evidence
- Mouse spider (Missulena): can cause a funnel-web-like syndrome — give funnel-web antivenom
- Antibiotics and debridement are not indicated for "necrotic arachnidism" lesions — reconsider the diagnosis (usually pyoderma or HSV)
ED approach to the funnel-web bite
Apply or check the pressure immobilisation bandage and immobilise the patient — keep still and supine.
Establish IV access, cardiac monitoring, and draw bloods including FBC, coagulation, U&E, CK.
Assess for systemic signs: perioral tingling, lacrimation, salivation, piloerection, fasciculation, hypertension, respiratory distress.
At ANY systemic sign, give funnel-web spider antivenom IV (typically 2 ampoules, repeated as needed) — have adrenaline ready.
Support the airway and breathing — respiratory failure and pulmonary oedema are the killers; prepare for intubation early.
Once symptom-free and stable after observation, remove the bandage and observe for recurrence before discharge.
Tetanus prophylaxis; counsel on serum sickness risk.
RAVE — Redback Antivenom, IV vs IM
Observational pharmacokinetic study informing randomised trial practice
Key finding
The case series and subsequent trial evidence found that intramuscular redback antivenom failed to achieve therapeutic levels and was no better than placebo, while the intravenous route relieved pain. As a result, the intramuscular route — once standard — has been abandoned in Australasia in favour of IV redback antivenom for the small minority of patients who require it at all. Most latrodectism is managed with analgesia, benzodiazepines, and observation.
Box jellyfish, blue-ringed octopus, and stonefish
Beyond stingray, three further marine envenomations are exam favourites because each has a specific intervention the candidate must name.[4]
Box jellyfish (Chironex fleckeri) — the most venomous marine animal — produces excruciating skin pain with characteristic cross-hatched, beaded, whip-like red welts, and can cause rapid cardiovascular collapse and death within minutes, especially in children. First aid is liberal dousing with household vinegar (acetic acid) to inactivate unfired nematocysts — never use fresh water, alcohol, or pressure immobilisation, all of which cause further firing (pressure bandaging, beneficial for elapid snakebite, is explicitly contraindicated for jellyfish stings).[10] Box jellyfish antivenom (CSL, ovine) is given intravenously for systemic envenomation (cardiac arrest, arrhythmia, hypotension, respiratory distress) alongside cardiopulmonary resuscitation and magnesium in refractory cases.[9][11]
Blue-ringed octopus (Hapalochlaena) saliva contains tetrodotoxin, a potent sodium-channel blocker that produces rapid-onset flaccid paralysis with preserved consciousness — patients may be "locked in" while fully awake. There is no antivenom; management is entirely supportive — prolonged mechanical ventilation until the toxin clears (typically 4–12 hours), with full recovery expected in survivors. The bite itself is often painless and unnoticed.[9]
Stonefish (Synanceia) spine puncture causes immediate, excruciating, radiating pain and local tissue necrosis. Like stingray, the venom is heat-labile — immerse in hot water at 45 °C for 30–90 minutes. Stonefish antivenom (CSL, equine) is given intramuscularly for severe pain unresponsive to hot water, multiple punctures, or systemic features. Address tetanus.[11]
Box jellyfish (Chironex fleckeri)
- Excruciating pain + cross-hatched beaded red welts; rapid cardiovascular collapse, especially in children
- First aid: vinegar (acetic acid) to inactivate nematocysts — NOT fresh water, alcohol, or pressure bandaging
- Antivenom: box jellyfish antivenom IV for systemic envenomation + CPR, magnesium for refractory arrhythmia
- Irukandji (Carukia barnesi): delayed (20–40 min) catecholamine surge — severe back/abdominal pain, hypertension, pulmonary oedema; analgesia, magnesium, antihypertensives, no antivenom routinely
Blue-ringed octopus
- Tetrodotoxin — sodium-channel blockade; rapid flaccid paralysis with preserved consciousness ("locked in")
- Bite often painless; death from respiratory failure
- NO antivenom — management is prolonged mechanical ventilation until toxin clears (4–12 h)
- Apply pressure immobilisation bandage to retard venom spread; full recovery expected with ventilatory support
Stonefish (Synanceia)
- Spine puncture — immediate severe radiating pain, local necrosis; venom heat-labile
- First aid: hot-water immersion at 45 °C for 30–90 minutes (test temperature on unaffected limb)
- Antivenom: stonefish antivenom IM for severe pain, multiple punctures, or systemic features
- Address tetanus; explore for retained spine fragments (radiopaque)
Complications and pitfalls
The recurring errors are: using flucloxacillin or cephalexin alone, which misses Pasteurella and Eikenella; closing a hand bite primarily, which seals in deep contamination; missing a retained tooth or barb fragment by failing to X-ray or explore; underestimating a clenched-fist injury as a trivial scratch when the joint is penetrated; forgetting tetanus and rabies on a contaminated or overseas wound; and discharging a patient with an insect-sting anaphylaxis without an adrenaline autoinjector and an allergy referral.[2][3][6]
Disposition and special populations
Most mammalian bites are managed with oral antibiotics and review at 48 hours. Admit or refer to hand surgery for clenched-fist injuries with joint or tendon involvement, established septic arthritis or tenosynovitis, deep space infection, retained foreign body, systemic sepsis, or failure to improve on oral therapy. The immunocompromised, asplenic, and diabetic patient is admitted at a lower threshold — watch particularly for Capnocytophaga canimorsus sepsis in the asplenic dog-bite patient, which can be fulminant. Pregnancy and breastfeeding are not contraindications to amoxicillin-clavulanate. Children with face bites are often admitted or transferred for plastic surgical repair.[3]
Exam pearls
- Amoxicillin-clavulanate is the single answer to "best antibiotic for a bite" — it covers every relevant organism in one drug.
- Pasteurella = cat/dog; Eikenella = human; Capnocytophaga = dog in the asplenic.
- Stingray: hot water 45 °C for 30 to 90 minutes, then explore for a retained barb.
- Fight-bite over the MCP joint = orthopaedic emergency, washout, never close.
- Rabies: any bat bite (including ANZ — Australian bat lyssavirus) and any overseas dog bite = seek public-health advice for vaccine and immunoglobulin.
- Tetanus on every bite; the bite is a tetanus-prone wound.
- Snakebite: elapid = neurotoxic + coagulopathic (Australia); viper = haemotoxic + cytotoxic (overseas). Pressure immobilisation bandage for elapids; polyvalent antivenom when species unknown.
- Do NOT remove the pressure immobilisation bandage to look at a snakebite — removal triggers systemic envenomation; assess, swab, and remove only when antivenom is ready.
- Ptosis is the earliest sign of neurotoxic snake envenomation — test sustained upgaze; INR > 5 with unrecordable fibrinogen = venom-induced consumption coagulopathy (recovers over 1–3 weeks; do not chase with FFP).
- Funnel-web spider = pressure immobilisation bandage + funnel-web antivenom IV (kills; autonomic storm); redback spider = cold pack ± IV antivenom (painful, rarely lethal; never use a pressure bandage).
- Latrodectism triad: severe local pain, sweating, piloerection (± priapism) — redback/widow spider.
- Box jellyfish: vinegar to inactivate nematocysts, then box jellyfish antivenom IV — never fresh water or a pressure bandage. Stonefish: hot water 45 °C then stonefish antivenom IM. Blue-ringed octopus: tetrodotoxin, no antivenom — prolonged ventilation.
- Vinegar for box jellyfish; hot water for stingray and stonefish — the two marine first-aids are opposites; mixing them up is a classic exam trap.[10]
Exam practice
SAQ — Suspected brown snake bite with venom-induced consumption coagulopathy
10 minutes · 10 marks
A 42-year-old wheat-belt farmer is brought to your rural emergency department 90 minutes after being bitten on the lateral ankle by a snake he describes as a brown snake about five feet long. Paramedics applied a pressure immobilisation bandage at the scene and the patient has remained still and supine. On arrival the bandage is intact, he is alert and pain-free (GCS 15), BP 132/78, HR 88, RR 16, SpO2 98 per cent on room air. There are two small puncture marks on the ankle with no local reaction. He has no bleeding and no ptosis and feels well. Bloods taken on arrival: INR off-scale (greater than 10), APTT greater than 150 seconds, fibrinogen less than 0.3 g/L, D-dimer greater than 20 mg/L; haemoglobin 152 g/L; platelets 220 x 10^9/L; CK 320 U/L; urinalysis negative for blood. The nearest toxicology service is reachable by telephone.
SAQ — Bee-sting anaphylaxis in the beekeeper
10 minutes · 10 marks
A 47-year-old commercial beekeeper with a known allergy to bee venom is brought to your emergency department by ambulance five minutes after a sting to the neck. He used his adrenaline autoinjector at the scene within two minutes. On arrival he is flushed, anxious and dyspnoeic: BP 78/44, HR 124, RR 28 with a loud expiratory wheeze and audible stridor, SpO2 90 per cent on 15 L oxygen via a non-rebreather mask. He has widespread urticaria over the trunk and face, marked tongue and lip angioedema, and is drooling. He is alert but beginning to tire. Intravenous access has been established by the paramedics.
Red flags
[4]References
- [1]Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 2014.PMID 24973422
- [2]Talan DA, Abrahamian FM, Moran GJ, Citron DM, Tan JO, Goldstein EJ. Clinical presentation and bacteriologic analysis of infected human bites in patients presenting to emergency departments. Clinical Infectious Diseases, 2003.PMID 14614671
- [3]Griego RD, Rosen T, Orengo IF, Wolf JE. Dog, cat, and human bites: a review. Journal of the American Academy of Dermatology, 1995.PMID 7490347
- [4]Clark RF, Girard RH, Rao D, Ly BT, Davis DP. Stingray envenomation: a retrospective review of clinical presentation and treatment in 119 cases. The Journal of Emergency Medicine, 2007.PMID 17630073
- [5]Niżnik Ł, Kiczorowska-Szarlej B, Chowaniec C, et al. Hot-water immersion (HWI) or ice-pack treatment (IPT) as first aid for human envenomations — a scoping review. Toxins, 2024.PMID 38922167
- [6]Manning SE, Rupprecht CE, Fishbein DB, et al. Human rabies prevention — United States, 2008: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recommendations and Reports, 2008.PMID 18496505
- [7]Warrell DA. Snake bite. Lancet, 2010.PMID 20109866
- [8]Isbister GK, Fan HW. Spider bite. Lancet, 2011.PMID 21762981
- [9]Currie BJ, Jacups SP. Prospective study of Chironex fleckeri and other box jellyfish stings in the 'Top End' of Australia's Northern Territory. Medical Journal of Australia, 2005.PMID 16336157
- [10]Fenner PJ, Williamson JA, Burnett JW. Pressure immobilisation bandages in first-aid treatment of jellyfish envenomation: current recommendations reconsidered. Medical Journal of Australia, 2001.PMID 11480696
- [11]Currie BJ. Marine antivenoms. Journal of Toxicology Clinical Toxicology, 2003.PMID 12807313
- [12]Isbister GK, Graudins A, White J, Currie BJ. Antivenom treatment in arachnidism. Journal of Toxicology Clinical Toxicology, 2003.PMID 12807312
- [13]Isbister GK. Failure of intramuscular antivenom in red-back spider envenoming. Emergency Medicine (Fremantle), 2002.PMID 12534488
- [14]Isbister GK, Jenkins S, Downes MA, et al. A randomised controlled trial and prospective cohort investigating antivenom for red-bellied black snake envenomation. Clinical Toxicology (Philadelphia), 2024.PMID 38913734
- [15]Cardona V, Ansotegui IJ, Ebisawa M, et al. World allergy organization anaphylaxis guidance 2020. World Allergy Organization Journal, 2020.PMID 33204386
- [16]Ruëff F, Bauer A, Becker S, et al. Diagnosis and treatment of Hymenoptera venom allergy: S2k Guideline of the German Society of Allergology and Clinical Immunology (DGAKI) in collaboration with the Arbeitsgemeinschaft für Berufs- und Umweltdermatologie e.V. (ABD), the Medical Association of German Allergologists (AeDA), the German Society of Dermatology (DDG), the German Society of Oto-Rhino-Laryngology, Head and Neck Surgery (DGHNOKC), the German Society of Pediatrics and Adolescent Medicine (DGKJ), the Society for Pediatric Allergy and Environmental Medicine (GPA), German Respiratory Society (DGP), and the Austrian Society for Allergy and Immunology (ÖGAI). Allergologie Select, 2023.PMID 37854067
- [17]Cooke MW. Are current UK tetanus prophylaxis procedures for wound management optimal? Emergency Medicine Journal, 2009.PMID 19934122