EM · Cardiogenic shock
Cardiogenic shock in the emergency department
Also known as Cardiac shock · Post-MI shock · Pump failure shock
Cardiogenic shock — the spiral of low cardiac output, compensatory vasoconstriction, rising afterload and deepening hypoperfusion; the SCAI shock stages (A to E); the cause-first management (immediate revascularisation for the infarct, surgery for the mechanical complication), the pharmacologic support (noradrenaline preferred over dopamine per SOAP-2; dobutamine or milrinone as inotrope), the mechanical-circulatory-support evidence (IABP no mortality benefit per IABP-SHOCK II; Impella and VA-ECMO as a bridge), and the culprit-only PCI principle of CULPRIT-SHOCK. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Cardiogenic shock is the state in which a primary cardiac pump failure produces inadequate tissue perfusion despite an adequate or excessive preload, and it is the spiral that kills — a falling output, a rising compensatory afterload, a deepening hypoperfusion, and a worsening ischaemia that feeds back into further failure. The Fellowship candidate must recognise the cold, poorly perfused, acidotic patient, treat the cause first — especially revascularising the infarct — support the circulation with the right agent, and know when to call for mechanical circulatory support.[1][3]
Definition and the SCAI shock stages
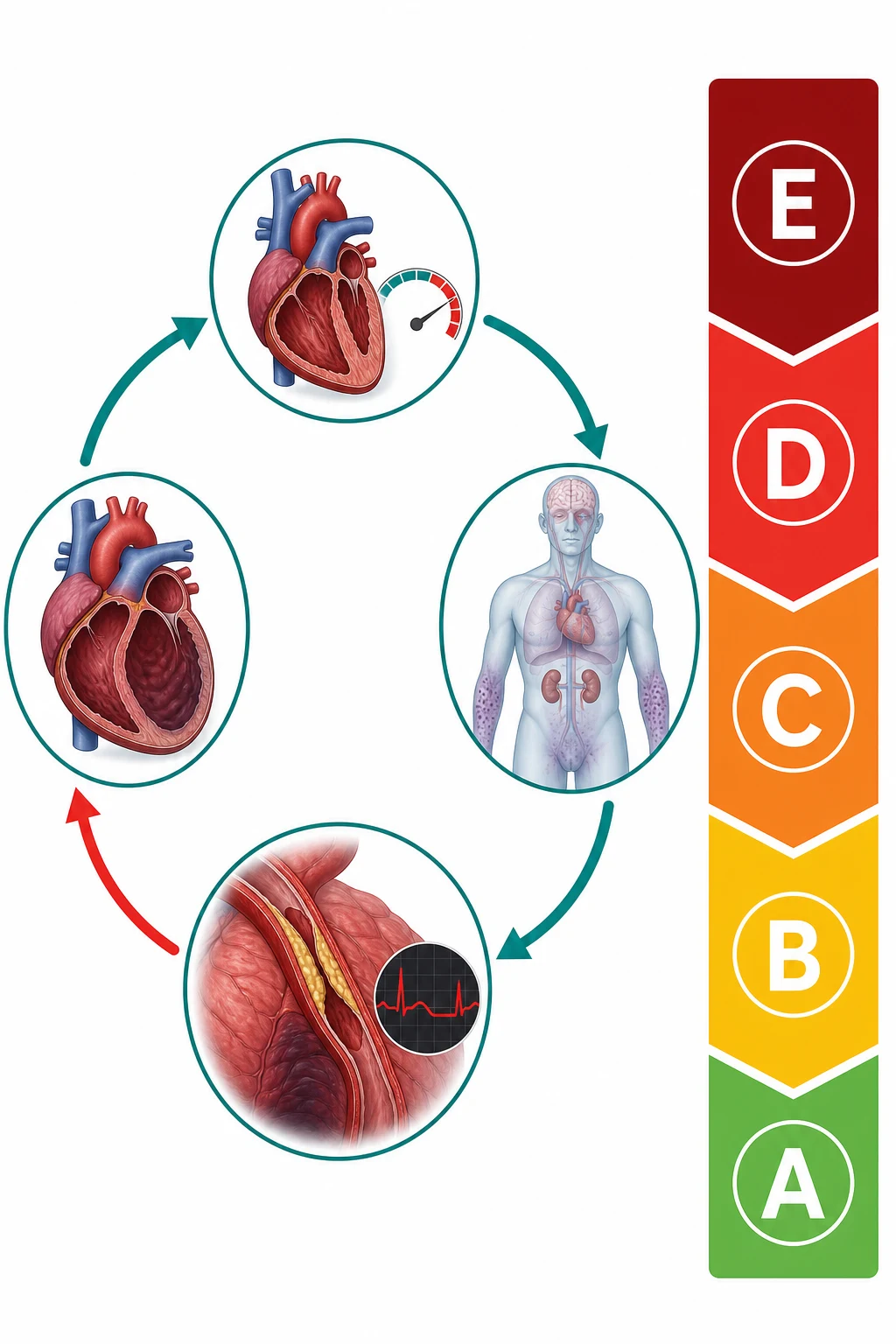
Cardiogenic shock is a state of tissue hypoperfusion from a primary cardiac pump dysfunction, with the clinical signs of hypotension, a cold periphery, a raised lactate and a low urine output, usually with pulmonary congestion (the wet–cold phenotype). The Society for Cardiovascular Angiography and Interventions (SCAI) stages grade it from A (at risk — a patient with a predisposing condition but no signs) through B (beginning — clinical and biochemical evidence, normotensive) and C (classic — hypoperfusion needing a pressor or an inotrope) to D (deteriorating — escalating support) and E (extremis — circulatory collapse or cardiac arrest). The stage guides the intensity of monitoring and the escalation.[9]
The SCAI consensus, endorsed by the American College of Cardiology, the American Heart Association, the Society of Critical Care Medicine and the Society of Thoracic Surgeons, was created because the older binary "shock / no shock" definition hid a continuum — patients who would imminently crash were labelled "not in shock" and under-monitored, while the staging makes the trajectory explicit.[9]
Applying the SCAI stages at the bedside
Stage A — At risk
A patient with a predisposing insult (a large infarct, a myocarditis, a decompensating cardiomyopathy) but no signs of hypoperfusion. Normotensive, normal lactate, warm, making urine. Action: high-acuity monitoring, serial lactate, early echo; anticipate deterioration.
Stage B — Beginning shock
Clinical or biochemical evidence of hypoperfusion beginning — a rising lactate, a cool periphery, a falling urine output, a creeping creatinine — but still normotensive (systolic over 90 and not on a pressor). Action: admit to a monitored bed, start the inotrope if the output is low, treat the cause.
Stage C — Classic shock
Hypoperfusion now with hypotension — systolic under 90, mean arterial pressure under 65, or needing a pressor or an inotrope to hold it. The cold, wet, oliguric, acidotic patient. Action: full resuscitation — revascularise the infarct, vasopressor + inotrope, call the cardiology and the MCS teams early.
Stage D — Deteriorating
Worsening perfusion despite escalating single-agent support — needing multiple pressors/inotropes, or a rising lactate on therapy, or worsening end-organ failure. Action: escalate to mechanical circulatory support (Impella, VA-ECMO) as a bridge; the window is closing.
Stage E — Extremis
Circulatory collapse — PEA or asystolic arrest, or refractory hypotension with no obtainable pressure. Action: CPR, emergency VA-ECMO (ECPR) where available, and a rapid decision on futility.
Stage A — At risk
- Predisposing condition, no hypoperfusion
- Normotensive, warm, normal lactate
- No pressor/inotrope
- Monitor, anticipate
Stage B — Beginning
- Biochemical/clinical hypoperfusion starting
- Still normotensive (SBP ≥ 90)
- Cool periphery, rising lactate
- Treat cause, inotrope if low output
Stage C — Classic
- Hypoperfusion + hypotension
- SBP < 90, MAP < 65, or on pressor
- Cold, wet, oliguric, acidotic
- Full resuscitation, early revascularisation
Stage D — Deteriorating
- Worsening despite escalating support
- Multiple agents or rising lactate on therapy
- Multi-organ failure entrenched
- Escalate to MCS (Impella/VA-ECMO)
Stage E — Extremis
- Circulatory collapse / arrest
- PEA, asystole, no obtainable BP
- Mortality > 80 per cent
- CPR, emergency ECPR, decide on futility
The spiral — why early intervention is everything
The cardiac output falls, and the body compensates with a sympathetic and a renin–angiotensin-driven vasoconstriction and tachycardia to hold the blood pressure. The raised systemic vascular resistance, however, increases the afterload on a failing ventricle, which lowers the stroke volume further and deepens the hypoperfusion; the ischaemia worsens the myocardial function and the cycle tightens. The lactate rises, the kidneys fail, the liver fails, the gut becomes ischaemic, and the systemic inflammatory response of shock itself perpetuates the vasodilation and the failure. Early intervention — the reperfusion of the infarct, the unloading of the ventricle, the right inotrope and the right pressor — breaks the spiral; delay entrenches an irreversible multi-organ failure.[1]
The spiral also explains why the timing of the intervention matters more than the agent chosen: a patient in SCAI stage B or C (early, compensated) responds to the inotrope and the pressor and the revascularisation; a patient in stage D or E (decompensated, with the multi-organ failure entrenched) may not respond to anything short of a full mechanical unloading and an extracorporeal support, and even then the mortality is high. The window is narrow, and the Fellowship candidate must act within it.[9]
The SCAI staging system itself was designed to standardise this assessment across the emergency, the critical-care and the cardiology teams, so that a patient is not lost between the thresholds of each service's individual definition of shock.[9]
The vicious cycle made explicit
The pathophysiology is a feedback loop, and naming each link is how the Fellowship candidate reasons about each drug and each device.[1]
The cardiogenic-shock vicious cycle — link by link
1 — The pump fails
A large infarct (≈ 40 per cent of the LV myocardium lost), a fulminant myocarditis, or a mechanical catastrophe drops the stroke volume. Cardiac output = stroke volume × heart rate, so the output falls.
2 — The blood pressure falls
Mean arterial pressure = cardiac output × systemic vascular resistance. With the output down, the pressure falls — the coronary perfusion pressure (diastolic BP − LVEDP) falls with it.
3 — The compensatory vasoconstriction
Sympathetic discharge and the renin–angiotensin–aldosterone axis constrict the arterioles and raise the SVR to defend the pressure. The periphery goes cold and the venous return is recruited.
4 — Afterload worsens the failing pump
The same vasoconstriction that defends the pressure raises the afterload on a ventricle that cannot eject — the stroke volume falls further. This is the trap: the compensation is maladaptive.
5 — Coronary hypoperfusion deepens the ischaemia
The falling diastolic pressure and the rising end-diastolic pressure squeeze the coronary perfusion gradient; the ischaemia extends beyond the original infarct, stunning more myocardium and feeding back to step 1.
6 — End-organ failure and the inflammatory spiral
The lactate rises, the kidneys fail, the liver fails, the gut becomes ischaemic, and a systemic inflammatory response (cytokine-driven vasoplegia) supervenes — the shock becomes self-sustaining even if the original cause is treated.
Causes
The commonest cause is the acute myocardial infarction — a large infarct, or a mechanical complication that appears three to five days afterwards: a ventricular-septal rupture (a new pansystolic murmur at the lower left sternal edge), a papillary-muscle rupture (an acute mitral regurgitation), or a free-wall rupture (a tamponade). The other causes are a decompensated chronic heart failure or a cardiomyopathy, a fulminant myocarditis, an acute valvular catastrophe (a severe mitral or aortic regurgitation or a critical aortic stenosis), a sustained arrhythmia, a peripartum cardiomyopathy, and a drug toxicity (a beta-blocker or a calcium-channel-blocker overdose). A right-ventricular infarct produces a right-heart shock with a raised venous pressure and clear lungs.[1]
The aetiologies and their distinguishing features
The acute MI accounts for the overwhelming majority — around 80 per cent of the cardiogenic shock — either from the sheer loss of the muscle or from a mechanical complication that declares itself days later. The non-MI causes are fewer but distinctive, and each carries a different definitive therapy.[1]
Acute MI (≈ 80%)
- Large infarct (> 40% LV) or mechanical complication
- ST changes on ECG; troponin raised
- Revascularise the culprit artery (SHOCK, CULPRIT-SHOCK)
- Watch for VSD/papillary rupture at 3–5 days
Mechanical complications of MI
- VSD — new loud pansystolic murmur, LLS edge, 3–5 days
- Papillary-muscle rupture — acute severe MR, pulmonary oedema
- Free-wall rupture — tamponade, electromechanical dissociation
- Surgery + MCS; thrombolysis contraindicated
Fulminant myocarditis
- Young patient, viral prodrome, global ST/T changes
- Echo: global hypokinesis, normal coronaries
- VA-ECMO bridge — many recover fully
- Endomyocardial biopsy if giant-cell suspected
Decompensated cardiomyopathy
- Chronic HFrEF with an acute precipitant
- Echo: dilated LV, low EF, known history
- Treat precipitant; guideline therapy; MCS as bridge
- Consider transplant/LVAD workup
Arrhythmia-driven
- Sustained VT, fast AF, complete heart block
- Rate-related cardiomyopathy or acute decompensation
- Cardiovert/pace; treat the rhythm
- Often reversible once rhythm controlled
Acute valvular catastrophe
- Critical aortic stenosis, acute severe MR/AR
- Endocarditis, chordal/papillary rupture
- Echo diagnostic; urgent surgery
- Avoid vasodilators in critical AS
Right ventricular infarct
- Inferior MI, raised JVP, clear lungs
- Echo: RV dysfunction; ST elevation in V4R
- Volume loading, inotrope, reperfusion
- Nitrate/narcotic cautious — preload-dependent
Drug toxicity
- Beta-blocker, CCB overdose; bupivacaine
- Bradycardia, hypotension, hyperglycaemia (CCB)
- High-dose insulin/euglycaemia, lipid emulsion
- Decontaminate; pacing; MCS for refractory
Peripartum cardiomyopathy
- Last month of pregnancy to 5 months postpartum
- Echo: LV systolic dysfunction
- Lactation-safe heart-failure therapy; bromocriptine
- MCS/transplant for refractory
Clinical presentation
The patient is cold, clammy and shut down: a systolic blood pressure under 90 (or over 30 below the baseline), a thready pulse, a slow capillary refill over two seconds, a mottled skin, an oliguria (under 0.5 mL per kilogram per hour), and an altered mental status. The lactate is raised and often rising. When the left ventricle is the failing pump the lungs are wet (a pulmonary oedema with crackles), which distinguishes the cardiogenic shock from the dry shock of hypovolaemia or obstruction. A new murmur after an infarct points to a mechanical complication. An early "warm" vasodilatory phase may precede the cold shutdown, but it evolves within hours.[7]
Recognising shock at the bedside — the cold, wet, oliguric patient
The recognition is clinical before it is biochemical. The patient is cold and clammy with a thready pulse, the peripheries are shut down (a capillary refill over two seconds, a mottled or marbled skin), and the brain and the kidneys slow (a confusion or an agitation, an oliguria under 0.5 mL per kilogram per hour). The jugular venous pressure is raised when the right heart is failing, and a third heart sound (S3) is the auscultatory signature of the failing, volume-overloaded ventricle. The lungs are wet with pulmonary oedema when the left ventricle is the failing pump (the cold-and-wet phenotype), which is the cardinal distinction from the cold-and-dry shock of hypovolaemia or the warm-and-dry shock of early sepsis. The lactate is raised and rising, and the trend matters more than the single value.[1]
Cold & wet (cardiogenic LV failure)
- Cold periphery + pulmonary oedema
- Raised JVP, S3 gallop
- Echo: poor LV, high LVEDP
- Noradrenaline + inotrope + cause; cautious fluid
Cold & dry (hypovolaemic / obstructive)
- Cold periphery, clear lungs
- Flat JVP (hypovolaemic) or raised JVP (obstructive)
- Responds to fluid (hypovolaemic) or treated as PE/tamponade
- Small IVC on echo
Warm & wet (septic / late cardiogenic)
- Warm periphery, vasoplegia
- Pulmonary oedema from capillary leak
- Echo: often hyperdynamic early
- Fluids, antibiotics, noradrenaline
RV-failure (right-heart shock)
- Raised JVP, clear lungs, hypotension
- RV infarct, massive PE, ARDS
- Preload-dependent — volume loading
- Reperfuse; inotrope; avoid vasodilators
Differential diagnosis
The shocked patient has a differential, and the bedside echocardiogram, the fluid response and the history resolve it.[1]
Cardiogenic shock
- Cold periphery, raised lactate; pulmonary oedema if LV
- Bedside echo: reduced LV/RV function, ± mechanical
- Troponin raised (MI); ECG: ischaemia/arrhythmia
- Treat the cause + noradrenaline + inotrope + MCS
Septic / distributive
- Warm early, high-output; source of infection
- Echo: usually hyperdynamic LV
- Responds to fluids initially; raised WCC/lactate
- Fluids, antibiotics, source control, noradrenaline
Hypovolaemic
- History of bleeding/dehydration; flat JVP
- Responds to fluid; echo: small IVC, hyperdynamic
- No pulmonary oedema
- Fluids ± transfusion
Obstructive (PE, tamponade, PTX)
- Raised JVP, clear lungs (unless tamponade with effusion)
- Echo: RV strain (PE), effusion (tamponade)
- Distinct pathways: thrombolysis, drainage, decompression
- Not a pressor/inotrope disease alone
Investigations and the SCAI targets
The lactate is the key perfusion marker — a raised and rising lactate signals worsening shock and a poor prognosis; the trend matters more than the single value. The arterial blood gas shows the metabolic or the lactic acidosis and the hypoxia. The bedside echocardiogram shows the reduced left or right ventricular function, a mechanical complication (a septal rupture, a papillary-muscle rupture), a valve lesion, or a pericardial effusion, and it distinguishes cardiogenic from the other shock types. The ECG identifies the ischaemia or the arrhythmia, the troponin the infarct, and a cardiac output monitor (where available) confirms the low output and the high systemic vascular resistance. The SCAI stage, the blood-pressure, the lactate and the urine-output criteria are reproduced.[9]
Immediate management — cause first, then support
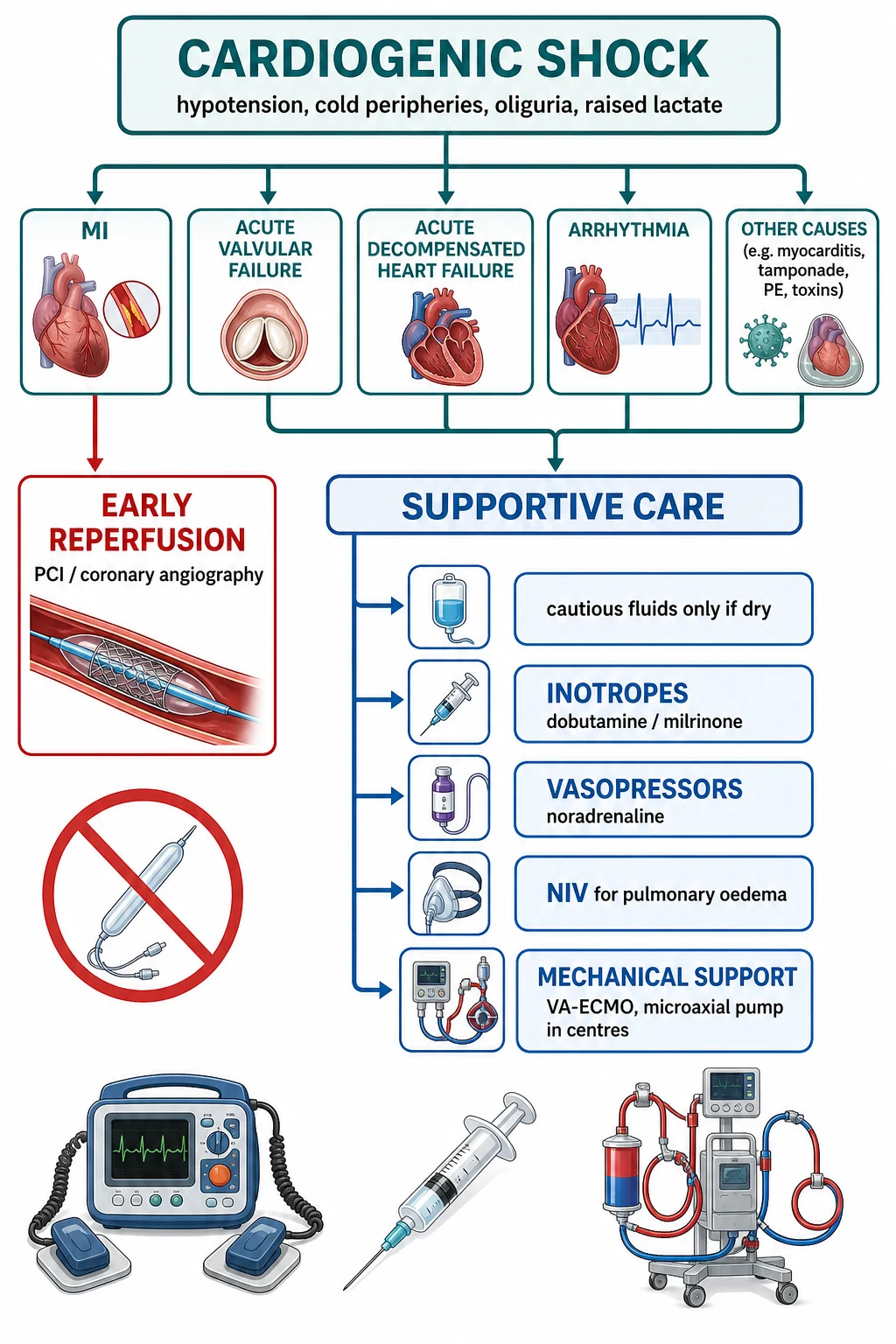
Stabilise the airway and the breathing with oxygen, with non-invasive or invasive ventilation if the patient is tiring; give a cautious fluid challenge (a small aliquot of 250 mL — not a large bolus, which worsens the pulmonary oedema) only if the patient is dry; and start the pharmacologic support while you treat the cause.[4]
The first 60 minutes — the cardiogenic-shock resuscitation in the ED
0 min — Recognise and call for help
Identify the cold, wet, oliguric, acidotic patient; stage by SCAI (B and above needs monitored care, C and above needs the resuscitation team). Alert cardiology and the cath-lab early — the time-to-revascularisation is the single biggest determinant of survival.
0 to 5 min — Airway, oxygen, monitoring
High-flow oxygen to hold the SpO₂ at 94 per cent; two large-bore cannulae; full monitoring (ECG, SpO₂, arterial line when safe); blood for lactate, troponin, blood gas, FBC, coagulation, group and hold, electrolytes, BNP. Apply non-invasive ventilation early for the pulmonary oedema (CPAP/BiPAP reduces the work of breathing and the afterload).
5 to 10 min — The bedside echo and the ECG
Echo: LV/RV function, a mechanical complication, a valve lesion, a tamponade, a dilated IVC. ECG: ischaemia, arrhythmia, right-sided leads (V4R) for the RV infarct. This is the investigation that distinguishes cardiogenic from the other shocks and finds the cause.
5 to 15 min — Cautious fluid if dry
A 250 mL aliquot of balanced crystalloid, reassessed — only if the patient is dry (clear lungs, small IVC). A large bolus into the failing, wet LV worsens the pulmonary oedema and the mitral regurgitation. The RV-infarct patient is preload-dependent and may need more.
5 to 15 min — Vasopressor and inotrope
Noradrenaline 0.05–0.5 mcg/kg/min titrated to a mean arterial pressure of 65 mmHg; add an inotrope (dobutamine 2.5–20 mcg/kg/min or milrinone 0.125–0.75 mcg/kg/min) for the low-output state. Adrenaline (0.05–1 mcg/kg/min) is the single agent when both pressor and inotrope are needed, but watch the lactate and the arrhythmia.
10 to 60 min — Treat the cause
MI-shock: activate the cath-lab for the culprit-only PCI (CULPRIT-SHOCK). Mechanical complication: surgery + MCS. Arrhythmia: cardiovert or pace. Drug toxicity: high-dose insulin/euglycaemia for the CCB/beta-blocker overdose. Fulminant myocarditis: VA-ECMO bridge.
Early — Escalate to mechanical circulatory support
In the deteriorating patient (SCAI D/E, or rising lactate on maximal pharmacology), call the MCS team: Impella to unload the LV, VA-ECMO for the biventricular or respiratory failure. The intra-aortic balloon pump is not routinely used (IABP-SHOCK II — no mortality benefit).
The shock ladder and the evidence
The vasopressor of choice is noradrenaline, preferred over dopamine because the dopamine carries a higher arrhythmic risk. The inotrope — dobutamine (a beta-1 agonist that raises the cardiac output but may worsen ischaemia and arrhythmia) or milrinone (a phosphodiesterase inhibitor that inodilates with less tachyarrhythmia but may vasodilate and drop the pressure) — is added for the low-output state. Mechanical circulatory support is escalated early in the deteriorating patient: the intra-aortic balloon pump has no mortality benefit (IABP-SHOCK II)[3] and is no longer routinely recommended; the Impella (a percutaneous left-ventricular assist device) and the veno-arterial extracorporeal membrane oxygenation (VA-ECMO) are used as a bridge to recovery, to a decision, or to a durable therapy (a transplant or a long-term LVAD).
The inotropes and the vasopressors — the agent-by-agent pharmacology
The choice of the agent follows the haemodynamic problem: a pressor for the pressure, an inotrope for the output, an agent that does both when both are failing. The doses are weight-based and titrated to the perfusion, not the number.[6]
Noradrenaline (pressor of choice)
- Alpha + mild beta-1 agonist
- 0.05–0.5 mcg/kg/min, titrate to MAP ≥ 65
- Restores coronary perfusion pressure
- Preferred over dopamine (SOAP II — less arrhythmia)
Dobutamine (inotrope)
- Beta-1 agonist; raises CO, lowers SVR
- 2.5–20 mcg/kg/min
- Fast onset, short half-life, easy to titrate
- Watch: tachyarrhythmia, myocardial ischaemia, hypotension
Milrinone (inodilator)
- PDE-3 inhibitor; inotrope + vasodilator
- 0.125–0.75 mcg/kg/min
- Less tachyarrhythmia than dobutamine
- May drop the BP; avoid in severe AS; renally cleared
Adrenaline (pressor + inotrope)
- Alpha + beta agonist; single-agent support
- 0.05–1 mcg/kg/min
- Useful when both pressure and output are low
- Raises lactate (anaerobic glycolysis), arrhythmogenic
Dopamine (avoid first-line)
- Dose-dependent alpha/beta/dopaminergic
- Higher arrhythmia risk than noradrenaline
- SOAP II: more arrhythmia, no mortality benefit
- Reserved for bradycardia-induced shock
Vasopressin (adjunct)
- V1 agonist; catecholamine-sparing
- 0.01–0.04 units/min
- Useful in the vasoplegic component
- Caution: mesenteric/digital ischaemia
Mechanical circulatory support — unloading the failing pump
When the pharmacology cannot hold the output, the logical therapy is to mechanically unload and support the ventricle — to break the afterload trap at the heart of the vicious cycle. The contemporary devices are the percutaneous LV assist (the Impella) and the veno-arterial ECMO; the intra-aortic balloon pump, the oldest and the simplest, has been demoted by the evidence.[7]
Intra-aortic balloon pump (IABP)
- Balloon in the descending aorta; inflates in diastole
- Raises coronary perfusion, lowers afterload modestly
- No mortality benefit (IABP-SHOCK II)
- Reserved for the mechanical complication bridge to surgery
Impella (percutaneous LVAD)
- Axial-flow pump across the aortic valve; drains LV → aorta
- Direct LV unloading; up to 2.5–5 L/min (cp/CP)
- Reduces LV work, raises the mean systemic pressure
- Risks: haemolysis, limb ischaemia, aortic regurgitation
VA-ECMO
- Drains RA → oxygenates → returns to femoral artery
- Supports both ventricles and the oxygenation
- 2–6 L/min; the only device for biventricular failure
- Risks: differential hypoxia, limb ischaemia, bleeding, LV afterload rise
The cause-treatment evidence
The SHOCK trial established that an early revascularisation of the infarct-related artery in the MI-shock patient reduced the long-term mortality despite no significant 30-day difference — the benefit emerges over months.[1] The CULPRIT-SHOCK trial showed that a culprit-only PCI (the infarct artery alone) in the patient with multivessel disease and shock produced a better outcome than a multivessel intervention during the acute episode — the non-culprit lesions are addressed later.[2]
The landmark trials
SHOCK — early revascularisation in MI-cardiogenic shock (NEJM 1999; 6-yr follow-up JAMA 2006)
New England Journal of Medicine / JAMA
PMID 10460813
Key finding
A multicentre randomised trial of 302 patients with the MI complicated by the shock, comparing the early revascularisation (PCI or CABG within 18 hours) against the initial medical stabilisation. The 30-day mortality was not significantly different, but the 6-month and the 6-year mortality were significantly lower with the early revascularisation (47.6 per cent vs 56.0 per cent at 6 years).<Cite id="5"/> The benefit was greatest in the under-75 age group.
Practice change
The early revascularisation is the cornerstone of the MI-shock management — the infarct is the cause, and the survival benefit emerges over months even though the 30-day difference is not significant. Revascularise the shocked infarct patient aggressively and early.
CULPRIT-SHOCK — culprit-only vs multivessel PCI in MI-shock (NEJM 2017)
New England Journal of Medicine
PMID 29083953
Key finding
A randomised trial of 1,075 patients with the multivessel disease and the acute MI-shock, comparing the culprit-lesion-only PCI (with the option of the staged non-culprit PCI later) against the immediate multivessel PCI. The culprit-only strategy reduced the 30-day composite of the death or the severe renal failure (45.9 per cent vs 55.4 per cent), driven by both the lower mortality and the lower renal failure.
Practice change
In the MI-shock with the multivessel disease, treat the culprit lesion only during the acute episode — the multivessel intervention during the shock worsens the outcome. The non-culprit lesions are addressed later in a staged fashion.
IABP-SHOCK II — intra-aortic balloon pump in MI-shock (NEJM 2012; long-term Circulation 2019)
New England Journal of Medicine / Circulation
PMID 22920912
Key finding
A randomised trial of 600 patients with the MI-shock planned for the early revascularisation, comparing the IABP against the no-IABP control. The 30-day mortality was identical (39.7 per cent vs 41.3 per cent), and the long-term follow-up at 5 to 6 years showed no mortality benefit and no quality-of-life difference.<Cite id="3"/><Cite id="4"/>
Practice change
The intra-aortic balloon pump has no mortality benefit in the routine MI-shock and is no longer recommended for the routine use. It is reserved for the specific indications — the mechanical complication as a bridge to the surgery, the refractory ischaemia, or the intractable arrhythmia.
ECLS-SHOCK — early VA-ECMO in infarct-related shock (NEJM 2023)
New England Journal of Medicine
PMID 37634145
Key finding
A multicentre randomised trial of 420 patients with the infarct-related cardiogenic shock, comparing the early routine VA-ECMO against the conventional care. The trial was stopped early for futility at the interim analysis; the 30-day all-cause mortality was not reduced (the ECMO arm trended numerically higher).<Cite id="7"/>
Practice change
The early routine VA-ECMO does not improve the outcome in the infarct-related shock. The ECMO remains a bridge for the patient who will die without it, but the selection is everything — the right patient, the right team, the right time — and the routine early cannulation is not supported.
SOAP II — dopamine vs noradrenaline for shock (NEJM 2010)
New England Journal of Medicine
PMID 20200382
Key finding
A multicentre randomised trial of 1,679 patients with any shock type, comparing the dopamine against the noradrenaline as the first-line vasopressor. There was no overall mortality difference, but the dopamine had a significantly higher rate of arrhythmic events (24.1 per cent vs 12.4 per cent) leading to the discontinuation, and a pre-specified cardiogenic-shock subgroup trended toward the higher mortality with the dopamine.<Cite id="6"/>
Practice change
The noradrenaline is the default vasopressor for the shock — the dopamine carries a higher arrhythmia risk without a mortality benefit. The dopamine is reserved for the bradycardia-induced shock where its chronotropy is wanted, and even there the pacing is preferable.
Complications and pitfalls
The complications are the multi-organ failure (the acute kidney injury, the hepatic dysfunction, the bowel ischaemia), the arrhythmia, the worsening ischaemia from the inotrope, and the complications of the mechanical support (a limb ischaemia, a bleeding, a haemolysis, an infection). The pitfalls are the inverse of the management: not revascularising the MI-shock early; giving large fluid boluses to the wet patient; using dopamine as the first-line pressor; missing the mechanical complication (a new murmur post-infarct); delaying the mechanical-support referral; and treating the blood pressure and the lactate rather than the cause.[7]
Prognosis and disposition
The mortality of a cardiogenic shock is around 40 to 50 per cent, lower with the early revascularisation of the infarct. Every patient is admitted to the intensive care or the critical-care unit, with the cardiology and the cardiothoracic involvement; the multi-organ failure is managed; and the longer-term options (a transplant or a left-ventricular assist device) are considered in selected survivors.[5]
Special populations
The elderly carry a higher mortality with more comorbidity. The young patient with a fulminant myocarditis may recover fully on a VA-ECMO bridge and is worth the aggressive support. The peripartum cardiomyopathy patient is managed with the heart-failure therapy and the lactation-safe drugs. The drug-toxicity shock (a beta-blocker or a calcium-channel-blocker overdose) receives the antidote-directed therapy. The post-cardiac-arrest shock is the post-ROSC stunned myocardium that often recovers over 24 to 48 hours.[4]
Evidence and regional guidelines
The contemporary framework is the SHOCK trial (early revascularisation)[1] and the CULPRIT-SHOCK principle (culprit-only PCI).[2] The mechanical-support evidence is the IABP-SHOCK II (no balloon-pump mortality benefit).[3] The noradrenaline-first approach follows the SOAP-2 evidence on the pressor safety. The pharmacologic and the MCS choices follow the ESC and the local cardiology pathways.
ANZ practice note. The cause-first approach, the noradrenaline vasopressor of choice, the culprit-only PCI in the MI-shock, and the early referral for a mechanical circulatory support (Impella, VA-ECMO) follow the ESC framework via the local cardiology, the intensive-care and the cardiothoracic pathways.[2]
Exam practice
SAQ — Cardiogenic shock complicating an anterior STEMI in the cath-lab window
10 minutes · 10 marks
A 62-year-old man presents four hours after the onset of crushing central chest pain. The ECG shows 3 mm ST elevation in V1 to V4 with reciprocal ST depression in the inferior leads — an anterior STEMI — and he has been given aspirin 300 mg, ticagrelor 180 mg and 5000 units of intravenous unfractionated heparin. As the cath-lab is being prepared he deteriorates: he is pale, clammy and mottled from the knees down, BP 74/52, HR 130 in sinus tachycardia, RR 28, SpO2 90 per cent on 15 L oxygen, and he has passed only 10 mL of urine in the last hour. The JVP is raised, there are bibasal crackles, and the bedside echo shows anterior and apical akinesia with an estimated ejection fraction of 18 per cent. The venous gas shows pH 7.22, lactate 6.2 mmol/L, and the troponin is markedly raised.
SAQ — Right-ventricular infarct with shock: the raised-JVP, clear-lungs trap
10 minutes · 10 marks
A 70-year-old man presents three hours after the onset of crushing central chest pain. The ECG shows 2 mm ST elevation in leads II, III and aVF with reciprocal ST depression in I and aVL, and the right-sided V4R shows 1 mm ST elevation. He is pale, cold and clammy: BP 76/50, HR 108 in sinus rhythm, RR 24, SpO2 94 per cent on room air. The JVP is raised to the angle of the jaw at 45 degrees, the lung fields are clear, and there is no pulmonary oedema. The bedside echo shows a dilated, poorly contracting right ventricle with preserved left-ventricular systolic function and a septum that bows into the LV in diastole. The venous gas shows pH 7.28, lactate 4.6 mmol/L. He has been given aspirin 300 mg, ticagrelor 180 mg and 5000 units of unfractionated heparin, and the nurse has just administered sublingual glyceryl trinitrate for the ongoing chest pain, after which his systolic fell from 110 to 76.
Exam pearls
- MI-shock → revascularise immediately (SHOCK trial) — the infarct is the cause and the spiral will not stop untreated.
- Noradrenaline is the preferred vasopressor; dopamine is no longer first-line (arrhythmia).
- Dobutamine or milrinone as the inotrope — watch the ischaemia and the arrhythmia.
- IABP has no mortality benefit (IABP-SHOCK II) — Impella and VA-ECMO are the devices that unload.
- Culprit-only PCI in multivessel MI-shock (CULPRIT-SHOCK) — multivessel during shock is worse.
- Find the mechanical complication: a new murmur post-infarct = VSD, papillary-muscle rupture, or free-wall rupture.
- The lactate is the perfusion marker — the trend matters more than the single value.
- The SCAI stages drive the escalation: A (at risk), B (beginning), C (classic — hypotensive, on a pressor), D (deteriorating — escalating support), E (extremis — arrest).
- The vicious cycle: low cardiac output → hypotension → coronary hypoperfusion → worsening LV function → deeper hypoperfusion. Break it with unloading and revascularisation, not pressors alone.
- Noradrenaline restores the coronary perfusion pressure; add dobutamine or milrinone for the output. A pure alpha-agonist (metaraminol) alone raises the afterload and drops the stroke volume — the number improves while the patient dies.
- S3 + raised JVP + cold periphery + wet lungs = cardiogenic shock at the bedside, before any investigation returns.
- The warm vasodilatory phase of the early cardiogenic shock mimics sepsis — the low cardiac output on the echo is the distinguishing clue.
- The RV infarct presents with the shock, a raised JVP and clear lungs (and ST elevation in V4R) — it is preload-dependent: volume-load, reperfuse, avoid the nitrates and the diuretics.
- VA-ECMO raises the LV afterload and can distend a failing LV — add an Impella (the ECPELLA strategy) to unload it.
- ECLS-SHOCK (2023): the early routine VA-ECMO does not reduce the mortality — reserve the ECMO for the patient who will die without it.
- The calcium-channel-blocker or beta-blocker overdose produces a cardiogenic shock treated with the high-dose insulin/euglycaemia, the calcium, and the lipid emulsion — escalate to the MCS for the refractory.[2]
Red flags
[4]References
- [1]Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock (SHOCK). New England Journal of Medicine, 1999.PMID 10460813
- [2]Thiele H, Akin I, Sandri M, et al. PCI strategies in patients with acute myocardial infarction and cardiogenic shock (CULPRIT-SHOCK). New England Journal of Medicine, 2017.PMID 29083953
- [3]Thiele H, Akin I, Sandri M, et al. Long-term outcome in patients with cardiogenic shock complicating acute myocardial infarction (IABP-SHOCK II). Circulation, 2019.PMID 30586721
- [4]Thiele H, Zeymer U, Neumann FJ, et al. Intraaortic balloon support for myocardial infarction with cardiogenic shock (IABP-SHOCK II). New England Journal of Medicine, 2012.PMID 22920912
- [5]Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction. JAMA, 2006.PMID 16757723
- [6]De Backer D, Biston P, Devriendt J, et al. Comparison of dopamine and norepinephrine in the treatment of shock (SOAP II). New England Journal of Medicine, 2010.PMID 20200382
- [7]Thiele H, Freund A, Gimenez MR, et al. Extracorporeal life support in infarct-related cardiogenic shock (ECLS-SHOCK). New England Journal of Medicine, 2023.PMID 37634145
- [8]van Diepen S, Katz JN, Albert NM, et al. Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation, 2017.PMID 28923988
- [9]Baran DA, Grines CL, Bailey S, et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock. Catheterization and Cardiovascular Interventions, 2019.PMID 31104355