EM · Community-acquired pneumonia
Community-acquired pneumonia
Also known as CAP · Pneumonia · Lobar pneumonia
Community-acquired pneumonia — the CURB-65 severity assessment (Confusion, Urea, Respiratory rate, Blood pressure, age 65), the pathogen classification (typical and atypical), the antibiotic regimens by severity (outpatient amoxicillin, ward IV amoxicillin and clarithromycin, ICU penicillin and a macrolide with Gram-negative cover), the Hour-1 sepsis bundle, the complications (parapneumonic effusion, empyema, lung abscess, ARDS), and the legionella and aspiration subtypes. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
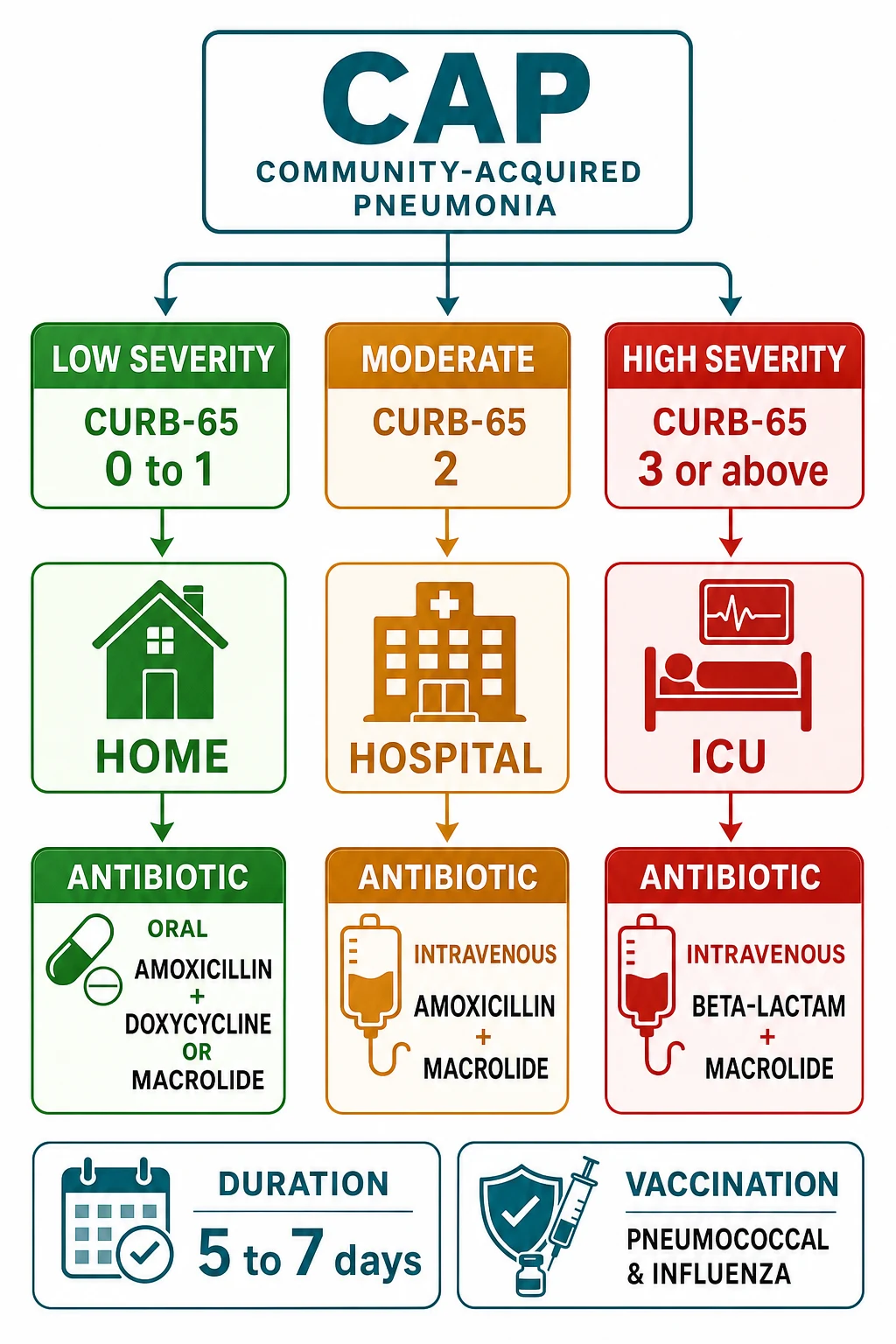
Community-acquired pneumonia is one of the commonest and most lethal infections the emergency physician manages, and the Fellowship candidate must assess its severity with the CURB-65 score, choose the antibiotic regimen by that score, and treat the accompanying sepsis within the first hour. The distinction between a mild pneumonia managed at home with oral amoxicillin and a severe pneumonia in the intensive care unit with intravenous penicillin and a macrolide is made entirely by the bedside assessment, not by the chest radiograph alone.[1][2]
Definition and classification
Community-acquired pneumonia is an acute infection of the lung parenchyma, acquired outside the hospital (or within 48 hours of admission). It is classified by the severity (the CURB-65, the PSI, or the SMART-COP score), by the site of care (outpatient, ward, intensive care), and by the pathogen — the typical bacteria (the pneumococcus, Haemophilus influenzae, Moraxella catarrhalis, and in the severe or the aspiration case the Gram-negatives and the Staphylococcus aureus), the atypical bacteria (Mycoplasma pneumoniae, Legionella pneumophila, Chlamydia pneumoniae), and the viruses (influenza, respiratory syncytial virus, and the SARS-CoV-2). The pathogen matters because it guides the antibiotic cover, but the severity matters more because it decides the site of care and the urgency.[6]
Causative organisms — the pathogen spectrum
The empiric regimen is shaped by the relative frequency of the pathogens, and the Fellowship candidate must be able to recite the spectrum in order. Streptococcus pneumoniae (the pneumococcus) is by far the commonest bacterial cause of the community-acquired pneumonia at every severity, and it is the organism the empiric regimen is built around. Haemophilus influenzae and Moraxella catarrhalis follow, particularly in the chronic-lung-disease patient. The atypicals — Mycoplasma pneumoniae, Legionella pneumophila, and Chlamydia pneumoniae — lack a peptidoglycan cell wall and are therefore unreachable by a beta-lactam alone; they demand a macrolide, a tetracycline, or a respiratory fluoroquinolone, which is why the moderate and the severe regimen always pairs a beta-lactam with a macrolide. The viruses (the influenza, the respiratory syncytial virus, and the SARS-CoV-2) are now recognised as a leading cause, and they warrant a respiratory PCR and, in season, an early neuraminidase inhibitor. Staphylococcus aureus (including the post-influenzal, often necrotising MRSA pneumonia) and the Gram-negative bacilli (the Klebsiella pneumoniae of the alcohol-excess patient, the Pseudomonas aeruginosa of the bronchiectatic lung) define the severe, the healthcare-associated, and the aspiration subgroups. The causative organism is identified in only about half the inpatient cases, which is why the empiric cover is built on the likely spectrum rather than on a confirmed isolate.[3][10]
Typical bacteria
- Streptococcus pneumoniae — the #1 cause at every severity
- Haemophilus influenzae — COPD, bronchiectasis
- Moraxella catarrhalis — COPD exacerbations
- Covered by: amoxicillin, benzylpenicillin, ceftriaxone, co-amoxiclav
- Cell-wall active agents work — beta-lactams are first-line
Atypical bacteria
- Mycoplasma pneumoniae — young adults, dry cough, myalgia
- Legionella pneumophila — hyponatraemia, GI, neuro, deranged LFTs
- Chlamydia pneumoniae — insidious, hoarse voice, sore throat
- Covered by: macrolide, doxycycline, respiratory fluoroquinolone
- NO cell wall → beta-lactams fail; pair with a macrolide
Viruses
- Influenza A/B — seasonal, sudden onset, myalgia
- Respiratory syncytial virus (RSV) — elderly, immunocompromised
- SARS-CoV-2 — hypoxaemia out of proportion, bilateral infiltrates
- Send respiratory PCR; start oseltamivir early in season
- Consider adding MRSA cover in post-influenzal pneumonia
Gram-negatives / S. aureus
- Klebsiella pneumoniae — alcohol excess, aspiration (Friedländer)
- Pseudomonas aeruginosa — bronchiectasis, severe COPD, prior ICU
- Staphylococcus aureus — post-influenzal, necrotising, cavitation
- Add Gram-negative cover (pip-tazo / ceftriaxone) if risk factors
- Add MRSA cover (vancomycin/linezolid) if post-influenzal or severe
Pathophysiology
The organisms reach the alveoli by micro-aspiration from the upper airway or by inhalation, evade the mucociliary and the macrophage defences, and trigger an inflammatory exudate that fills the alveolar space — the consolidation. The consolidated lung segment has a ventilation–perfusion mismatch (blood flows through underventilated alveoli), which produces the hypoxia. The local inflammation triggers a systemic inflammatory response that, in the severe case, progresses to the sepsis and the septic shock. The causative organism is never identified in about half the inpatient cases, which is why the empiric regimen is broad enough to cover the likely spectrum.[7]
The CURB-65 severity score
The CURB-65 is the bedside severity score that the Fellowship candidate must be able to calculate instantly and reproduce. Each of the five features scores one point.[4]
CURB-65 — five features, one point each
CURB-65
New mental disorientation (abbreviated mental test ≤8, or disorientation in person, place or time)
Blood urea nitrogen (urea) above 7 mmol/L — a marker of sepsis severity and dehydration
30 breaths per minute or more
Systolic below 90 mmHg or diastolic 60 mmHg or below
65 years or older
The CURB-65 score then directs the site of care. A score of 0 or 1 supports outpatient management (home, with oral antibiotics and a safety-net). A score of 2 warrants an inpatient admission to the ward (intravenous antibiotics, monitored). A score of 3, 4 or 5 is severe and warrants an intensive-care-level admission and intravenous broad-spectrum cover. The score is a guide, not a rule — the clinical judgement (the oxygenation, the social circumstances, the comorbidity) modifies it — but it provides the objective framework for the disposition decision.[1]
Alternative severity scores — PSI, CRB-65, and SMART-COP
The CURB-65 is the bedside favourite because all five variables are available at the first assessment, but the Fellowship candidate must know the alternatives and when each is stronger. The Pneumonia Severity Index (PSI / the PORT score) of Fine is the most accurate predictor of the short-term mortality, stratifying the patient into the five risk classes (I–V) by 20 weighted variables (the demography, the comorbidity, the examination, the laboratory and the radiographic findings).[5] Its strength is a high negative predictive value — it safely identifies the low-risk class I–II patient for the discharge — but it is a paper or an app score, not a bedside one, and it can underestimate an ill young patient with a single dangerous vital sign. The CRB-65 drops the urea (no blood test needed) and is the community and the pre-hospital tool: a score of 0 is safe for the home, and a score of 1 or more warrants the hospital assessment. The SMART-COP of Charles was derived specifically to predict the need for the intensive respiratory or the vasopressor support, and it outperforms the CURB-65 for the prediction of the ICU-level need.[6] Its eight variables (the low Systolic BP, the low Multi-lobar involvement, the low Albumin, the high Respiratory rate, the high Tachycardia, the Confusion, the low Oxygenation, the low arterial pH) flag the patient who will decompensate; a SMART-COP of 3 or more predicts the need for the intensive support.
CURB-65
- 5 variables, 1 point each (max 5)
- Confusion, Urea >7, RR ≥30, BP <90/60, Age ≥65
- Bedside — no calculator needed
- 0–1 home, 2 ward, 3–5 ICU
- Predicts 30-day mortality; ANZ/BTS first-line
PSI (PORT)
- ~20 weighted variables, 5 risk classes (I–V)
- Best mortality predictor; highest negative predictive value
- Paper/app score — too complex for the bedside
- Class I–II discharge, IV–V consider ICU
- Can underestimate a single ill young patient
CRB-65
- 4 variables — drops the urea (no bloods needed)
- Confusion, RR ≥30, BP <90, Age ≥65
- The community / pre-hospital tool
- 0 = safe home; ≥1 = hospital assessment
- Use where venepuncture is impractical
SMART-COP
- 8 variables predicting the need for IRVS
- SBP, Multilobar, Albumin, RR, HR, Confusion, O₂, pH
- Best predictor of ICU / ventilatory / vasopressor need
- ≥3 = high risk of needing intensive support
- Sensitive for early deterioration that CURB-65 may miss
SMART-COP — eight variables, two points for the worst
SMART-COP
Below 90 mmHg (2 points)
Multilobar involvement on the chest radiograph (1 point)
Albumin below 3.5 g/dL (1 point)
≥25 breaths/min, age-adjusted (1 point)
Heart rate ≥125 beats/min (1 point)
New disorientation (1 point)
Oxygenation low — SaO₂ <90% or PaO₂ <60 mmHg (2 points)
Arterial pH below 7.35 (2 points)
Clinical presentation
The patient presents with a fever, a productive cough (purulent, or the rusty sputum of the pneumococcus), a dyspnoea, and a pleuritic chest pain, often with rigors and a generalized malaise. The signs include a tachypnoea, a tachycardia, a focal reduction in the chest expansion, a dull percussion note, crackles or a bronchial breathing over the consolidated segment, and a hypoxia. The confusion (especially in the elderly) is a sign of severity, not a primary neurological problem. The atypical pneumonias (mycoplasma, legionella) present more insidiously, with a dry cough, a headache, a myalgia, and the prominent gastrointestinal or the neurological features. The examination and the severity scoring are the first actions; the chest radiograph confirms the consolidation.[4]
Differential diagnosis
The breathless, febrile patient with a chest-radiograph abnormality has a differential, and the history, the bloods and the imaging resolve it.[1]
Community-acquired pneumonia
- Fever, purulent sputum, focal consolidation
- CURB-65 scores the severity; antibiotics within 1 h
- Blood cultures, sputum, urinary antigens
- Typical or atypical pathogen
Pulmonary embolism
- Pleuritic pain, syncope; DVT signs
- No fever (usually); no purulent sputum
- Wells/PERC → D-dimer → CTPA
- Anticoagulation, not antibiotics
Pulmonary oedema
- No fever; raised JVP, crackles, S3
- BNP raised; echo shows LV dysfunction
- CXR: bat-wing, Kerley B, cardiomegaly
- Diuretic, nitrate, not antibiotic
Tuberculosis / malignancy
- Chronic, weight loss, night sweats (TB)
- Upper-lobe predominant; cavitation
- Sputum AFB; CT; biopsy for malignancy
- Specific therapy, not empiric antibiotics
Investigations
The chest radiograph confirms the diagnosis and shows the pattern and the extent of the consolidation, a multilobar involvement (a marker of severity), and any complication (a parapneumonic effusion, a cavitation). The blood cultures are taken before the antibiotics (but do not delay the antibiotic dose beyond 45 minutes for the cultures). The sputum is sent for the Gram stain, the culture and the sensitivity, and a urinary antigen for the pneumococcus and the legionella is sent in the moderate and the severe case. A respiratory viral PCR (influenza, SARS-CoV-2, RSV) is sent in the season. The bloods include the full blood count, the urea and electrolytes (the urea is the CURB-65 criterion), the C-reactive protein, the liver function tests (the derangement raises legionella), and the sodium (the hyponatraemia raises legionella). An arterial blood gas is taken in the severe case to quantify the hypoxia and the acidosis, and the lactate is the key marker of the sepsis severity.[4]
Immediate management — the severity-directed antibiotic regimen
Stabilise the airway and the breathing with oxygen to a saturation target of 94 to 98 per cent (88 to 92 in the chronic obstructive pulmonary disease). If the patient is in sepsis, apply the Hour-1 bundle: the cultures are drawn, the antibiotics are given, a balanced crystalloid is infused for the hypotension or the lactataemia, and a vasopressor is started if the fluid does not hold the pressure. Then the antibiotic regimen, directed by the CURB-65 and the likely pathogen.[8]
[8]CURB-65 score and the disposition
The aspiration pneumonia (in the alcohol-excess, the seizure, or the stroke patient) adds an anaerobic cover: co-amoxiclav, or clindamycin with a gentamicin. The legionella pneumonia presents with the hyponatraemia, the gastrointestinal symptoms, the neurological features and the deranged liver function tests, and is covered by the macrolide; the urinary antigen confirms it, and public health is notified. The antibiotic course is 5 to 7 days for the simple case, and 7 to 14 days for the legionella, the staphylococcal, or the complicated case. The patient is reassessed at 48 hours and switched to the oral route when the temperature settles, the respiratory rate normalises, and the patient is eating.[8]
ED disposition and the door-to-antibiotic clock
The disposition in the emergency department fuses the CURB-65 score with the clinical judgement — the score is the framework, never the sole arbiter. A low score (0–1) is discharged home only if the oxygenation, the social circumstances, the oral intake, and the ability to return are all reassuring; a single point of clinical concern (a rising lactate, a multilobar radiograph, an immunocompromise, a pregnant patient) overrides the score and admits. The elderly, the pregnant, and the socially-isolated patient may warrant the admission at a score that would send a younger, well-supported patient home. Conversely, the score of 2 is a ward admission, but the score of 3 or more — or any of the SMART-COP high-risk markers, or a lactate above 2 mmol/L with the hypotension — escalates to the high-dependency or the intensive care.[3]
The door-to-antibiotic time is the single most modifiable emergency-department process measure, and the Fellowship candidate must know both the benchmarks. The classic benchmark, drawn from the Meehan Medicare cohort of more than 14 000 elderly inpatients, is a first antibiotic within 4 hours of the presentation for the admitted patient — the antibiotic within this window was associated with a lower in-hospital mortality and a shorter stay.[9] For the patient with the severe sepsis or the septic shock, the standard is tighter: the Surviving Sepsis Campaign Hour-1 bundle mandates the broad-spectrum antibiotics within 1 hour of the recognition of the sepsis or the shock.[7] The reason is the Kumar data — in the septic-shock cohort, the survival fell by approximately 7.6 percentage points for every hour the effective antimicrobial was delayed after the onset of the hypotension.[8] The cultures are drawn before the antibiotics, but the antibiotic dose is never delayed beyond 45 minutes for the cultures.
The first 60 minutes of the severe community-acquired pneumonia
0 min — recognise and the ABCDE
The airway, the high-flow oxygen to the 94–98 per cent target (88–92 in the COPD), the full monitoring, two large-bore cannulae. Score the CURB-65 and the SMART-COP at the bedside.
0–15 min — the bloods, the cultures, and the lactate
The venous gas and the lactate, the FBC, the U&E (the urea), the CRP, the LFTs, the coagulation. The two blood cultures, the sputum, and the urinary pneumococcal and legionella antigens before the antibiotics. Do NOT delay the antibiotic beyond 45 min for the cultures.
0–60 min — the Hour-1 sepsis bundle
The broad-spectrum antibiotics within 1 hour of the recognition (ceftriaxone 2 g IV + azithromycin 500 mg IV for the severe CAP; add vancomycin if the post-influenpal or the MRSA is suspected). The 30 mL/kg crystalloid for the hypotension or the lactate ≥4. The vasopressor (noradrenaline) if the fluid does not hold the MAP ≥65.
15–30 min — the imaging and the diagnostics
The chest radiograph (the consolidation, the multilobar involvement, the effusion). The ABG if the hypoxaemic or the acidotic. The respiratory viral PCR in the season. The HIV test. Consider the bedside ultrasound (the B-lines, the consolidation, the effusion).
30–60 min — the disposition by the score and the trajectory
The CURB-65 0–1 with the reassuring clinical picture → the home with the oral amoxicillin and the safety-net. The CURB-65 2 → the ward. The CURB-65 ≥3, the SMART-COP ≥3, the lactate ≥2 with the hypotension, or the failing oxygenation → the HDU/ICU.
60 min onward — the reassessment
Recheck the SpO₂, the RR, the BP, the GCS, the lactate clearance. The rising lactate or the worsening gas exchange → the escalation (the non-invasive or the invasive ventilation, the second vasopressor). Document the time of the first antibiotic for the audit.
The door-to-antibiotic clock
Complications and pitfalls
The complications of the severe pneumonia are the sepsis and the septic shock, the respiratory failure (the acute respiratory distress syndrome in the worst case), the parapneumonic effusion and the empyema (an effusion that is loculated or purulent needs a chest drain, not just the antibiotics), and the lung abscess (a cavitating infection, often staphylococcal or anaerobic, needing a prolonged antibiotic course and sometimes a surgical drainage). The pitfalls are the dangerous inverse of the management: under-scoring the severity; delaying the antibiotics for the cultures beyond the 45-minute cap; not covering the atypicals; missing the legionella (the hyponatraemia, the gastrointestinal features, the deranged liver function tests); missing the aspiration; and not reassessing the oxygenation and the clinical trajectory at the 48-hour mark.[8]
Prognosis and disposition
The CURB-65 score predicts the 30-day mortality, which rises from about 1 per cent at a score of 0 to over 30 per cent at a score of 5. The disposition follows the score (the home, the ward, or the intensive care). The clinical response is reassessed at 48 hours — a failure to improve (a persistent fever, a rising inflammatory marker, a worsening radiograph) prompts a review of the antibiotic choice, a search for a complication (an effusion, an abscess, an empyema), and the consideration of a resistant organism or an alternative diagnosis.[6]
Special populations
The elderly present atypically (a confusion, a fall, a reduced appetite rather than a fever and a cough) and have a higher mortality at every CURB-65 level. The chronic obstructive pulmonary disease patient has a more severe course and a broader pathogen spectrum (the pseudomonas risk), which may warrant the Gram-negative cover. The immunocompromised patient (the neutropenic, the transplant, the HIV-positive) requires the broadest empiric cover and an early consideration of the opportunistic pathogens (the Pneumocystis, the fungal). The pregnant patient receives the beta-lactam and the macrolide, which are safe in pregnancy. The alcohol-excess patient has the aspiration risk and the Klebsiella predisposition.[9]
Evidence and regional guidelines
The contemporary frameworks are the British Thoracic Society community-acquired-pneumonia guideline[1] and the NICE pneumonia guideline, which are aligned,[2] alongside the ATS/IDSA 2019 guideline of Metlay[3] and the earlier IDSA/ATS consensus of Mandell.[10] The CURB-65 score (Lim[4]), the PSI (Fine[5]) and the SMART-COP (Charles[6]) are the three validated severity scores. The sepsis management follows the Surviving Sepsis Campaign 2021.[7] The empiric antibiotic choices follow the local antibiogram and the hospital's resistance patterns. The drug choices are global; the exact regimen, the atypical cover, and the site-of-care thresholds are local.
ANZ practice note. The CURB-65 severity scoring and the empiric antibiotic regimen follow the Therapeutic Guidelines (eTG) and the local hospital antibiogram; the Gram-negative cover (piperacillin-tazobactam or ceftriaxone) is added for the severe, the nursing-home, or the recently-antibiotic-exposed patient, and the atypical cover (azithromycin or clarithromycin) is routine in the moderate and the severe case.[4]
Landmark evidence
Metlay 2019 — ATS/IDSA CAP Guideline
Am J Respir Crit Care Med
PMID 31573350
Key finding
The joint American Thoracic Society / Infectious Diseases Society of America clinical practice guideline for the diagnosis and the treatment of the community-acquired pneumonia in adults. It endorses the empiric beta-lactam–macrolide or the respiratory-fluoroquinolone regimen, the routine atypical cover, the corticosteroid consideration in the severe CAP, and the radiographic follow-up.
Practice change
The contemporary North-American standard — the empiric regimen and the severity-directed disposition mirror the BTS/NICE framework. The beta-lactam plus the macrolide is the global consensus for the severe CAP.
Lim 2003 — the original CURB-65 (Thorax)
Thorax
PMID 12728155
Key finding
An international derivation and validation study of the CURB-65 severity score in the community-acquired pneumonia. The 30-day mortality rose from 1.5 per cent at a score of 0 to 57 per cent at a score of 5, validating the 0–1 home, 2 ward, 3–5 ICU disposition thresholds.
Practice change
The evidence base for the bedside score that every emergency physician calculates — the foundation of the severity-directed antibiotic regimen.
Kumar 2006 — the antibiotic-timing in the septic shock (Crit Care Med)
Crit Care Med
PMID 16625125
Key finding
A retrospective cohort of 2158 patients with the septic shock. The effective antimicrobial therapy within the first hour of the hypotension was associated with a survival of 79.9 per cent; each additional hour of the delay reduced the survival by approximately 7.6 percentage points.
Practice change
The quantitative justification for the Hour-1 antibiotic mandate in the severe CAP with the septic shock — the antibiotic is the single most time-critical intervention.
Charles 2008 — the SMART-COP score (Clin Infect Dis)
Clin Infect Dis
PMID 18558884
Key finding
A derivation and validation study of the SMART-COP score for the prediction of the need for the intensive respiratory or the vasopressor support in the community-acquired pneumonia. A score of 3 or more identified the high-risk patient with a sensitivity that exceeded the CURB-65 for the ICU-level need.
Practice change
When the question is "ward or ICU", the SMART-COP is the more sensitive tool — use it alongside the CURB-65 for the borderline or the deteriorating patient.
Meehan 1997 — the door-to-antibiotic benchmark (JAMA)
JAMA
PMID 9403422
Key finding
A cohort study of 14 069 Medicare inpatients aged ≥65 with the community-acquired pneumonia. The antibiotic administered within 8 hours of the arrival was associated with a lower 30-day mortality, establishing the time-to-antibiotic as a measurable quality benchmark.
Practice change
The origin of the door-to-antibiotic clock — the basis for the 4-hour (and now the 1-hour severe-sepsis) targets that the emergency department audits.
Fine 1997 — the Pneumonia Severity Index (NEJM)
N Engl J Med
PMID 8995086
Key finding
A prospective cohort study deriving and validating the Pneumonia Severity Index (the PORT score), a 20-variable model stratifying the community-acquired pneumonia into five mortality classes. The class I and II patients were low-risk and candidates for the outpatient therapy.
Practice change
The most accurate mortality prediction rule, and the high-negative-predictive-value tool for the safe discharge decision when the CURB-65 is borderline.
Evans 2021 — Surviving Sepsis Campaign (Crit Care Med)
Crit Care Med
PMID 34643578
Key finding
The 2021 international guidelines for the management of the sepsis and the septic shock. They recommend the antibiotics within 1 hour for the suspected sepsis with the shock or the high likelihood, the 30 mL/kg crystalloid for the hypotension or the lactate ≥4, and the early vasopressor to hold the MAP ≥65.
Practice change
The Hour-1 bundle is the operational standard for the severe CAP that presents as the sepsis — the antibiotic within 1 hour is non-negotiable.
Davies 2010 — BTS Pleural Disease Guideline (Thorax)
Thorax
PMID 20696693
Key finding
The British Thoracic Society guideline for the management of the pleural infection in adults. It stratifies the parapneumonic effusion into the categories 1–4, defines the indicators for the chest drain (the pus, the positive culture, the pH <7.2, the loculation), and recommends the intrapleural tPA/DNase for the complicated effusion failing the drainage.
Practice change
The framework for the parapneumonic-effusion complication — the pH <7.2 or the pus is the drain, not just the antibiotic. The CAP that develops a complicated effusion is managed jointly with the respiratory team.
Exam pearls
- CURB-65: Confusion, Urea >7, RR ≥30, BP <90/≤60, age ≥65 → 0–1 home, 2 ward, 3–5 ICU/consider. Calculate it at the bedside — it is the BTS/NICE and eTG default.
- Door-to-antibiotic: <4 h for the admitted CAP (Meehan), <1 h for the severe sepsis/septic shock (Surviving Sepsis Hour-1). Antibiotics are the most time-critical intervention in the severe CAP.
- Empiric therapy by severity: outpatient — amoxicillin (or doxycycline/clarithromycin if penicillin-allergic); ward non-severe — IV amoxicillin + clarithromycin (or a respiratory fluoroquinolone); severe/ICU — ceftriaxone/benzylpenicillin + macrolide, add Gram-negative cover (pip-tazo) and vancomycin for the MRSA/post-influenpal risk.
- Cover the atypicals (Mycoplasma, Legionella, Chlamydia) with a macrolide — they have no cell wall, so a beta-lactam alone fails. The beta-lactam + macrolide pair is the two halves of the empiric spectrum.
- Legionella: hyponatraemia, GI symptoms, neurological features, raised LFTs → urinary antigen, macrolide (or fluoroquinolone), notify public health. The course is 7–14 days.
- Lactate is the key sepsis marker — a lactate ≥2 with hypotension, or ≥4 alone, triggers the Hour-1 bundle and the ICU discussion. A rising urea is the sepsis severity, not a primary renal problem.
- SMART-COP ≥3 predicts the need for intensive support — use it when the question is "ward or ICU". The PSI (Fine) is the most accurate mortality predictor and the safe-discharge arbiter for the borderline CURB-65 of 2.
- Switch to oral when afebrile + RR normal + eating (usually at 48 h) — the criteria for the step-down. A failure to improve at 48 h prompts the review of the antibiotic, the search for a complication, and the reconsideration of the diagnosis.
- A parapneumonic effusion that is loculated or purulent (or pH <7.2) is an empyema → chest drain ± intrapleural tPA/DNase, not just antibiotics. Send the pleural fluid for the pH, the LDH, the Gram stain and the culture.
- Aspiration pneumonia (alcohol excess, seizure, stroke) adds anaerobic cover — co-amoxiclav, or clindamycin ± gentamicin. The Klebsiella predisposition in the alcohol-excess patient is the "Friedländer" pneumonia.
- The post-influenpal pneumonia is often staphylococcal (MRSA) and necrotising — add vancomycin or linezolid and look for the cavitation on the CT. Send the respiratory viral PCR and start oseltamivir early in season.
- The non-resolving consolidation at 6 weeks is a red flag for the bronchial malignancy — arrange the repeat chest radiograph at 6 weeks for every admitted CAP, and the CT/bronchoscopy if it has not resolved.
- Cultures before antibiotics, but never delay the antibiotic >45 min for the cultures. The blood cultures, the sputum, and the urinary pneumococcal/legionella antigens are sent in the moderate and the severe case.
- Oxygen target 94–98 per cent (88–92 in the COPD retainer) — do not give the high-flow oxygen indiscriminately to the chronic CO₂ retainer. The hypoxaemic, tiring patient is heading for the ventilatory support.
- The elderly present atypically — confusion, a fall, a reduced appetite rather than the fever and the cough — and have a higher mortality at every CURB-65 level. A low threshold for the admission and the bloods.
- Consider corticosteroids in the severe CAP (hydrocortisone) per the ATS/IDSA 2019 suggestion — they may reduce the mortality and the ARDS in the severe case, but are not routine in the uncomplicated CAP.[6]
Exam practice
SAQ — CURB-65 scoring and the ward-level community-acquired pneumonia
10 minutes · 10 marks
A 68-year-old man with type 2 diabetes and a 40-pack-year smoking history presents with three days of fever, a productive rust-coloured sputum, right-sided pleuritic chest pain and worsening dyspnoea. On arrival he is alert and oriented (GCS 15), temperature 38.6 degrees C, heart rate 104, respiratory rate 26, blood pressure 124/72, SpO2 93 per cent on room air. Bloods: urea 8.4 mmol/L, WCC 17.2, CRP 185, sodium 136, lactate 1.8. The chest radiograph shows right lower lobe consolidation. The urinary pneumococcal antigen is positive.
SAQ — Severe community-acquired pneumonia with septic shock requiring ICU
12 minutes · 10 marks
A 54-year-old previously well man is brought to the emergency department with two days of fever, a productive cough, myalgia and a progressive breathlessness, followed by the drowsiness. There is an influenza-like illness in the household. On arrival he is drowsy (GCS 13) and confused, pale and mottled peripherally: temperature 38.9 degrees C, heart rate 132, respiratory rate 34, blood pressure 78/46 (MAP 56), SpO2 86 per cent on 15 L via a non-rebreather. Bloods: urea 12.4 mmol/L, WCC 24.5, CRP 320, sodium 128, lactate 4.6, creatinine 165. The chest radiograph shows bilateral multilobar consolidation. The ABG: pH 7.24, PaO2 7.2 kPa, PaCO2 4.1 kPa, bicarbonate 16. The qSOFA is 3.
Red flags
[6]References
- [1]Lim WS, Baudouin SV, George RC, et al. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax, 2009.PMID 19783532
- [2]Lim WS. British Thoracic Society community acquired pneumonia guideline and the NICE pneumonia guideline: how they fit together. Thorax, 2015.PMID 25977290
- [3]Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med, 2019.PMID 31573350
- [4]Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax, 2003.PMID 12728155
- [5]Fine MJ, Auble TE, Yealy DM, et al. A prediction rule to identify low-risk patients with community-acquired pneumonia. N Engl J Med, 1997.PMID 8995086
- [6]Charles PG, Wolfe R, Whitby M, et al. SMART-COP: a tool for predicting the need for intensive respiratory or vasopressor support in community-acquired pneumonia. Clin Infect Dis, 2008.PMID 18558884
- [7]Evans L, Rhodes A, Alhazzani W, et al. Executive summary: Surviving Sepsis Campaign: International Guidelines for the Management of Sepsis and Septic Shock 2021. Crit Care Med, 2021.PMID 34643578
- [8]Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med, 2006.PMID 16625125
- [9]Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA, 1997.PMID 9403422
- [10]Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis, 2007.PMID 17278083
- [11]Davies HE, Davies RJ, Davies CW, et al. Management of pleural infection in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax, 2010.PMID 20696693