EM · End-of-life and goals of care
End-of-life care and goals-of-care discussions in the emergency department
Also known as Goals-of-care conversation · Not for resuscitation · DNAR · Treatment limitation · Palliative care in the ED · Advance care planning
End-of-life care and goals-of-care discussions in the emergency department — recognising the dying patient across the illness trajectories, the structured goals-of-care conversation (framing, the patient's values, realistic outcomes, and the shared decision), the not-for-resuscitation order and limitation of treatment (not for intubation, CPR, dialysis), the ED palliative pathway with its symptom-control pharmacology (morphine 2.5 mg SC/IV, midazolam 2.5 mg SC, glycopyrrolate 200 micrograms SC, haloperidol 0.5 to 2 mg IV), the family meeting, bereavement support, cultural and spiritual considerations, and the legal and ethical framework of the advance care directive, the enduring guardian and substituted judgement. The differential — the reversible causes of deterioration that must not be missed — runs through every decision. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
End-of-life care in the emergency department is the active, total care of patients whose condition is no longer responsive to curative or life-prolonging treatment, delivered in the one setting least built for it. The modern ED sees a rising tide of older, frailer, multi-morbid patients in the final months of life — many arrive without a prior goals-of-care discussion, and the emergency clinician must, in a single encounter, recognise the dying patient, reverse what is reversible, hold an honest conversation about values and realistic outcomes, and either escalate, limit, or redirect treatment accordingly.[2] This is not the failure of resuscitation; it is a distinct clinical competence, examined directly in the Fellowship OSCE and woven through every high-stakes SAQ on the deteriorating patient. The work rests on a single ethical premise: that the right care is the care aligned with the patient's own values, expressed when they could express them, and applied faithfully when they no longer can.[1]
Definition and scope
End-of-life care encompasses the recognition that a patient is dying, the goals-of-care conversation that aligns treatment with values and prognosis, the limitation or withdrawal of life-sustaining treatment when it cannot meet the patient's goals, the active symptom control that follows, and the support of the family through bereavement. In the ED it is delivered under time pressure, often without a prior relationship, and frequently as a pivot — a patient admitted for one thing is now recognised as dying of another. Primary palliative care — the symptom control, communication and decision-making that every emergency clinician must provide — is distinguished from specialist palliative care, the consultation service called for complex pain, refractory symptoms, or difficult family dynamics.[2] The scope is deliberately wide: the patient brought in dead, the peri-arrest patient whose ceiling is undecided, the patient with known advanced disease in steady decline, and the catastrophic irreversible injury all fall within it.
Recognising the dying patient — the trajectories and the terminal phase
Recognition precedes every other step. The clinician who cannot name the dying patient will either overtreat reversible decline as terminal or undertreat active dying as reversible, and both errors cause harm. Three illness trajectories are taught because they predict the pattern of presentation. The short trajectory is sudden death — the arrest, the massive haemorrhage, the catastrophic intracranial event — where the question is whether resuscitation is appropriate at all. The cancer trajectory is a steady decline with a relatively predictable terminal phase of weeks to days. The organ-failure and frailty trajectory — advanced heart failure, dementia, end-stage respiratory disease — is punctuated by acute deteriorations, each one a possible end, and is the commonest source of goals-of-care uncertainty in the ED.[1]
The terminal phase — the last hours to days of life — has recognisable signs. The patient becomes bedbound, drowsy, and increasingly difficult to rouse; oral intake falls; swallowing becomes unsafe. Peripheries cool and mottle as perfusion fails; the pulse thins and speeds; respiration patterns change, with Cheyne-Stokes breathing, noisy secretions (the death rattle), and eventual apnoeic pauses. Urine output falls, skin perfusion worsens, and consciousness narrows toward unresponsiveness. Recognising these signs lets the clinician reframe the plan from cure to comfort, to summon the family, and to start the symptom-control pathway before the distress is entrenched. Critically, the same signs can be produced by a reversible cause, and so recognition of the terminal phase is always paired with exclusion of the reversible mimics below.[1]
The goals-of-care conversation — framing, values, realistic outcomes, shared decision
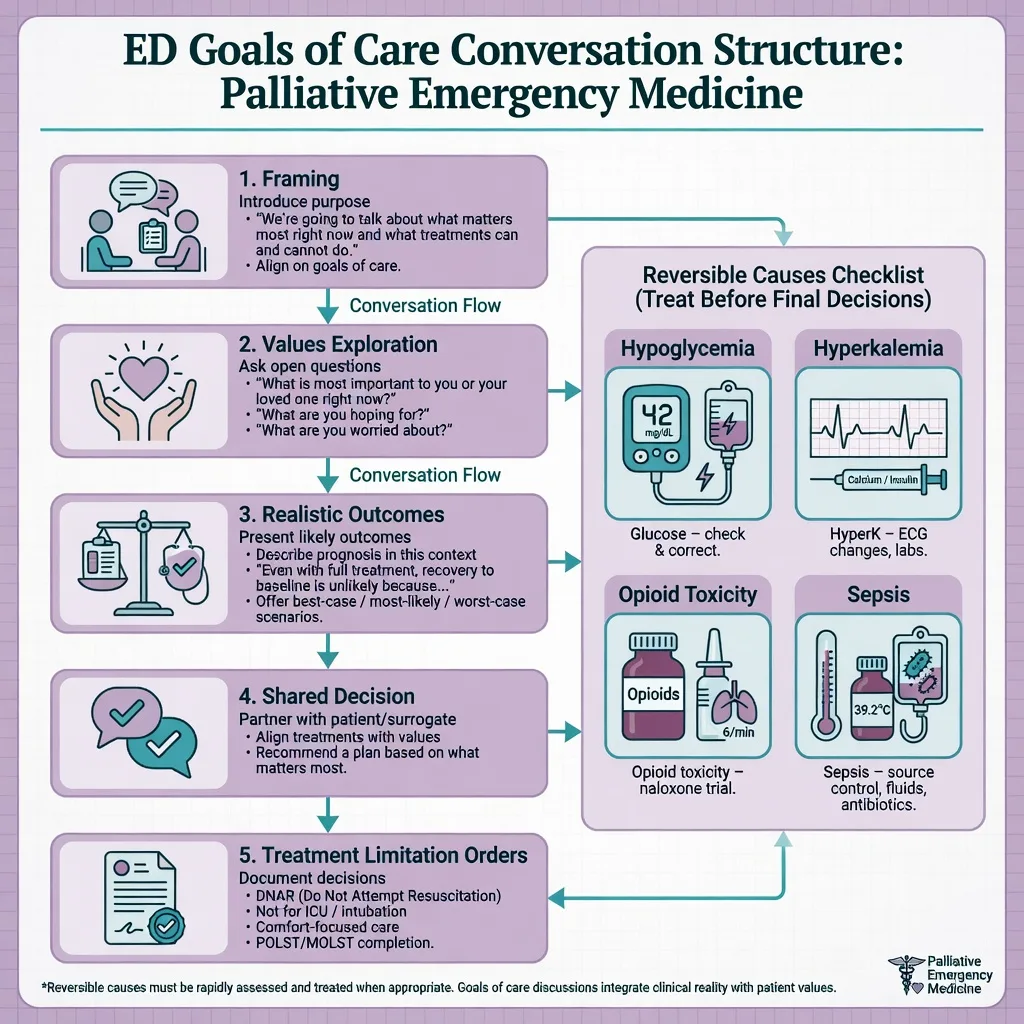
The goals-of-care conversation is the centrepiece, and it is structured. It is not a single question but a sequence — framing the conversation, exploring the patient's values and prior expressed wishes, offering a realistic prognosis, and arriving together at a shared decision. The Serious Illness Conversation Guide, evaluated in the cluster-randomised Serious Illness Care Program, is the structured prompt set that anchors the modern approach: ask what the patient understands about their illness, how much they want to know, what matters most to them, what they are hoping for and worried about, and what they would be willing and not willing to go through.[1]
Framing is the first move. The clinician names the conversation explicitly — "I would like to talk about what matters most to you, so that the care we give matches your wishes" — so the patient and family understand the purpose is alignment, not abandonment. Values are explored before numbers: "What does a good day look like for you now?" and "What would you not want to put up with?" define the outcomes that matter, and they are the raw material for every later decision. Realistic outcomes are offered honestly and without false reassurance — the clinician avoids both brutal honesty ("you will probably die today") and dishonest optimism ("everything will be fine"), instead describing the likely trajectory in plain terms: "your father's heart and kidneys are failing, and I am worried that the treatments to keep him alive would cause him suffering without giving him back the life he values." The shared decision is then made explicit — what will be done (ward-level care, symptom control, antibiotics, fluids, a trial of non-invasive ventilation, a defined period of escalation) and what will not (cardiopulmonary resuscitation, intubation, ICU, dialysis). The decision is documented, communicated to the team and the receiving unit, and revisited as the picture evolves.[1]
[1]Limitation of treatment and the not-for-resuscitation order
A goals-of-care decision crystallises into orders. The not-for-resuscitation (DNAR, or DNACPR in the United Kingdom) order is the instruction that, in the event of cardiac arrest, cardiopulmonary resuscitation will not be attempted. It is a medical order, made on the balance of clinical futility and the patient's wishes, and it does not preclude any other treatment — fluids, antibiotics, oxygen, non-invasive ventilation, ward care all continue unless separately limited. Treatment limitation extends the same logic to specific interventions: not for intubation, not for ICU, not for dialysis, not for cardiopulmonary resuscitation. Each is a deliberate, documented choice, made because the intervention cannot achieve an outcome the patient would value.[1]
The language matters and is examined. "Not for resuscitation" is reframed at the bedside as "we will focus entirely on your comfort and dignity, and we will not pursue treatments that we believe would cause harm without benefit" — never as "we will do nothing", which is both inaccurate and cruel. A comfort-focused plan is an active, intensive plan: symptom assessment and control, family presence, psychological support, environmental attention, and a named clinician. The orders are written in the record, entered in the electronic escalation system, and communicated verbally at handover, because an undocumented or ambiguous ceiling is the seed of the harmful "slow code". Where capacity is present the patient decides; where it is absent the decision is made with the substitute decision-maker under the legal framework below.[1]
Differential diagnosis — the reversible causes that must not be missed
The ethical obligation to provide comfort never relieves the diagnostic obligation to exclude a reversible cause. A patient who looks terminal may be hypoglycaemic, opioid-toxic, hyperkalaemic, or septic, and a comfort-only plan applied to a treatable condition is a catastrophic miss. The differential is therefore enumerated explicitly and excluded with targeted, proportionate tests before the plan is fixed — a glucose, a venous blood gas, an electrolyte panel, a temperature, and where indicated a bedside ultrasound or CT.[3]
Metabolic and endocrine
- Hypoglycaemia — check a bedside glucose on every drowsy or declining patient; reversible in minutes with 50 mL of 50 percent dextrose IV
- Hyperglycaemia and diabetic ketoacidosis — VBG glucose, ketones, pH; the obtunded diabetic is treatable, not dying
- Hypercalcaemia and hyperkalaemia — the arrhythmic or profoundly weak patient; an ECG and electrolyte panel exclude the lethal electrolyte disturbance
- Adrenal crisis and myxoedema coma — the hypotensive, hyponatraemic patient responds to hydrocortisone and thyroxine
Toxic and drug-related
- Opioid toxicity — pinpoint pupils, respiratory depression, reversed by naloxone titrated to respiratory rate, not full alertness
- Benzodiazepine and alcohol effects, and withdrawal states that mimic terminal agitation
- Medication accumulation in renal or hepatic failure — review the drug chart before attributing drowsiness to dying
Infective and hypoxic
- Sepsis — the febrile or hypothermic, hypotensive patient; cultures and early antibiotics can reverse apparent decline
- Hypoxia and hypercapnia from a reversible respiratory cause — pneumonia, pulmonary oedema, a blocked airway
- Hypovolaemia from haemorrhage or dehydration — responds to blood and fluid when the goal permits
Mechanical and neurological
- Cardiac tamponade, tension pneumothorax, massive pulmonary embolism — the obstructive causes of shock, reversible at the bedside or by thrombolysis
- Intracranial catastrophe — subdural or extradural haematoma, raised intracranial pressure; a CT excludes the treatable lesion
- Unrecognised pain or urinary retention causing agitation rather than true terminal restlessness
The discipline is to ask, at every goals-of-care decision, "what reversible cause have I excluded?" Only when that question is answered is a comfort-only plan ethically secure.[2]
Symptom control — the palliative drug doses (the ED palliative pathway)
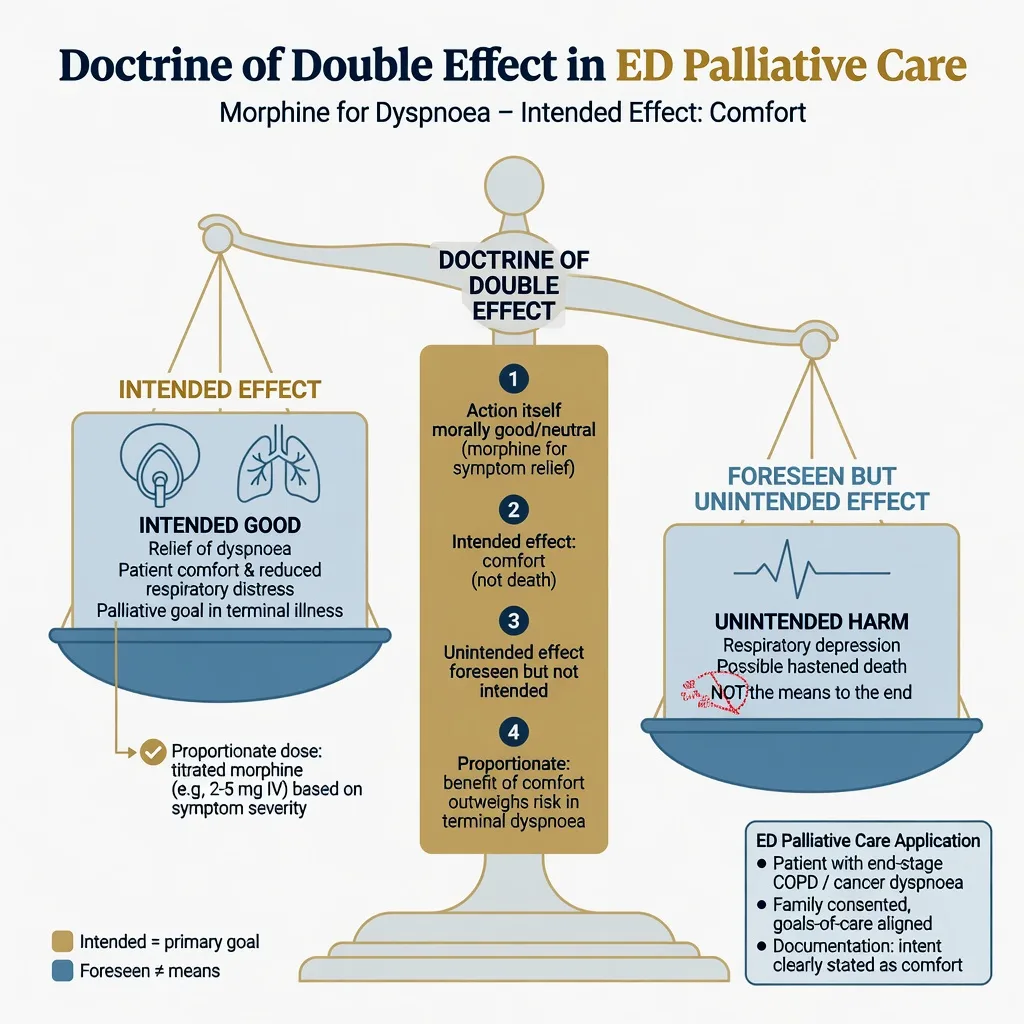
Once the goal is comfort, the ED clinician controls symptoms promptly, by a route that works, and without the fear of hastening death that paralyses the untrained prescriber. The principle is that symptom relief in the dying is ethically and legally supported under the doctrine of double effect: when the intent is comfort and the dose is proportionate to the symptom, an unintended foreseen consequence (such as respiratory depression) does not make the act wrongful, and proportionate titrated opioids do not shorten survival in the dying patient.[3][2] Four agents cover almost the entire terminal symptom burden in the ED, and each is given as a stat dose then, once need is established, placed on a syringe driver for continuous delivery.
The four symptoms of the terminal phase and their first-line drugs
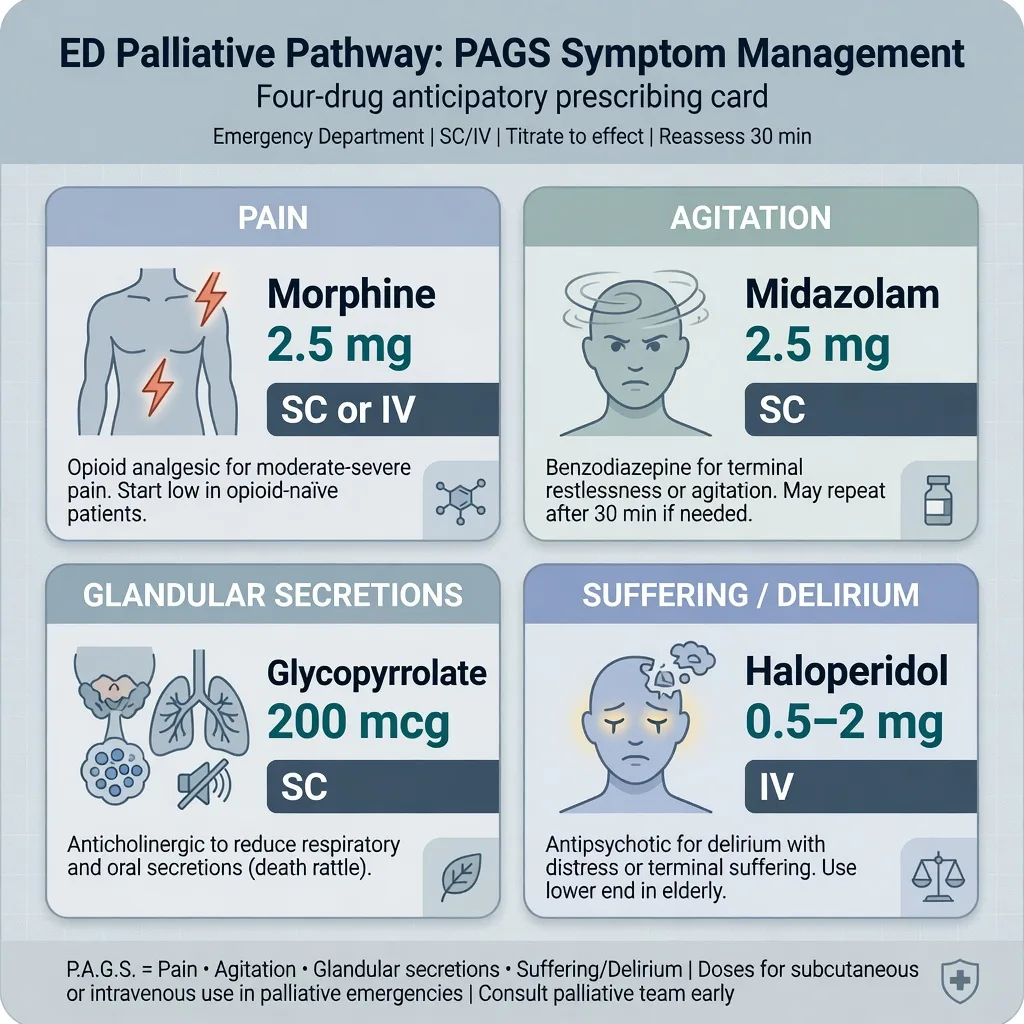
PAGS
Morphine 2.5 mg subcutaneously or intravenously, repeated and titrated to effect — first-line for pain and for the distressing dyspnoea of the failing circulation
Midazolam 2.5 mg subcutaneously, repeated and titrated — for terminal restlessness, anxiety, and the agitated delirium of hypoxia and hypoperfusion
Glycopyrrolate 200 micrograms subcutaneously — for the death rattle of respiratory secretions; suction is both ineffective and distressing and is avoided
Haloperidol 0.5 to 2 mg intravenously — for terminal delirium and agitation where a benzodiazepine alone is insufficient or where it worsens confusion
Each drug is chosen for the symptom in front of the clinician, documented with the indication, the dose, and the response, and reassessed frequently. Adjuncts extend the pathway as needed: metoclopramide 10 mg subcutaneously for nausea and gastric stasis, hyoscine butylbromide 20 mg subcutaneously for colic and as an alternative antimuscarinic for secretions, and a fan, positioning, and cool air across the face for refractory dyspnoea where oxygen has not helped. The route favours the subcutaneous space in the dying patient, because intravenous access is often lost and the subcutaneous route is reliable, painless, and suited to a syringe driver. The intent, the dose, and the response are documented at every step — this is the record that distinguishes palliative symptom control from euthanasia and that protects both the patient and the clinician.[3]
[3]The family meeting
The family meeting converts the goals-of-care decision into a shared understanding. It is held in a private room, with the door closed, phones silenced, tissues available, and the right people present — the senior clinician, the nurse caring for the patient, a named family spokesperson, and an interpreter where needed. The SPIKES structure of breaking bad news applies: a perception question ("What have the doctors told you about how serious this is?"), an invitation, a warning shot, the news in plain language, the naming of emotion with silence, and a strategy and summary. The clinician asks what the patient would have wanted, drawing on known values rather than the surrogate's own preference — this is substituted judgement, and it is the core of the meeting.[1]
The hardest dynamic is the family request for "everything". The clinician does not argue but reframes: "I want everything for your mother too — everything that will help her. I am worried that CPR and the breathing machine would cause her suffering without giving her back the life she valued. Can you tell me what she would consider a good outcome, so we make sure we are doing everything to achieve that?" This converts a conflict over interventions into a shared search for the patient's goals, and it is almost always resoluble. The agreed plan is stated in plain language, summarised in writing, and a named clinician and timeframe for follow-up are given. The meeting is never rushed, and it ends with an offer to stay or to return.[1]
Bereavement support
Bereavement begins in the ED, not after discharge. The family of a patient who dies, or who is recognised as dying, needs three things from the emergency clinician: honest information, the chance to be present, and acknowledgement of their grief. The family is offered time with the patient — before, during, and after death — and the opportunity to be present at the moment of death is offered wherever it is feasible, because the memory of that moment shapes bereavement for years. After a death, the family is offered the chance to see and touch the body, given bereavement information in their language, and connected to a named contact and to community or palliative bereavement services. The clinician normalises the grief reaction, avoids medicalising it, and is alert to complicated grief and to the rare family at risk of harm. The same support is offered to the staff — a death, particularly an unexpected or a paediatric one, affects the team, and the structured debrief is a clinical obligation, not a courtesy.[2]
Cultural and spiritual considerations
Culture and spirituality shape every layer of the encounter: who is told, who decides, how grief is shown, what language is acceptable around death, and what must happen to the body. The clinician does not assume a norm but asks. In many traditions the family, not the patient, is the legitimate recipient of serious news, and a direct disclosure against family wishes may be experienced as cruelty; the clinician negotiates by exploring the family's reason, by offering to be present, and by affirming that the patient's own autonomy remains. A trained medical interpreter — never a family member, never a child — is used whenever there is a language barrier. Rituals around the body matter: some traditions require the body to be turned, washed only by family, handled by a same-sex clinician, or buried within hours. Spiritual and pastoral care is offered and its access facilitated, and the organ-donation conversation is approached with cultural humility, decoupled from the moment of grief. The clinician who is curious, respectful, and willing to be guided will rarely go wrong.[1]
Errors and pitfalls
The recurring errors are two opposites and several around them. The first opposite is treating reversible decline as dying — applying a comfort-only plan to hypoglycaemia, opioid toxicity, hyperkalaemia, or a tamponade, and burying a treatable condition. The second is treating active dying as reversible — intubating and escalating a patient in the terminal phase of advanced disease because no one held the goals-of-care conversation, subjecting them to futile, harmful intervention. Between them sit the slow code (a resuscitation that is half-hearted because no one documented a ceiling — it is harmful, dishonest, and unacceptable), the doctrine-of-double-effect anxiety that withholds proportionate morphine from a breathless patient and leaves them to suffer, the "do nothing" framing that makes a comfort plan sound like abandonment, and the undocumented order that fails at handover. Failure to exclude reversible causes, failure to involve the substitute decision-maker, failure to use a trained interpreter, and failure to debrief the team complete the list. Each is preventable by the structure above.[3]
Regional and legal framework
The legal and ethical scaffold is region-specific in its instruments but common in its principles: capacity is presumed, autonomy is sovereign, an advance refusal of treatment is binding, and a patient who lacks capacity is decided for in their own best interests using substituted judgement. The instruments differ.[3]
ANZ practice note. An advance care directive (or Advance Health Directive in Queensland, Refusal of Treatment Certificate in Victoria) is a written statement of a person's future medical treatment preferences, and a valid directive refusing treatment is legally binding. An enduring guardian (or Medical Treatment Decision Maker in Victoria, Person Responsible in New South Wales) is the legally appointed substitute decision-maker who consents to or refuses treatment when the patient lacks capacity. Substituted judgement is the standard — the guardian decides as the patient would have decided, not as they would decide for themselves. Coronial referral is governed by each state and territory's coroners legislation, and organ donation is coordinated through DonateLife.[2]
Special populations
The paediatric end-of-life conversation demands a senior clinician, both parents where possible, honesty pitched to the developmental age, and the active involvement of the paediatric palliative service. The cognitively impaired patient is assessed for capacity at the decision in question, supported to decide where possible, and never excluded by default; the substitute decides by substituted judgement. The culturally and linguistically diverse patient is approached through a trained interpreter and with respect for family-led decision-making. The previously fit patient with a sudden catastrophic injury presents the hardest pivot — there has been no time to discuss values, and the clinician must hold uncertainty, exclude the reversible, and make a time-limited prognostic judgement before any limitation decision. The clinician-patient or colleague's relative is held to the same rigour, with the added discipline of not minimising because the conversation is uncomfortable.[1]
Evidence and regional guidelines
The Serious Illness Care Program cluster-randomised trial established that a structured conversation guide, used by non-palliative clinicians, increases the frequency and quality of goals-of-care discussions without increasing distress — it is the evidence base for the structured prompt set used at the bedside.[1] The United States Best Practice Guidelines for Primary Palliative Care in the Emergency Department codify the ED clinician's role in screening, communication, symptom control and referral, and define primary palliative care as a core emergency competence.[2] The doctrine of double effect, the ethical foundation for proportionate symptom control in the dying, has been systematically reviewed and affirms that intent and proportionality, documented at the bedside, distinguish palliative care from euthanasia.[3] Regional instruments differ in name and statute but converge on the principles of capacity, binding advance refusals, and substituted judgement.
SAQ — The goals-of-care conversation in advanced dementia with a family demand for everything
10 minutes · 10 marks
An 84-year-old woman is brought to the emergency department from a residential aged-care facility with three days of increasing drowsiness and a low-grade fever. She has advanced Alzheimer dementia (bedbound, barely speaking, requiring full nursing care for six months), stage IV ischaemic heart failure with an ejection fraction of 25 per cent, stage 4 chronic kidney disease, and recurrent aspiration events. She has been declining over the last three months. On arrival: GCS 11 (E3V3M5), RR 28, SpO2 88 per cent on room air, BP 92/58, HR 108 in atrial fibrillation, temperature 37.9 degrees C, with bilateral basal crackles and cool mottled peripheries to the knees. Her daughter, who has travelled from interstate, is distressed and demands that everything be done, including admission to intensive care and full resuscitation if she arrests. The transfer documents contain a signed advance care directive, completed two years ago when she had capacity, in which she refuses cardiopulmonary resuscitation, intubation and intensive care, and nominates her daughter as her enduring guardian. The daughter states she is now overriding the directive because her mother would not have wanted to be left to die.
SAQ — Symptom control in the terminal phase: the four-drug palliative pathway
10 minutes · 10 marks
A 72-year-old man with metastatic non-small-cell lung cancer is brought to the emergency department in the terminal phase. He is semiconscious and grimacing with each breath, respiratory rate 28 with laboured breathing and audible upper-airway secretions (the death rattle), agitated and restless, intermittently picking at the sheets. He has been treated with oral morphine at home but his oral intake has fallen over the last 48 hours. On arrival: BP 88/52, HR 124 in sinus tachycardia, SpO2 86 per cent on room air, with cool mottled peripheries, thready pulse and Cheyne-Stokes respiration. The reversible causes have been excluded — bedside glucose 5.8 mmol/L, venous gas pH 7.34, potassium 4.2 mmol/L, lactate 1.8 mmol/L, and a bedside ultrasound showing no tamponade, pneumothorax or large pulmonary embolism. He has no advance directive but his wife and son are present, agree he is dying, and a comfort-only plan has been set with the family and the oncology team.
Exam pearls
- Recognition precedes every decision — name the trajectory (sudden, cancer, organ-failure and frailty) and the terminal phase, then exclude the reversible mimics before fixing a comfort plan.
- The four stems of the goals-of-care conversation — framing, the patient's values, realistic outcomes, the shared decision — answered in that order.
- The DNAR order is reframed, never as "doing nothing": "we will focus entirely on your comfort and dignity".
- The four terminal-phase drugs — morphine 2.5 mg SC/IV for pain and breathlessness, midazolam 2.5 mg SC for agitation, glycopyrrolamine 200 micrograms SC for secretions, haloperidol 0.5 to 2 mg IV for delirium — each with indication, dose and response documented.
- The reversible differential — hypoglycaemia, opioid toxicity, hyperkalaemia, sepsis, hypoxia, tamponade, the intracranial event — excluded with a glucose, a VBG, an electrolyte panel, an ECG and bedside ultrasound before comfort care is fixed.
- The legal instruments — advance care directive (ANZ), ADRT and lasting power of attorney (UK), POLST and durable power of attorney (US) — each binding when valid, each applied by substituted judgement when capacity is lost.
- The "everything" request is reframed, not refused: "I want everything for your mother too — everything that will help her."[1]
Red flags
[3]References
- [1]Paladino J, Bernacki R, Neville BA, et al. Evaluating an Intervention to Improve Communication Between Oncology Clinicians and Patients With Life-Limiting Cancer: A Cluster Randomized Clinical Trial of the Serious Illness Care Program. JAMA Oncology, 2019.PMID 30870556
- [2]Loffredo AJ, Hogan ER, Ford DW, Lamba S, Grudzen CR. United States Best Practice Guidelines for Primary Palliative Care in the Emergency Department. Annals of Emergency Medicine, 2021.PMID 34353647
- [3]Makarem RA, Akel MA, Khatib AA, et al. The principle of double effect in palliative care: a systematic review of ethical and clinical applications. BMC Palliative Care, 2026.PMID 42185809