EM · Paracetamol poisoning
Paracetamol poisoning
Also known as Acetaminophen poisoning · Acetaminophen overdose · Paracetamol overdose · NAPQI hepatotoxicity
Paracetamol (acetaminophen) overdose — the commonest cause of acute liver failure in the developed world, and a self-poisoning that is silent in the first 24 hours. The mechanism (the CYP2E1 oxidation to NAPQI, the glutathione depletion, the zone-3 centrilobular necrosis), the time-critical Rumack-Matthew nomogram (the paracetamol level drawn at 4 hours post-ingestion), the antidote (N-acetylcysteine — 150 mg/kg over 1 hour, then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours, 300 mg/kg over 21 hours), the indications (any level above the treatment line, unknown time with a detectable level, the staggered overdose, the late presentation with hepatic injury), the King's College criteria for transplantation, and the principles of treating the established acute liver failure. ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Paracetamol poisoning is the single commonest cause of acute liver failure in the developed world and one of the few toxin exposures with a specific, highly effective antidote that is time-critical. The Fellowship candidate must understand the mechanism (the CYP2E1 oxidation to NAPQI, the glutathione depletion, the zone-3 centrilobular necrosis), the four-phase clinical course, the Rumack-Matthew nomogram and its limitations, the three-bag 21-hour intravenous N-acetylcysteine regimen, and the King's College criteria that trigger a liver-transplant referral.[1][2] The dangerous feature is the silent first 24 hours — the patient who has taken a lethal dose feels well, has normal liver function tests, and may be discharged home unless the clinician reads the level against the nomogram and treats with N-acetylcysteine.[4]
Definition and classification
Paracetamol (acetaminophen, N-acetyl-p-aminophenol) is an analgesic and antipyretic available without prescription. Acute paracetamol poisoning is the ingestion of a potentially hepatotoxic dose, defined as 150 mg/kg or 7.5 g in an adult, whichever is less, taken over a period of one hour or less. Staggered overdose (also called repeated supratherapeutic ingestion, RSI) is the ingestion of doses above the therapeutic maximum over a period longer than one hour, often over days for pain; it is more dangerous than a single acute overdose because the nomogram cannot be applied, the patient often presents late, and the clinician may underestimate the risk.[1] The clinical course is divided into four phases that frame every management decision.
Pathophysiology — NAPQI, glutathione, and the centrilobular necrosis
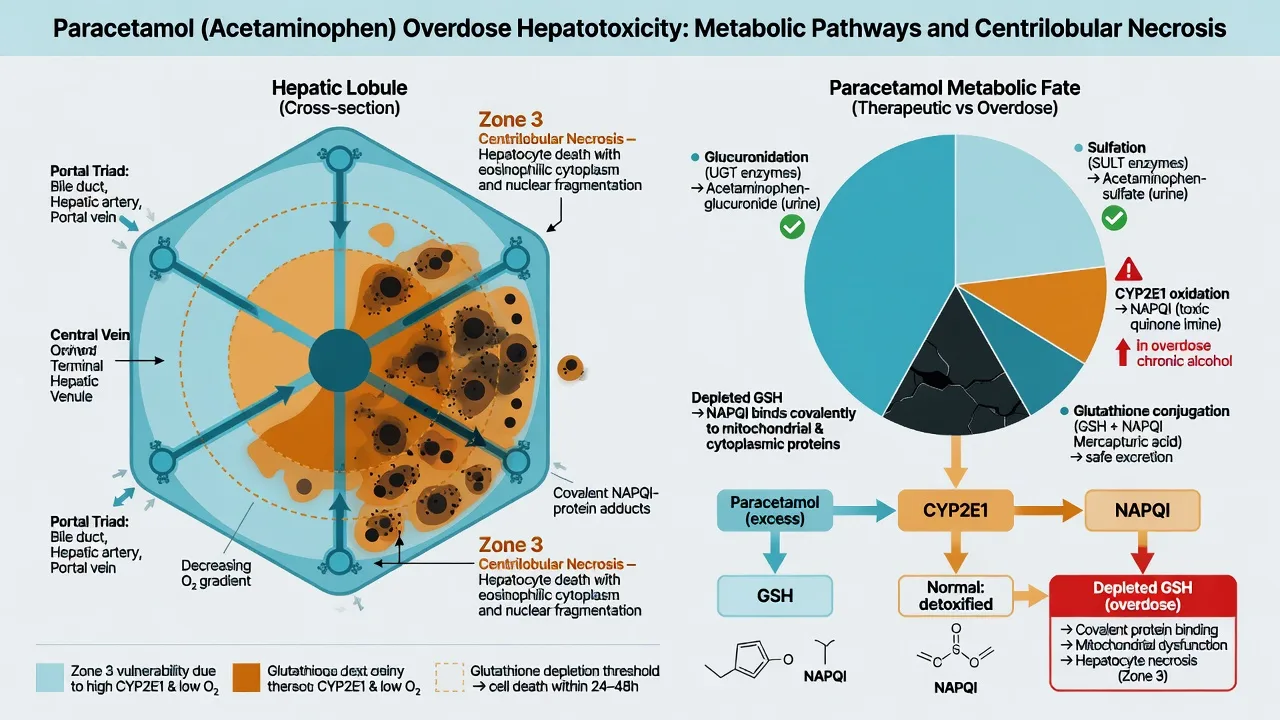
Therapeutic paracetamol is metabolised in the liver by three pathways. About 90 per cent is conjugated — 40 to 60 per cent by glucuronidation and 20 to 40 per cent by sulfation — to non-toxic, water-soluble metabolites excreted in the urine. About 2 to 5 per cent is oxidised by CYP2E1 (and a small amount by CYP1A2 and CYP3A4) to the highly reactive electrophile N-acetyl-p-benzoquinone imine (NAPQI).[1]
[10]Glutathione depletion is accelerated by anything that pre-depletes stores — fasting, malnutrition, chronic alcohol misuse, anorexia, HIV, cachexia — or that induces CYP2E1 — chronic ethanol, rifampicin, phenytoin, carbamazepine, isoniazid, St John's wort. These are the "high-risk" patients in whom some guidelines apply a lower treatment line (the UK 100 mg/L line at 4 hours, versus the standard 200 mg/L line for the lower-risk patient).[4]
Sources, epidemiology, and the rationale for pack-size restrictions
Paracetamol is the most commonly ingested drug in self-poisoning worldwide, the leading cause of acute liver failure in the United Kingdom, the United States, and Australasia, and accounts for the largest single call volume to poison information centres. The UK introduced pack-size restrictions (16 g per pack in non-pharmacy outlets, 32 g in pharmacies) in 1998, with a measurable fall in paracetamol-related death and transplant.[1] Despite this, paracetamol remains the leading toxin cause of acute liver failure, and most fatalities follow a staggered overdose or a delayed presentation rather than a large single acute ingestion.[4]
Clinical presentation — the four phases
The single acute overdose follows a stereotyped four-phase course. The Fellowship candidate must know the phases because the timing of presentation dictates what is found clinically and how the level is interpreted.[6]
The four phases of single acute paracetamol overdose
In phase 1 the patient feels well or has only nausea, vomiting, pallor and diaphoresis; liver enzymes are normal and the patient can be entirely asymptomatic despite having taken a lethal dose — this is the trap. In phase 2 the right-upper-quadrant pain appears and the ALT and INR begin to rise; an oliguria may develop. In phase 3 the patient develops the full picture of fulminant hepatic failure — jaundice, encephalopathy, coagulopathy, hypoglycaemia, metabolic acidosis and acute kidney injury. In phase 4, surviving patients recover completely without chronic liver disease, while non-survivors progress to multi-organ failure and death typically between days 3 and 5.[3]
Differential diagnosis — the cause of the transaminitis and the acute liver failure
When a patient presents with a markedly raised ALT or with acute liver failure, the differential is the cause of the hepatocyte injury; the history and the paracetamol level resolve most, but the others must be considered because the management diverges and several (the mushroom, the viral, the ischaemic) are missed by a narrow tox-focused history.[3]
Paracetamol
- History of overdose; ALT often over 1000 U/L
- Massively raised ALT with low bilirubin early
- Nomogram level above the treatment line
- N-acetylcysteine; supportive care
Amanita phalloides
- Mushroom foraging history; severe GI phase at 6–12 h
- Phase of cytopathic hepatic failure at 48–72 h
- No paracetamol level; mushroom history is key
- Silibinin, high-dose penicillin, NAC, transplant
Ischaemic hepatitis ("shock liver")
- Hypotensive episode — sepsis, arrest, haemorrhage
- ALT and LDH rise and fall within 48–72 h
- No paracetamol exposure
- Treat the underlying shock; liver recovers
Acute viral hepatitis
- Travel, IV drug use, blood exposure; prodrome
- ALT high but bilirubin high, slow evolution
- Viral serology positive (A, B, E, HSV, EBV)
- Supportive; antivirals for HBV, HSV
Drug-induced liver injury (DILI)
- Other culprits: statins, anti-epileptics, antibiotics
- Pattern mixed or cholestatic; eosinophilia may occur
- Temporal relationship to a new drug
- Withdraw the culprit; supportive
Bedside assessment
The bedside assessment of the paracetamol-overdose patient has two goals: to estimate the time of ingestion (which determines whether the nomogram can be used) and to detect complications. The history must establish the time, the dose, the formulation (immediate-release vs modified-release), the intent, and any co-ingestants. A staggered history, an unknown time, or a mixed overdose each remove the option of using the nomogram and force the clinician toward empirical N-acetylcysteine.[1] The examination documents the conscious level, the vital signs, the hydration, the presence of right-upper-quadrant tenderness, the stigmata of chronic liver disease, and any sign of hepatic encephalopathy (asterixis is the bedside marker of the early encephalopathy). A psychiatric and self-harm risk assessment is begun once the patient is medically stable.
Investigations — the 4-hour paracetamol level and the nomogram
The cornerstone investigation is the serum paracetamol level drawn at 4 hours post-ingestion. Levels drawn before 4 hours are uninterpretable because absorption and distribution are incomplete; if the patient presents after 4 hours, the level is drawn immediately on arrival.[1]
[1]The accompanying blood panel is the ALT (or AST), the INR, the creatinine, the venous blood gas (pH, lactate, bicarbonate), the glucose, the phosphate, the bilirubin, the lipase, and the beta-hCG in any woman of child-bearing age. The lactate is a marker of massive overdose: an early high lactate reflects mitochondrial NAPQI toxicity and predicts hepatotoxicity even before the transaminases rise.[5] A low phosphate (under 0.5 mmol/L) in phase 2 to 3 is a marker of depleted ATP and a poor prognosis. A salicylate level, an ethanol level, and a urine drug screen are sent if co-ingestion is suspected; the ECG rules out a co-ingested cardiotoxic agent (the widened-QRS tricyclic, the tachyarrhythmia of the salicylate).[1]
Immediate management — decontamination, the nomogram decision, and the first bag of N-acetylcysteine
The immediate management is built around three decisions: resuscitation, decontamination, and the antidote. Resuscitation follows ABCDE — most paracetamol overdoses are cardiovascularly stable, but the late-presenting patient may be in shock from hepatotoxicity, sepsis, or haemorrhage. Activated charcoal 50 g (1 g/kg in the child) orally or via nasogastric tube is given within 1 hour of ingestion (some centres extend to 2 to 4 hours for modified-release preparations) and reduces paracetamol absorption; it is most useful when the ingestion was large and within the time window.[1]
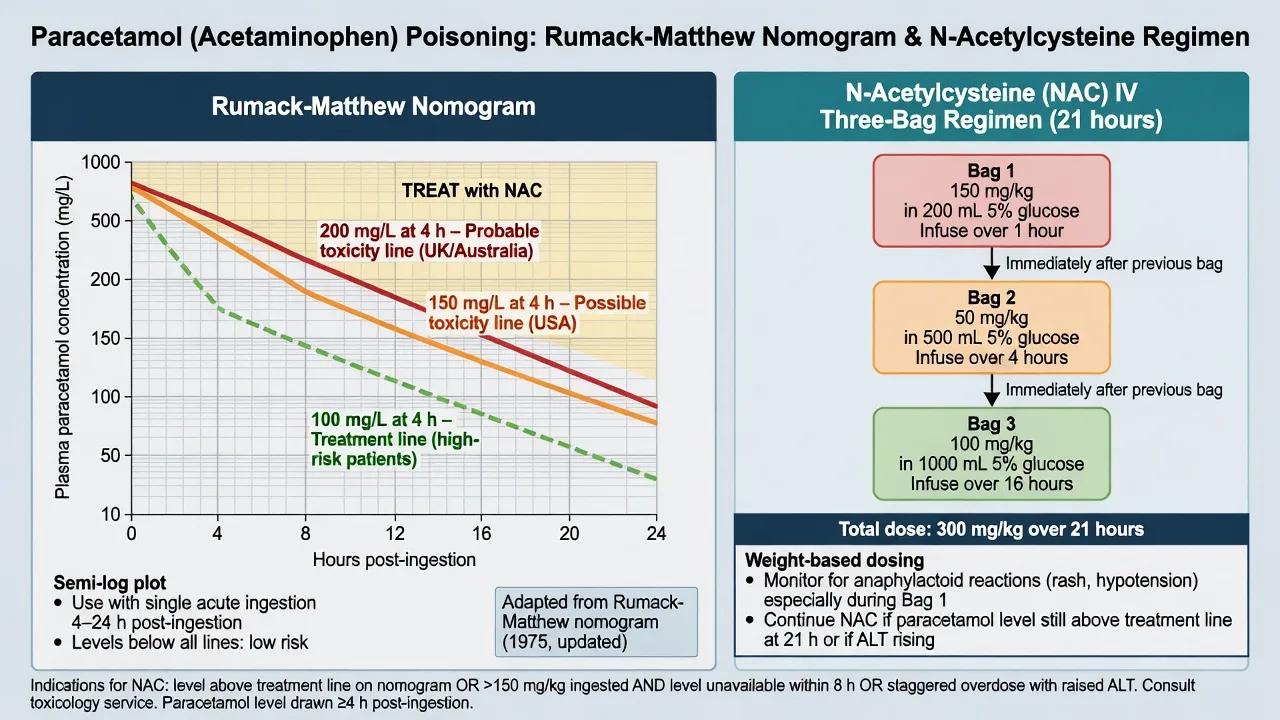
The nomogram decision follows. If the patient has taken a single acute ingestion and presents within 24 hours, a 4-hour (or later) level is plotted on the nomogram; if the level is on or above the treatment line, N-acetylcysteine is started. If the time of ingestion is unknown, the overdose was staggered, or the patient presents in or after phase 2 with hepatic injury, N-acetylcysteine is started empirically and the level is awaited.[4]
The three-bag 21-hour IV N-acetylcysteine regimen
The antidote is N-acetylcysteine (NAC), which works by replenishing hepatic glutathione and by supplying cysteine, the rate-limiting precursor for glutathione synthesis; it also acts as a free-radical scavenger and a sulphur donor, and improves tissue oxygen delivery in established hepatotoxicity. NAC is remarkably effective when given within 8 hours of ingestion — it provides virtually complete protection against hepatotoxicity — and it remains beneficial when given later, even after hepatotoxicity has developed.[2]
The standard intravenous regimen across ANZ, the UK, and North America is the three-bag 21-hour regimen: 150 mg/kg over 1 hour, then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours — a total of 300 mg/kg over 21 hours.[2] The first bag was originally given over 15 minutes (the regimen was designed for oral NAC, where the load is one large dose), but the high plasma concentration produced a non-allergic, dose-related anaphylactoid reaction (flushing, urticaria, bronchospasm) in up to 20 per cent of patients; lengthening the loading bag to 1 hour reduced this rate substantially.[2]
The oral 72-hour regimen (140 mg/kg loading, then 70 mg/kg every 4 hours for 17 doses) is an alternative where IV NAC is unavailable; it is effective but vomiting is the major practical problem and an antiemetic is routinely required. The oral route is now rarely used in the developed world.[2]
Definitive management — the escalation ladder, the modified regimen, and stopping NAC
The escalation ladder in paracetamol poisoning is short: most patients complete the 21-hour course and are discharged. The patient with a rising INR or ALT at the end of the 21-hour course, or with acute liver failure, continues NAC — either by extending the third bag at 100 mg/kg over 16 hours (the "modified" or "prolonged" regimen) or by switching to a continuous infusion at 6.7 mg/kg per hour until the INR is below 1.3, the ALT is falling, the paracetamol level is undetectable, and the encephalopathy has resolved.[3] The prognostic markers guide the duration: a falling ALT, a falling INR, an improving lactate, and a clearing paracetamol level signal recovery; a rising INR, a falling phosphate, a rising lactate, or a rising creatinine signal deterioration and the need for a transplant referral.
Subtypes and scenarios — the modified-release preparation and the staggered overdose
Two scenarios deserve special attention because the nomogram fails in each. The modified-release (sustained-release) paracetamol preparation (common in Australasia) produces a biphasic absorption with two peak serum concentrations; the recommendation is to draw two levels 4 hours apart (the first at 4 hours post-ingestion), and to start N-acetylcysteine if either level is above the treatment line.[1] The staggered overdose / repeated supratherapeutic ingestion is the more dangerous pattern: the nomogram cannot be applied because no single ingestion time exists, and these patients present later with established injury. The threshold to treat is lower — any detectable paracetamol level with a raised ALT or INR, or a substantial ingestion history alone (over 150 mg/kg or over 7.5 g in any 24-hour window) — and NAC is started empirically.[4]
Complications and pitfalls — hepatic failure, acidosis, and the anaphylactoid reaction
The complications of untreated or late-treated paracetamol overdose are the complications of fulminant hepatic failure: encephalopathy (graded I to IV), coagulopathy (the rising INR is the most sensitive marker of synthetic failure), hypoglycaemia (impaired gluconeogenesis), metabolic acidosis (the high lactate from mitochondrial failure), acute kidney injury (the same NAPQI mechanism in the proximal tubule, plus the hepatorenal physiology), and progression to multi-organ failure.[3][5]
The pitfalls are equally well described. The first is the missed 4-hour level — drawing the level too early (before absorption is complete) or too late (after 24 hours) and either over- or under-treating. The second is the misapplied nomogram — applying it to a staggered overdose, an unknown-time ingestion, or a co-ingestion that delays gastric emptying. The third is the delayed NAC — withholding NAC because the patient looks well in phase 1, when phase 1 is exactly the window in which NAC is most effective. The fourth is the anaphylactoid reaction to NAC, which is managed by slowing or pausing the infusion and giving an antihistamine (chlorphenamine 10 mg IV) — not by abandoning the antidote; the reaction is dose-rate-related and largely affects the first bag. The fifth is the false reassurance of a falling ALT in the recovery phase — the ALT falls as the hepatocytes die (no live cells to release enzyme), so a falling ALT with a rising INR is a deterioration, not an improvement.[3]
Prognosis and disposition — the King's College criteria for transplantation
The prognosis depends entirely on the timing of NAC. A patient treated within 8 hours of a single acute ingestion has a near-zero mortality; a patient presenting in phase 3 has a mortality that approaches 30 per cent without transplantation. The King's College Criteria (KCC) identify the paracetamol-induced acute liver failure patient who will not survive without a transplant; meeting KCC carries a mortality of 80 per cent or more with medical management alone and is the trigger for an urgent transplant-centre referral.[3]
The King's College criteria for transplantation in paracetamol-induced acute liver failure
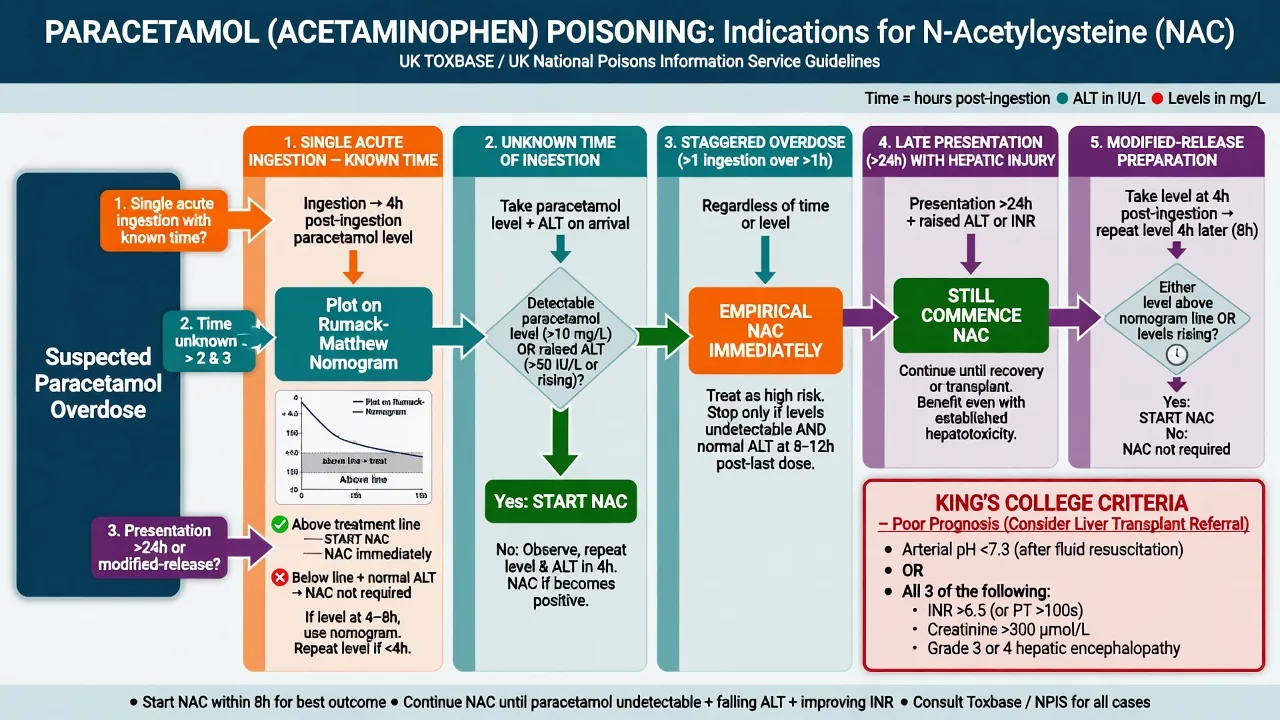
The arterial pH criterion alone (below 7.3 after fluid resuscitation) meets KCC regardless of the encephalopathy grade; the triad of INR over 6.5, creatinine over 300 micromol/L and grade III to IV encephalopathy meets KCC only when all three are present. The Bernal dynamic model (Lancet Gastroenterology & Hepatology 2016) refined the static KCC by serially tracking the lactate, the INR and the encephalopathy and predicts survival with a higher sensitivity, especially in the borderline patient; the modern transplant-centre referral uses both.[3]
The disposition is determined by the clinical phase. The phase 1 patient with a level below the treatment line is discharged (with a psychiatric assessment if the overdose was deliberate). The patient given NAC within 8 hours and recovering is discharged when the INR is normal and the ALT is falling. The patient with a rising INR, encephalopathy, or any KCC component is admitted to a high-dependency or intensive-care unit and referred to the liver transplant service.[3]
Special populations
Pregnancy is not a contraindication to NAC, which crosses the placenta and protects the fetus; the same mg/kg regimen is used, and the threshold to treat is unchanged because the maternal hepatocyte is the target. The malnourished, alcoholic, anorexic, HIV-positive, or CYP-inducing-drug patient is the "high-risk" patient in whom the lower (100 mg/L at 4 hours) treatment line is applied, because glutathione stores are depleted and NAPQI formation is induced. The paediatric patient is dosed identically by weight; liquid formulations are absorbed faster and the 4-hour level remains the reference. The late presenter (over 24 hours) with any sign of hepatic injury is treated with NAC regardless of the nomogram — the antidote works in established hepatotoxicity.[4][3]
The worked algorithm — when to give N-acetylcysteine
The single most common Fellowship error is mis-applying the nomogram to a presentation it was never designed for. The decision to treat branches on the pattern of ingestion, not on the level alone. The algorithm below collapses the UK, US, and ANZ guidance into one pathway.[1][4]
The decision to start N-acetylcysteine — five pathways
Pathway 1 — single acute ingestion, known time, presenting within 24 h
Draw a paracetamol level at 4 h post-ingestion (or immediately if the patient presents after 4 h). Plot the level on the Rumack–Matthew nomogram against the time since ingestion. **Treat with NAC if the level is on or above the treatment line** — the 200 mg/L line for the standard-risk patient, the 100 mg/L line for the high-risk patient (CYP2E1 induction or glutathione depletion). This is the only pathway in which the nomogram is valid.
Pathway 2 — unknown time of ingestion
The nomogram CANNOT be used because the x-axis (time) is unknown. **Treat empirically** if the paracetamol level is detectable (above the assay detection limit, typically >10 mg/L), OR if the ALT is above 50 U/L, OR if there is any objective sign of hepatic injury. If the level is undetectable AND the ALT and INR are normal AND more than 8 h have clearly elapsed, the patient can be observed and discharged.
Pathway 3 — staggered overdose / repeated supratherapeutic ingestion
The nomogram CANNOT be used because no single ingestion time exists. **Treat empirically** if a detectable paracetamol level is present, OR the ALT is raised, OR the ingestion exceeds 150 mg/kg or 7.5 g in any 24-hour window. The threshold to treat is deliberately low — the staggered overdose carries a higher mortality than the single acute ingestion and presents later.
Pathway 4 — late presentation (over 24 h) with established or evolving injury
The nomogram is invalid after 24 h. **Treat if the paracetamol level is still detectable, OR the ALT or INR is abnormal** (INR over 1.3, ALT above the normal range). NAC works in established hepatotoxicity — it is never "too late" to give the antidote, and survival in paracetamol-induced acute liver failure improves with NAC regardless of the time from ingestion.
Pathway 5 — modified-release (sustained-release) preparation
Biphasic absorption produces two peaks. **Draw two levels 4 h apart**, the first at 4 h post-ingestion. Start NAC if EITHER level is above the treatment line. Continue to a third level if the second is still rising — absorption can continue for many hours.
The treatment lines compared — UK, US, and ANZ
The three English-speaking guideline bodies use slightly different thresholds, and the Fellowship candidate is expected to know that the principle is identical (a 4-hour level on a log-linear treatment line) while the cut-off differs. The discrepancy reflects different philosophies of sensitivity versus NAC-anaphylactoid-reaction burden.[4]
UK (2012 CHM)
- Single treatment line for ALL patients: 100 mg/L at 4 h
- Separate 50 mg/L line for the highest-risk (rarely used)
- Lower threshold = higher sensitivity, more NAC given
- Anaphylactoid-reaction rate higher with more NAC use
US (FDA / Rumack–Matthew)
- Treatment line: 150 mg/L at 4 h (the original Rumack line)
- No separate high-risk line in the FDA labelling
- Lower NAC-utilisation rate than the UK
- Risk of under-treating the glutathione-depleted patient
ANZ (APIC network)
- Standard line: 200 mg/L at 4 h for the low-risk patient
- High-risk line: 100 mg/L at 4 h (alcohol, malnutrition, enzyme induction)
- Two levels 4 h apart for modified-release preparations
- Endorses the 21-hour three-bag regimen
Shared principle
- All lines halve every 4 h (log-linear) from the 4-hour point
- All extend from 4 h to (at most) 24 h
- All agree NAC for the staggered, unknown-time, and late presentation
- All use the 300 mg/kg / 21-hour three-bag IV regimen
Intravenous versus oral N-acetylcysteine
Both routes replenish glutathione and detoxify NAPQI; both are effective when given early. The intravenous route is the modern standard because it is reliable, faster to peak, and does not depend on the vomiting patient retaining the dose.[2][8]
IV three-bag (21 h)
- 300 mg/kg total: 150 over 1 h, 50 over 4 h, 100 over 16 h
- Reliable absorption; first-line in the developed world
- Anaphylactoid reactions in 8–20 per cent (mostly bag 1)
- Course completed in 21 h; easy to extend if the INR is rising
Oral (72 h)
- 140 mg/kg load, then 70 mg/kg every 4 h for 17 doses
- Efficacy equivalent to IV when the full course is retained
- Vomiting is the practical problem — antiemetic essential
- Course is 72 h; largely obsolete in the developed world
IV two-bag (modified)
- 200 mg/kg over 4 h, then 100 mg/kg over 16 h (Schmidt 2018)
- Lower peak concentration = fewer anaphylactoid reactions
- Emerging alternative; not yet universal
- Same total dose, simpler nursing, better tolerance
SNAP (12-hour shortened)
- Scottish and Newcastle Acetylcysteine Protocol — 100 mg/kg over 2 h then 200 mg/kg over 10 h (total 300 mg/kg in 12 h)
- Designed to cut infusion interruptions and anaphylactoid reactions versus the concentrated classic load
- Stopping rules and extension criteria are protocol-specific — check local toxicology endorsement before using as default
- Exam default remains the three-bag 21-hour regimen unless the station specifies SNAP
Choice
- IV three-bag is the global default and the exam answer
- Use oral only if IV is unavailable and retention is assured
- Modified two-bag and SNAP are evidence-supported alternatives under local policy
- Never withhold NAC for want of a route preference
Managing the anaphylactoid (non-allergic) reaction to NAC
The reaction to NAC is an anaphylactoid (non-IgE, dose-rate-related) reaction, not a true allergy — it is driven by the high peak plasma histamine concentration produced by the rapid loading bag, and it is almost always confined to the first hour of the infusion. The rate is 8 to 20 per cent with the old 15-minute load and under 5 per cent with the modern 1-hour load. The cardinal rule is: do not abandon the antidote — the reaction is manageable, the untreated hepatotoxicity is lethal.[2][11]
Managing the NAC anaphylactoid reaction — never abandon the antidote
1 — Recognise
Flushing, urticaria, pruritus in the first 30–60 min of bag 1. More severe: bronchospasm, angioedema, hypotension. Distinguish from true anaphylaxis (which is rarer and may need adrenaline) — most reactions are mild, cutaneous, and rate-related.
2 — Pause or slow the infusion
For a mild reaction (flushing, urticaria) **stop the infusion temporarily** and give an antihistamine (chlorphenamine 10 mg IV, or cetirizine). Once the rash settles (usually 15–30 min), **restart at half the rate** and titrate back up. For a moderate reaction (bronchospasm), add a bronchodilator (salbutamol nebuliser) and restart more slowly.
3 — Treat the severe reaction
Hypotension or airway compromise: **adrenaline 0.5 mg IM** (adult anaphylaxis dose), IV fluids, and senior/critical-care support. This is rare. The infusion is held but the intention is to resume once the patient is stable — a true anaphylaxis to NAC is a reason to continue under intensive-care monitoring, not to stop.
4 — Premedicate for the known reactor
For a patient with a previous reaction, premedicate with an H1-blocker (chlorphenamine 10 mg IV) ± an H2-blocker (ranitidine/famotidine) 30 min before bag 1. The modified two-bag regimen (no concentrated loading bag) reduces the rate and is an option. Document the reaction and the successful re-challenge — a prior reaction is NOT a contraindication to future NAC.
5 — Document and re-challenge
Record the reaction, its severity, and the manoeuvre that resolved it. The patient can be given NAC again in the future with premedication — the alternative (withholding the antidote) is worse than the reaction. True IgE-mediated allergy to NAC is exceedingly rare.
Single acute versus staggered overdose — the key comparison
The single acute overdose is the textbook case; the staggered overdose is the one that kills. The Fellowship candidate must contrast the two because the management, the nomogram validity, and the prognosis all diverge.[4]
Single acute
- One ingestion over <1 h; time known
- Nomogram VALID — plot the 4-hour level
- NAC within 8 h gives near-zero mortality
- Often a deliberate self-harm gesture; psychiatric overlay
Staggered / RSI
- Repeated supra-therapeutic doses over >1 h, often days
- Nomogram INVALID — no single ingestion time
- Higher mortality; presents later in phase 2–3
- Often "therapeutic misadventure" — pain, confusion, intent unclear
Modified-release
- Sustained-release formulation; biphasic absorption
- Two levels 4 h apart; treat if either above the line
- Prolonged absorption — continued monitoring
- Common in ANZ; less so in the UK and US
Co-ingestion
- Opioid, anticholinergic, or antemetic delays gastric emptying
- Nomogram may MISLEAD — absorption still ongoing at 4 h
- Draw a second level if co-ingestion suspected
- Treat the co-ingestant on its own merits
The staggered / unknown-time / late-presentation thresholds — when the nomogram cannot be used
The landmark trials
The evidence base for paracetamol-poisoning management spans five decades and is unusually complete for a toxicological topic. The Fellowship candidate should be able to name the pivotal studies behind the nomogram, the NAC regimen, and the transplant criteria.[1]
Smilkstein — oral NAC efficacy in acetaminophen overdose (NEJM 1988)
New England Journal of Medicine
PMID 3059186
Key finding
The US national multicentre study (1976–1985) of 11,195 patients treated with oral NAC, analysing hepatotoxicity (AST over 1000 U/L) against the time from ingestion to NAC. Among patients treated within 8 h, hepatotoxicity developed in only 1.6 per cent and there were no deaths; among those treated at 16 h or later, hepatotoxicity rose to 41 per cent and mortality climbed.
Practice change
Established the 8-hour window as the critical cut-off — NAC within 8 hours virtually abolishes hepatotoxicity — and validated the oral NAC regimen that preceded the IV protocol.
Smilkstein — the 48-hour IV NAC protocol (Ann Emerg Med 1991)
Annals of Emergency Medicine
PMID 1928874
Key finding
A 48-hour intravenous NAC protocol (150 mg/kg over 15 min, then 50 mg/kg over 4 h, then 100 mg/kg over 16 h, then further maintenance) in 179 patients. Efficacy matched the oral regimen with fewer dosing/vomiting problems, establishing IV NAC as a viable route. Anaphylactoid reactions were noted and concentrated in the loading dose.
Practice change
Validated intravenous NAC and laid the pharmacokinetic backbone for the modern three-bag regimen; the 15-minute load was later lengthened to 1 hour to cut the anaphylactoid rate.
Prescott — IV NAC as the treatment of choice for paracetamol poisoning (BMJ 1979)
British Medical Journal
PMID 519312
Key finding
The seminal Edinburgh series demonstrating that intravenous NAC, given early after paracetamol overdose, prevented hepatotoxicity. Prescott showed that the protective effect depended on reaching adequate hepatic cysteine/glutathione concentrations before NAPQI had bound its targets — the biological rationale for the time-critical 8-hour window.
Practice change
Established IV NAC as the treatment of choice and introduced the loading-dose concept that survives in every modern regimen.
Schmidt — modified two-bag IV acetylcysteine, fewer adverse effects (Clin Toxicol 2018)
Clinical Toxicology (Philadelphia)
PMID 29792347
Key finding
A prospective study comparing a modified two-bag protocol (200 mg/kg over 4 h then 100 mg/kg over 16 h — eliminating the concentrated loading bag) against the standard three-bag regimen. The two-bag protocol produced a significantly lower rate of anaphylactoid reactions (cutaneous, bronchospastic) with equivalent NAC exposure.
Practice change
Provides the evidence for lengthening/dissolving the loading bag to minimise the dose-rate-related anaphylactoid reaction — the pharmacokinetic rationale behind the modern 1-hour load.
O'Grady — the King's College Criteria for fulminant hepatic failure (Gastroenterology 1989)
Gastroenterology
PMID 2490426
Key finding
The King's College Hospital derivation cohort of patients with fulminant hepatic failure (including paracetamol-induced) that established the static prognostic criteria: for paracetamol-induced ALF, arterial pH below 7.3 alone, OR all three of INR over 6.5, creatinine over 300 micromol/L, and grade III–IV encephalopathy. Patients meeting KCC had a mortality above 80 per cent with medical management alone.
Practice change
Defined the criteria that still trigger the urgent liver-transplant referral; the original benchmark against which the later dynamic (Bernal) models are judged.
Bernal — blood lactate as an early predictor in paracetamol ALF (Lancet 2002)
Lancet
PMID 11867109
Key finding
A cohort of patients with paracetamol-induced acute liver failure at King's College, showing that an early arterial lactate (above 3.5 mmol/L after fluid resuscitation) — measured before the INR or encephalopathy had peaked — independently predicted non-survival and improved on the static King's College criteria. A combined lactate-plus-KCC model raised sensitivity for death without sacrificing specificity.
Practice change
Established lactate as an early, dynamic prognostic marker that is now incorporated into the modern transplant-referral algorithm alongside the King's College pH criterion.
Memory aids — the mechanism and the transplant criteria
The King's College Criteria for paracetamol-induced acute liver failure
KING
Arterial pH below 7.3 after adequate fluid resuscitation — this single criterion ALONE meets KCC, regardless of the encephalopathy grade
Prothrombin time over 100 s / INR over 6.5 — the first limb of the triad (all three must be present together)
Serum creatinine above 300 micromol/L — the second limb of the triad, reflecting the hepatorenal / NAPQI tubular injury
Grade III–IV hepatic encephalopathy — the third limb; only when INR + creatinine + encephalopathy are ALL present does the triad meet KCC
The pathophysiology in five steps — the mechanism of the centrilobular necrosis
NAPQI
The toxic electrophile: N-acetyl-p-benzoquinone imine, formed by CYP2E1 oxidation of paracetamol when glucuronidation and sulfation saturate
NAPQI binds covalently to cysteine residues on hepatocyte proteins (the mitochondrial and cytosolic targets), producing cellular dysfunction
Centrilobular (zone 3) necrosis — the region of highest CYP2E1 activity, lowest oxygen tension, and most dependent blood supply
At therapeutic dose NAPQI is detoxified by conjugation with glutathione; when glutathione falls below 30 per cent of normal, NAPQI accumulates
CYP2E1 inducers (ethanol, isoniazid, rifampicin, phenytoin) and glutathione depleters (fasting, malnutrition, alcohol, HIV) make the high-risk patient — use the lower treatment line
Evidence and regional guidelines
The evidence base and the regional practice are well aligned across the Anglosphere. The UK national guideline (the 2012 revision published by the Commission on Human Medicines, audited by Bateman in 2014) introduced the single 100 mg/L "treatment line" for all patients (with a separate 50 mg/L line rarely used for the highest-risk) and lowered the threshold for NAC, which increased NAC use without increasing jaundice or transplant admissions.[4] The US guideline (the American College of Emergency Physicians and the FDA-approved labelling) uses the Rumack-Matthew 150 mg/L line. The Australian and New Zealand guideline (the ANZ position statements from the Australasian Poisons Information Centre network) endorses the 21-hour three-bag regimen, applies the lower treatment line in the high-risk patient, and recommends two levels 4 hours apart for the modified-release preparation.[1][2] The three-bag 21-hour regimen itself (150 mg/kg over 1 hour, 50 mg/kg over 4 hours, 100 mg/kg over 16 hours) is the modern global standard, having replaced the older 20.25-hour regimen that delivered the loading bag over 15 minutes; the change to the 1-hour load reduced the anaphylactoid rate without compromising efficacy.[2]
ANZ practice note. The ANZ approach follows the modified-release-aware framework: a 4-hour level on the Rumack-Matthew nomogram, with a second level drawn 4 hours later for any modified-release ingestion; the standard 21-hour three-bag N-acetylcysteine regimen (150 mg/kg over 1 hour, 50 mg/kg over 4 hours, 100 mg/kg over 16 hours); empirical NAC for the staggered overdose or unknown-time ingestion; and a low threshold for the high-risk line in the alcoholic, malnourished, or enzyme-induced patient. The King's College criteria drive the transplant referral. Activated charcoal 50 g is offered within 1 to 2 hours of an acute ingestion.[7]
Exam practice
SAQ — Staggered paracetamol overdose with established hepatotoxicity
12 minutes · 10 marks
A 27-year-old woman is brought to the emergency department 22 hours after a staggered ingestion of approximately 40 tablets of 500 mg paracetamol (20 g) taken over six hours. She is vomiting, has right-upper-quadrant pain and is increasingly confused. T 36.9, HR 108, BP 104/64. ALT 2840 U/L, INR 4.8, creatinine 176 micromol/L, bilirubin 95 micromol/L, venous pH 7.29, lactate 4.1 mmol/L, phosphate 0.42 mmol/L. Paracetamol level 90 mg/L.
SAQ — Massive single paracetamol ingestion with early lactate rise
10 minutes · 10 marks
A 19-year-old man presents 90 minutes after ingesting 50 g of paracetamol in a single dose. He is alert and vomiting. T 37.1, HR 96, BP 118/72. The 4-hour paracetamol level is 420 mg/L. ALT 32 U/L, INR 1.0, lactate 5.2 mmol/L, pH 7.36.
Exam pearls
- The mechanism: paracetamol → CYP2E1 → NAPQI → glutathione depletion → centrilobular (zone 3) necrosis. Glutathione under 30 per cent is the tipping point.
- The 21-hour three-bag regimen: 150 mg/kg over 1 hour, then 50 mg/kg over 4 hours, then 100 mg/kg over 16 hours — total 300 mg/kg over 21 hours.
- The level is drawn at 4 hours post-ingestion (or as soon as possible if the presentation is later); never before 4 hours.
- The indications for NAC: any level above the treatment line, OR the unknown-time ingestion with a detectable level, OR the staggered overdose, OR the late presentation with hepatic injury.
- NAC works at any time — give it even in established hepatotoxicity; it improves survival in paracetamol-induced acute liver failure.
- The anaphylactoid reaction to the first bag is dose-rate-related: slow the infusion and give chlorphenamine; do not abandon the antidote.
- The King's College criteria: arterial pH below 7.3 alone, OR all three of INR over 6.5, creatinine over 300 micromol/L, grade 3 to 4 encephalopathy — refer for transplant.
- The high lactate and the low phosphate are markers of poor prognosis.
- A falling ALT with a rising INR is deterioration (the hepatocytes have all died) — not recovery.
- The staggered or unknown-time overdose: treat if the level is detectable, the ALT is over 50, the INR is over 1.3, or the dose exceeds 150 mg/kg or 7.5 g — the nomogram is never used.
- The five pathways to NAC: single-acute-above-line; unknown-time-detectable; staggered; late-with-injury; modified-release-two-levels.
- NAC works at any time — it improves survival in established paracetamol ALF by glutathione repletion, sulphur donation, and free-radical scavenging, not only NAPQI neutralisation.
- The four prognostic bloods: rising INR, rising lactate (over 3.5), falling phosphate (under 0.5), arterial pH under 7.3 — track the trend, not the single value.
- The anaphylactoid reaction is dose-rate-related and confined to bag 1: slow/stop the infusion, give chlorphenamine, restart at half rate — never abandon the antidote.
- The lactate is the earliest prognostic marker in massive overdose — it rises from mitochondrial NAPQI toxicity before the transaminases move.
- Co-ingest an opioid/anticholinergic and the nomogram can mislead — delayed gastric emptying keeps absorption going past 4 hours; send salicylate, ethanol, and a urine drug screen.
- NAC in obesity: dose per actual body weight but cap the bag weight (commonly 100–110 kg) per local policy — never under-dose the obese patient.[10]
Model answer — A 24-year-old woman, 20 g of paracetamol 6 hours ago, ALT 45 U/L, INR 1.1, paracetamol level 180 mg/L. Outline the immediate management.
Immediate management. The presentation is a single acute ingestion at a known time, so the paracetamol level can be plotted on the Rumack-Matthew nomogram. At 6 hours post-ingestion the treatment line crosses approximately 80 mg/L (it halves every 4 hours from 200 mg/L at 4 hours); a level of 180 mg/L is well above the line. The indication for N-acetylcysteine is met. The first step is the first bag of the 21-hour three-bag regimen — 150 mg/kg over 1 hour — commenced immediately, followed by 50 mg/kg over 4 hours and 100 mg/kg over 16 hours, total 300 mg/kg over 21 hours. A baseline set of bloods is sent: ALT, INR, creatinine, venous gas (pH, lactate), glucose, phosphate, beta-hCG, and a salicylate and ethanol level for any co-ingestion. Activated charcoal 50 g is offered (within the 1- to 2-hour window it is well past, so it is not given here). The patient is observed for the anaphylactoid reaction in the first hour; if it occurs, the infusion is slowed and chlorphenamine 10 mg IV given, the antidote is not stopped. The INR and ALT are checked at the end of the 21-hour course: if normal or falling, NAC is stopped; if the INR is rising or above 2.0, the third bag is continued. A psychiatric and self-harm risk assessment is performed once the patient is medically stable. The expected outcome with NAC within 8 hours is complete recovery.[10]
SAQs
SAQ — Acute paracetamol overdose and N-acetylcysteine
10 minutes · 10 marks
A 23-year-old woman (62 kg) is brought to the ED 5 hours after taking 25 g of immediate-release paracetamol in a deliberate self-harm gesture. She is nauseated but otherwise asymptomatic. Blood pressure 118/72, pulse 88, GCS 15, abdomen soft. A paracetamol level drawn on arrival returns at 220 mg/L. ALT 34 U/L, INR 1.0, creatinine 76 micromol/L, venous lactate 1.8 mmol/L, glucose 5.2 mmol/L. Beta-hCG negative.
SAQ — Staggered paracetamol overdose
10 minutes · 10 marks
A 58-year-old man with chronic back pain and daily alcohol use (60 g/day) presents with 3 days of right-upper-quadrant pain, nausea and confusion. He has been taking 8-10 g of paracetamol per day for the past 4 days for worsening pain. On examination he is jaundiced, flapping tremor present, GCS 13. ALT 4,800 U/L, INR 4.2, creatinine 210 micromol/L, arterial pH 7.32, lactate 4.1 mmol/L, phosphate 0.4 mmol/L, paracetamol level 65 mg/L. Time of last dose uncertain.
Red flags
[10]References
- [1]Bateman DN, Dart RC, Dear JW, et al. Fifty years of paracetamol (acetaminophen) poisoning: the development of risk assessment and treatment 1973-2023 with particular focus on contributions published from Edinburgh and Denver. Clinical toxicology (Philadelphia, Pa.), 2023.PMID 38197864
- [2]Bateman DN, Dear JW, Carroll R, et al. New regimens for intravenous acetylcysteine, where are we now? Clinical Toxicology (Philadelphia), 2016.PMID 26666290
- [3]Bernal W, Lee WM, Wendon J, Larsen FS, Williams R. Development and validation of a dynamic outcome prediction model for paracetamol-induced acute liver failure: a cohort study. Lancet Gastroenterology & Hepatology, 2016.PMID 28404094
- [4]Bateman DN, Carroll R, Pettie J, et al. Effect of the UK's revised paracetamol poisoning management guidelines on admissions, adverse reactions and costs of treatment. British journal of clinical pharmacology, 2014.PMID 24666324
- [5]Shah AD, Wood DM, Dargan PI. Understanding lactic acidosis in paracetamol (acetaminophen) poisoning. British Journal of Clinical Pharmacology, 2011.PMID 21143497
- [6]Smilkstein MJ, Knapp GL, Kulig KW, Rumack BH. Efficacy of oral N-acetylcysteine in the treatment of acetaminophen overdose. Analysis of the national multicenter study (1976 to 1985). New England Journal of Medicine, 1988.PMID 3059186
- [7]Smilkstein MJ, Bronstein AC, Linden C, Augenstein WL, Kulig KW, Rumack BH. Acetaminophen overdose: a 48-hour intravenous N-acetylcysteine treatment protocol. Annals of Emergency Medicine, 1991.PMID 1928874
- [8]Prescott LF, Illingworth RN, Critchley JA, Stewart MJ, Adam RD, Proudfoot AT. Intravenous N-acetylcystine: the treatment of choice for paracetamol poisoning. British Medical Journal, 1979.PMID 519312
- [9]O'Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology, 1989.PMID 2490426
- [10]Bernal W, Donaldson N, Wyncoll D, Wendon J. Blood lactate as an early predictor of outcome in paracetamol-induced acute liver failure: a cohort study. Lancet, 2002.PMID 11867109
- [11]Schmidt LE, Rasmussen DN, Petersen TS, et al. Fewer adverse effects associated with a modified two-bag intravenous acetylcysteine protocol. Clinical Toxicology (Philadelphia), 2018.PMID 29792347