EM · Post-cardiac arrest care
Post-cardiac-arrest care
The post-ROSC bundle that determines neurological survival: the oxygen and the carbon-dioxide targets, the circulation and the reperfusion, the targeted-temperature evidence (TTM2: normothermia over hypothermia), the seizure and glucose control, the identification and treatment of the cause, the avoidance of the secondary brain injuries, and the multimodal deferred prognostication.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
The return of spontaneous circulation is the end of the arrest and the beginning of the post-arrest care, and the post-arrest care is what determines whether the survivor wakes neurologically intact. The resuscitated patient is, in effect, a patient with an injured brain in a recovering circulation, and the goal of the hours that follow is to optimise the oxygen delivery, to protect the brain from secondary injury, and to identify and treat the cause. The Fellowship-level understanding rests on the post-ROSC bundle — the targets for oxygen, ventilation, circulation, temperature, glucose and seizures — and on the evidence that has refined it, above all the targeted-temperature trials.[3]

The principle and the post-ROSC bundle
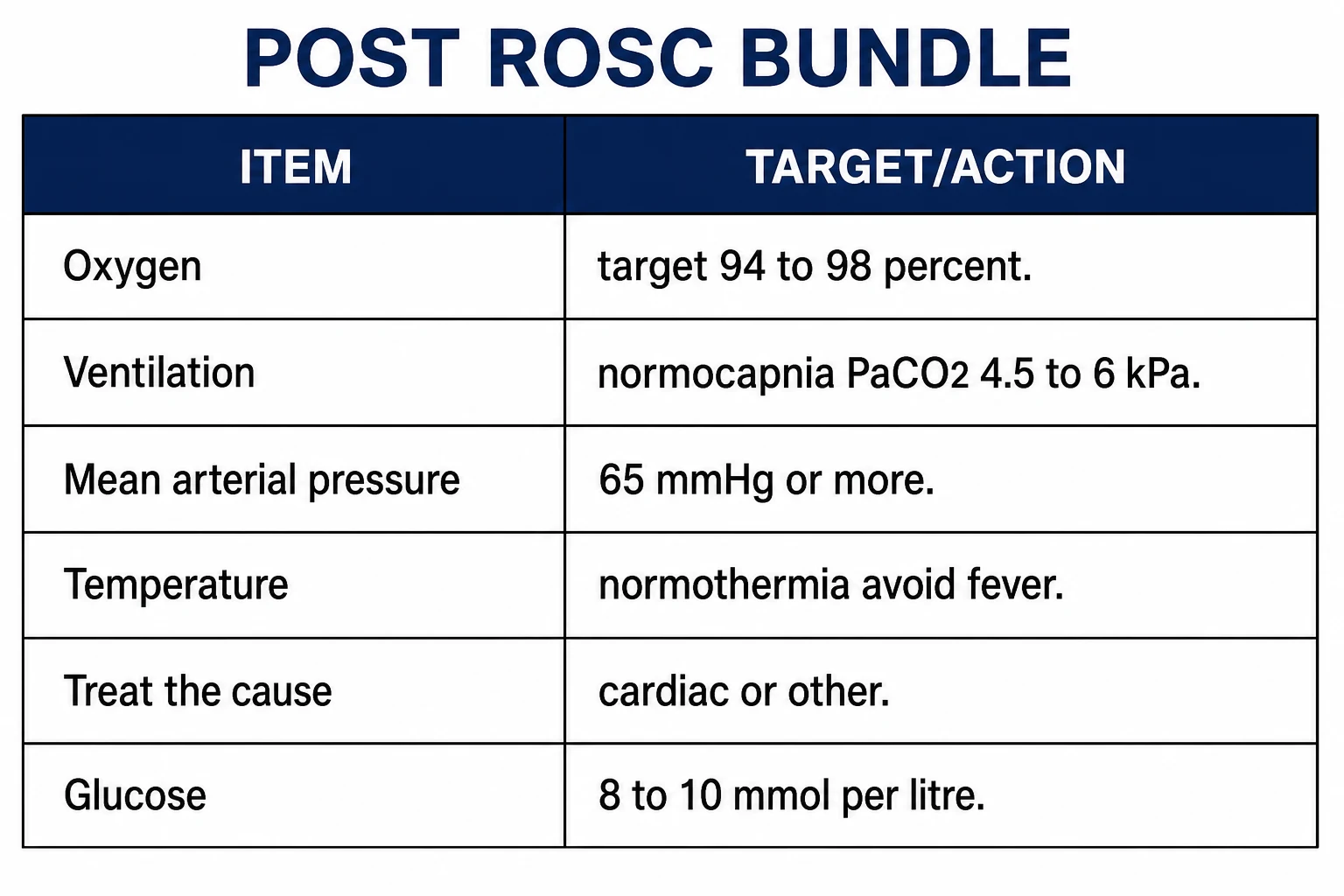
The injured brain after cardiac arrest is exquisitely vulnerable to a second insult, and the post-ROSC bundle is a set of targets designed to prevent one. The patient is managed in a critical-care environment, intubated and ventilated, sedated and monitored. The bundle, applied from the moment of ROSC, comprises the oxygen and the carbon-dioxide targets, a mean arterial pressure that supports the cerebral and the coronary perfusion, the control of the temperature and the seizures, the control of the glucose, and the identification and the treatment of the cause.[2][4]
Airway, breathing and the oxygen target
Both extremes of oxygen are harmful: the hypoxia causes a secondary brain injury and the hyperoxia generates free radicals and causes absorption atelectasis and vasoconstriction. The patient is ventilated to an oxygen saturation target of 94 to 98 per cent, titrating the fraction of inspired oxygen down from 100 per cent as soon as the saturation permits. The EXACT trial, comparing a restrictive against a liberal oxygen strategy in the comatose survivor, found that the restrictive strategy was not superior, and the contemporary practice is the avoidance of both hypoxia and hyperoxia with a normoxic target rather than an aggressive drive to the lowest fraction.[3]
Ventilation and the carbon-dioxide target
The carbon dioxide is the principal regulator of the cerebral vascular tone: a low carbon dioxide constricts the cerebral vessels and reduces the cerebral blood flow, and a high carbon dioxide raises the intracranial pressure. The patient is ventilated to normocapnia — a PaCO2 in the normal range, 4.5 to 6.0 kPa (35 to 45 mmHg) — and hyperventilation, which produces a hypocapnia and a cerebral ischaemia, is avoided. The protective reflex of the CO2-reactive cerebral vasculature is one of the reasons the ventilation is controlled and monitored with the blood gas, and the aggressive hyperventilation that was once practised for the presumed neuroprotection is no longer recommended.[3]
Circulation and reperfusion
The mean arterial pressure is supported to 65 mmHg or more (higher in the chronically hypertensive), with fluid, vasopressors and inotropes as needed, to maintain the cerebral and the coronary perfusion. The hypotension in the hours after ROSC is associated with a worse neurological outcome, and it is actively treated. The cause of the arrest is investigated and treated: a 12-lead electrocardiogram (once the patient is stable) screens for the ST-elevation myocardial infarction, the bedside echocardiography assesses the contractility and excludes a tamponade or a pulmonary embolism, and the patient with a presumed cardiac cause is referred for the urgent coronary angiography and the percutaneous intervention, which improves the outcome.[1]
Targeted temperature management: the evidence
The temperature management has been the most contested and the most refined element of the bundle, and the candidate is expected to know the evolution. The early trials (the Hypothermia After Cardiac Arrest and the Bernard trials, in 2002) found that cooling to 32 to 34 degrees after a witnessed VF arrest improved the neurological outcome, and the practice of therapeutic hypothermia was adopted. The 2013 TTM trial found no difference between targeting 33 and 36 degrees, narrowing the target. The TTM2 trial, in 2021, found that targeting hypothermia at 33 degrees did not improve the outcome over normothermia, and was associated with more arrhythmia.[1] The contemporary practice, codified by the guidelines, is to maintain normothermia — a core temperature around 37 degrees — and to actively treat fever (the temperature kept below 37.5 to 37.7), for at least 72 hours.[2] The targeted hypothermia at 33 degrees is no longer recommended as a routine.
Seizures, glucose and metabolism
Seizures are common after cardiac arrest and they worsen the secondary brain injury, so they are detected (with the continuous electroencephalogram in the comatose patient) and treated (with a levetiracetam, a sodium-channel agent or a propofol infusion). The glucose is controlled to a moderate range — 8 to 10 mmol per litre — with the avoidance of both the hypoglycaemia (which injures the brain) and the tight control (which the critical-care evidence found to be harmful through the hypoglycaemic episodes). The electrolytes, the haemoglobin and the perfusion are maintained, and the patient is nursed with the head elevated and the normovolaemia preserved.[3]
Neuroprotection: avoiding the secondary injuries
The unifying principle of the post-arrest care is the prevention of the secondary brain injury, and every element of the bundle contributes to it.[2]
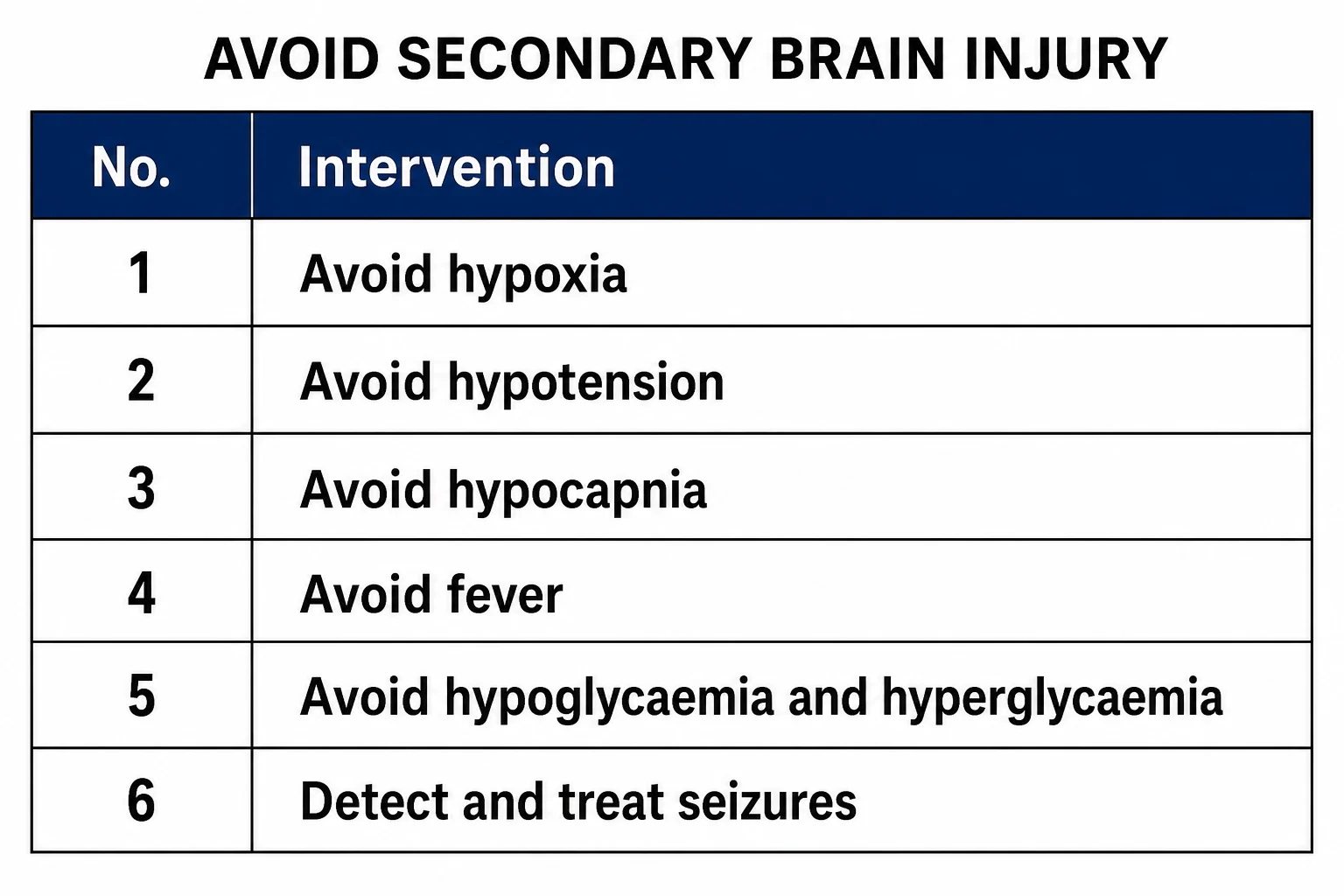
The hypoxia and the hyperoxia, the hypotension, the hypocapnia, the fever, the glucose extremes and the untreated seizure each compound the primary anoxic injury, and the disciplined maintenance of the normoxia, the normocapnia, the perfusion, the normothermia, the moderate glucose and the seizure control is the practical expression of the neuroprotection.[1]
Differential diagnosis
The Fellowship-level differential of the post-arrest patient is the cause of the arrest itself, because the uncorrected cause — an occluded coronary, a massive embolism, a catastrophic bleed — defeats the post-ROSC bundle however meticulously it is applied. The framework is the four Hs and four Ts, but the causes are distinguished at the bedside by the rhythm, the history and the focused workup.[1]
- Cardiac (coronary) cause — the commonest cause in the shockable rhythm: an ST-elevation myocardial infarction or an ischaemia-driven ventricular fibrillation. Distinguished by the 12-lead ECG (the ST elevation, a new conduction block), the wall-motion abnormality on the bedside echocardiography, and confirmed at the urgent coronary angiography.
- Pulmonary embolism — a massive embolism presenting with a pulseless electrical activity or a refractory ventricular fibrillation. Distinguished by a high-risk setting (immobility, malignancy, recent surgery), a preload-dependent echocardiogram with a dilated right ventricle, and treated with the systemic thrombolysis.
- Hypoxia and asphyxia — the drowning, the airway obstruction, the asthma, the opiate or the respiratory failure. Distinguished by a non-shockable initial rhythm, an evident environmental or toxicological cause, and a hypoxaemic arrest that responds to the oxygenation.
- Hypovolaemia and haemorrhage — a massive gastrointestinal, aortic or traumatic bleed. Distinguished by the signs of the volume depletion, a pulseless electrical activity, a falling haemoglobin and a positive FAST scan.
- Tension pneumothorax and tamponade — the obstructive causes. Distinguished by the clinical signs (the unilateral breath sounds and the tracheal deviation; the distended neck veins and the muffled heart sounds) and the bedside ultrasound, with the immediate needle decompression or pericardiocentesis.
- Toxin and electrolyte — the drug overdose (a tricyclic antidepressant, a sodium-channel blocker, a beta-blocker) and the hyperkalaemia or the hypokalaemia. Distinguished by the history, the widening QRS or the peaked T waves on the ECG, and the point-of-care biochemistry.[1]
Identifying and treating the cause
The cause of the arrest is sought and treated in parallel with the bundle, because the uncorrected cause — an occluded coronary artery, a massive pulmonary embolism, a catastrophic haemorrhage, a toxin — will defeat the post-arrest care. The cardiac cause is the commonest in the shockable arrest, and the urgent coronary angiography with the percutaneous intervention for the occluded artery is part of the bundle. The pulmonary embolism is treated with the anticoagulation or the thrombolysis, the haemorrhage with the blood and the source control, the toxin with the antidote.[2]
Management: the post-ROSC drug doses
The post-arrest patient often needs pharmacological support while the cause is identified and the bundle is applied, and the Fellowship candidate is expected to know the agents and their doses. The vasopressors, the inotropes, the anticonvulsants and the anti-arrhythmics are the core of the post-ROSC pharmacology.[2][4]
- Noradrenaline 0.05 to 0.5 mcg/kg/min intravenously — the first-line vasopressor, titrated to a mean arterial pressure of 65 mmHg or more; it is the preferred agent for the vasodilatory shock after ROSC.
- Adrenaline 0.05 to 0.5 mcg/kg/min intravenously — the alternative vasopressor and inotrope, used when noradrenaline is unavailable or a combined inotropic effect is needed.
- Dobutamine 2 to 20 mcg/kg/min intravenously — the inotrope for the low-cardiac-output state from a stunned myocardium or a cardiomyopathy, often started alongside the vasopressor.
- Levetiracetam 60 mg/kg intravenously (to a maximum of 4500 mg) — the first-line anticonvulsant for the post-arrest seizure, with a propofol or a midazolam infusion for the refractory or the status epilepticus.
- Amiodarone 300 mg intravenously — for the recurrent ventricular fibrillation or the pulseless ventricular tachycardia in the early post-ROSC period, with a further 150 mg if it recurs, followed by an infusion of 900 mg over 24 hours.
- Aspirin 300 mg orally (or per rectum) — once an acute coronary syndrome is identified and the airway is protected, alongside the second antiplatelet and the anticoagulation for the angiography.
- Morphine 5 mg intravenously, titrated — the analgesic and anxiolytic for the intubated and sedated patient, given with a benzodiazepine and a propofol infusion for the sedation.[2]
Prognostication
The neurological prognostication is multimodal and deferred, performed at 72 hours or more after the ROSC, and ideally after the sedation has been off for long enough to assess. The ERC/ESICM algorithm integrates the clinical examination (the brainstem reflexes, the motor response, the presence of the myoclonus), the electrophysiology (the continuous or the standard EEG, and the somatosensory evoked potentials), the biomarkers (the neuron-specific enolase), and the imaging (the cerebral computed tomography or the magnetic resonance).[2] No single predictor is sufficient, and the early pessimistic prediction — made on the clinical examination alone in the first day, under sedation — is famously unreliable and often wrong. The prognostication is made by a team, at the right time, with the right tests, and the self-fulfilling prophecy of the prematurely withdrawn care is the pitfall the candidate must avoid.
Organ donation and regional practice
The patient who does not recover neurological function, or who meets the criteria for the neurological death, is considered for the organ donation — a decision made with the family and the donation service, and one in which the emergency and the critical-care teams have an essential early role. The guidelines are regional: the ERC/ESICM guidelines and the ILCOR consensus integrate the global evidence, and the ARC/NZRC guidelines govern the Australasian practice; the bundle is the same in outline.[2][4][5]
The post-ROSC targets — the one-glance card
The post-ROSC bundle targets
The post-ROSC first 60 minutes
The first hour after the return of spontaneous circulation is when the secondary brain injuries are acquired or prevented. The disciplined application of the bundle in this window — not the intensive-care day that follows — is the single biggest modifiable determinant of the neurological outcome. The emergency physician owns this hour.[2]
The post-ROSC first 60 minutes — the ED protocol
Confirm the ROSC: a palpable pulse, a rising end-tidal CO₂, and a measurable blood pressure. Do NOT resume compressions for a weak pulse.
Optimise the oxygenation: titrate the FiO₂ down from 100% to the lowest concentration that holds the SpO₂ at 94 to 98%. Leave the patient on 100% only if the saturation is marginal.
Set the ventilator: a tidal volume of 6 to 8 mL/kg ideal body weight, a rate of 10 to 12, and the FiO₂ titrated. Target a PaCO₂ of 35 to 45 mmHg (4.5 to 6.0 kPa) — send the arterial blood gas at 15 to 20 minutes.
Support the circulation: aim for a MAP of 65 mmHg or more from the outset. Start the noradrenaline early — do not tolerate a "permissive" hypotension. A fluid bolus of 250 to 500 mL if hypovolaemic, then the vasopressor.
Obtain the 12-lead ECG as soon as the patient is stable; if there is an ST-elevation myocardial infarction, activate the catheterisation laboratory — the door-to-balloon time starts now.
Perform the focused bedside echocardiography: assess the left-ventricular contractility, exclude a tamponade and a right-heart strain, and guide the vasoactive choice.
Insert the arterial line, the central line, and the temperature probe. Start the temperature management (normothermia with the fever avoidance) from the ED, not the ICU.
Send the bloods: the full blood count, the coagulation, the electrolytes including the magnesium and the phosphate, the troponin, the lactate, the beta-hCG in the woman of childbearing age, and the toxicology screen.
Sedate and analgese: a propofol or a midazolam infusion with a fentanyl, avoiding the prolonged neuromuscular blockade unless the ventilation is difficult.
Arrange the transfer to the ICU with the continuing bundle — the handover includes the arrest rhythm, the downtime, the cause, the targets, and the drugs.
Targeted temperature management — the deep dive
The temperature management is the most evidence-rich and the most frequently examined element of the post-arrest care, and the Fellowship candidate must know the trial lineage in detail. The narrative has moved through three eras.[2]
The three eras of the targeted temperature management
Era 1 — therapeutic hypothermia (2002-2013)
- The Hypothermia After Cardiac Arrest (HACA) trial and the Bernard trial, both in 2002
- The HACA trial: the VF/VT OHCA cooled to 32-34°C had a better neurological outcome than the normothermia
- Adopted into the guidelines: the cooling of the comatose adult after a VF arrest to 32-34°C for 12-24 hours
- The selection bias and the lack of the blinding were later criticised
Era 2 — TTM (2013-2021)
- The 2013 TTM trial (Nielsen, NEJM): no difference between the 33°C and the 36°C target in the comatose OHCA survivor
- The target range widened; the 36°C was accepted
- The fever avoidance became as important as the hypothermia
- The practice began to shift toward the normothermia with the fever control
Era 3 — normothermia (TTM2, 2021 onward)
- The TTM2 trial (Dankiewicz, NEJM 2021): the hypothermia at 33°C was NOT superior to the normothermia
- More arrhythmias and the trend toward the higher mortality in the hypothermia group
- The contemporary practice: the normothermia (around 37°C) with the active fever avoidance (≤ 37.5 to 37.7°C) for at least 72 hours
- The 32-34°C hypothermia is no longer routinely recommended
Hypothermia After Cardiac Arrest (HACA) trial
New England Journal of Medicine
PMID 12398870
Key finding
The comatose survivors of the witnessed VF/VT out-of-hospital cardiac arrest cooled to 32-34°C for 24 hours had a favourable neurological outcome at 6 months in 55% versus 39% in the normothermia group (RR 1.40, 95% CI 1.08-1.81).
Practice change
Established the therapeutic hypothermia as the standard of care for the VF arrest — the foundation of the modern targeted temperature management.
Bernard et al — the Melbourne hypothermia trial
New England Journal of Medicine
PMID 12114037
Key finding
The comatose OHCA survivors cooled to 33°C for 12 hours had a good neurological outcome (discharged home or to rehab) in 49% versus 26% in the normothermia (P=0.046).
Practice change
The small, single-centre trial that, alongside the HACA, drove the adoption of the hypothermia.
TTM trial — 33°C versus 36°C
New England Journal of Medicine
PMID 24237006
Key finding
The 939 comatose OHCA survivors randomised to the 33°C versus the 36°C target; no difference in the all-cause mortality (50% vs 48%) or the neurological outcome at 180 days.
Practice change
The two targets were equivalent; the 36°C was accepted as the wider target and the practice shifted toward the normothermia.
TTM2 — hypothermia versus normothermia
New England Journal of Medicine
PMID 34133859
Key finding
The 1850 comatose OHCA survivors randomised to the hypothermia at 33°C versus the normothermia with the fever avoidance; no difference in the death at 180 days (50% vs 48%). The hypothermia group had more arrhythmias and the trend toward the worse outcome.
Practice change
The routine hypothermia at 33°C is NOT superior to the normothermia with the active fever avoidance; the contemporary practice is the normothermia and the fever control.
The practical temperature management
The temperature is monitored continuously with a bladder, an oesophageal, or a rectal probe (the oesophageal is the most accurate for the core temperature). The fever (over 37.5 to 37.7°C) is treated with the intravenous paracetamol 1 g, the surface cooling (the gel pads, the fans, the ice packs to the groin and the axillae), and the intravascular cooling device if available. The rewarming, if the hypothermia was used, is slow — no more than 0.25 to 0.5°C per hour — to avoid the rebound of the intracranial pressure and the electrolyte shifts. The temperature is maintained for at least 72 hours.[1]
Haemodynamic optimisation — the deep dive
The cerebral autoregulation is impaired after the cardiac arrest, and the cerebral blood flow becomes pressure-passive: a fall in the mean arterial pressure translates directly into a fall in the cerebral perfusion, and a rise into a rise in the intracranial pressure. The haemodynamic target is therefore both a floor and a ceiling — the MAP kept at 65 mmHg or more, and the hypertensive surges treated.[3]
The vasopressor and the inotrope strategy
Noradrenaline
- The first-line vasopressor; 0.05 to 0.5 mcg/kg/min IV
- An alpha agonist with a modest beta-1 effect; raises the SVR
- The preferred agent for the vasodilatory post-arrest shock
- Titrated to the MAP ≥ 65; the chronically hypertensive may need a higher target
Adrenaline
- 0.05 to 0.5 mcg/kg/min IV; the combined alpha and beta effect
- The alternative when the noradrenaline is unavailable, or for the added inotropy
- Raises the lactate and the myocardial oxygen demand; the second-line
- The high-dose adrenaline is associated with the worse outcome
Dobutamine
- 2 to 20 mcg/kg/min IV; the beta-1 inotrope
- For the low-cardiac-output state (the stunned myocardium, the cardiomyopathy)
- Often combined with the noradrenaline (the vasodilation from the dobutamine is offset)
- May cause the tachycardia and the arrhythmia; titrate carefully
Vasopressin
- 0.01 to 0.04 U/min IV; the V1 receptor agonist
- A catecholamine-sparing adjunct in the refractory vasodilatory shock
- Not a first-line; the evidence in the post-arrest shock is limited
- The fixed-dose; not titrated
Oxygen and ventilation — the deep dive
The oxygen target
The brain after the cardiac arrest is caught between the Scylla of the hypoxia and the Charybdis of the hyperoxia. The hypoxia causes the ongoing anoxic injury; the hyperoxia generates the reactive oxygen species, causes the absorption atelectasis, and the cerebral vasoconstriction. The EXACT trial resolved the question: the restrictive strategy (the SpO₂ of 88 to 92%) was not superior to the liberal strategy (the SpO₂ of 98% or more, with the FiO₂ titrated down), and the contemporary practice is the normoxia — the SpO₂ of 94 to 98%, the FiO₂ titrated to the lowest that maintains the target.[3]
EXACT — the oxygen targets after the cardiac arrest
New England Journal of Medicine
PMID 36027567
Key finding
The 789 comatose OHCA survivors randomised to the restrictive oxygen (the SpO₂ 88-92%) versus the conservative/liberal (the PaO₂ target normal). The restrictive strategy was NOT superior for the neurological outcome at 90 days. The hyperoxia avoidance, not the aggressive restriction, is the goal.
Practice change
The normoxic target (SpO₂ 94-98%, the FiO₂ titrated) is the standard; the deliberate hypoxia is not superior and may be harmful.
The ventilation and the carbon dioxide
The carbon dioxide is the master regulator of the cerebrovascular tone. The PaCO₂ below 35 mmHg (the hypocapnia) constricts the cerebral vessels and reduces the cerebral blood flow by 2 to 4% per mmHg drop; the PaCO₂ above 45 (the hypercapnia) raises the intracranial pressure. The target is the normocapnia — the PaCO₂ of 35 to 45 mmHg (4.5 to 6.0 kPa) — and the ventilation is controlled and monitored with the serial arterial blood gases.[3]
[3] [1]Coronary angiography — the reperfusion strategy
The acute coronary syndrome is the commonest cause of the out-of-hospital cardiac arrest, and the urgent coronary angiography with the percutaneous coronary intervention is part of the post-arrest bundle for the patient with a presumed cardiac cause. The decision to activate the catheterisation laboratory is made on the ECG and the clinical context, not delayed for the cardiac enzymes.[1]
The immediate versus the deferred angiography
Immediate angio (the obvious STEMI)
- The ST-elevation MI: the immediate angiography, the same as the non-arrest STEMI
- The door-to-balloon time starts at the ED arrival; the 90-minute target applies
- The patient is transferred directly from the ED to the catheterisation laboratory
- The bundle (the oxygen, the MAP, the temperature) is continued during the procedure
Immediate angio (the high-suspicion non-STEMI)
- The no-ST-elevation but the high suspicion (the cardiac rhythm at presentation, the history of the angina, the shocked state)
- The COACT trial and the TOMAHAWK trial: the immediate angiography is NOT superior to the deferred in the no-ST-elevation OHCA without the shock
- The exception: the shock state, the haemodynamic instability, the ongoing ischaemia — these get the immediate angio
- The decision is individualised; the stable patient without the ST elevation can wait for the angio after the initial stabilisation
Deferred angio
- The no-ST-elevation, the stable patient: the angiography after the stabilisation (24 to 72 hours)
- The troponin is NOT the decision-maker — the troponin is raised after every arrest
- The non-cardiac cause (the drowning, the overdose, the PE) does not need the angiography
- The echocardiography (the wall-motion abnormality) and the clinical picture guide the timing
COACT — immediate versus delayed angiography in the no-STE-OHCA
New England Journal of Medicine
PMID 31242382
Key finding
The 552 comatose survivors of the no-ST-elevation OHCA randomised to the immediate versus the delayed coronary angiography; no difference in the 90-day neurological outcome (64.5% vs 64.0% good outcome).
Practice change
The immediate angiography is NOT routinely superior to the deferred in the stable no-ST-elevation OHCA; the ST-elevation and the unstable patient still get the immediate angio.
TOMAHAWK — immediate versus delayed angiography in the no-STE-OHCA
New England Journal of Medicine
PMID 36195155
Key finding
The 530 comatose no-ST-elevation OHCA survivors randomised to the immediate versus the deferred angiography; no difference in the all-cause mortality at 30 days (44% vs 44%).
Practice change
The deferred strategy is safe in the stable no-ST-elevation OHCA; the immediate angiography adds the contrast load and the procedural risk without the benefit.
Seizure detection and management
The seizures and the status epilepticus are common after the cardiac arrest (the clinical seizures in 10 to 20%, the electrographic seizures on the continuous EEG in 20 to 30%), and they worsen the secondary brain injury. The clinical detection is confounded by the sedation and the neuromuscular blockade, and the continuous electroencephalography is the gold standard for the detection.[1]
[3]The post-arrest seizure types
Clinical seizure
- The overt motor activity: the tonic-clonic, the focal twitching, the convulsive status
- Detected clinically; treated immediately with the levetiracetam or the benzodiazepine
- The motor activity may be masked by the sedation or the paralysis
- The predictor of the worse outcome, but NOT universally fatal
Myoclonus
- The brief, irregular, multifocal jerks; the "post-anoxic myoclonus"
- The status myoclonus (the continuous, the first 24 hours) is a strong predictor of the poor outcome
- Distinguished from the seizure: the myoclonus is cortical OR subcortical; the EEG helps
- Treated with the clonazepam, the levetiracetam, or the valproate; the propofol for the refractory
Non-convulsive / electrographic
- The seizure on the EEG without the clinical correlate
- The non-convulsive status epilepticus: the continuous epileptiform discharges
- Detected ONLY by the continuous EEG; the most easily missed
- Treated as the status epilepticus: the benzodiazepine, the levetiracetam, the propofol infusion
Prognostication — the multimodal algorithm
The prognostication of the neurological outcome is the most fraught decision in the post-arrest care, because the premature or the overly pessimistic prediction becomes the self-fulfilling prophecy: the care is withdrawn, and the patient dies, confirming the prediction. The Fellowship-level prognostication is multimodal, deferred, and team-based.[2]
The ERC/ESICM prognostication algorithm
The multimodal prognostication algorithm (the ERC/ESICM 2025)
Wait: no prognostication before 72 hours after the ROSC, AND at least 72 hours after the rewarming is complete. The sedation is off, the metabolic and the toxic causes are excluded, and the normothermia is maintained.
The clinical examination: the brainstem reflexes (the pupillary, the corneal, the gag, the cough), the motor response to the pain, the presence of the myoclonus. The absent brainstem reflexes or the extensor posturing (the GCS M1-M3) at 72 hours are the concerning signs.
The somatosensory evoked potentials (the SSEP): the bilaterally absent N20 cortical response (the median-nerve SSEP) is the most robust single predictor of the poor outcome, with the false-positive rate near zero.
The electroencephalography: the malignant patterns (the suppressed background, the burst-suppression, the status epilepticus, the generalised periodic discharges) are associated with the poor outcome but are NOT sufficient alone.
The neuron-specific enolase (the NSE): the serum level above 60 ng/mL (at 24 to 72 hours) is associated with the poor outcome; the cut-off varies by the assay and the laboratory.
The neuroimaging: the cerebral CT for the gross oedema (the loss of the grey-white differentiation, the sulcal effacement); the MRI for the diffusion restriction in the cortex, the basal ganglia, the thalamus.
The integration: NO single modality is sufficient. The poor outcome is predicted by the concordance of two or more modalities (the absent N20 plus the malignant EEG plus the high NSE, for example). The prognostication is made by the team — the intensivist, the neurologist, the nursing — and communicated to the family.
Transfer to the intensive care unit
The post-arrest patient is transferred to the ICU as soon as the ED stabilisation is complete — the airway secured, the ventilation set, the MAP supported, the temperature started, the ECG done, and the cause investigated to the point of the definitive plan (the angiography, the thrombolysis, the surgical source control). The transfer is a high-risk handover, and the bundle continues uninterrupted.[2]
The safe transfer to the ICU — the checklist
The airway is secured: the endotracheal tube is confirmed on the capnography and the chest X-ray; the ventilator is set to the post-arrest targets (the Vt 6-8 mL/kg, the FiO₂ titrated, the PEEP 5-10).
The circulation is supported: the arterial line is in, the MAP ≥ 65 on the vasopressor; two points of the large-bore IV access; the blood is sent and the cross-match is available if needed.
The monitoring is continuous: the SpO₂, the ECG, the invasive blood pressure, the capnography, and the temperature probe are all on and the alarms are set.
The drugs are drawn up: the sedation and the analgesia infusions running; the vasopressor on the pump; the rescue drugs (the adrenaline, the amiodarone, the levetiracetam) available.
The documentation is complete: the arrest timeline (the downtime, the rhythm, the interventions), the ROSC time, the post-arrest blood gases and the ECG, the cause and the definitive plan, the family communication.
The receiving ICU team is briefed: the structured handover (the ISBAR — the identify, the situation, the background, the assessment, the recommendation) with the specific targets (the MAP, the SpO₂, the PaCO₂, the temperature, the glucose) and the plan (the angiography, the CT, the cEEG).
Common pitfalls
The recurring errors are: allowing the hyperoxia by leaving the fraction at 100 per cent; hyperventilating to a hypocapnia; tolerating the hypotension; targeting the 33-degree hypothermia that the TTM2 trial showed is not superior and that causes more arrhythmia; not treating the fever; not detecting the seizures (without the continuous EEG); a prognostication that is too early, too single-modal, or made under sedation; and the failure to identify and treat the cause. The post-arrest patient who is "just observed" pending the intensive-care bed, without the bundle applied, is the patient who survives to a poor neurological outcome.[1]
SAQ — The post-ROSC bundle and the secondary brain injury
10 minutes · 10 marks
A 56-year-old man has just achieved the return of spontaneous circulation after an out-of-hospital ventricular fibrillation arrest of an estimated 12 minutes. He is intubated and unconscious, the blood pressure is 85 over 50, the saturation is 99 per cent on the fraction of inspired oxygen of 1.0, and the core temperature is 37.8 degrees Celsius.
SAQ — Coronary reperfusion and seizure control after the arrest
10 minutes · 10 marks
A 62-year-old woman is resuscitated from an out-of-hospital cardiac arrest. The initial rhythm was a ventricular fibrillation, the downtime was 15 minutes, and the post-arrest 12-lead electrocardiogram shows no ST elevation but a left bundle branch block. She remains comatose and intubated.
Red flags
The following features identify the post-arrest patient at risk of a poor outcome or a preventable secondary injury, in which the bundle is applied and the prognostication deferred:[1]
[3]References
- [1]Dankiewicz J, Cronberg T, Lilja G, et al. Hypothermia versus normothermia after out-of-hospital cardiac arrest (TTM2). New England Journal of Medicine, 2021.PMID 34133859
- [2]Nolan JP, Sandroni C, Böttiger BW, et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines: post-resuscitation care. Intensive Care Medicine, 2025.PMID 41123621
- [3]Schmidt H, Kjaergaard J, Hassager C, et al. Oxygen targets in comatose survivors of cardiac arrest (EXACT). New England Journal of Medicine, 2022.PMID 36027567
- [4]Drennan IR, Berg KM, Böttiger BW, et al. Advanced Life Support: 2025 International Liaison Committee on Resuscitation Consensus on Science with Treatment Recommendations (ILCOR CoSTR). Resuscitation, 2025.PMID 41117578
- [5]Nolan JP, Sandroni C, Cariou A, et al. European Resuscitation Council and European Society of Intensive Care Medicine Guidelines 2025 Post-Resuscitation Care. Resuscitation, 2025.PMID 41117575