EM · Burn management
Burn management
The burn management from the depth classification and the TBSA estimation through the Parkland resuscitation formula, the inhalation injury and the carbon monoxide, the escharotomy for the circumferential burn, the wound dressings and the debridement, the electrical and the chemical burns, and the transfer criteria to the burn centre.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
The burn injury is managed in the emergency department by the structured approach that addresses the airway and the inhalation injury first, the fluid resuscitation of the burn shock, the estimation of the depth and the surface area, the wound management, and the decision on the transfer to the burn centre. The Fellowship candidate must know the Parkland formula, the Rule of Nines, the depth classification, the inhalation injury, the escharotomy, the electrical and the chemical burns, and the systemic complications that follow the large burn.[4][5]
The ED resuscitation — the structured approach in the first hour
The burn patient is managed by the same primary survey as the other trauma patient, with the burn-specific modifications. The airway (and the inhalation injury) is the first priority because the airway obstruction from the thermal oedema is the rapidly lethal event. The catastrophic haemorrhage is controlled (the direct pressure, the tourniquet). The oxygen (the 100 per cent via the non-rebreather mask for every suspected inhalation injury), the IV access (the two large-bore cannulae, the bloods including the carboxyhaemoglobin and the lactate), and the fluid resuscitation (the Parkland for the burn over 10 per cent in the child or 15 per cent in the adult) follow. The analgesia (the intravenous opioid titrated), the tetanus prophylaxis, the urinary catheter (to monitor the resuscitation), and the nasogastric tube (for the burn over 20 per cent TBSA, to decompress the gastric ileus and the Curling-ulcer prophylaxis) complete the first hour.[4][5]
The first hour of the burn resuscitation — the ED checklist
A — Airway with the cervical-spine control
Assess the airway and the inhalation-injury signs (the facial burns, the singed hairs, the carbonaceous sputum, the hoarseness, the stridor). Give the 100 per cent oxygen via the non-rebreather. Intubate EARLY if the inhalation injury is suspected and progressing — the early intubation is safer than the late. The cervical spine is protected in the fall, the explosion, the jump to escape.
B — Breathing and the ventilation
Assess the work of the breathing, the oxygen saturation (lies in the CO poisoning — use the co-oximetry), the chest movement (the circumferential chest burn restricts the ventilation — the escharotomy). The arterial blood gas, the carboxyhaemoglobin, the lactate, and the chest X-ray.
C — Circulation and the fluid resuscitation
Two large-bore cannulae, the bloods (the FBC, the U and E, the CK, the coagulation, the group and save, the carboxyhaemoglobin, the lactate, the blood gas). Start the Parkland resuscitation (the Ringer lactate 4 mL per kg per per cent TBSA) for the burn over 10 per cent in the child or 15 per cent in the adult. The half in the first 8 hours from the time of the burn.
D — Disability
The GCS, the pupils (the CO poisoning produces the depressed conscious level), the blood glucose (the child, the diabetic). The analgesia (the IV opioid titrated) is given early — the burn pain is severe.
E — Exposure, the cooling, and the estimate
Expose the whole patient (keep warm — the hypothermia worsens the coagulopathy). Cool the burn (the running water at 15 to 25 degrees for 20 minutes, within the first 3 hours — NOT the ice). Estimate the TBSA (the Rule of Nines or the Lund-Browder, exclude the superficial) and the depth. Cover with the cling film for the transfer.
The adjuncts
The urinary catheter (for the urine-output titration of the resuscitation) and the nasogastric tube (for the burn over 20 per cent TBSA — the gastric ileus and the aspiration risk). The tetanus prophylaxis. The analgesia titrated. The antibiotics are NOT given prophylactically (they do not prevent the infection and they select the resistant organisms).
The disposition
Apply the burn-centre transfer criteria. Notify the burn centre early — the retrieval and the bed take the time. Document the time of the burn, the weight, the TBSA, the depth, the Parkland calculation, the fluid given, and the urine output.
The burn depth
The burn depth determines the healing, the scarring and the need for the surgery.[4][5] The superficial (the epidermal) burn is red, painful, blanching, without the blisters (the sunburn). The superficial dermal burn is red, painful, blistering, blanching. The deep dermal burn is red-and-white, slowly blanching, less painful (the nerve damage). The full-thickness burn is white, leathery, non-blanching, painless (the nerve destruction), and it requires the surgery. The deep dermal and the full-thickness burns need the surgical assessment for the excision and the grafting.
The burn depth — the categories and the discrimination
The burn depth is classified by the layer of the skin injured, and it determines the healing potential and the need for the surgery. The traditional four categories are the superficial (epidermal), the superficial dermal (the superficial partial-thickness), the deep dermal (the deep partial-thickness), and the full-thickness. Some systems add a fifth — the deep full-thickness (the injury extends into the subcutaneous fat, the fascia or the muscle).[14]
| The depth | The appearance | The sensation | The blanching | The healing | The surgery |
|---|---|---|---|---|---|
| The superficial (epidermal) | The red, the dry, the no blisters (the sunburn) | The painful | The brisk | The 3 to 6 days, the no scar | The none |
| The superficial dermal (the superficial partial) | The red, the wet, the blistering | The very painful | The brisk | The 7 to 14 days, the minimal scar | The none |
| The deep dermal (the deep partial) | The red-and-white, the mottled, the moist | The less painful (the nerve damaged) | The slow or the sluggish | The 14 to 28 days, the hypertrophic scar | The grafting if not healed at 3 weeks |
| The full-thickness | The white, the waxy, the leathery, the dry | The painless (the nerve destroyed) | The none | The none (the skin appendages destroyed) | The excision and the grafting |
| The deep full-thickness (the fourth-degree) | The charred, the thrombosed veins, the muscle or the bone visible | The painless | The none | The none | The excision, the grafting, the flap, the amputation |
The laser-Doppler scan — the objective depth assessment
When to scan
The laser-Doppler imaging (the LDI) measures the dermal perfusion at 48 to 72 hours after the burn. It is most accurate for the intermediate-depth burns (the superficial vs the deep dermal) where the clinical judgement is least reliable. The scan is performed on the day 2 or the day 3, when the perfusion has stabilised.
What it measures
The LDI scans the burn with the near-infrared laser and measures the Doppler shift of the moving red cells in the dermis. The perfusion is colour-coded: the high perfusion (the red or the yellow) indicates the superficial burn that will heal; the low perfusion (the blue or the green) indicates the deep burn that will need the graft.
The accuracy
The LDI has the sensitivity and the specificity over 90 per cent for the prediction of the healing within 14 days — far superior to the clinical assessment (around 60 to 70 per cent). It reduces the unnecessary surgery on the burns that would have healed, and the delayed surgery on the burns that would not.
The limitations
The LDI is not available in every centre; it is not accurate before the 48 hours (the perfusion is unstable); it is less reliable on the pigmented skin, the infected burn, and the heavily blistered burn; and it cannot assess the full-thickness burn (the perfusion is already absent).
The laser-Doppler imaging for the burn depth (Wang, 2020 — the meta-analysis; Shin, 2016)
The burn surface area
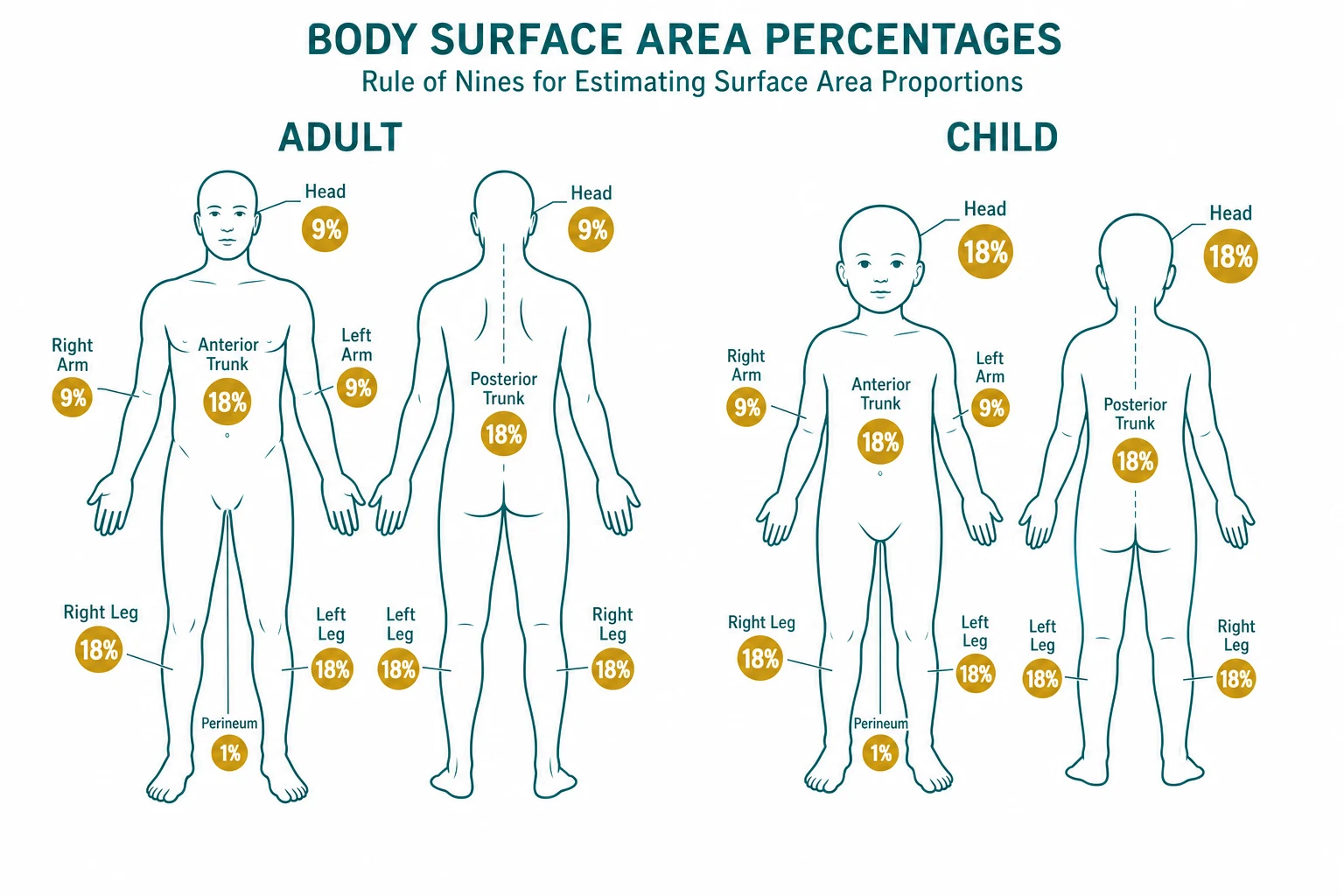
The total body surface area (the TBSA) is estimated to guide the fluid resuscitation. The Rule of Nines assigns 9 per cent to the head, 9 per cent to each arm, 18 per cent to each leg, 18 per cent to the anterior trunk, 18 per cent to the posterior trunk, and 1 per cent to the perineum. The Lund and Browder chart is more accurate for the children (whose head is proportionally larger and the legs smaller). The palm method (the patient's palm including the fingers is approximately 1 per cent of the TBSA) is used for the small or the scattered burns. The superficial burns are NOT counted in the TBSA for the resuscitation.[4]
The TBSA estimation — the methods and the accuracy
The total body surface area (the TBSA) drives the fluid resuscitation, so the accurate estimation matters. The three methods — the Rule of Nines (the Wallace), the Lund and Browder chart, and the palmar-surface method — are used together for the cross-check. Only the partial-thickness and the full-thickness burns are counted; the superficial (the erythema) is excluded.[6][10]
| The body region | The adult (the Rule of Nines) | The child (the Lund-Browder) | The infant |
|---|---|---|---|
| The head and the neck | 9 per cent | 18 per cent (at birth) down to 9 per cent (at 10 years) | 18 to 19 per cent |
| Each arm | 9 per cent | 9 per cent | 9 per cent |
| The anterior trunk | 18 per cent | 18 per cent | 18 per cent |
| The posterior trunk | 18 per cent | 18 per cent | 18 per cent |
| Each leg | 18 per cent | 14 per cent (at birth) up to 18 per cent (at 10 years) | 14 per cent |
| The perineum | 1 per cent | 1 per cent | 1 per cent |
The TBSA estimation — the workflow in the emergency department
Expose and cool
Remove the clothing (the rescuer wears the gloves — the chemical may persist), cool the burn with the running water at 15 to 25 degrees for 20 minutes (within the first 3 hours), and then expose the whole body for the assessment. Keep the patient warm — the hypothermia worsens the coagulopathy and the outcome.
Estimate the per-region
Use the Rule of Nines (the adult) or the Lund-Browder chart (the child) for the large contiguous burns. Mark the burns on the chart. Cross-check with the palmar method for the scattered burns. Exclude the superficial (the erythema).
Sum and document
Add the regions for the total per cent TBSA (the partial- plus the full-thickness). Document the per-region and the total, and the depth, on the burn chart. The re-estimation on the day 1 and the day 2 is expected — the burn evolves (the blanching in the partial-thickness may become the fixed colour of the full-thickness).
Cross-check with the fluid plan
Use the per cent TBSA for the Parkland formula. If the urine output is below the target despite the calculated rate, re-estimate the TBSA (the underestimation is the commonest cause of the under-resuscitation) and the depth (the deeper burn leaks more).
The fluid resuscitation: the Parkland formula
The burn shock is the hypovolaemic shock from the massive fluid shift into the burned tissue (the capillary leak, the oedema), and it is managed by the formula-guided resuscitation. The Parkland formula gives 2 to 4 millilitres of the Ringer's lactate per kilogram per per cent TBSA over the first 24 hours from the time of the burn, with half in the first 8 hours and the remainder over the next 16 hours. The formula is a starting point, and the actual rate is titrated to the urine output (0.5 to 1 millilitre per kilogram per hour in the adult, 1 to 1.5 in the child). The colloid is considered after the first 24 hours (when the capillary leak resolves). The fluid creep (the excessive fluid from the underestimation of the leak or the formula error) causes the oedema and the compartment syndrome, and it is avoided by the urine-output titration.[1][4]
The Parkland worked example — the calculation that the candidate must do
The formula is the starting point. The total 24-hour volume is calculated, half is given in the first 8 hours from the time of the burn, and the rate is then titrated to the urine output. The worked example: a 70 kg adult with a 40 per cent TBSA burn, presenting 2 hours after the burn. The Parkland volume (using 4 mL per kg per per cent) is 4 × 70 × 40 = 11,200 mL of the Ringer lactate over 24 hours. Half (5,600 mL) is given in the first 8 hours from the time of the burn — but 2 hours have already elapsed, so the 5,600 mL is given over the remaining 6 hours, at approximately 933 mL per hour. The remainder (5,600 mL) is given over the next 16 hours, at 350 mL per hour. The urine output is checked hourly and the rate is adjusted to maintain 0.5 to 1 mL per kg per hour.[11][1]
The Parkland resuscitation — the calculation in steps
Establish the parameters
The weight (the estimated or the measured — the obese patient is tricky), the per cent TBSA (the Rule of Nines or the Lund-Browder, counting only the partial- and the full-thickness burns), and the time since the burn (the clock starts at the burn, not the arrival).
Calculate the 24-hour volume
The Ringer lactate volume = 4 mL times the weight (kg) times the per cent TBSA. Some centres use 2 mL per kg per per cent (the modified Brooke) for the smaller burn; the trend is toward the lower volume to avoid the fluid creep. The 4 mL Parkland is the standard starting point.
Give half in the first 8 hours
The first half is given over the 8 hours FROM THE TIME OF THE BURN. If the patient arrives 3 hours after the burn, the first half is given over the remaining 5 hours, not the 8 hours.
Give the second half over 16 hours
The remaining half over the next 16 hours (the 8th to the 24th hour from the burn).
Titrate to the urine output
The urine output target is 0.5 to 1 mL per kg per hour in the adult, 1 to 1.5 mL per kg per hour in the child (under 30 kg), and 1.5 to 2 mL per kg per hour in the electrical injury (to flush the myoglobin). The rate is adjusted up or down by 25 to 33 per cent each hour based on the output. The formula is a guess; the urine output is the truth.
After 24 hours
The colloid (the 5 per cent albumin) is introduced — the capillary leak has largely resolved and the colloid stays in the intravascular space. The maintenance fluid is added in the child. The wound loss and the evaporative loss are replaced separately.
| The resuscitation formula | The crystalloid volume (first 24 h) | The origin | The notes |
|---|---|---|---|
| The Parkland (Baxter) | 4 mL per kg per per cent TBSA | The 1968 formula | The most widely used starting point; the high crystalloid load risks the fluid creep |
| The modified Brooke | 2 mL per kg per per cent TBSA | The 1970s revision | The lower volume; preferred by many burn centres for the moderate burn |
| The Rule of 10s | 10 times the per cent TBSA (in 100s of mL per hour); add 100 mL per hour for every 10 per cent above the initial | The military and the pre-hospital | The simple, the rapid, the weight-free estimate for the first hour |
| The colloid-based (the Shen and others) | The colloid added early | The modern trend | The reduction of the fluid creep and the oedema |
The Parkland vs the modified Brooke — the accuracy and the outcome (Alotaibi, 2025; Dahl, 2023)
The inhalation injury
The inhalation injury is the commonest cause of the death in the burn patient, and it is assessed in the first minutes. The supraglottic thermal injury (the upper airway oedema from the hot gas) can obstruct over the hours, and the early intubation (before the oedema closes the airway) is safer than the late. The signs are the facial burns, the singed nasal hairs, the carbonaceous sputum, the hoarseness and the stridor. The carbon monoxide poisoning (the CO binds the haemoglobin and the cytochrome, producing the tissue hypoxia) is treated with the 100 per cent oxygen (which displaces the CO from the haemoglobin and reduces the half-life from 4 to 5 hours to 40 to 80 minutes). The cyanide poisoning (from the combustion of the plastics and the wool) is treated with the hydroxocobalamin (which binds the cyanide to form the cyanocobalamin), supported by the systematic review evidence.[2][4]
The airway in the inhalation injury — the early intubation
The supraglottic thermal injury (the oedema of the supraglottic structures from the hot gas, the steam, or the direct flame) progresses over 6 to 24 hours. The oedema closes the airway with terrifying speed once the swelling reaches the critical narrowing of the glottis — the early intubation (while the airway is still patent and the anatomy is visible) is far safer than the late attempt through the swollen, distorted, bleeding tissues. The signs that mandate the early intubation are the progressive hoarseness, the stridor (a late, pre-arrest sign), the drooling, the labour of the breathing, and the deep burns of the face and the neck.[16][17][18]
The inhalation injury — the assessment and the airway decision
Recognise the risk
The history: the fire in an enclosed space, the exposure to the smoke, the steam, the explosion, the loss of consciousness. The signs: the facial burns, the singed nasal hairs and eyebrows, the carbonaceous sputum, the soot in the mouth and the pharynx, the hoarseness, the wheeze, the stridor. Any one of these is the inhalation injury until proven otherwise.
Assess the airway and the gas exchange
The fibre-optic nasendoscopy at the bedside shows the supraglottic oedema, the soot, and the mucosal change. The chest X-ray is often normal early (it lags). The arterial blood gas and the carboxyhaemoglobin level are taken on the arrival. The lactate is raised in the cyanide poisoning (the cellular hypoxia despite the well-oxygenated blood).
The early intubation decision
Intubate EARLY if the hoarseness is progressing, there is any stridor, the facial burns are deep, the work of breathing is rising, the patient needs the transfer with an unsecured airway, or the bronchoscopy shows the severe lower-airway injury. The cuffed tube is sized smaller (the oedema narrows the glottis) and the difficult-airway equipment and the surgical airway plan are ready.
The carbon monoxide and the cyanide
The 100 per cent oxygen via the non-rebreather mask (or the ventilator) is given to every suspected inhalation injury — it reduces the carboxyhaemoglobin half-life from 4 to 5 hours to 40 to 80 minutes. The cyanide is suspected in the enclosed-space fire with the persistent lactic acidosis despite the oxygen, the soot, and the hypotension; the hydroxocobalamin 5 g IV (the adult dose) is given on the suspicion.
| Feature | The carbon monoxide poisoning | The cyanide poisoning |
|---|---|---|
| The source | The incomplete combustion (the car exhaust, the faulty heater, the enclosed-space fire) | The combustion of the plastics, the wool, the polyurethane (the house fire, the industrial fire) |
| The mechanism | The CO binds the haemoglobin (the carboxyhaemoglobin), shifts the curve left, and binds the cytochrome | The cyanide binds the cytochrome a3, halting the oxidative phosphorylation — the cellular hypoxia despite the high venous and arterial oxygen |
| The pulse oximetry | Falsely normal (the CO-Hb absorbs at the same wavelength as the oxy-Hb) | Normal |
| The blood gas | The metabolic acidosis is mild early; the carboxyhaemoglobin is raised | The severe metabolic (lactic) acidosis, the high venous oxygen (the tissues cannot extract) |
| The classic sign | The cherry-red skin (rare, the pre-mortem) | The bitter-almond breath (rare) |
| The treatment | The 100 per cent oxygen; the hyperbaric oxygen for the severe case | The hydroxocobalamin (the cyanide binds the cobalt to form the cyanocobalamin); the sodium thiosulphate is the alternative |
| The half-life | 4 to 5 hours on the room air; 40 to 80 minutes on the 100 per cent oxygen | Determined by the detoxification rate |
Hydroxocobalamin for the smoke-inhalation cyanide (Jin, 2025) — the systematic review
The escharotomy
The circumferential full-thickness burn to a limb or the chest forms an inelastic eschar that prevents the expansion of the underlying tissue (the oedematous muscle or the chest wall), producing the compartment syndrome or the ventilatory compromise. The escharotomy — the incision through the full-thickness eschar down to the subcutaneous fat (which is painless because the nerves in the full-thickness burn are destroyed) — releases the constriction. The incisions are made along the medial and the lateral aspects of the limb or the anterior chest wall, and the release is confirmed by the improvement in the perfusion or the ventilation.[4][5]
The escharotomy — the indications and the technique
The escharotomy is the surgical release of the inelastic full-thickness eschar that constricts the underlying tissue. It is performed when the circumferential (or the near-circumferential) full-thickness burn compromises the circulation (the limb) or the ventilation (the chest).[19][20]
The escharotomy — the decision and the technique
Recognise the constriction
The circumferential full-thickness burn on the limb or the chest. The limb signs are the progressive pain, the paraesthesia, the pallor, the prolonged capillary refill, and the reduced or the absent pulse (a late sign — use the Doppler to detect the flow before the pulse is lost). The chest signs are the rising peak airway pressure in the ventilated patient, the reduced tidal volume, and the respiratory distress.
Mark the incision lines
The limb: the mid-lateral and the mid-medial lines from the proximal to the distal extent of the eschar, crossing the joints at the midline (avoid the neurovascular bundles that run the postero-medial and the postero-lateral aspects). The chest: the bilateral anterior axillary lines from the clavicle to the costal margin, joined by the subcostal and the transverse incisions (the grid or the coat-hanger pattern) to release the chest wall.
Incise through the eschar to the fat
The scalpel or the diathermy incises through the full-thickness eschar (which is painless — the nerve endings are destroyed) down to the subcutaneous fat; the release is confirmed by the separation of the eschar edges and the bulging of the underlying fat. Do NOT incise into the healthy tissue below the fat (the painful, the bleeding, and the muscle-damaging).
Confirm the release
The limb: the return of the Doppler signal, the improved capillary refill, the warmed and the pink distal digit. The chest: the fall in the peak airway pressure, the rise in the tidal volume. If the release is inadequate, the fasciotomy is the next step (the deep compartment is also involved in the electrical and the high-voltage injury).
Control the bleeding and dress
The bleeding points are controlled with the diathermy; the escharotomy wound is dressed with the non-adherent dressing. The limb is elevated. The patient is transferred to the burn centre for the definitive wound care.
The wound management
The burn wound is cooled (within 3 hours of the injury, with the running water at 15 to 25 degrees for 20 minutes — not ice), cleaned, the blisters are deroofed (the large or the ruptured) or left (the small, the intact), and dressed. The silver sulfadiazine is the traditional dressing (the antimicrobial, but it delays the healing and the assessment). The modern dressings include the nanocrystalline silver (the Acticoat), the hydrocolloids, the biosynthetic membranes and the vacuum-assisted closure. The tetanus prophylaxis is given. The deep dermal and the full-thickness burns are referred for the early excision and the grafting (within 3 to 5 days).[4][5]
The dressings — the options and the trade-offs
| The dressing | The indication | The advantage | The limitation |
|---|---|---|---|
| The silver sulfadiazine (SSD) | The traditional | The antimicrobial, the cheap | Delays the healing, the pseudoeschar (the grey staining obscures the depth), the leucopenia, the sulpha allergy |
| The nanocrystalline silver (Acticoat) | The partial-thickness | The sustained silver release for 3 days, the reduced dressing changes | The cost; keep moist with the sterile water (not the saline — it precipitates) |
| The hydrocolloid (Duoderm) | The superficial, the small | The occlusive, the autolysis, the pain-free | The bulky, the malodorous gel, the not for the infected wound |
| The biosynthetic (Biobrane) | The clean partial-thickness | The adheres in 24 h, the pain relief, the outpatient management | The not for the infected or the heavily exudative wound |
| The VAC (vacuum-assisted closure) | The graft, the large wound | The promotes the granulation, the reduces the oedema | The machine, the power, the not for the unexplored cavity |
| The cling film (the transfer) | The ED dressing for the transfer | The transparent, the non-adherent, the occlusive | The not a definitive dressing — for the transfer only |
The electrical and the chemical burns
The electrical burn — the injury from the electrical current, which enters and exits the body — causes the deep tissue injury along the path (the muscle, the nerve, the vessel), which is disproportionate to the visible skin injury. The cardiac monitoring (the arrhythmia), the ECG, the serum CK and the myoglobin (the rhabdomyolysis and the AKI), and the compartment syndrome assessment are essential. The chemical burn is irrigated copiously with the water (for the acid) or carefully brushed off and then irrigated (for the dry powder). The tar burns are cooled with the water and removed with the solvent (the paraffin or the MEDISSOL).[4][3]
The chemical burn — the priority is the decontamination
The chemical burn continues to injure until the agent is removed or neutralised — the irrigation is the treatment, not the dressing. The acid burn is irrigated copiously with the running water for at least 30 minutes (the water dilutes and the heat dissipates). The alkali (the caustic, the oven cleaner, the cement) burn is irrigated for much longer (one to two hours) because the alkali dissolves the tissue by the liquefactive necrosis that continues as long as the agent is present. The dry powder is brushed off FIRST (the water activates some powders) and then irrigated. The hydrofluoric acid burn is a special case — the fluoride ion binds the calcium and magnesium, producing the deep tissue necrosis and the lethal hypocalcaemia; it is irrigated and then treated with the topical calcium gluconate gel (and the intra-arterial calcium for the severe case).[5]
The chemical burn — the decontamination in steps
Remove the agent
Brush off the dry powder first (the water may activate it), remove the contaminated clothing (the rescuer wears the gloves and the gown — the chemical injures the rescuer too), and isolate the clothing in a sealed bag.
Irrigate copiously
The running water at body temperature for at least 30 minutes for the acid and one to two hours for the alkali. The irrigation continues until the pH of the effluent is neutral (test with the litmus paper). The high-volume low-pressure irrigation is preferred — the high-pressure jet drives the chemical deeper.
The special agents
The hydrofluoric acid — apply the calcium gluconate gel (massage in continuously) and consider the intra-arterial calcium for the deep burn. The white phosphorus — keep wet (it ignites on contact with the air) and remove the particles in the dark room (they glow). The tar — cool with the water, then remove with the solvent (the paraffin or the commercial remover such as MEDISSOL); never peel the cooled tar off forcibly.
Assess the depth and the systemic effect
The chemical burn is often deeper than it appears — reassess at 24 hours. The bloods include the calcium and the magnesium for the hydrofluoric acid, the renal function and the CK for the systemic toxicity, and the ECG for the electrolyte-driven arrhythmia.
| Feature | The acid burn | The alkali burn |
|---|---|---|
| The pH | Below 7 | Above 7 |
| The necrosis | The coagulative (the eschar forms, limiting the penetration) | The liquefactive (no eschar, deep and continuing penetration) |
| The irrigation time | At least 30 minutes | One to two hours |
| The severity | Often less deep (the coagulum limits it) | Often more deep (the continuous liquefaction) |
| The classic agent | The sulphuric, the hydrochloric, the hydrofluoric | The sodium hydroxide, the potassium hydroxide, the cement |
The transfer to the burn centre
The criteria for the transfer to the burn centre (per the ANZBA and the ABA criteria) include: the partial-thickness burn over 10 per cent TBSA, the full-thickness burn over 5 per cent, the burns to the face, the hands, the feet, the genitals, the perineum or the major joints, the electrical or the chemical burns, the inhalation injury, the burns with the comorbidity or the associated trauma, and the burns in the child, the elderly or the pregnant patient.[5]
The burn-centre transfer criteria in detail
The decision to transfer is structured around the ABA (American Burn Association) and the ANZBA (Australian and New Zealand Burn Association) consensus criteria. The burns that meet any one of the following are referred to a designated burn centre for the definitive care.[5]
| The criterion | The threshold |
|---|---|
| Partial-thickness burn | Greater than 10 per cent of the total body surface area |
| Full-thickness burn | Any full-thickness burn (and especially over 5 per cent) |
| The special sites | The face, the hands, the feet, the genitals, the perineum, and the major joints |
| The electrical burns | Including the lightning injury — the deep injury is disproportionate to the skin |
| The chemical burns | Especially the alkali — the continuous liquefactive necrosis |
| The inhalation injury | The commonest cause of the death in the burn — needs the burn-centre airway and ventilation |
| The associated trauma | The burn combined with the fracture, the head injury or the comorbidity |
| The comorbidity | The diabetes, the immunosuppression, the anticoagulation, the renal failure |
| The extremes of age | The child (under 10), the elderly (over 65), and the pregnant patient |
| The circumferential burn | The limb or the chest — the escharotomy risk |
Common pitfalls
The recurring errors are: not securing the airway early in the inhalation injury; underestimating the TBSA (counting the superficial); using the crystalloid instead of the Ringer's lactate; not titrating to the urine output; missing the compartment syndrome or the ventilatory compromise from the circumferential burn; cooling with ice (causes the frostbite); applying the silver sulfadiazine without cleaning; and not checking the carbon monoxide level.[17]
SAQ — Adult flame burn with inhalation injury
10 minutes · 10 marks
A 55-year-old man is rescued from a house fire. He has deep partial- and full-thickness burns to the face, the anterior chest and both arms (estimated 40 per cent TBSA), singed nasal hairs, carbonaceous sputum, and a hoarse voice. The oxygen saturation reads 99 per cent but he is confused and the carboxyhaemoglobin returns at 31 per cent.
SAQ — High-voltage electrical injury and the compartment syndrome
10 minutes · 10 marks
A 30-year-old electrician sustains an 11,000-volt contact injury to the right arm. There is a small entry wound on the right palm and a larger exit wound on the right forearm. The creatine kinase is 8,500 units per litre, the urine is dark, and the right forearm is tense and swollen with reduced finger movement.
Red flags
[17]References
- [1]Hsiao KH, et al. Adapted approaches to initial fluid management of patients with major burns. Burns Open, 2024.PMID 39540031
- [2]Jin WY, et al. Evidence for hydroxocobalamin in cyanide toxicity caused by smoke inhalation: a systematic review. Emergency Medicine International, 2025.PMID 41497958
- [3]Rossaint R, Bouillon B, Cerny V, et al. The European guideline on management of major bleeding and coagulopathy following trauma (fifth edition). Critical Care, 2023.PMID 36859355
- [4]Galvagno SM Jr, Nahmias JT, Young DA Advanced Trauma Life Support(®) Update 2019: Management and Applications for Adults and Special Populations. Anesthesiology clinics, 2019.PMID 30711226
- [5]Tejiram S, Romanowski KS, Palmieri TL Initial management of severe burn injury. Current opinion in critical care, 2019.PMID 31567292
- [6]Moore RA, Popowicz P, Burns B. Rule of nines. StatPearls, 2026.PMID 30020659
- [7]García-Ballesteros DI, Rivera-Martínez DDC, García-Pérez MM, et al. Evaluation and optimization of the Wallace rule of nines for the estimation of total body surface area burned. Journal of Emergency Medicine, 2023.PMID 37709577
- [8]Williams RY, Wohlgemuth SD. Does the 'rule of nines' apply to morbidly obese burn victims? Journal of Burn Care and Research, 2013.PMID 23702858
- [9]Borhani-Khomani K, Partoft S, Holmgaard R, et al. Assessment of burn size in obese adults; a literature review. Journal of Plastic Surgery and Hand Surgery, 2017.PMID 28417654
- [10]Giretzlehner M, Ganitzer I, Haller H, et al. Technical and medical aspects of burn size assessment and documentation. Medicina (Kaunas), 2021.PMID 33807630
- [11]Mehta M, Tudor GJ. Parkland formula. StatPearls, 2026.PMID 30725875
- [12]Dahl R, Galet C, Lilienthal M. Regional burn review: neither Parkland nor Brooke formulas reach 85% accuracy mark for burn resuscitation. Journal of Burn Care and Research, 2023.PMID 37010149
- [13]Alotaibi AM, Albulayhid NA, Aljabr KA, et al. The impact of resuscitation strategies on burn patient outcomes: Parkland vs. modified Brooke's formula. International Journal of Burns and Trauma, 2025.PMID 41278384
- [14]Shin JY, Yi HS. Diagnostic accuracy of laser Doppler imaging in burn depth assessment: systematic review and meta-analysis. Burns, 2016.PMID 27215151
- [15]Wang R, Zhao J, Zhang Z, et al. Diagnostic accuracy of laser Doppler imaging for the assessment of burn depth: a meta-analysis of 20 studies. Journal of Burn Care and Research, 2020.PMID 31872859
- [16]Foncerrada G, Culnan DM, Capek KD, et al. Inhalation injury in the burned patient. Annals of Plastic Surgery, 2018.PMID 29461292
- [17]Bittner EA, Sheridan R. Acute respiratory distress syndrome, mechanical ventilation, and inhalation injury in burn patients. Surgical Clinics of North America, 2023.PMID 37149380
- [18]Milton-Jones H, Soussi S, Davies R, et al. An international RAND/UCLA expert panel to determine the optimal diagnosis and management of inhalation injury in burn patients. Critical Care, 2023.PMID 38012797
- [19]Lee H, Rahul F, Makled B, et al. Cognitive task analysis of escharotomy. Military Medicine, 2023.PMID 37948234
- [20]Wang CF, Hughes PG. Escharotomy. StatPearls, 2026.PMID 29489153