EM · Paediatric trauma
Paediatric trauma
The paediatric trauma from the physiological differences to the modified primary survey with the weight-based resuscitation, the unique injury patterns (the head injury, the pulmonary contusion without the rib fracture, the abdominal injury), the Waddell triad, the SCIWORA, the Salter-Harris growth-plate fractures, the non-accidental injury (the TEN-4 BCDR bruising rule and the sentinel injuries), the PECARN head-injury rule, and the transfer to the paediatric trauma centre.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
The paediatric trauma differs from the adult trauma in the anatomy, the physiology, the psychology and the mechanism, and the emergency physician who applies the adult approach without the modification misses the injury and mismanages the resuscitation. The child has the proportionally larger head (more head injury), the compliant chest wall (the pulmonary contusion without the rib fracture), the proportionally larger solid organs (more abdominal injury), the smaller blood volume per kilogram (less reserve), the larger surface-area-to-mass ratio (more heat loss), and the developing skeleton (the growth-plate injury). The resuscitation is the weight-based, the vitals are the age-specific, and the non-accidental injury is always considered.[3]

The physiological differences
The child is not a small adult. The head is proportionally larger and heavier (the centre of gravity is higher), so the head injury is the commonest serious injury in the paediatric trauma. The blood volume is smaller per kilogram (80 millilitres per kilogram vs 70 in the adult) but the absolute volume is small (a 10-kilogram child has only 800 millilitres total — a 200 millilitre loss is a 25 per cent loss). The child compensates well through the tachycardia and the vasoconstriction, maintaining the blood pressure until the late decompensation — the hypotension is a late, pre-terminal sign. The chest wall is compliant (the ribs bend rather than break), so the significant intrathoracic injury may occur without the rib fracture. The abdominal organs are proportionally larger and less protected by the ribs and the musculature. The surface area is larger relative to the mass, so the child loses heat rapidly (the hypothermia worsens the acidosis and the coagulopathy).[3]
The Fellowship candidate must be able to recite the anatomical and physiological differences, because every modification of the adult primary survey flows from them. The open fontanelle and the unfused sutures of the infant allow the intracranial volume to expand before the pressure rises, so the infant with the raised intracranial pressure may show the bulging fontanelle, the increasing head circumference or the vomiting rather than the falling GCS — the classical Cushing response (the hypertension with the bradycardia and the irregular respiration) is a very late and often absent sign. The larynx is anterior and high, the tongue is proportionally large, the epiglottis is long and floppy (the U-shaped omega-shaped epiglottis of the infant), and the narrowest point of the paediatric airway is the cricoid cartilage (not the glottis, as in the adult) — this is the anatomical rationale for the uncuffed endotracheal tube and for the risk of the rapid obstruction at the subglottis by the oedema or the blood. The trachea is short, so the right main-bronchus intubation and the accidental extubation are separated by a few millimetres of tube movement. The developing skeleton has the open growth plates (the physis), so the forces that would sprain a ligament or dislocate a joint in the adult instead fracture through the growth plate in the child (the Salter-Harris fracture). The abdominal wall is thin and the musculature is underdeveloped, so the solid organs (the liver and the spleen) are exposed to the direct blow, and the bladder is intra-abdominal until the pelvis deepens in the early childhood.[3]
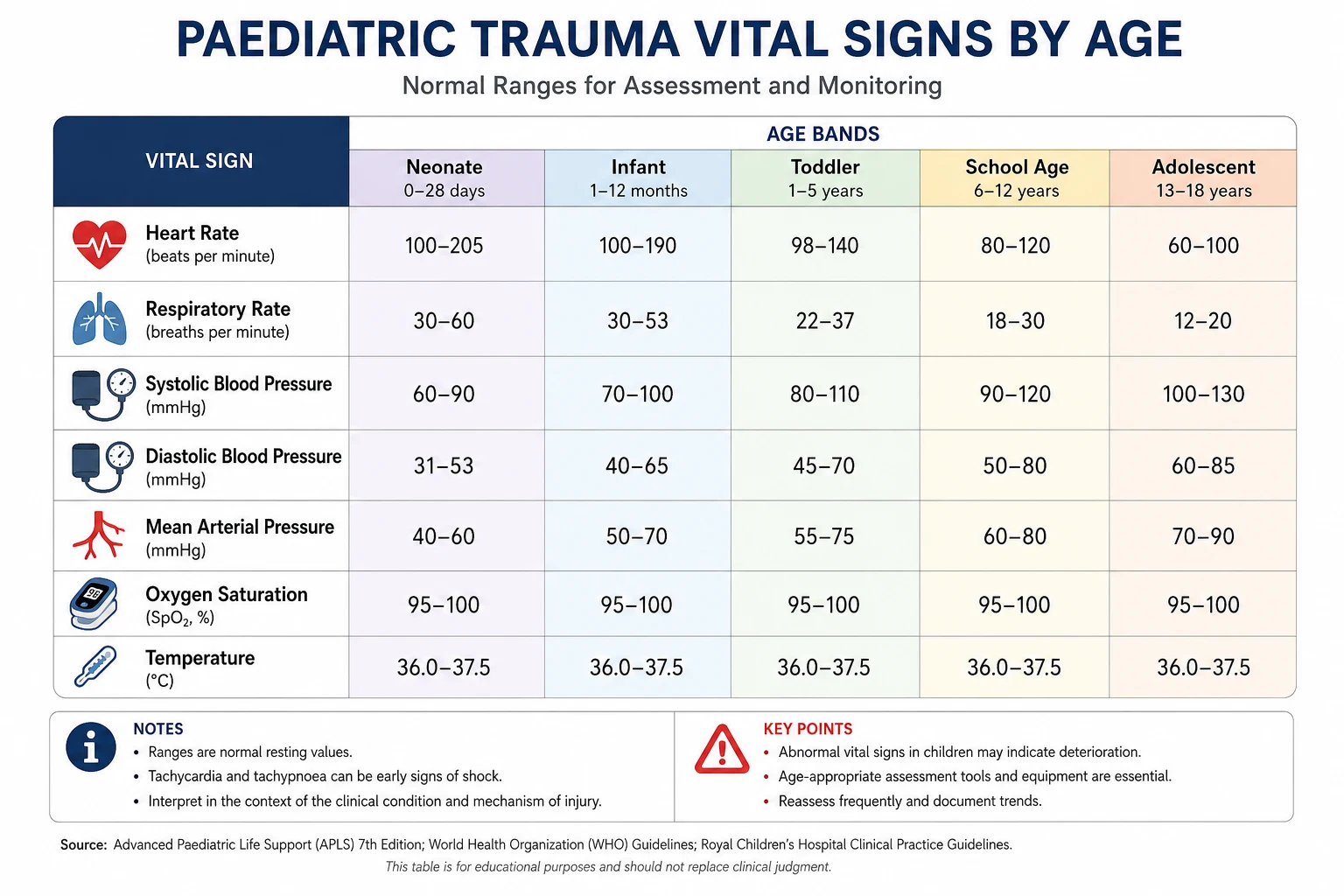
The age-specific vital signs
The single most common error in the paediatric trauma is applying the adult vital signs to the child. The normal heart rate of the resting adult (60 to 100 beats per minute) is the bradycardia for the infant and the toddler, and the normal adult blood pressure is the hypotension for the small child. Every drug, every fluid bolus and every interpretation of the shock is governed by the age, and the resus bay must display the age-appropriate ranges from the moment of the arrival.[3]
Neonate (<1 mo)
- HR 100 to 205 (median 140); SBP 60 to 90
- RR 30 to 60; cap refill <2 s
- A low HR or low BP is pre-terminal — resuscitate immediately
- Patent ductus, transitional circulation still possible
Infant (1–12 mo)
- HR 100 to 160; SBP 70 to 90
- RR 30 to 40; weight roughly 4 to 10 kg
- Blood volume only 80 mL/kg — a 5-kg infant has 400 mL total
- Tachycardia to 160 may be pain or fever or shock — investigate
Toddler (1–3 yr)
- HR 90 to 150; SBP 80 to 110
- RR 24 to 40; weight roughly 10 to 15 kg
- The mobile explorer — falls, ingestions, NAI peak
- Spleen and liver palpable — normal, not hepatosplenomegaly
Pre-school (3–5 yr)
- HR 80 to 140; SBP 80 to 110
- RR 22 to 34; weight roughly 14 to 18 kg
- Pedestrian-struck and the Waddell triad begin here
- Can localise pain — use the paediatric GCS reliably
School-age (6–12 yr)
- HR 70 to 120; SBP 80 to 120
- RR 18 to 30; weight roughly 20 to 40 kg
- Bicycle, sport and playground injuries dominate
- Cuff size matters — a small cuff falsely elevates the BP
Adolescent (13+ yr)
- HR 60 to 100; SBP 100 to 130 (approaches adult)
- RR 12 to 20; weight 40+ kg — adult drug doses apply
- Risk-taking, MVAs, intentional injury
- Consider pregnancy, substance use, and safeguarding
The primary survey modifications
The primary survey follows the C-A-B-C-D-E with the modifications. The weight is estimated (the Broselow tape or the formula) and the drug doses and the fluid volumes are calculated. The airway is managed with the awareness that the child's airway is anterior, the tongue is proportionally larger, the epiglottis is floppy, and the narrowest point is the cricoid (not the glottis) — the uncuffed tube is traditionally used for the under-8 child, though the cuffed tube is increasingly accepted with the careful cuff pressure monitoring. The breathing is assessed with the age-specific rate, and the tension pneumothorax is decompressed. The circulation is assessed with the awareness that the tachycardia and the prolonged capillary refill are the early signs; the fluid bolus is 10 to 20 millilitres per kilogram of the warmed crystalloid or the blood. The disability uses the paediatric GCS (or the AVPU). The exposure keeps the child warm — the temperature is monitored and the active warming is used.[3]
A — Airway and the paediatric airway differences
The paediatric airway has six features that change the intubation from the adult practice: the occiput is large (it flexes the neck and obstructs the airway when the child is supine — a shoulder roll restores the neutral sniffing position), the tongue is proportionally large (it fills the oral cavity and falls back), the larynx is high and anterior (C3 to C4 in the infant versus C6 in the adult), the epiglottis is long, floppy and angled (use the straight Miller blade to lift it directly), the cricoid is the narrowest point (not the glottis — the subglottic oedema closes the airway quickly), and the trachea is short (the tube that is correctly placed can slip into the right main bronchus with the head flexion, or extubate with the head extension). The pre-oxygenation, the careful tube sizing (the age-based formula: internal diameter in millimetres equals age in years divided by 4 plus 4; or the little-finger rule for the uncuffed tube), and the confirmation with the end-tidal capnography are the non-negotiables.[7]
[4] [3]C — Circulation, the weight-based bolus and the intraosseous access
The fluid bolus in the paediatric trauma is 10 to 20 millilitres per kilogram of the warmed isotonic crystalloid (the balanced crystalloid is preferred over the normal saline for the avoidance of the hyperchloraemic acidosis), given rapidly and reassessed. The child who does not improve after the second bolus is presumed to be bleeding, and the resuscitation switches to the blood products (the packed red cells, the plasma, the platelets in the weight-based ratio, or the whole blood) and the early source control — the crystalloid is not escalated beyond the second bolus. The FEAST trial taught the cautionary lesson that the aggressive fluid bolus is not harmless: in the children with the severe infection, the bolus increased the mortality, and the principle is extrapolated to the trauma — the bolus is targeted, reassessed and not given indiscriminately.[6]
When the intravenous access is difficult — and it is difficult in the shocked, the cold, the dark-skinned or the obese child — the intraosseous (IO) access is the rapid, reliable fallback, not the third or the fourth attempt at the peripheral cannula. The IO needle is placed in the proximal tibia (the flat anteromedial surface, 1 to 2 cm below the tibial tuberosity), the distal tibia, or the proximal humerus, and it delivers every drug, every fluid and every blood product at the same speed as the intravenous route. The pain of the infusion (the periosteal distension) is relieved with the lignocaine, and the complications (the extravasation, the fracture, the infection, the fat embolism) are rare when the technique is correct.[6]
[6]The Broselow tape and the weight estimation
The paediatric resuscitation fails when the weight is guessed — and the weight is guessed badly by the experienced clinician and the novice alike. The Broselow tape (the length-based tape) is laid alongside the child, and the colour-coded zone at the child's length gives the weight, the drug doses, the fluid volumes and the equipment sizes without the arithmetic. The tape was validated in the original Lubitz study and is the standard at the bedside of every paediatric resus bay.[7]
The age-based formula (the weight in kilograms equals twice the age plus ten, for the one- to ten-year-old) is the verbal alternative when the tape is unavailable, but it underestimates the weight in the modern, heavier child and overestimates it in the malnourished — the Broselow tape is the more accurate and the more rapid. The parental estimate (asking the carer) is surprisingly accurate for the known weight of the regular patient. The Broselow colour-coded system extends to the pre-packed drug drawers and the equipment trays, so the airway adjuncts, the laryngoscope blades, the endotracheal tubes, the suction catheters and the chest drains are pre-sized by the colour, and the team does not hunt for the right size in the heat of the resus.[7]
Estimating the weight and dosing the drugs at the bedside
Lay the Broselow tape
Place the child supine and lay the tape from the crown of the head to the heel. The red-to-grey colour zone at the child's heel length gives the estimated weight in kilograms. The same colour codes the pre-packed drug drawer and the equipment tray.
Use the age formula if no tape
Weight (kg) = (age in years × 2) + 8, or the simpler (age × 2) + 10 for the 1- to 10-year-old. This is a verbal fallback; the tape and the parental estimate are more accurate.
Calculate the dose by the weight
Fluid bolus 20 mL/kg; adrenaline 0.01 mg/kg (0.1 mL/kg of 1:10,000); TXA 15 mg/kg; cuffed ETT size (age/4) + 3.5 mm; defibrillation 4 J/kg. Every dose is per kilogram and checked by the second clinician.
Open the colour-coded tray
The Broselow colour at the child's length matches the pre-packed drawer — the ETT, the laryngoscope blade, the suction catheter, the intraosseous needle and the chest drain are all in the colour zone. No arithmetic, no hunting, no delay.
Reassess after every bolus
After each 20 mL/kg bolus, reassess the HR, the capillary refill, the perfusion and the mental state. The child who does not improve after the second bolus is bleeding — switch to blood products and pursue the source control.
The unique injury patterns
The head injury is the commonest serious paediatric injury (the large head, the thin skull), and the growing brain is more vulnerable to the diffuse injury. The pulmonary contusion without the rib fracture is the classic paediatric pattern (the compliant chest wall absorbs the energy without fracturing, but the underlying lung is injured). The abdominal injury is common (the proportionally larger solid organs, the less-protected abdomen) — the handlebar injury, the seat-belt sign. The Waddell triad (the femur fracture, the torso injury and the head injury) follows the pedestrian-struck mechanism (the child is struck, thrown onto the bonnet and then onto the road). The growth-plate (the Salter-Harris) fractures affect the developing skeleton.[3]
The pulmonary contusion and the elastic chest wall
The paediatric ribs are cartilaginous and elastic, and they bend rather than break — the energy of the impact is transmitted through the intact rib cage to the underlying lung, where it produces the alveolar-capillary disruption, the haemorrhage and the oedema of the pulmonary contusion. The chest radiograph at the arrival may be normal or show only the faint haziness, while the subsequent CT and the clinical course reveal the significant contusion. The child with the significant mechanism and the chest-wall blow is observed, oxygenated and monitored for the 24 to 48 hours, because the contusion ripens and the hypoxia worsens over the first day. The rib fractures, when they do occur in the child, signify a high-energy transfer and are associated with the significant underlying injury — the flail segment, the cardiac contusion, the great-vessel injury.[2]
[4]The Salter-Harris growth-plate fractures
The growth plate (the physis) is the cartilaginous zone at the end of the long bone, and it is the weakest point of the immature skeleton — the ligament and the tendon are stronger than the growth plate, so the force that sprains the adult joint fractures through the child's physis. The Salter-Harris classification grades the fracture by the involvement of the physis, the metaphysis and the epiphysis, and it predicts the prognosis: the higher the grade, the greater the risk of the growth disturbance and the premature fusion.[5]
SALTER-HARRIS — the growth-plate fracture grades, in order
SALTER
The fracture through the growth plate alone, separating the epiphysis from the metaphysis. Often radiographically occult; the child who will not bear weight after the injury has it until proven otherwise. Excellent prognosis.
The commonest (75 per cent); the fracture through the physis and up into the metaphysis, leaving a metaphyseal fragment (the Thurston-Holland sign). Good prognosis.
Through the physis and down through the epiphysis into the joint. Needs the anatomical reduction to restore the joint surface; intermediate risk of the growth arrest.
Through all three zones and into the joint. High risk of the premature growth arrest and the angular deformity; the orthopaedic urgency.
The compression injury of the growth plate, often radiographically normal at the presentation. Presents months later with the limb-length discrepancy or the angular deformity. The worst prognosis.
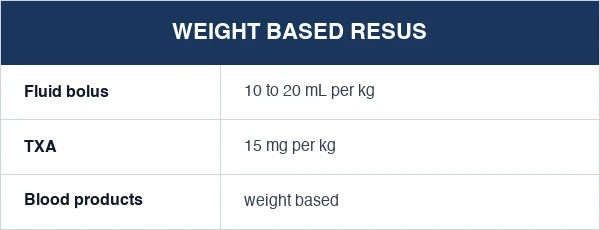
The weight-based resuscitation
The paediatric resuscitation is the weight-based: the fluid bolus (10 to 20 millilitres per kilogram of the warmed balanced crystalloid or the blood), the tranexamic acid (15 milligrams per kilogram, supported by the CRASH-2 evidence for the adult and the paediatric extension),[1][2] the blood products (the massive transfusion at the weight-based ratio), the adrenaline (0.01 milligrams per kilogram for the arrest), and the intubation drugs (all per kilogram). The Broselow tape or the length-based tape provides the rapid weight estimate and the dosing chart at the bedside. The permissive hypotension is less well-defined in the child — the child is resuscitated to the age-appropriate blood pressure rather than deliberately kept hypotensive (the evidence is extrapolated from the adult).[3]
The massive transfusion in the child follows the same principles as the adult — the early activation, the balanced ratio of the packed cells to the plasma to the platelets (the 1-to-1-to-1, scaled to the weight), the tranexamic acid within the three-hour window, the warming, the calcium replacement (the citrate chelation), and the minimisation of the crystalloid. The threshold for the activation is the physiological derangement and the anticipated bleeding, not the haemoglobin (which is the last to fall). The paediatric massive transfusion protocol delivers the weight-based packs (the 10-millilitre-per-kilogram red cells, the plasma and the platelets in the fixed ratio), and the O-negative blood is used until the crossmatched blood is ready.[2]
FEAST (Maitland, NEJM 2011) — fluid bolus in African children with severe infection
PECARN (Kuppermann, Lancet 2009) — children at very low risk of clinically-important brain injury
The SCIWORA
The Spinal Cord Injury Without Radiological Abnormality (SCIWORA) is the paediatric phenomenon — the ligamentous laxity of the cervical spine allows the spinal cord to be injured (the momentary subluxation, the distraction, the ischaemia) without the bony fracture on the imaging. The child with the neurological deficit after the trauma is assumed to have the spinal cord injury regardless of the normal imaging — the MRI is the definitive assessment. The immobilisation is maintained until the clinical or the MRI clearance.[3]
The SCIWORA is the diagnosis that distinguishes the paediatric from the adult cervical-spine practice. The adult cervical-spine injury is almost always accompanied by the bony fracture or the ligamentous disruption visible on the CT, and the clearance rests on the CT. The child under 8 has the elastic, ligamentous, horizontally-faceted cervical spine that allows the transient pathological motion — the flexion-extension, the distraction, the lateral tilt — that stretches or compresses the cord and then snaps back, leaving the normal CT and the injured cord. The high index of the suspicion is the operative principle: any child with the neck pain, the neurological symptom, the transient neurological deficit (the "stinger", the transient paralysis, the Lhermitte sign) or the dangerous mechanism is immobilised and imaged with the MRI, and the normal CT does not clear the spine.[4]
The cervical-spine clearance in the child under 8 years
Immobilise from the scene
The child is immobilised in the appropriately sized semi-rigid collar on the spinal board with the head blocks and the tape. The large occiput is accommodated by the occipital recess (the padded board) or the shoulder roll, so the cervical spine is neutral, not flexed.
Apply the high index of suspicion
Under 8 years, the ligamentous laxity and the horizontal facets allow the SCIWORA. Any neck pain, any focal neurological deficit, any transient neurological symptom, the dangerous mechanism (the high fall, the high-speed MVA, the diving injury) — the spine is not cleared clinically in these children.
Obtain the CT
The CT of the cervical spine identifies the bony injury and the gross malalignment. A normal CT does NOT exclude the SCIWORA — the ligamentous and the cord injury are not seen on the CT.
Obtain the MRI if any deficit or concern
The MRI is the definitive assessment for the cord, the ligament and the disc injury. The child with the persistent neurological deficit, the severe neck pain or the dangerous mechanism and the normal CT proceeds to the MRI before the collar is removed.
Clear clinically or by the MRI
The awake, cooperative, non-intoxicated child with no neck pain, no neurological deficit, no dangerous mechanism and a normal CT (and normal MRI if obtained) is cleared clinically — the collar is removed and the range of the motion assessed.
The non-accidental injury
The non-accidental injury (the inflicted injury, the child abuse) must be considered in every paediatric trauma, particularly when the history is inconsistent, the presentation is delayed, or the injuries are inconsistent with the developmental stage.[3][5] The red flags: the bruises in the non-mobile infant, the fractures of different ages, the retinal haemorrhages (the shaking injury), the rib fractures (the squeeze), the femur fracture in the non-walking child, the skull fracture from the short fall, and the intra-abdominal injury from the blunt blow. The inconsistent history, the changing history, and the delay in the presentation are the key triggers. The mandatory reporting is the legal obligation.
The sentinel injury is the seemingly minor injury in an infant (the bruise, the intra-oral injury, the femur fracture, the skull fracture) that, on the careful review, is inconsistent with the history and the developmental stage and that signals the abuse — the injury that, if investigated, would have prevented the subsequent, more serious injury. The TEN-4 BCDR is the validated clinical decision rule that quantifies the bruising concern: the bruising on the Torso, the Ear, or the Neck in a child 4 years or younger, or any bruising in a pre-cruising infant (less than 6 months or not yet rolling/crawling), is highly predictive of the abuse and triggers the full work-up.[5]
The TEN-4 BCDR — the bruising decision rule
The TEN-4 BCDR was derived and validated by Pierce and colleagues on the cohort of the children under 6 with the concern for the abuse. The rule is simple, memorable and high-yield: any bruising in the TEN region (the Torso, the Ear, the Neck), or any bruising in a pre-cruising infant, or any bruising in a child under 4 years that is not consistent with the history — these are the red-flag bruises that demand the skeletal survey, the coagulation screen, the head imaging and the child-protection referral.[5]
History red flags
- The history inconsistent with the injury or the developmental stage
- The changing or the evolving history between the informants
- The delay in the presentation beyond the reasonable explanation
- The unwitnessed injury in the pre-verbal child; the implausible mechanism
Bruising (TEN-4 BCDR)
- Bruising on the Torso, Ear or Neck in a child 4 yr or younger
- Any bruising in the pre-cruising infant (under 6 mo or not mobile)
- Bruises of different ages; patterned bruising (the hand, the belt, the ligature)
- The TEN-4 BCDR sensitivity 95.6% for abuse — high-yield and validated
Fracture red flags
- Rib fractures (esp. posterior) — the squeeze
- Femur fracture in the non-walking child
- Skull fracture from the short fall
- Fractures of different ages; the metaphyseal corner (classic metaphyseal lesion)
Internal injury
- Retinal haemorrhages (shaking — abusive head trauma)
- Intra-abdominal injury (liver, spleen, small bowel) from the blunt blow
- Duodenal haematoma — the delayed vomiting after the blow
- The death of an infant without the adequate explanation (SIDS vs abuse)
The paediatric GCS and the disability
The paediatric Glasgow Coma Scale modifies the adult verbal component for the pre-verbal child, because the infant cannot name the words or orient to the place. The paediatric GCS uses the age-appropriate motor commands (the spontaneous movement, the localisation of the pain, the withdrawal, the flexion, the extension) and the verbal alternatives (the coos and babbles, the irritable cry, the groans to pain, the no response). The eye opening and the motor components are largely preserved from the adult scale. The paediatric GCS is recorded at the arrival and after every significant intervention, and the trend is more informative than the absolute — the falling GCS signals the rising intracranial pressure and the expanding haematoma.[7]
The AVPU (Alert, responds to Voice, responds to Pain, Unresponsive) is the rapid alternative for the pre-hospital and the deteriorating child, and the rough correlation is the Alert equals the GCS 15, the Voice equals the GCS 13 to 14, the Pain equals the GCS 9 to 12, and the Unresponsive equals the GCS 8 or below — the Pain and the Unresponsive levels trigger the airway consideration. The blood glucose is checked in every child with the altered consciousness, because the hypoglycaemia is the rapidly reversible cause of the coma and the seizure, and the child with the TBI and the hypoglycaemia has the doubly threatened brain — the perfusion and the substrate.[7]
[8]Analgesia in the paediatric trauma
The pain of the paediatric trauma is systematically under-treated, and the under-treatment is the harm — the uncontrolled pain drives the catecholamine surge, the tachypnoea, the splinting and the atelectasis, and it impairs the assessment and the cooperation. The intranasal fentanyl (1.5 to 2 micrograms per kilogram, atomised into the nares) is the rapid, needle-free, opioid analgesic for the moderate-to-severe pain, with the onset within 5 to 10 minutes and the effect comparable to the intravenous morphine.[8] It is the first analgesic in the child with the pain and the difficult access, and it bridges the gap to the definitive intravenous analgesia.
The intravenous morphine (0.1 to 0.2 milligrams per kilogram) and the intranasal ketamine (the dissociative analgesia for the painful procedures) are the alternatives. The paracetamol (15 milligrams per kilogram orally or intravenously) and the ibuprofen (10 milligrams per kilogram orally, in the absence of the bleeding and the renal concern) are the foundational non-opioid analgesics. The procedural sedation (the ketamine 4 milligrams per kilogram intramuscularly or 1 to 1.5 milligrams per kilogram intravenously) is the option for the fracture reduction and the wound repair in the trained and the monitored setting. The regional analgesia (the fascia-iliaca block for the femur fracture) is the opioid-sparing adjunct that the modern trauma service delivers early.[8]
Borland (Emerg Med Australas 2011) — intranasal fentanyl for paediatric analgesia
The hypothermia prevention
The child loses heat rapidly — the large surface-area-to-mass ratio, the thin subcutaneous fat and the limited thermoregulatory reserve conspire to drop the core temperature during the exposure, the resuscitation and the transfer. The hypothermia is not the benign inconvenience; it is the arm of the lethal triad (the hypothermia, the acidosis and the coagulopathy) that worsens the outcome of the trauma, and it disables the coagulation cascade at every step. The active warming is the non-negotiable from the first minute: the wet clothes are removed, the warmed blanket and the forced-air warmer are applied, the fluids and the blood products are warmed, and the ambient temperature of the resus bay is raised. The core temperature (not the peripheral) is monitored, and the target is the normothermia, the 36 to 37 degrees Celsius.[1]
[1]The trauma team activation criteria in the paediatric patient
The paediatric trauma team activation uses the same physiological, anatomical and mechanistic framework as the adult, but the physiological thresholds are the age-adjusted and the mechanism is weighted for the paediatric vulnerability. The deliberate over-triage is the principle: it is better to call the team for the child who turns out to be minimally injured than to under-call and discover the deteriorating child alone in the resus bay. The paediatric-specific criteria include the age-adjusted hypotension (the SBP below the fifth percentile for the age, roughly 70 plus twice the age in years), the paediatric trauma score below 11, the GCS below 13, and the dangerous mechanism in the small child (the fall from the twice-the-height, the high-speed MVA, the pedestrian struck, the bicycle handlebar).[3]
[3]The transfer to the paediatric trauma centre
The definitive care of the major paediatric trauma is the paediatric trauma centre, and the decision to transfer is made early, at the first recognition of the injury severity or the limitation of the local resources. The transfer is not the failure of the receiving hospital — it is the correct routing of the child to the centre with the paediatric intensive care, the paediatric surgery, the paediatric anaesthesia and the paediatric radiology. The pre-transfer packaging secures the airway, the lines, the monitors and the ventilation before the move; the child is transferred by the appropriately skilled team (the paediatric retrieval service where available); and the receiving centre is contacted early for the acceptance, the bed and the handover.[1]
[2]The differential diagnosis — separating the traumatic from the medical
- The accidental vs the non-accidental injury — the bruise, the fracture or the head injury in the pre-mobile or the pre-verbal child is the non-accidental injury until the consistent history, the consistent mechanism and the consistent developmental stage are confirmed. The TEN-4 BCDR bruising, the femur fracture in the non-walker, the posterior rib fractures and the retinal haemorrhages are the high-specificity markers that demand the full child-protection work-up.
- The traumatic brain injury vs the medical collapse — the child found unconscious at the scene of the minor or the no apparent trauma may have the primary medical event (the hypoglycaemia, the seizure, the arrhythmia, the intracranial haemorrhage from the arteriovenous malformation or the aneurysm) that caused the fall, rather than the fall that caused the brain injury. The blood glucose, the ECG, the CT and the careful history distinguish the primary traumatic from the primary medical, because both may coexist.
- The pulmonary contusion vs the aspiration and the pneumonia — the hypoxia and the infiltrate after the chest trauma may be the contusion, but the aspiration of the gastric content at the scene or the early post-traumatic pneumonia produces the same radiograph. The mechanism, the distribution (the contusion under the point of the impact, the aspiration in the dependent segments), the white-cell count and the evolution over the 24 to 48 hours distinguish them, and the management is the supportive ventilation and the oxygenation in both.
- The intra-abdominal injury vs the minor abdominal wall contusion — the handlebar injury and the seat-belt sign mark the high risk of the hollow-viscus and the solid-organ injury, but the child with the superficial bruise and the benign abdomen may be observed. The CT with the intravenous contrast is the definitive assessment; the FAST is the rapid but insensitive screen; the serial examination and the haemoglobin trend catch the evolving injury.
- The SCIWORA vs the spinal cord lesion of the medical cause — the child with the acute paraparesis after the trauma has the SCIWORA until the MRI proves otherwise, but the transverse myelitis, the spinal-cord infarction and the arteriovenous malformation present similarly without the trauma. The history, the MRI and the cerebrospinal-fluid analysis distinguish them, and the immobilisation is maintained until the assessment is complete.[4]
The ATLS paediatric modifications — the summary
The Advanced Trauma Life Support course codifies the paediatric modifications, and the Fellowship candidate must recite them. The weight is estimated (the Broselow tape, the length-based tape, the age formula) and every dose is calculated per kilogram. The airway uses the straight-blade laryngoscopy, the uncuffed (or the carefully cuffed) tube, the shoulder roll, and the early intubation for the GCS of 8 or below. The breathing uses the age-specific rates and the paediatric-sized equipment. The circulation uses the 10-to-20-millilitre-per-kilogram bolus, the intraosseous access after the failed intravenous attempt, and the blood products for the non-responder. The disability uses the paediatric GCS and the blood glucose. The exposure keeps the child warm. The cervical spine in the under-8 child is managed with the high index of the suspicion and the awareness of the SCIWORA. The non-accidental injury is considered in every child, and the transfer to the paediatric trauma centre is arranged early for the definitive care.[3]
ATLS paediatric — the seven modifications in one breath
PAEDTXA
The age-specific HR, RR and BP — a child's 'normal adult' HR is the bradycardia of the late shock. Display the ranges from the arrival.
The anterior high larynx, the large tongue, the floppy epiglottis, the cricoid as the narrowest point. Straight blade, uncuffed (or monitored cuffed) tube, shoulder roll.
The Broselow tape — the weight, the drug doses, the fluid volumes and the equipment sizes from the single colour zone at the child's length. No arithmetic in the resus bay.
Fluid 20 mL/kg, adrenaline 0.01 mg/kg, TXA 15 mg/kg, defib 4 J/kg. Every dose checked by the second clinician. IO access after the failed IV.
The large surface-area-to-mass ratio loses heat fast. Warmed fluids, forced-air warmer, raised ambient temperature, remove the wet clothes. Normothermia is the target.
The under-8 cervical spine — the high index of the suspicion, the normal CT does not exclude the SCIWORA, the MRI for the deficit or the concern. Large occiput on the padded board.
The non-accidental injury in every child — the TEN-4 BCDR bruising, the sentinel injury, the fractures of different ages, the inconsistent history. Mandatory reporting.
Common pitfalls
The recurring errors are: applying the adult vitals to the child (the normal adult HR is the bradycardia for a child); underestimating the blood loss (the small absolute volume); accepting the hypotension as the first sign (it is late); missing the pulmonary contusion without the rib fracture; not considering the non-accidental injury; the hypothermia from the prolonged exposure; the repeated peripheral cannulation when the intraosseous access is the faster route; clearing the under-8 cervical spine on the CT alone and missing the SCIWORA; under-treating the pain and the anxiety; treating the fluid bolus as harmless and missing the FEAST lesson; failing to call the trauma team or the paediatric retrieval early; and not estimating the weight with the Broselow tape and guessing the dose.[7]
[7] [7] [4]Exam practice
SAQ — The pedestrian-struck child with the Waddell triad
10 minutes · 10 marks
A 6-year-old boy is brought to the trauma bay 30 minutes after being struck by a car at 40 km/h while crossing the road. He was thrown approximately 3 metres. On arrival he is crying but consolable, GCS 14 (irritable), HR 150, BP 95/60, RR 32, SpO2 94 per cent on room air. There is a deformed and shortened right thigh (a closed femur fracture), decreased breath sounds on the left with the bruising over the left flank, and a 2-cm laceration on the right temporal region. The abdomen is tender in the left upper quadrant. The weight is estimated at 22 kg by the Broselow tape.
SAQ — The non-accidental injury and the TEN-4 BCDR bruising rule
10 minutes · 10 marks
A 14-month-old girl is brought to the emergency department by her mother with the history that she 'rolled off the change table' 2 hours ago. On examination she is GCS 15, alert and interactive, with the bruises on the right ear, the left flank and the back. There is a faint bruise on the abdomen. The mother reports no other injuries. The developmental history is that she is not yet walking. The skeletal survey is booked.
Red flags
[5]References
- [1]Rossaint R, Bouillon B, Cerny V, et al. The European guideline on management of major bleeding and coagulopathy following trauma (fifth edition). Critical Care, 2023.PMID 36859355
- [2]CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2). Lancet, 2010.PMID 20554319
- [3]Guyther J, Wiltjer R Pediatric Trauma. Emergency medicine clinics of North America, 2023.PMID 36424042
- [4]Kuppermann N, Holmes JF, Dayan PS, et al.; Pediatric Emergency Care Applied Research Network (PECARN). Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet, 2009.PMID 19758692
- [5]Pierce MC, Kaczor K, Acker D, et al. Validation of a clinical decision rule to predict abuse in young children based on bruising characteristics (TEN-4 BCDR). JAMA Network Open, 2021.PMID 33852003
- [6]Maitland K, Kiguli S, Opoka RO, et al. (FEAST trial). Mortality after fluid bolus in African children with severe infection. New England Journal of Medicine, 2011.PMID 21615299
- [7]Lubitz DS, Seidel JS, Chameides L, Luten RC, Zaritsky AL, Campbell FW. A rapid method for estimating weight and resuscitation drug dosages from length in the pediatric age group. Annals of Emergency Medicine, 1988.PMID 3377285
- [8]Borland M, Esson A, Babl F, et al. Equivalency of two concentrations of fentanyl administered by the intranasal route for acute analgesia in children in a paediatric emergency department. Emergency Medicine Australasia, 2011.PMID 21489168