EM · Upper airway obstruction
Upper airway obstruction in the emergency department
Also known as Airway obstruction · Stridor · Epiglottitis · Angioedema airway
Upper airway obstruction — the stridor and drooling presentations, the infectious causes (epiglottitis, retropharyngeal abscess, Ludwig's angina, croup) and the non-infectious (angioedema, anaphylaxis, foreign body, burn, malignancy), the Poiseuille law rationale (r to the fourth power), the golden rules (do not agitate the suspected epiglottitis; call the senior anaesthetist and ENT immediately), the cause-specific management with doses (nebulised adrenaline, ceftriaxone, dexamethasone, icatibant), and the can't-intubate-can't-oxygenate rescue (the scalpel-bougie-tube cricothyroidotomy). ACEM-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Upper airway obstruction is one of the few true emergencies in which seconds determine the outcome, and it is the condition that tests the Fellowship candidate's discipline most: the instinct to examine and investigate must be overridden by the principle of not agitating a precarious airway, the senior help must be summoned before it is needed, and the front-of-neck access must be prepared before the patient arrests. The causes range from the infectious to the allergic to the traumatic, but the framework — recognise, don't agitate, call for help, secure the airway — applies to all.[1][2]
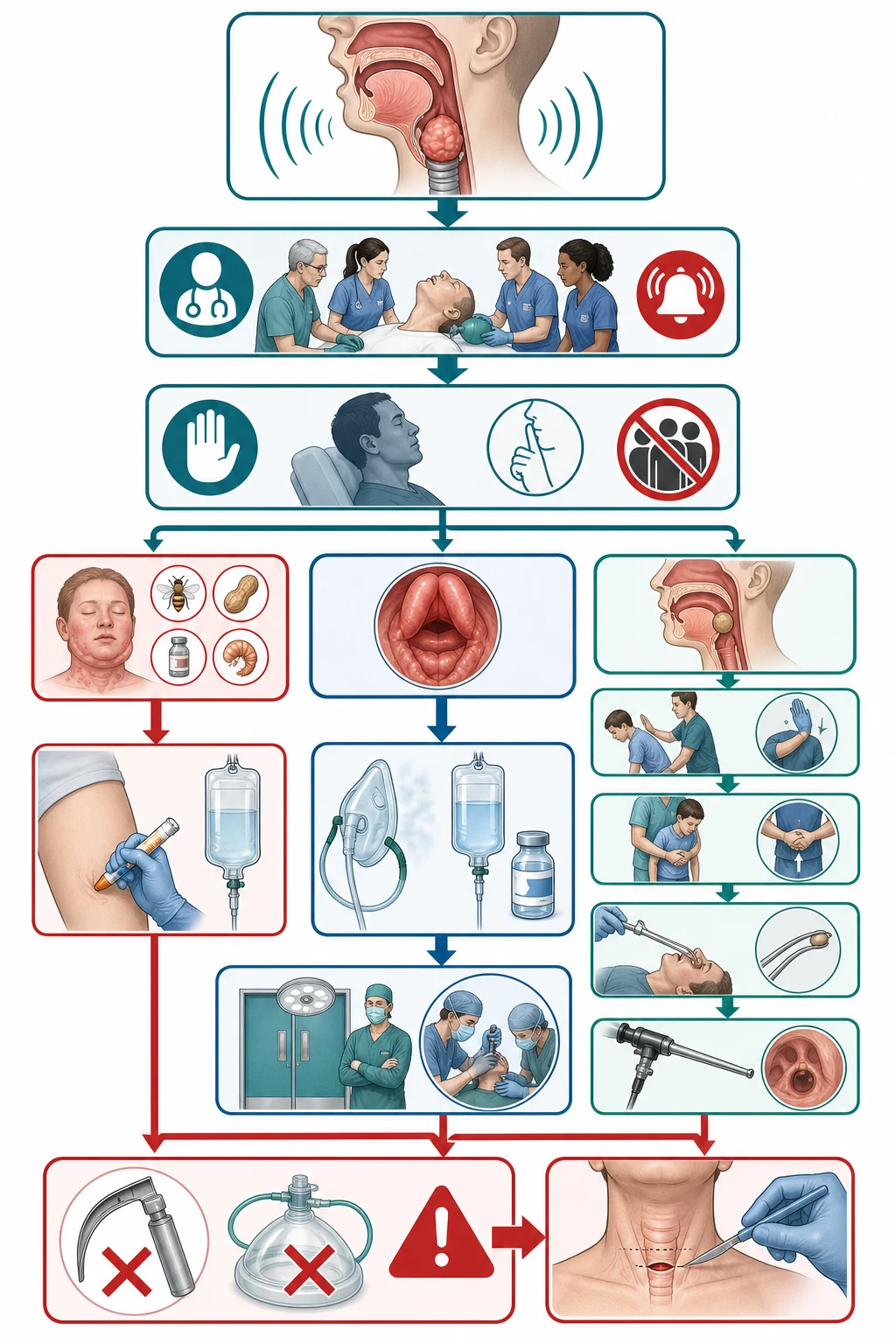
The framework — recognise, don't agitate, call, secure
The single most important principle is that the patient with a threatened upper airway is balanced on a knife edge, and the wrong intervention — a tongue depressor, a lie-flat, an upset child or adult — can tip them into a complete obstruction and an arrest. The Fellowship candidate must recognise the stridor at rest, the drooling, the tripod posture, the exhaustion, and the drowsiness as the signs of a critical narrowing, and then apply the framework: summon the senior anaesthetist and the ENT or the maxillofacial surgeon at once; keep the patient in their chosen position; do not examine the throat of the suspected epiglottitis; give the humidified oxygen; and prepare the difficult-airway equipment (the videolaryngoscope, the flexible scope, and the scalpel-bougie-tube for the front-of-neck access) from the first minute.[3]
Why a small narrowing is a big problem — Poiseuille's law
The airflow through a tube is proportional to the fourth power of the radius (Poiseuille's law), so a 50 per cent reduction in the airway radius reduces the flow by a factor of sixteen (0.5 to the fourth power is 0.0625). This is why a small reduction in the upper-airway radius from an oedema or a swelling produces a disproportionate and a rapidly escalating work of breathing, and why the paediatric airway — already narrower than the adult's — is so much more dangerous for the same degree of swelling. It is also why the stridor at rest is the sign that the airway is critically narrowed: the patient can no longer generate enough flow to overcome the resistance without the maximal effort, and the next step is the exhaustion and the obstruction.[3]
[4]The stridor and its level — inspiratory, biphasic, expiratory
The character and the phase of the stridor localises the level of the obstruction with a reliability that the Fellowship candidate must be able to apply at the bedside, because the level directs both the investigation (the nasendoscopy vs the bronchoscopy) and the definitive-airway plan. The stridor is generated when a high-velocity turbulent airflow passes through a narrowed segment — it is the audible equivalent of the Poiseuille collapse. The phase depends on where in the respiratory cycle the airway is dynamically narrowed:[3]
Inspiratory stridor
- Localises to the SUPRAGLOTTIC / extrathoracic upper airway (nose, nasopharynx, oropharynx, supraglottis)
- Extrathoracic airway narrows on INSPIRATION (negative intrathoracic pressure sucks the floppy supraglottic tissues inward)
- Causes: epiglottitis, supraglottitis, severe croup, peritonsillar/retropharyngeal abscess, Ludwig's angina, angioedema of the tongue and supraglottis
- Soft, wet, crowing quality — worsens with agitation and supine posture
Biphasic stridor
- Localises to the GLOTTIC / subglottic FIXED lesion (the larynx proper or the immediate subglottis)
- Heard in BOTH inspiration and expiration because the fixed narrowing limits flow in both directions
- Causes: laryngeal foreign body, bilateral vocal cord palsy, laryngeal tumour, subglottic stenosis (post-intubation), severe croup with subglottic oedema
- Often louder and harsher than the pure inspiratory; signals a critical, fixed narrowing
Expiratory stridor
- Localises to the INFRAGLOTTIC / intrathoracic airway (lower trachea, carina, main bronchi)
- Intrathoracic airway is compressed on EXPIRATION by the positive intrathoracic pressure
- Causes: tracheal foreign body, tracheal tumour, extrinsic tracheal compression (retrosternal goitre, vascular ring, mediastinal mass), tracheomalacia
- May be mistaken for wheeze — but is monophonic and fixed, unlike the polyphonic asthmatic wheeze
The other bedside signs that quantify the threat
Beyond the stridor phase, the Fellowship candidate must grade the threat from a small set of bedside signs that the airway is failing. The tripod posture — the patient sitting forward, bracing the hands on the knees or the bed, and extending the neck — splints the upper airway open by recruiting the accessory muscles and extending the oropharyngeal axis; abandoning it (lying flat for a scan) is a recognised precipitant of the complete obstruction and the arrest. The drooling is the objective sign that the patient cannot swallow their own secretions — it is the hallmark of the epiglottitis and the deep neck space infection, and it is rarely seen in the angioedema or the croup. The muffled "hot potato" voice (as if speaking with a hot potato in the mouth) is the acoustic fingerprint of the oropharyngeal and the supraglottic swelling (the peritonsillar abscess, the epiglottitis, the Ludwig's); a hoarse voice points to the larynx itself (the vocal cord lesion, the post-intubation oedema). The progression from the stridor with effort to the stridor at rest to the silent chest (the loss of the stridor as the patient tires and the flow falls below the threshold that generates the sound) to the drowsiness is the trajectory of the failing airway, and it is the indication to secure the airway before the silent chest becomes the arrest.[3]
[3]Tripod / sniffing posture
- Sitting forward, hands on knees, neck extended
- Recruits accessory muscles; splints the upper airway open
- Do NOT force the patient supine for cannulation or imaging
- Abandoning the posture predicts complete obstruction
Drooling
- Cannot swallow saliva; spit pool in the floor of mouth
- Hallmark of epiglottitis, retropharyngeal abscess, Ludwig's
- Rarely prominent in angioedema or croup
- Combined with fever and toxicity = the infected airway triad
"Hot potato" voice
- Muffled, as if a hot potato in the mouth
- Localises to the OROPHARYNGEAL / SUPRAGLOTTIC swelling
- Peritonsillar abscess, epiglottitis, Ludwig's
- A hoarse voice → think larynx (vocal cord) not oropharynx
Tracheal tug / accessory muscle use
- Sternal notch retraction on inspiration; severe work of breathing
- Marks the critical narrowing with the maximal effort
- The next step is exhaustion, then silent chest, then arrest
- Pre-oxygenase, call the team, prepare the FONA
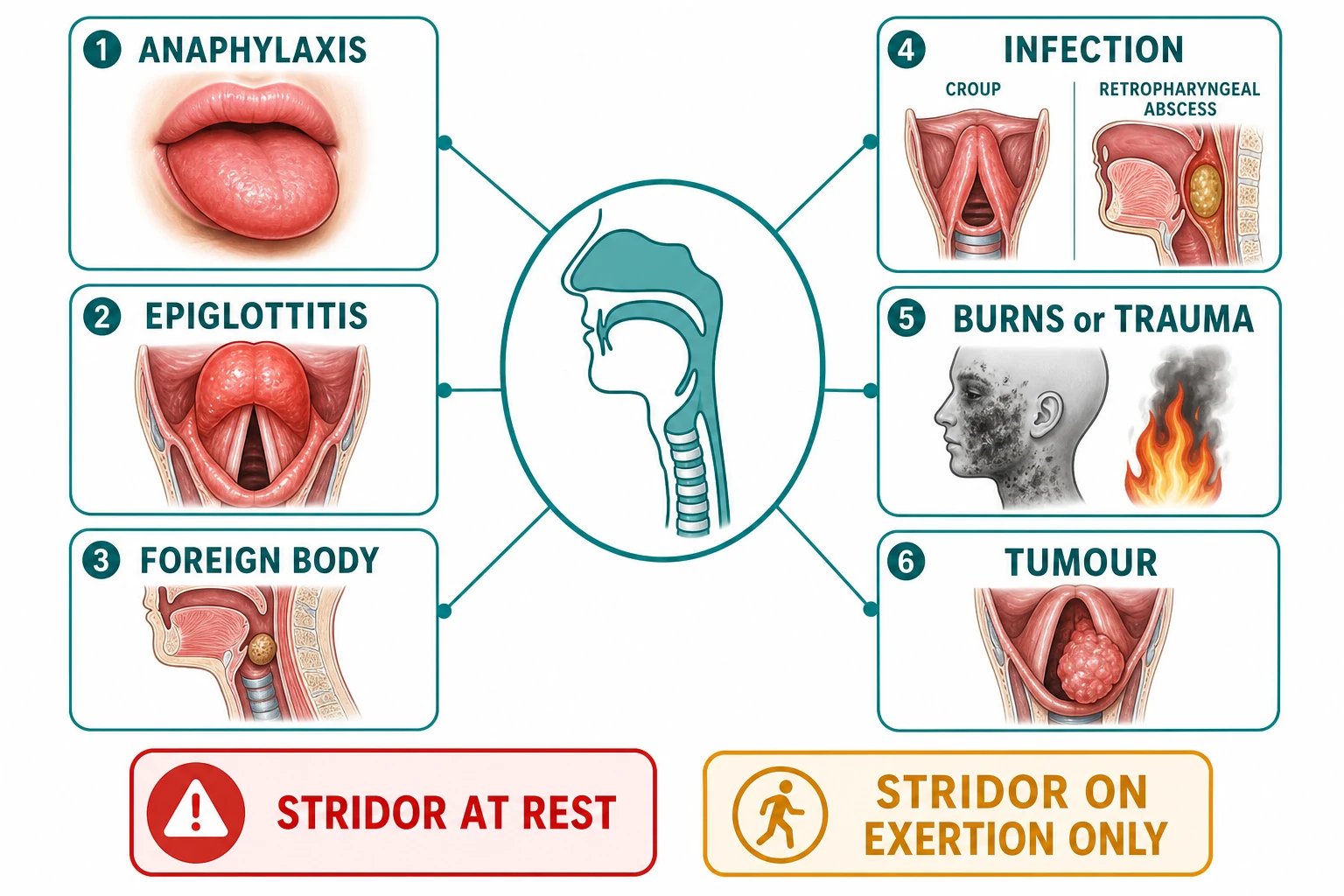
Differential diagnosis — the causes
The causes of the upper airway obstruction are grouped into the infectious and the non-infectious, and the identification of the cause guides the specific therapy alongside the airway framework.[3]
Epiglottitis
- Septic, rapid; drooling, can't swallow, tripod posture
- Fever, toxic; the "thumb sign" on the lateral neck
- DON'T examine the throat → call ENT + anaesthetics → theatre
- Ceftriaxone 2 g IV + dexamethasone 8 mg after airway secured
Angioedema (ACE-i)
- Lip/tongue/face swelling; ACE inhibitor cause
- Bradykinin-mediated — adrenaline may NOT work
- Nebulised adrenaline 1:1000 5 mL; icatibant; prepare FONA
- Stop the ACE inhibitor permanently
Foreign body
- Sudden onset; choking history (children, impaired swallow)
- Back blows / Heimlich if conscious; if unconscious → FONA
- May need direct laryngoscopy / Magill forceps
- Paeds → paediatric anaesthetist + ENT
Anaphylaxis / burn / Ludwig's
- Anaphylaxis: multi-system, urticaria → IM adrenaline 500 mcg
- Burn/inhalation: early intubation before the oedema closes
- Ludwig's: bilateral submandibular cellulitis, trismus → dental origin
- Each has its specific pathway
The infectious causes
The acute epiglottitis (or the supraglottitis) is the most dangerous of the infectious causes, and the one that most tests the discipline of not agitating. The adult patient presents with a fever, a toxicity, a severe sore throat, a drooling, an inability to swallow the secretions, a muffled voice, and a tripod posture (sitting forward and extending the neck to open the airway). The stridor may be soft or absent until the obstruction is nearly complete. The lateral neck radiograph shows the swollen epiglottis as the "thumb sign", but the investigation must NOT be performed before the airway is secured or in the process of being secured by the senior team. The management is the inhalational induction and the intubation by a senior anaesthetist in the theatre, with the ENT surgeon scrubbed and ready for the front-of-neck access; the ceftriaxone 2 g intravenously and the dexamethasone 8 mg are given after the airway is secured.[1]
The retropharyngeal abscess presents with a neck stiffness, a dysphagia, a fever and a toxicity; the CT (if the airway is safe) shows the collection; the management is the surgical drainage by the ENT and the intravenous antibiotics. The Ludwig's angina is a bilateral submandibular cellulitis from a dental infection, with a floor-of-mouth swelling, a tongue elevation, a trismus and a drooling; the airway may be extremely difficult and the management is the early definitive airway and the surgical decompression. The croup (paediatric) presents with a barky cough, a stridor and a fever, and is managed with the nebulised adrenaline and the dexamethasone.[3]
The non-infectious causes
The angioedema of the ACE inhibitor is the increasing cause of the adult upper airway obstruction. It is bradykinin-mediated, not histamine-mediated, which is why the intramuscular adrenaline — the cornerstone of the anaphylaxis algorithm — may not work: the swelling is driven by the bradykinin, not the histamine. The management is the nebulised adrenaline 1:1000 in 5 mL (to reduce the mucosal oedema by the alpha-1 vasoconstriction), the icatibant (a bradykinin B2 receptor antagonist, specific for the hereditary and the ACE-inhibitor angioedema), the intravenous adrenaline if the airway is closing, and the permanent cessation of the ACE inhibitor. The airway team must be warned and the front-of-neck access prepared, because the swelling can progress to a complete obstruction within hours.[2]
The anaphylaxis with the upper airway obstruction is managed with the intramuscular adrenaline 500 micrograms into the anterolateral thigh, repeated every five minutes as needed, with the full anaphylaxis algorithm (the oxygen, the fluid, the chlorphenamine, the hydrocortisone, the positioning). The foreign body obstruction is managed with the back blows and the Heimlich manoeuvre if the patient is conscious, and with the direct laryngoscopy and the Magill forceps (or the FONA if unconscious and unventilatable). The burn or the inhalation injury produces a progressive airway oedema that may close the airway within hours — the early intubation, before the oedema makes it impossible, is the principle.[3]
Ludwig's angina — the cellulitis that elevates and displaces the tongue
Ludwig's angina is a rapidly spreading, bilateral cellulitis of the submandibular, sublingual and submental spaces — a polymicrobial infection (streptococci, oral anaerobes, Prevotella, Fusobacterium) seeded from an apical dental abscess, most often the second or third mandibular molar whose roots project below the mylohyoid line into the submandibular space. The defining anatomy is that the infection is a bilateral, board-hard woody induration of the floor of the mouth with no fluctuance (it is a cellulitis, not a drainable abscess until late), and the pathognomonic physical sign is the elevation and posterior displacement of the tongue — the swollen sublingual space pushes the tongue up and back, and the tongue base then obstructs the supraglottic inlet. The patient is febrile, toxic, drooling, with marked trismus, a muffled "hot potato" voice, and severe dysphagia; the stridor may be subtle until the obstruction is nearly complete, because the tongue displacement worsens with lying flat.[5]
[3]The diagnosis is clinical; the contrast CT of the neck (only in a patient whose airway is safe or accompanied by the airway team) confirms the spreading cellulitis, identifies drainable collections, and localises the dental source. The management is the early definitive airway (most require intubation or a tracheostomy), the broad-spectrum intravenous antibiotics (co-amoxiclav 1.2 g, or ampicillin-sulbactam, or clindamycin if penicillin-allergic, covering oral anaerobes), and the surgical source control — the extraction of the offending tooth and the drainage of any collection. The dexamethasone 8 mg intravenously is given to reduce the oedema. The mortality, historically as high as 50 per cent, is now below 10 per cent with modern airway management and antibiotics, but the airway death remains the failure mode.[3]
Ludwig's angina
- Bilateral submandibular + sublingual cellulitis from a mandibular molar
- Woody, board-hard floor of mouth — NOT fluctuant
- Tongue elevated and displaced posteriorly
- Do NOT lay flat; upright posture, theatre, FONA ready
Peritonsillar abscess (quinsy)
- Unilateral peritonsillar collection; Uvula pushed to the opposite side
- Trismus, "hot potato" voice, severe odynophagia
- Fluctuant — drainable with needle aspiration or incision
- Airway threat is lower; drainage + antibiotics usually suffice
Retropharyngeal abscess
- Collection in the retropharyngeal space (nodes in children, foreign body/spread in adults)
- Stiff neck, dysphagia, refusal to move the neck
- Widened prevertebral soft tissue on lateral neck X-ray
- CT to confirm; surgical drainage + IV antibiotics
Peritonsillar vs Ludwig's — the discriminator
- Quinsy is UNILATERAL and the uvula is pushed across
- Ludwig's is BILATERAL and the floor of mouth is swollen
- Quinsy is usually drainable in the ED
- Ludwig's is a theatre airway — do not instrument in the ED
Acute epiglottitis in detail — the "thumb sign" and the discipline of not looking
The acute epiglottitis (supraglottitis in the adult) is a Haemophilus influenzae type b (and, in the vaccine era, increasingly streptococcal and staphylococcal) cellulitis of the supraglottic structures — the epiglottis, the aryepiglottic folds, the arytenoids. The swollen, oedematous epiglottis classically has the appearance of a large, red, cherry that prolapses posteriorly over the glottic inlet like a ball valve. The presentation is the abrupt onset (hours, not days) of a severe sore throat (often disproportionate to the oropharyngeal appearance — the throat looks normal), a high fever and toxicity, a muffled voice, drooling, and a preference for the tripod (sniffing) posture — sitting forward with the neck extended to splint the airway open. The stridor is a late and ominous sign in the adult, signalling that the obstruction is nearly complete.[1]
[1]The management is the discipline of not agitating the airway: no tongue depressor, no oropharyngeal examination, no lying flat, no upsetting cannulation in the frightened child, no sending to radiography unaccompanied. Summon the senior anaesthetist and the ENT surgeon immediately; transfer to theatre; perform an inhalational (sevoflurane) induction with the patient sitting upright, maintaining spontaneous ventilation, with the ENT surgeon gowned and scrubbed and a rigid bronchoscope and a tracheostomy set opened at the head of the table. After the airway is secured, give ceftriaxone 2 g intravenously (or cefotaxime — to cover Hib and the streptococci) and dexamethasone 8 mg intravenously to reduce the oedema. Take blood cultures before the antibiotic. Epiglottitis is one of the few conditions in which the wrong move — the tongue depressor — can convert a precarious airway into an arrest within seconds.[1]
[1] [1]Suspected epiglottitis — the operational sequence
Recognise the triad: severe sore throat disproportionate to the oropharyngeal appearance, drooling, difficulty swallowing secretions — plus fever, toxicity, muffled voice, tripod posture
Do NOT agitate: no tongue depressor, no oropharyngeal exam, no lying flat, no upsetting cannulation in the frightened child
Call for help EARLY: senior anaesthetist + ENT surgeon summoned to the bedside immediately; do not wait for deterioration
Keep the patient upright in the tripod / sniffing posture; give humidified oxygen; do not force the cannulation if it upsets the patient
In the stable cooperative ADULT: a calm flexible nasendoscopy by a senior, sitting upright, confirms the swollen cherry-red epiglottis
Transfer to theatre with the airway team; inhalational sevoflurane induction, upright, spontaneous ventilation maintained
ENT surgeon scrubbed, rigid bronchoscope and tracheostomy set ready at the head of the bed for the front-of-neck access
After the airway is secured: ceftriaxone 2 g IV (after blood cultures), dexamethasone 8 mg IV; admit to ICU for the extubation plan
Retropharyngeal abscess — the stiff neck and the swallow that fails
The retropharyngeal space lies between the buccopharyngeal fascia anteriorly and the prevertebral fascia posteriorly, extending from the skull base down to the level of T1/T2 in the superior mediastinum — a route by which a retropharyngeal infection can track into the danger space and the mediastinum, producing a life-threatening descending necrotising mediastinitis. In children under four, the retropharyngeal lymph nodes (of Henle) seed from an upper respiratory infection and suppurate; in adults, the causes are a penetrating injury (a fish bone, a foreign body, a procedural perforation), a spread from a neighbouring deep neck space, or, increasingly, intravenous drug use and immunocompromise. The presentation is a fever, a dysphagia, an odynophagia, a stiff neck (torticollis) and a refusal to extend the neck, a muffled voice, and — in the child — a reluctance to move and a stridor. The drooling and the stridor appear with the larger collections.[4]
The lateral neck radiograph (in a patient in whom it is safe, taken in true lateral with full inspiration and the neck extended to avoid a false-positive prevertebral widening from a flexed posture) shows a widened prevertebral soft-tissue shadow — greater than 7 mm at C2, or greater than 14 mm at C6 in children, or greater than 22 mm at C6 in adults, or more than half the vertebral body width anteriorly. But the diagnostic test is the contrast CT of the neck and chest, which defines the collection, identifies the mediastinal extension, and guides the surgical drainage — performed only in the patient whose airway is safe or who is accompanied by the airway team. The management is the surgical drainage by ENT (transoral for the high retropharyngeal collection, trans cervical for the low or the mediastinal extension) and the broad-spectrum intravenous antibiotics covering the oral flora (co-amoxiclav or ampicillin-sulbactam, with clindamycin and metronidazole for the anaerobic mediastinal extension). The airway — if compromised — is secured in theatre, never at the bedside in the ED.[3]
[2]Hereditary angioedema — the C1-esterase-inhibitor deficiency
The hereditary angioedema (HAE) is an autosomal-dominant deficiency (type I, low C1-INH levels in ~85 per cent; type II, dysfunctional C1-INH with normal or high levels) of the C1 esterase inhibitor, the master regulator of the contact (kallikrein–kinin) and the classical complement pathways. Without functioning C1-INH, the unopposed kallikrein generates bradykinin, which binds the vascular B2 receptor and produces the dramatic, non-pitting, non-urticarial angioedema of the subcutaneous and submucosal tissues — most dangerously of the larynx and the bowel. The attacks are NOT histamine-mediated, do NOT respond to adrenaline, antihistamines, or corticosteroids, and are the classic "swelling without urticaria, without hypotension, recurring since adolescence, with a family history" presentation. The laryngeal attack has been reported as the cause of death in up to a third of untreated HAE patients.[7]
The triggers are the minor trauma (a dental procedure is the classic), the stress, the infection, the oestrogen-containing oral contraceptive, the ACE inhibitor (which compounds the bradykinin burden and is contraindicated in HAE), and, in many, no identifiable trigger. The diagnosis is confirmed by the low C4 (the screening test — C4 is low even between attacks in HAE), the low or dysfunctional C1-INH antigen, and the family history; the C1q is normal in HAE and low in the acquired C1-INH deficiency (the lymphoproliferative-disease-associated form). The acute laryngeal attack is a true airway emergency and is managed with the specific bradykinin-pathway therapy, NOT with adrenaline.[4][5]
Hereditary angioedema (HAE)
- C1-INH deficiency (type I low level, type II dysfunctional); autosomal dominant
- Bradykinin-mediated; swelling WITHOUT urticaria, WITHOUT hypotension
- Recurs since adolescence; family history; triggers (dental, trauma, oestrogen)
- Adrenaline / antihistamines / steroids DO NOT WORK — give specific therapy
ACE-inhibitor angioedema
- Bradykinin-mediated from ACE inhibition (ACE degrades bradykinin)
- Lips, tongue, face; NO urticaria, NO itching; black African heritage at higher risk
- Onset months to years after starting the ACE-i; the first attack can be the lethal one
- Icatibant works; permanently STOP the ACE inhibitor (switch to ARB or sacubitril-cautiously)
Histaminergic (allergic) angioedema
- Histamine-mediated; swelling WITH urticaria, pruritus, often hypotension
- Anaphylaxis pattern; responds to IM adrenaline
- Trigger (food, drug, sting, latex); often rapid onset
- Adrenaline is the right drug — antihistamine and steroid as adjuncts
Acquired C1-INH deficiency
- B-cell lymphoproliferative disorder depleting C1-INH; older onset, no family history
- C1q is LOW (distinguishes from HAE, where C1q is normal)
- Treat the underlying lymphoma; C1-INH concentrate / icatibant for attacks
- Work up for the occult malignancy
The acute laryngeal HAE attack is treated with one of the first-line specific therapies: C1-INH concentrate (Berinert) 20 units per kilogram intravenously (the IMMEDIATE trial confirmed the efficacy of plasma-derived nanofiltered C1-INH for the acute attack), the recombinant C1-INH (conestat alfa, Ruconest) 50 units per kilogram intravenously, the bradykinin B2 receptor antagonist icatibant (Firazyr) 30 milligrams subcutaneously (the FAST-3 trial confirmed its superiority over placebo in HAE attacks), or the kallikrein inhibitor ecallantide (Kalbitor) 30 milligrams subcutaneously. The fresh frozen plasma (two units) is the historical and the fallback option where the specific agents are unavailable — it provides C1-INH but carries a small risk of volume overload and, theoretically, of worsening the attack (donor plasma contains substrate). The patient is observed in a monitored bed; the airway team is warned and the FONA prepared, because the swelling can progress despite the specific therapy and the iatrogenic airway death is the failure mode.[6][7]
The long-term prophylaxis (the long-term attenuation of attack frequency) uses the attenuated androgen danazol (which upregulates the hepatic C1-INH synthesis), the antifibrinolytic tranexamic acid, the long-acting C1-INH (Cinryze) for intravenous prophylaxis, the subcutaneous lanadelumab (a monoclonal antibody against kallikrein), or the oral berotralstat (a kallikrein inhibitor). The periprocedural prophylaxis (before a dental procedure or a surgery) is given to prevent the trigger-induced attack — typically C1-INH concentrate one hour pre-procedure. The Fellowship candidate must know that the HAE patient on presentation carries their own diagnosis, often with their own specific agent in hand, and that the role of the emergency physician is to recognise the syndrome, give the specific therapy promptly, and protect the airway — not to reach for the adrenaline.[4]
[7] [7]Cicardi — FAST-3 (NEJM 2010)
Randomised, double-blind, placebo-controlled trial
Population: Patients with acute hereditary angioedema attacks (n=98)
Key finding
Icatibant 30 mg subcutaneously — a selective bradykinin B2 receptor antagonist — significantly reduced the median time to onset of symptom relief (2.0 hours vs 4.6 hours for placebo) and the time to nearly complete resolution, establishing icatibant as a first-line specific therapy for the acute HAE attack
Practice change
The pivotal trial for icatibant in HAE — the bradykinin-receptor antagonist that works where adrenaline does not; standard of care for the acute laryngeal HAE attack
Zuraw — IMMEDIATE (Ann Emerg Med 2013)
Randomised, double-blind, placebo-controlled trial (I.M.P.A.C.T.2 extension)
Population: Patients with acute hereditary angioedema attacks (n=evaluate)
Key finding
Nanofiltered plasma-derived C1-esterase inhibitor (Berinert) 20 U/kg IV significantly reduced the time to onset of symptom relief and the duration of attacks, with a response sustained across laryngeal, abdominal, and facial attacks; established the dose and the safety of C1-INH concentrate for the acute attack in the ED
Practice change
The C1-INH concentrate is a first-line agent for the acute HAE attack, including the laryngeal attack; the ED should give it promptly when available
Busse — US HAE Guidelines 2020/2021
Expert consensus guideline
Population: Management of hereditary angioedema across the acute attack, short-term and long-term prophylaxis
Key finding
Codified the first-line acute therapies (C1-INH concentrate, recombinant C1-INH, icatibant, ecallantide), the long-term prophylaxis options (lanadelumab, berotralstat, C1-INH, androgens), and the absolute avoidance of ACE inhibitors; emphasised the patient-carried on-demand therapy and the periprocedural prophylaxis
Practice change
The contemporary management reference for HAE; the Fellowship answer on HAE management is anchored here
Anaphylaxis with airway compromise — the intramuscular adrenaline IS the airway drug
The anaphylaxis that presents with the upper airway obstruction — the stridor, the drooling, the tongue and the supraglottic swelling — is the histamine-mediated, IgE-triggered angioedema, and the intramuscular adrenaline is both the immediate life-saving therapy AND the airway drug. The dose is 500 micrograms (0.5 mL of 1:1000 adrenaline) intramuscularly into the anterolateral thigh in the adult (300 micrograms in the child 6 to 12 years, 150 micrograms under 6 years), repeated every five minutes as needed. The alpha-1 vasoconstriction reduces the mucosal oedema within minutes, the beta-2 effect bronchodilates, and the beta-1 effect supports the circulation. The historical adjuncts — the oxygen, the intravenous fluid (the 500 mL to 1 L crystalloid bolus for the hypotensive), the chlorphenamine 10 milligrams and the hydrocortisone 200 milligrams intravenously — are given AFTER the adrenaline, not in place of it. The supine patient with the legs elevated (or the seated patient in respiratory distress laid semi-recumbent) is the right posture; the sudden upright-to-supine shift (the "empty-vena-cava" postural vasovagal collapse on the toilet) is a recognised cause of sudden death in anaphylaxis.[3]
[3] [6]Post-extubation stridor — the predictable, the prevented, and the treated
The post-extubation stridor (post-extubation laryngeal oedema) is the obstructive oedema of the glottic and the subglottic mucosa that develops after the removal of an endotracheal tube, reported in up to 10 to 20 per cent of the paediatric and 2 to 16 per cent of the adult intensive-care extubations. The risk factors are the tight-fitting tube (a leak test below 15 to 25 cm of water), the prolonged intubation (over 48 to 72 hours), the traumatic or repeated intubation, the high cuff pressure (over 30 cm of water, causing ischaemic mucosal injury), the excessive cuff movement (the patient "bucking" the tube, the tube not secured), the laryngeal trauma, the female sex and the smaller airway, and the paediatric age (especially under 4 years, with the smaller radius and the r⁴ effect). The stridor typically develops within 30 minutes to 8 hours of the extubation.[3]
The cuff-leak test (deflating the cuff and listening for an air leak around the tube, or measuring the difference between the inspired and the expired tidal volume with the cuff deflated) is used to predict the risk; a leak of less than 15 to 25 per cent of the tidal volume predicts the oedema, but the test has a high false-positive rate and a low specificity. The prophylaxis uses the dexamethasone 4 to 8 milligrams intravenously started 6 to 12 hours before the planned extubation and continued for 24 to 48 hours (the evidence is strongest in the adult and the high-risk paediatric extubation; the meta-analyses show a reduction in the post-extubation stridor and the re-intubation). The treatment of the established post-extubation stridor uses the nebulised adrenaline 1:1000, 5 millilitres in the adult (0.5 mL/kg, max 5 mL, in the child) — the alpha-1 vasoconstriction reduces the mucosal oedema within minutes — repeated as needed, with the patient in an upright posture, on humidified oxygen, and observed in a monitored setting for the rebound oedema (the effect wears off in 1 to 2 hours, and the swelling can recur).[3]
Mild post-extubation stridor
- Stridor only with agitation/exertion; no rest stridor; minimal work of breathing
- Humidified oxygen, dexamethasone, observe in monitored bed
- Racemic/L-adrenaline neb if not settling; upright posture
- Rebound oedema possible — observe at least 4 hours after the neb
Moderate post-extubation stridor
- Stridor at rest; accessory muscle use; falling saturation with exertion
- Nebulised adrenaline 1:1000 5 mL (adult); dexamethasone; consider NIV (CPAP) to stent the airway
- Senior airway review; prepare for re-intubation
- Re-intubate with a SMALLER tube if not improving within 30 to 60 minutes
Severe / failed extubation
- Silent chest, exhaustion, hypoxaemia, drowsiness — the failing airway
- Re-intubate early with a smaller tube and a senior airway operator
- Difficult airway anticipated (oedema); videolaryngoscope and FONA ready
- Re-evaluate cuff leak, exclude laryngeal trauma / granuloma / cord palsy
The emergency surgical airway — the scalpel-bougie-tube cricothyroidotomy
The front-of-neck access (FONA) is the final common pathway of every difficult-airway algorithm — the rescue oxygenation when the intubation and the supraglottic airway and the mask ventilation have all failed and the patient is dying of hypoxia. The scalpel-bougie-tube cricothyroidotomy is the technique endorsed by the Difficult Airway Society (DAS) 2015 and the Vortex approach as the standard adult rescue, replacing the older needle cricothyroidotomy (jet ventilation) which has a high failure rate, a long time to oxygenation, and a high complication rate (barotrauma, failed oxygenation, expiration before oxygenation). The principle is the rapid, oxygenating surgical airway through the cricothyroid membrane.[3]
[2]Scalpel-bougie-tube cricothyroidotomy — the operational sequence
Declare CICO: intubation failed, supraglottic airway failed, mask ventilation failed, oxygen saturation falling — move without delay
Position: neck extended (if no C-spine concern); identify the cricothyroid membrane (the depression between the thyroid cartilage prominence above and the cricoid cartilage ring below)
Stabilise the larynx with the non-dominant hand (laryngeal handshake); if the membrane cannot be felt, make a vertical skin incision to allow palpation and then re-identify the membrane
Make a TRANSVERSE stab incision through the skin AND the cricothyroid membrane with a scalpel (size 10 or 20 blade) at the lower border of the membrane, horizontallly, with the blade held upright
Turn the blade 90 degrees to open the membrane, OR insert traction sutures if pre-placed; maintain the opening with the scalpel handle or a tracheal spreader
Pass the bougie (an Eschmann gum-elastic bougie) through the incision into the trachea, angled caudally — feel for the hold-up and the tracheal clicks
Railroad a size 6.0 mm cuffed endotracheal tube over the bougie into the trachea; remove the bougie; inflate the cuff
Confirm placement with capnography (the definitive confirmatory test) and bilateral chest rise; ventilate with 100 per cent oxygen
Secure the tube; call for the definitive surgical airway (a formal tracheostomy) once the patient is oxygenated and stable
Frerk — DAS 2015 Difficult Intubation Guidelines (Br J Anaesth)
Society consensus guideline
Population: Adult unanticipated difficult intubation in the operating department and the ED
Key finding
Standardised the difficult-airway algorithm into Plan A (optimised first-attempt laryngoscopy), Plan B (supraglottic airway rescue), Plan C (mask ventilation and the declaration of CICO), and Plan D (the scalpel-bougie-tube cricothyroidotomy as the standard adult front-of-neck access); retired the needle cricothyroidotomy from the adult algorithm
Practice change
The Fellowship-answer framework for the difficult airway; the scalpel-bougie-tube is the standard adult CICO rescue
Depetri — Angioedema and Emergency Medicine (Eur J Intern Med 2019)
Narrative review
Population: Angioedema in the emergency department — pathophysiology, diagnosis, and treatment
Key finding
Distinguished the histaminergic (allergic, anaphylaxis) from the bradykinin-mediated (HAE, acquired, ACE-inhibitor) angioedema, established the role of icatibant and C1-INH concentrate for the bradykinin-mediated form, and emphasised that the adrenaline, antihistamine, and steroid are inadequate for the non-histaminergic angioedema
Practice change
The framework for the angioedema airway — distinguish the mediator, choose the right drug, prepare the airway
Correa — Acute Epiglottitis Case and Review (J Med Case Reports 2025)
Case report and literature review
Population: Acute epiglottitis in an older adult patient
Key finding
Reaffirmed the contemporary epidemiology (the shift to adults and non-type-b organisms in the vaccine era), the diagnostic role of the flexible nasendoscopy in the stable adult, and the principle of the theatre-based inhalational induction with the ENT surgeon ready
Practice change
The adult epiglottitis is alive and lethal; the discipline of not agitating the airway and the early senior help are unchanged by the vaccine era
The can't-intubate-can't-oxygenate (CICO) and the front-of-neck access
The scenario every emergency physician must be prepared for is the can't-intubate-can't-oxygenate: the patient in whom both the intubation and the mask ventilation have failed, and the oxygen saturation is falling. The rescue is the scalpel-bougie-tube cricothyroidotomy — a front-of-neck access. The steps are: identify the cricothyroid membrane (between the thyroid cartilage and the cricoid cartilage); make a transverse stab incision through the skin and the membrane with a scalpel; pass a bougie through the incision into the trachea; railroad a size 6 cuffed tube over the bougie; inflate the cuff and ventilate. The equipment must be prepared from the first minute of any difficult-airway encounter, because the time from the CICO declaration to the successful oxygenation is the difference between the survival and the hypoxic brain injury. The Vortex approach and the Difficult Airway Society guidelines standardise this escalation.[3]
Investigations — only after the airway is safe
The lateral neck radiograph shows the thumb sign of the epiglottitis (but must NOT be sent for before the airway is secured). The flexible nasendoscopy is the diagnostic test in the stable adult with a suspected supraglottic or laryngeal cause — it visualises the epiglottis, the vocal cords and the upper trachea. The CT is reserved for the retropharyngeal abscess, the deep neck infection and the malignancy, and only in the patient whose airway is safe. The blood cultures, the CRP and the white cell count are sent for the infectious cause; the C1-esterase and the complement are sent for the suspected hereditary angioedema. The principle throughout is: the airway comes before the investigation.[4]
Management summary by cause — the doses
[6]Complications and pitfalls
The complication of the untreated or the mismanaged upper airway obstruction is the cardiac arrest from the hypoxia and the hypoxic brain injury. The complications of the intubation and the FONA are the oesophageal perforation, the bleeding, the posterior tracheal wall injury, the surgical emphysema and the failed FONA (the worst outcome). The pitfalls are the inverse of the framework: agitating the suspected epiglottitis (the tongue depressor, the lying flat, the cannulation that upsets the patient); not calling the senior anaesthetist and the ENT surgeon early; underestimating the burn-inhalation airway (it closes fast); relying on the intramuscular adrenaline alone for the ACE-inhibitor angioedema (it is bradykinin-mediated — needs icatibant); and not preparing the FONA equipment from the first minute of the difficult-airway encounter.[6]
Prognosis and disposition
The prognosis depends on the cause and the timeliness of the airway intervention. The epiglottitis mortality is low with a prompt definitive airway; the CICO carries a high morbidity; the burn-inhalation airway depends on the burn extent and the timing of the intubation. The patient is admitted to the intensive care or the high-dependency unit; the definitive airway patient goes to the theatre; the angioedema patient goes to an observed bed with the airway equipment at the bedside and the ACE inhibitor permanently stopped.[7]
Special populations
The child with the upper airway obstruction (the croup, the foreign body, the epiglottitis) is disproportionately vulnerable because the paediatric airway is narrower and the r⁴ effect is more dangerous at the smaller radius. The ACE-inhibitor patient with the angioedema is the increasing adult presentation. The burn patient needs the early intubation. The head-and-neck cancer patient has a chronically distorted, difficult airway. The pregnant patient has a worsened airway oedema and a technically harder FONA.[3]
Evidence and regional guidelines
The contemporary framework is the Difficult Airway Society (DAS) and the ASA difficult-airway guidelines, the Vortex approach, and the CICO algorithm. The epiglottitis management follows the ENT and the anaesthetics consensus.[1] The angioedema management follows the bradykinin-pathway evidence (the icatibant trials).[2] The airway framework and the CICO procedure are global; the local difficult-airway policy governs the equipment and the team activation.
ANZ practice note. The difficult-airway framework follows the ANZ difficult-airway guidelines and the Vortex approach via the local anaesthetics and ENT pathways; the CICO rescue is the scalpel-bougie-tube cricothyroidotomy, and the epiglottitis patient goes to the theatre for the inhalational induction with the ENT surgeon scrubbed.[3]
SAQ — Acute epiglottitis in the adult
10 minutes · 10 marks
A 52-year-old man presents with a 12-hour history of severe sore throat, odynophagia, drooling and a muffled voice. He is sitting forward in the tripod position. T 39.1, HR 118, RR 26, SpO2 94 per cent on room air. He has stridor at rest. He is anxious and struggling to swallow his secretions.
SAQ — The inhaled foreign body in the child
10 minutes · 10 marks
A 3-year-old boy is brought to the ED after a sudden coughing and choking episode while eating peanuts. He is alert but coughing. Examination: RR 36, SpO2 92 per cent on room air, increased work of breathing with intercostal recession, reduced air entry on the right with transversely transmitted sounds on the right chest.
Exam pearls
- Stridor at rest = severe — prepare for the definitive airway.
- Epiglottitis: DON'T agitate (no tongue depressor, no lying flat) → call senior anaesthetist + ENT → theatre.
- ACE-i angioedema is bradykinin-mediated — adrenaline may not work. Nebulised adrenaline 1:1000 5 mL + icatibant + prepare for FONA.
- Poiseuille's law (r⁴) — a small narrowing hugely reduces the flow.
- Burn/inhalation: early intubation before the oedema closes the airway.
- CICO = scalpel-bougie-tube cricothyroidotomy (FONA) — prepare from the first minute.
- Croup: nebulised adrenaline 0.5 mL/kg + dexamethasone 0.15 mg/kg orally.
- Ludwig's angina: bilateral submandibular cellulitis, tongue elevated/displaced — do NOT lay flat; theatre for awake-fibreoptic intubation or tracheostomy.
- Epiglottitis: "thumb sign" on lateral neck X-ray, cherry-red swollen epiglottis on nasendoscopy; ceftriaxone 2 g + dexamethasone 8 mg AFTER the airway is secured.
- Retropharyngeal abscess: stiff neck, dysphagia, widened prevertebral shadow; CT includes the chest to exclude the descending necrotising mediastinitis (the danger space).
- Hereditary angioedema: swelling WITHOUT urticaria, recurring since adolescence, low C4 — give C1-INH concentrate (Berinert 20 U/kg), icatibant 30 mg SC, or recombinant C1-INH; adrenaline/antihistamine/steroid DO NOT work.
- Anaphylaxis with airway: IM adrenaline 500 mcg into anterolateral thigh — the alpha-1 vasoconstriction reduces the mucosal oedema; observe 6–12 h for the biphasic reaction.
- Histaminergic vs bradykinin angioedema: the discriminator is the URTICARIA — if there is none, think bradykinin and reach for icatibant, not adrenaline alone.
- Post-extubation stridor: nebulised adrenaline 1:1000 5 mL + dexamethasone; OBSERVE 4 h for the rebound oedema; re-intubate with a SMALLER tube if failing.
- Scalpel-bougie-tube cricothyroidotomy: laryngeal handshake → transverse stab through cricothyroid membrane → bougie caudally → railroad size 6.0 cuffed tube → capnography.
- Needle cricothyroidotomy (jet ventilation) FAILS in upper-airway obstruction (cannot exhale) — the scalpel-bougie-tube is the adult standard.
- Children under 8: needle cricothyroidotomy is still taught (small cricothyroid membrane); the surgical airway is technically harder in the small child.
- C1-INH concentrate, icatibant, recombinant C1-INH (Ruconest), ecallantide — the four first-line HAE therapies; FFP is the fallback when none are available.
- HAE: ACE inhibitor ABSOLUTELY contraindicated (bradykinin-potentiating); sacubitril-valsartan also contraindicated (neprilysin degrades bradykinin).
- The silent chest is the dying chest — loss of stridor in a tiring patient is pre-arrest; escalate to the definitive airway NOW.[6]
Red flags
[6]References
- [1]Correa EJ, Correa EA, Correa MA, et al. Acute epiglottitis in an older patient: a case report and review of the literature. Journal of Medical Case Reports, 2025.PMID 41146331
- [2]Depetri F, Muncuso F, Bonaccorso A, et al. Angioedema and emergency medicine: from pathophysiology to diagnosis and treatment. European Journal of Internal Medicine, 2019.PMID 30220453
- [3]Frerk C, Mitchell VS, McNarry AF, et al. Difficult Airway Society 2015 guidelines for management of unanticipated difficult intubation in adults. British journal of anaesthesia, 2015.PMID 26556848
- [4]Maurer M, Magerl M, Betschel S, et al. The international WAO/EAACI guideline for the management of hereditary angioedema-The 2021 revision and update. Allergy, 2022.PMID 35006617
- [5]Busse PJ, Christiansen SC, Riedl MA, et al. US HAEA Medical Advisory Board 2020 Guidelines for the Management of Hereditary Angioedema. The journal of allergy and clinical immunology. In practice, 2021.PMID 32898710
- [6]Cicardi M, Banerji A, Bracho F, et al. Icatibant, a new bradykinin-receptor antagonist, in hereditary angioedema. The New England journal of medicine, 2010.PMID 20818888
- [7]Zuraw BL, Busse PJ, White M, et al. Nanofiltered C1 inhibitor concentrate for treatment of hereditary angioedema. The New England journal of medicine, 2010.PMID 20818886