ICU · Antimicrobial Stewardship
Antimicrobial resistance in the ICU: mechanisms, organisms, and management
Also known as MDR organisms in ICU · VRE, ESBL, CRE, CPE · Antibiotic resistance · ESBL pneumonia · Carbapenem-resistant Enterobacterales · MRSA, VRE, CRPA, CRAB · Beta-lactamases — KPC, NDM, OXA-48 · Novel antibiotics for MDR Gram-negatives
Multidrug-resistant (MDR) organisms are endemic in the ICU and independently increase mortality, length of stay, and cost. Resistance arises from beta-lactamases (ESBL — CTX-M; AmpC; carbapenemases — KPC class A, NDM/VIM/IMP class B metallo-beta-lactamases, OXA-48 class D), altered targets (PBP2a in MRSA via mecA; D-Ala-D-Lac in VRE via vanA/B; QRDR mutations in fluoroquinolone resistance), efflux pumps, porin loss (OprD in Pseudomonas), and enzymatic modification. The ICU core threats are MRSA, VRE, ESBL-Enterobacterales, CRE/CPE, carbapenem-resistant Pseudomonas aeruginosa (CRPA) and carbapenem-resistant Acinetobacter baumannii (CRAB). Management demands rapid molecular diagnostics (carbapenemase typing), empiric broad therapy within one hour of sepsis, then aggressive de-escalation using novel beta-lactam/beta-lactamase inhibitor combinations (ceftazidime-avibactam for KPC/OXA-48; meropenem-vaborbactam and imipenem-relebactam for KPC; ceftolozane-tazobactam and cefiderocol for MDR Pseudomonas; aztreonam-avibactam for NDM/MBL), supported by infection-control bundles (contact precautions, cohorting, surveillance screening, decolonisation) and antimicrobial stewardship (PK/PD-optimised dosing, extended infusions, therapeutic drug monitoring, shortest effective duration).
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
SAQ — Carbapenem-resistant Klebsiella pneumoniae bacteraemia in a repatriated patient (NDM metallo-beta-lactamase)
10 minutes · 10 marks
A 62-year-old man is admitted to ICU in septic shock 10 days after repatriation from a three-week hospitalisation in New Delhi for polytrauma (splenectomy, temporary colostomy, broad-spectrum antibiotics). On examination: T 39.1 degrees C, HR 132, BP 78/45 on noradrenaline 0.4 mcg/kg/min (MAP 58 after 30 mL/kg crystalloid), RR 30, SpO2 94 percent on FiO2 0.5, GCS 13, urine output 15 mL/h. Lactate 5.2 mmol/L, creatinine 220 micromol/L (baseline 85), platelets 92, INR 1.7. Two of two peripheral blood cultures grow Klebsiella pneumoniae resistant to meropenem, ertapenem, all cephalosporins, fluoroquinolones and aminoglycosides; carbapenemase PCR has been sent and is pending.
SAQ — Vancomycin-resistant Enterococcus faecium (vanA VRE) bacteraemia complicated by VRE ventilator-associated pneumonia
10 minutes · 10 marks
A 67-year-old man is day 14 of an ICU admission for necrotising pancreatitis. He has a triple-lumen central venous catheter, an arterial line, and is intubated for abdominal sepsis and ARDS. He now develops fever (38.9 degrees C), HR 118, BP 96/58, rising lactate to 3.1 mmol/L, and purulent endotracheal secretions. Two of two peripheral blood cultures grow Enterococcus faecium resistant to vancomycin and ampicillin (vanA VRE), susceptible to linezolid and daptomycin (daptomycin MIC 1 mg/L). Platelets 140 x 10^9/L, creatinine 160 micromol/L. Transthoracic echo shows no vegetations.
Clinical pearls
Red flags
Overview — why antimicrobial resistance dominates ICU practice
Antimicrobial resistance (AMR) is one of the top ten global public health threats and is magnified in the ICU, where antibiotic pressure is intense, patients are vulnerable, and the consequences of ineffective empiric therapy are measured in hours of added mortality. The WHO publishes a priority pathogens list ranking carbapenem-resistant Gram-negatives as the highest-priority ("critical") targets for new drug development.[3] In a critically ill patient, the single biggest decision the intensivist makes is whether to broaden empiric cover to capture likely MDR organisms — because inappropriate empiric therapy independently raises mortality, yet every unnecessary antibiotic day drives further resistance, C. difficile, and toxicity.
AMR is not one problem but many. Resistance is encoded by genes on chromosomes, plasmids, transposons and integrons, spreads horizontally between bacteria (plasmid transfer, conjugation), and is selected by antibiotic exposure (the ICU itself is a resistance factory). The intensivist must know (1) the mechanism of each resistance phenotype, because it predicts which drug classes fail and which novel agents work; (2) the organism and its risk factors, to calibrate empiric therapy; and (3) the stewardship and infection-control bundle that contains spread. This topic maps the resistance mechanisms, the six core ICU MDR organisms, the novel antibiotics that have transformed therapy since 2015, and the bundles that prevent and de-escalate.[3]
Definitions — MDR, XDR, PDR (Magiorakos 2012)
The internationally agreed (ECDC/CDC consensus) definitions are built around antimicrobial categories (drug classes), not individual agents, and apply to acquired resistance.[4] Every fellowship candidate must be able to quote them.
[4]Applying the definitions correctly: (1) count categories, not drugs — an organism resistant to three cephalosporins counts as resistant to one category and is not yet MDR; (2) only acquired resistance counts (intrinsic Pseudomonas ampicillin resistance does not); (3) the isolate must have been tested against nearly all agents — you cannot call an organism "PDR" if half the panel was never tested; (4) breakpoints are revised (CLSI M100, EUCAST) — apply the current breakpoint.[4]
Mechanisms of resistance — the molecular basis
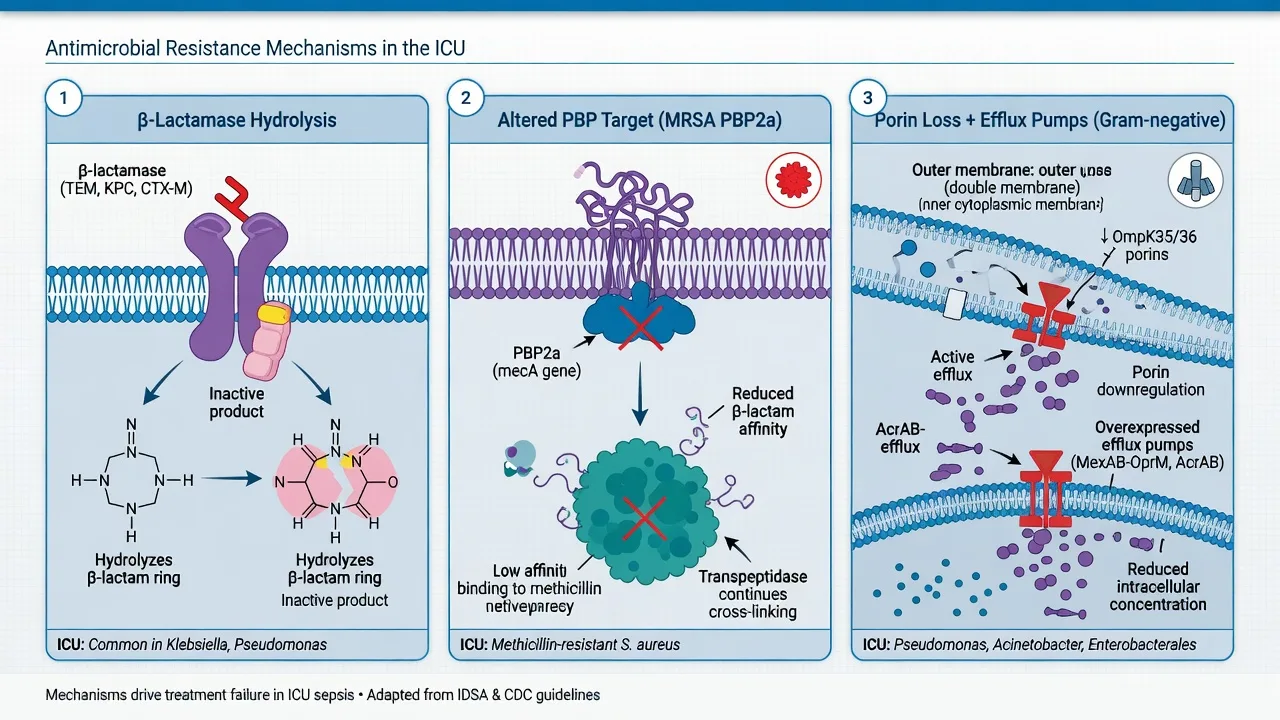
Resistance mechanisms fall into a small number of strategies: (1) enzymatic inactivation of the drug (beta-lactamases, aminoglycoside-modifying enzymes, chloramphenicol acetyltransferases); (2) target alteration (PBP2a, D-Ala-D-Lac, QRDR mutations, D-Ala-D-Ala to D-Ala-D-Ser); (3) reduced intracellular accumulation via decreased influx (porin loss, e.g., OprD in Pseudomonas) or increased efflux (AcrAB-TolC, Mex pumps); (4) bypass of the inhibited pathway (alternative PBP); and (5) protection of the target (tetracycline-resistance ribosomal protection proteins). The ICU intensivist needs fluency with the beta-lactamase family tree in particular, because it dictates which novel beta-lactamase inhibitor to deploy.[3][17]
Beta-lactamases — Ambler classification
Beta-lactamases are classified by Ambler molecular class (A-D), which reflects the active-site chemistry. This is not pedantry: class A, C and D are serine beta-lactamases (inhibited by classical inhibitors like clavulanate, tazobactam, and the novel diazabicyclooctanes avibactam/relebactam and boronic acids vaborbactam); class B are metallo-beta-lactamases requiring zinc at the active site, inhibited by EDTA chelation but NOT by any licensed beta-lactamase inhibitor, and intrinsically unable to hydrolyse aztreonam.[17]
[7]ESBL — Extended-Spectrum Beta-Lactamases
ESBLs are Ambler class A serine beta-lactamases that hydrolyse the oxyimino-beta-lactams — penicillins and 3rd-generation cephalosporins (ceftriaxone, ceftazidime) and (for many) the 4th-generation cefepime — but not carbapenems or cephamycins. They are typically plasmid-encoded, which means they spread horizontally and frequently carry co-resistance genes (fluoroquinolones, aminoglycosides, co-trimoxazole) on the same plasmid — explaining why ESBL isolates are so often multiply resistant. CTX-M has overtaken TEM and SHV as the dominant ESBL family worldwide, with bla(CTX-M-15) the single most common allele.[5][17]
Inoculum effect: cephalosporins can look susceptible at low inoculum but fail at the high bacterial loads seen in bacteraemia, pneumonia, or undrained abscess. This is why cephalosporins are not reliable for ESBL even when reported susceptible, and why MERINO established the carbapenem as the standard of care.[5]
AmpC beta-lactamases
AmpC are class C enzymes that are either chromosomally encoded and inducible (the "SPICE/SPACE" organisms — Serratia, Pseudomonas, Indole-positive Proteae [Morganella, Providencia], Citrobacter, Enterobacter; some add Acinetobacter) or plasmid-acquired (in E. coli, Klebsiella). Induction occurs on exposure to beta-lactams (especially clavulanate, which paradoxically induces AmpC), so therapy can select for a derepressed mutant during treatment — the clinical scenario of an Enterobacter bacteraemia that develops cephalosporin resistance mid-therapy. Cefepime is relatively stable to AmpC (a key reason it is preferred over 3rd-gen cephalosporins for known AmpC producers); carbapenems are the reliable backstop for serious AmpC infections.[17]
Carbapenemases — the highest-yield distinction
Carbapenemases hydrolyse carbapenems (and virtually all other beta-lactams). Identifying the type of carbapenemase — by PCR (KPC/NDM/OXA-48/VIM/IMP), CarbaNP, modified carbapenem inactivation method (mCIM), or MALDI-TOF hydrolysis assay — drives the drug choice.[3][17]
[7]The pearl that saves lives: NDM is a metallo-beta-lactamase — avibactam and vaborbactam do NOT inhibit it, so ceftazidime-avibactam or meropenem-vaborbactam monotherapy for an NDM producer fails. But aztreonam is structurally stable to metallo-enzymes, so the combination aztreonam-avibactam works: avibactam shields aztreonam from any co-produced ESBL/AmpC/KPC, while the MBL cannot touch aztreonam. NDM producers also frequently co-carry 16S rRNA methylases (conferring aminoglycoside resistance) and plasmid-borne colistin resistance (mcr), narrowing salvage options.[17]
Non-beta-lactam resistance mechanisms
[5]The six core ICU MDR organisms
[7]MRSA — methicillin-resistant Staphylococcus aureus
VRE — vancomycin-resistant Enterococcus
ESBL — Extended-Spectrum Beta-Lactamase Enterobacterales
CRE — Carbapenem-Resistant Enterobacterales
CRPA — Carbapenem-Resistant Pseudomonas aeruginosa
Pseudomonas aeruginosa is intrinsically difficult (low outer-membrane permeability, AmpC, broad efflux) and acquires resistance readily. Difficult-to-treat resistance (DTR) denotes non-susceptibility to all first-line anti-pseudomonals (piperacillin-tazobactam, ceftazidime, cefepime, aztreonam, meropenem, imipenem, ciprofloxacin, levofloxacin). The IDSA 2024 guidance prefers novel BL/BLI over polymyxins when susceptible.[17]
CRAB — Carbapenem-Resistant Acinetobacter baumannii
CRAB is a WHO "critical priority" pathogen, endemic in many ICUs, and one of the most therapy-limited organisms in practice. Resistance is driven by OXA-type carbapenemases (OXA-23, OXA-24/40, OXA-58), AdeABC efflux, and often polymyxin co-resistance.[11]
Novel antibiotics for MDR Gram-negatives — the post-2015 armamentarium
Five novel agents — ceftazidime-avibactam, meropenem-vaborbactam, imipenem-relebactam, ceftolozane-tazobactam, cefiderocol — plus plazomicin and eravacycline have transformed the treatment of MDR Gram-negative infections, displacing colistin as first-line for many susceptible isolates and reducing nephrotoxicity.[3][17]
[17]Infection control — containing MDR in the ICU
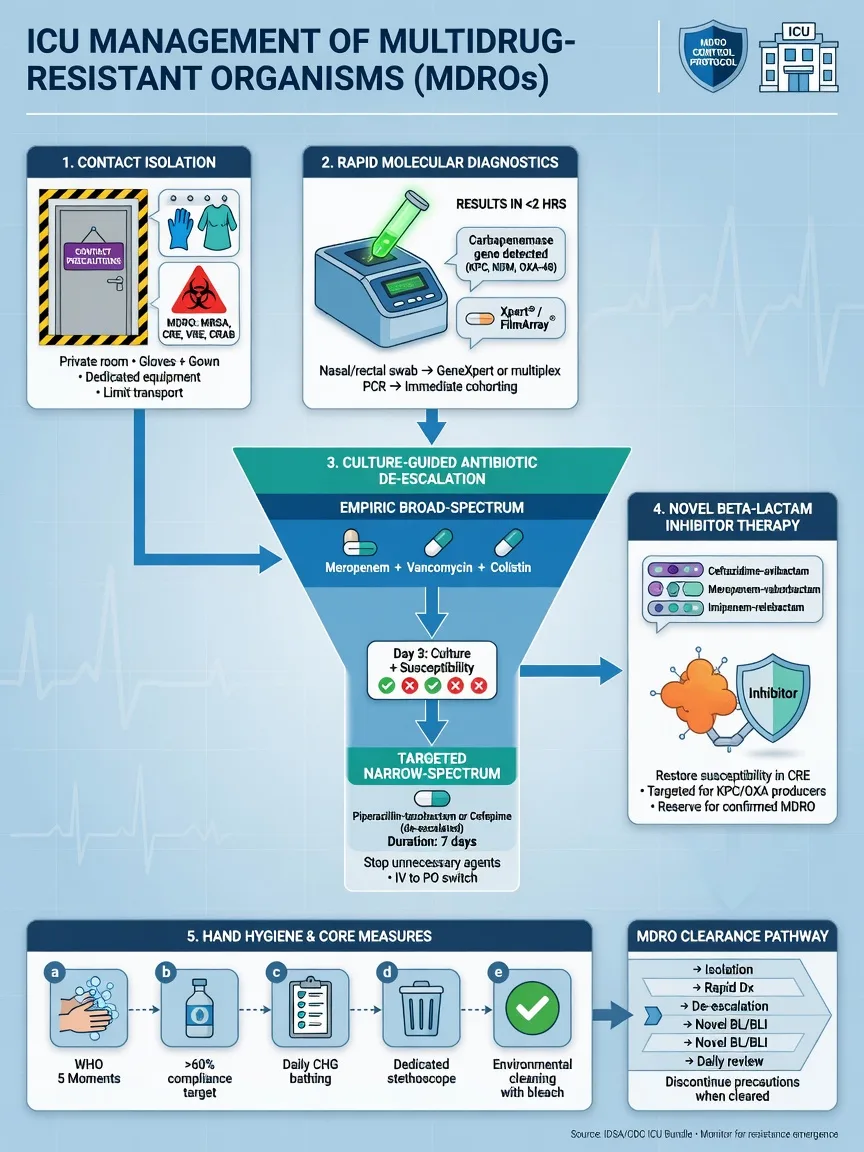
Infection control is the only intervention that prevents MDR spread; treatment of individual patients does not. The bundle (CDC, ESCMID) rests on standard precautions applied rigorously, contact precautions for MDR, surveillance, cohorting, decolonisation, and environmental hygiene.[14]
[14]Antimicrobial stewardship — the intensivist's daily discipline
Stewardship protects the patient (right drug, right dose, right duration), protects the unit (less resistance, less C. difficile), and protects the population (preserves agents for the future). The ICU is where stewardship pays the largest dividend because antibiotic exposure per patient-day is highest.[1][18]
Prognosis — why MDR doubles mortality
[7]Why MDR doubles mortality: the excess is driven by (1) inappropriate empiric therapy — the initial antibiotic misses the organism because of resistance, and each hour of delay in septic shock raises mortality ~8%; (2) greater virulence and comorbidity in the affected population (sicker patients get MDR); (3) use of toxic salvage agents (colistin) with their own failure modes. The corollary: a current antibiogram, rapid molecular diagnostics, getting the first antibiotic right, and aggressive source control close most of the mortality gap.[1][3]
Key trials and evidence
MERINO (Harris PNA 2018, JAMA) — meropenem vs piperacillin-tazobactam for ceftriaxone-resistant E. coli/Klebsiella bacteraemia
TANGO II (Wunderink 2018, Infect Dis Ther) — meropenem-vaborbactam vs best-available therapy for CRE
RESTORE-IMI 1 (Motsch 2020, Clin Infect Dis) — imipenem-relebactam vs colistin + imipenem for imipenem-nonsusceptible infection
ASPECT-NP (Martin-Loeches 2023, Ann Intensive Care) — ceftolozane-tazobactam for ventilated nosocomial pneumonia
CREDIBLE-CR (Bassetti 2021, Lancet Infect Dis) — cefiderocol vs best-available therapy for carbapenem-resistant Gram-negative infection
EPIC-cUTI (Wagenlehner 2019, NEJM) — plazomicin vs levofloxacin for complicated UTI
IDSA 2024 Guidance on Treatment of AMR Gram-Negative Infections (Tamma PD 2024, Clin Infect Dis)
Lange 2019 (Lancet) — Management of drug-resistant tuberculosis
Exam pitfalls and high-yield summary
SPICESPICE organisms — the inducible AmpC family
KNIFECarbapenemase classes — "KNIFE" for the ICU
References
- [1]Niederman MS, Torres A. Severe community-acquired pneumonia. European Respiratory Review, 2022.PMID 36517046
- [3]Tacconelli E, Carrara E, Savoldi A, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infectious Diseases, 2018.PMID 29276051
- [4]Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clinical Microbiology and Infection, 2012.PMID 21793988
- [5]Harris PNA, Tambyah PA, Lye DC, et al. Effect of Piperacillin-Tazobactam vs Meropenem on 30-Day Mortality for Patients With E coli or Klebsiella pneumoniae Bloodstream Infection and Ceftriaxone Resistance: A Randomized Clinical Trial. JAMA, 2018.PMID 30208454
- [6]Rybak MJ, Le J, Lodise TP, et al. Therapeutic Monitoring of Vancomycin for Serious Methicillin-resistant Staphylococcus aureus Infections: A Revised Consensus Guideline. Clinical Infectious Diseases, 2020.PMID 32658968
- [7]Shields RK, Nguyen MH, Chen L, et al. Pneumonia and Renal Replacement Therapy Are Risk Factors for Ceftazidime-Avibactam Treatment Failures and Resistance among Patients with Carbapenem-resistant Enterobacteriaceae Infections. Antimicrobial Agents and Chemotherapy, 2018.PMID 29507064
- [8]Wunderink RG, Giamarellos-Bourboulis EJ, Rahav G, et al. Effect and Safety of Meropenem-Vaborbactam versus Best-Available Therapy in Patients with Carbapenem-Resistant Enterobacteriaceae Infections in the TANGO II Randomized Trial. Infectious Diseases and Therapy, 2018.PMID 30270406
- [9]Motsch J, Murta de Oliveira C, Stus V, et al. RESTORE-IMI 1: A Multicenter, Randomized, Double-blind Trial Comparing Efficacy and Safety of Imipenem/Relebactam versus Colistin plus Imipenem in Patients with Imipenem-nonsusceptible Infections. Clinical Infectious Diseases, 2020.PMID 31400759
- [10]Martin-Loeches I, Shorr AF, Wunderink RG, et al. Outcomes in participants with ventilated nosocomial pneumonia and organ failure treated with ceftolozane/tazobactam in the ASPECT-NP trial. Annals of Intensive Care, 2023.PMID 36773112
- [11]Bassetti M, Echols R, Matsunaga Y, et al. Efficacy and safety of cefiderocol or best available therapy for the treatment of serious infections caused by carbapenem-resistant Gram-negative bacteria (CREDIBLE-CR): a randomised, open-label, blinded-endpoint, pathogen-focused, descriptive study. Lancet Infectious Diseases, 2021.PMID 33058795
- [12]Zhanel GG, Cheung D, Adam H, et al. Review of Eravacycline, a Novel Fluorocycline Antibacterial Agent. Drugs, 2016.PMID 26863149
- [13]Wagenlehner FME, Cloutier DJ, Komirenko AS, et al. Once-Daily Plazomicin for Complicated Urinary Tract Infections. New England Journal of Medicine, 2019.PMID 30786187
- [14]Tacconelli E, Cataldo MA, Dancer SJ, et al. ESCMID guidelines for the management of the infection control measures to reduce transmission of multidrug-resistant Gram-negative bacteria in hospitalized patients. Clinical Microbiology and Infection, 2014.PMID 24329732
- [15]Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clinical Infectious Diseases, 2011.PMID 21208910
- [16]Lange C, Dheda K, Chesov D, et al. Management of drug-resistant tuberculosis. Lancet, 2019.PMID 31526739
- [17]Tamma PD, Heil EL, Justo JA, et al. Infectious Diseases Society of America 2024 Guidance on the Treatment of Antimicrobial-Resistant Gram-Negative Infections. Clinical Infectious Diseases, 2024.PMID 39108079
- [18]Lawandi A, Yek C, Kadri SS, et al. IDSA guidance and ESCMID guidelines: complementary approaches toward a care standard for MDR Gram-negative infections. Clinical Microbiology and Infection, 2022.PMID 35150882
- [19]Huang SS, Septimus E, Hayden MK, et al. Effect of body surface decolonisation on bacteriuria and candiduria in intensive care units: an analysis of a cluster-randomised trial. Lancet Infectious Diseases, 2016.PMID 26631833
- [20]Heaney M, Mahoney MV, Gallagher JC. Eravacycline: The Tetracyclines Strike Back. Annals of Pharmacotherapy, 2019.PMID 31081341