ICU · Infection / global health
Tropical & Global Infections — Malaria, Dengue, TB, Influenza & COVID
Also known as Severe malaria · Falciparum malaria · Artesunate · Cerebral malaria · AQUAMAT · SEAQUAMAT · Exchange transfusion malaria · Dengue · Dengue shock syndrome · Dengue NS1 antigen · Melioidosis · Burkholderia pseudomallei · Severe enteric fever · Typhoid · Intestinal perforation typhoid · Scrub typhus · Orientia tsutsugamushi · Murine typhus · Doxycycline · Leprosy · Severe tuberculosis · Miliary TB · TB meningitis · RIPE therapy · Severe influenza · Severe COVID-19 · Dexamethasone COVID
The tropical and the global infections in the ICU: the severe malaria (the Plasmodium falciparum — the cerebral, the ARDS, the AKI, the severe anaemia, the hypoglycaemia, the hyperparasitaemia; the IV artesunate the WHO first-line, the superior to the quinine, the AQUAMAT and the SEAQUAMAT the mortality benefit; the blood smear or the RDT), the dengue (the plasma leak — the pleural effusion, the ascites, the haemoconcentration; the dengue shock syndrome; the cautious the fluids in the leak phase; the NS1 antigen; the warning signs; the paracetamol NOT the NSAIDs; the platelets or the FFP for the bleeding), the melioidosis (the Burkholderia pseudomallei — the pneumonia, the liver and the spleen abscess; the ceftazidime or the meropenem the intensive then the eradication the TMP-SMX), the severe enteric fever (the typhoid — the intestinal perforation, the encephalopathy, the ceftriaxone or the azithromycin, the carrier state), the rickettsial (the scrub typhus and the murine typhus — the doxycycline), the leprosy, the severe TB (the miliary or the TB meningitis; the RIPE plus the steroids for the meningitis and the pericarditis; the GeneXpert; the isolation), the severe influenza (the viral pneumonia or the ARDS; the secondary bacterial; the oseltamivir within 48 h or the severe), and the severe COVID-19 (the hypoxic ARDS; the dexamethasone the RECOVERY; the remdesivir; the tocilizumab; the anticoagulation; the prone or the lung-protective).
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
The tropical and the global infections are the endemic (the tropics) and the pandemic (the influenza, the COVID) infections that present to the ICU. The returned traveller with the fever, the severe pneumonia, or the multi-organ failure warrants the consideration of the malaria, the dengue, the melioidosis, the enteric fever, the rickettsial disease, the TB, the influenza, and the COVID. The early the specific therapy (the artesunate for the malaria, the oseltamivir for the influenza, the dexamethasone for the COVID, the RIPE for the TB, the doxycycline for the scrub typhus, the ceftazidime for the melioidosis) is the survival-critical.[1]
The two questions the fellow MUST ask of any febrile ICU admission: (1) Has this patient left the endemic area within the relevant incubation window? (malaria — weeks to months; dengue — up to 2 weeks; scrub typhus — 1 to 3 weeks; melioidosis — decades, the latency the longest of any bacterium), and (2) what is the time-critical empiric agent that covers the diagnosis I must not miss? The empirical artesunate within the hour for any smear-pending returned traveller from a malarious area is the single highest-yield exam answer in this domain.[4]
Severe malaria (Plasmodium falciparum)

- The Plasmodium falciparum — the severe form. The endemic the tropics and the sub-tropics. The returned traveller — the ANY the fever within the 3 months of the return from the endemic area = the malaria until proven otherwise.[1]
- The severe malaria criteria (WHO) — the impaired consciousness (the cerebral malaria — the GCS under 11 or the unrousable), the seizures, the respiratory distress (the ARDS, the metabolic acidosis), the shock, the AKI (the creatinine over 265 µmol/L or the urine output under 0.5 mL/kg/h), the severe anaemia (the Hb under 70 in the adult, the under 50 in the child), the hypoglycaemia (the under 2.2 mmol/L — the common, the quinine-exacerbated), the jaundice (the bilirubin over 50), the hyperparasitaemia (the over 2 per cent, or the over 10 per cent in the non-immune), the acidosis (the bicarbonate under 15, the lactate over 5), the haemoglobinuria (the blackwater fever), the important parasitaemia plus the end-organ.[1][4]
- The diagnosis — the blood smear (the thick for the detection, the thin for the species and the parasitaemia); the rapid diagnostic test (the RDT — the HRP-2 the antigen); the repeat the smear the every 6 to 12 hours if the first negative and the suspicion high — a single smear misses the low-parasitaemia.[4]
- The treatment — the IV artesunate (the WHO first-line — the 2.4 mg/kg at 0, 12, 24 hours then daily; the superior to the quinine, the mortality benefit). The loading plus the course. The doxycycline or the clindamycin after the artesunate (the radical cure, the clear the late gametocytes — the falciparum has no liver hypnozoite, the no primaquine the required for the relapse-prevention, BUT the single low-dose primaquine the gametocytocidal for the transmission-block).[1][2][3]
- The quinine — the alternative (the 20 mg/kg loading then 10 mg/kg the q8h; the hypoglycaemia risk the insulin-driven, the QT prolongation, the tinnitus, the cinchonism). The artemether the IM the alternative if the IV artesunate the unavailable.[4]
- The supportive — the ICU, the ventilation for the ARDS, the transfusion for the severe anaemia (the under 70, or the under 80 with the severe disease), the treat the hypoglycaemia (the 10 to 50 per cent glucose, the quinine-exacerbated — monitor the bedside glucose hourly), the haemodiafiltration for the AKI. The exchange transfusion for the hyperparasitaemia (the controversial — the over 10 per cent in the non-immune, or the over 5 per cent with the end-organ). The monitor the parasitaemia — the fall expected at the 24 to 48 hours; the no clearance by the 72 hours = the artesunate resistance (the emerging in the Greater Mekong).[1][4]
Cerebral malaria — the brain-killing phenotype
- The cerebral malaria — the unrousable coma (the GCS under 11, the Blantyre under 3 in the child), the seizures (the often the subclinical — the continuous the EEG), the decorticate or the decerebrate the posturing, the opisthotonus. The exclude the meningitis, the encephalitis, the metabolic (the hypoglycaemia the must-be-excluded), the post-malaria the neurological syndrome.[4][12]
- The pathology — the sequestration of the parasitised erythrocytes in the cerebral microvasculature (the cytoadherence the PfEMP-1 to the ICAM-1, the E-selectin; the rosetting; the reduced the deformability). The retinopathy (the white-centred the haemorrhages, the retinal whitening, the vessel discolouration — the unique to the malaria, the distinguishes the true the cerebral malaria from the incidental parasitaemia plus the coma).[12]
- The management — the IV artesunate the immediate (the do NOT the wait the smear the if the high the suspicion), the airway the protection, the seizure the control (the NOT the phenobarbital the routine — the high-dose the phenobarbital the increased the mortality in the SEAQUAMAT), the normoglycaemia, the avoid the prophylactic the mannitol (the no evidence). The CT to exclude the mass or the haemorrhage. The lumbar the puncture the once the stable and the coagulation the normal — to exclude the concomitant the meningitis.[3][4]
ARDS, AKI and the blackwater fever in the severe malaria
- The malaria ARDS — the commonest the pulmonary manifestation (the 5 to 25 per cent of the severe); the alveolar-capillary the leak, the cytoadherence in the pulmonary the microvasculature, the inflammatory the cytokines. The worse in the non-immune and the high-parasitaemia. The lung-protective the ventilation, the conservative the fluids, the prone the positioning, the iNO / the ECMO the rescue. The differentiate the from the fluid-overload the pulmonary the oedema.[1][4]
- The malaria AKI — the 30 to 40 per cent of the severe; the mechanisms the multifactorial (the acute the tubular the necrosis from the renal the microvascular the sequestration, the haemoglobinuria, the hypovolaemia, the DIC). The blackwater fever — the massive the intravascular the haemolysis (the Hb the over 265 µmol/L, the haemoglobinuria, the dark-red the urine) — the seen with the quinine and the severe falciparum. The renal the replacement the therapy the early (the CVVH / the haemodiafiltration); the usually the reversible.[1][4]
- The exchange transfusion — the controversial. The rationale: the rapid the reduction of the parasitaemia the independent of the drug the action. The indications (the traditional): the parasitaemia the over 10 per cent in the non-immune; the over 5 per cent with the end-organ (the cerebral, the ARDS, the AKI); the failure to clear the parasitaemia the within 24 hours. The evidence: the observational the studies the conflicting; the no RCT; the modern the IV artesunate the rapidly effective (the over 95 per cent clearance the within 48 hours) the reduces the marginal the benefit. The not the routine — the consider the individual the basis.[4]
Post-malaria neurological syndrome — the post-treatment trap
- The post-malaria neurological syndrome (PMNS) — the self-limiting the acute the confusional state, the seizures, the tremor, the ataxia, the psychosis the occurring the days to the weeks the AFTER the clearance of the parasitaemia and the recovery. The more the common after the quinine and the severe the cerebral malaria. The pathogenesis the immune-mediated. The differentiate the from the recurrent the malaria (the smear negative), the meningoencephalitis, the drug the toxicity. The management the supportive (the anticonvulsants, the sedation); the steroids the sometimes the used. The resolves the within the days to the weeks.[1][4]
Dengue and severe TB
Dengue (severe / dengue shock syndrome)
- The dengue virus (the flavivirus — the four the serotypes, the DEN-1 to DEN-4; the homotypic the immunity the lifelong, the heterotypic the transient — the second the infection the worse, the antibody-dependent the enhancement) — the Aedes mosquito (the aegypti the principal). The endemic the tropics.[1][5]
- The phases — the febrile (the day 2 to 7, the high the fever, the retro-orbital the pain, the myalgia, the rash — the "breakbone"), the critical (the plasma leak at the defervescence — the day 3 to 7, the 24 to 48 the hours the around the fever the settling), the recovery (the day 7 to 10, the reabsorption, the risk of the fluid-overload the pulmonary the oedema).[5]
- The diagnosis — the NS1 antigen (the early — the day 1 to 5; the sensitive in the febrile the phase), the IgM (the from the day 4 to 5, the peaks the 2 weeks), the IgG (the secondary the infection the high the titre early), the RT-PCR (the first 5 days). The combination of the NS1 plus the IgM the maximises the yield. The thrombocytopenia (the platelets the under 100), the leucopenia, the rising the haematocrit (the over 20 per cent the baseline = the significant the plasma the leak).[5]
- The severe dengue (WHO 2009) — the plasma leakage (the pleural effusion, the ascites, the haemoconcentration — the haematocrit the over 20 per cent the baseline), the shock (the dengue shock syndrome — the narrow pulse pressure the under 20 mmHg), the severe bleeding (the GI, the menorrhagia, the intracranial), the severe organ impairment (the hepatitis the AST the over 1000, the encephalitis, the myocarditis, the AKI).[5]
- The warning signs (the transition to the severe — the day the defervescence the highest-risk) — the abdominal the pain or the tenderness, the persistent the vomiting (the over 3 in the day), the clinical the fluid the accumulation (the ascites, the pleural the effusion), the mucosal the bleeding, the lethargy / the restlessness, the postural the hypotension, the hepatomegaly the over 2 cm, the rapid the platelet the drop the with the rising the haematocrit. The any the one the warning the sign the = the admit / the ICU-monitor.[5]
- The management — the fluid resuscitation (the cautious the crystalloid in the leak phase — the titrate to the perfusion and the haematocrit; the avoid the overload — the pulmonary the oedema in the recovery the phase when the leak the resolves), the isotonic the crystalloid the first-line (the 5 to 10 mL/kg the bolus the over the 30 min the for the shock; the repeat the only the if the still the shocked; the NEVER the rapid the boluses the in the stable-with-leak), the colloid the reserved the for the refractory the shock, the platelets or the FFP for the bleeding (the NOT the prophylactic the platelets — the no the outcome the benefit, the risk the fluid the overload), the monitor the haematocrit. The paracetamol (the NOT the NSAIDs — the bleeding risk, the platelet the function).[5][6]
Severe TB (miliary / TB meningitis)
- The Mycobacterium tuberculosis. The disseminated (the miliary — the pulmonary plus the extra-pulmonary; the ARDS, the miliary the CXR pattern — the 1 to 2 mm the nodules the uniformly the distributed). The TB meningitis — the basal meningitis, the cranial-nerve palsies (the VI the commonest), the hydrocephalus, the vasculitis (the stroke).[1]
- The diagnosis — the AFB smear, the GeneXpert or the NAAT (the rapid, the detects the rifampicin the resistance), the culture (the gold the standard, the 2 to 6 the weeks). The CSF (the TB meningitis — the lymphocytic the pleocytosis, the low the glucose the under 2.2, the high the protein the over 1.5, the cobweb the coagulum).[1]
- The treatment — the RIPE (the rifampicin, the isoniazid, the pyrazinamide, the ethambutol) the 2 months plus the RH the 4 months; the TB meningitis the 4-drug plus the steroids (the dexamethasone — the mortality the benefit, the tapered the over the 6 to 8 weeks). The MDR-TB — the individualised, the longer. The isolation (the negative the pressure) for the pulmonary.[1]
- The steroids for the TB meningitis (the Dexamethasone, the tapered over 6-8 weeks — the definitive the mortality the benefit, the Thwaites 2004 NEJM) and the TB pericarditis (the mortality the benefit).[1]
- The isolation (the negative pressure) for the pulmonary until the smear-negative (the usually the 2 weeks the of the effective the therapy).[1]
Melioidosis (Burkholderia pseudomallei) — the "the great mimicker"
- The Burkholderia pseudomallei — the Gram-negative the bacillus (the oxidase-positive, the bipolar the safety-pin the staining) the endemic the to the northern the Australia (the Top the End), the Southeast the Asia (the Thailand, the Cambodia, the Vietnam), the and the increasing the recognised the globally (the India, the Brazil, the the Pacific). The environmental the saprophyte — the soil and the surface the water. The transmission the percutaneous (the inoculation the from the soil, the occupational the risk — the rice the farmers, the gardeners), the inhalation (the severe the pneumonic the after the monsoonal the rains, the storms), the ingestion. The incubation the 1 to 21 days the (the acute), BUT the latency the up to the 62 years — the longest of the any the bacterium (the reactivation the decades the later).[7][8]
- The risk the factors — the diabetes the mellitus (the 30 to 60 per cent), the hazardous the alcohol the use, the chronic the renal the disease, the chronic the lung the disease, the immunosuppression (the steroid, the TNF-inhibitor, the malignancy), the thalassaemia. The healthy the rare. The mortality the up to the 40 per cent the in the septicaemic.[7]
- The clinical the phenotypes — the pneumonia (the 50 per cent — the most the common; the upper-the-lobe the consolidation, the cavitation, the mimic the TB); the bacteraemic the septic the shock (the 20 per cent — the mortality the over 40 per cent, the high the mortality the within the 48 the hours); the disseminated (the multiple the abscesses — the liver, the spleen, the subcutaneous, the parotid [the children], the prostate [the men], the brain [the brainstem the abscess the classic]); the localised (the skin the ulcer, the abscess the at the inoculation the site).[7]
- The diagnosis — the culture (the gold the standard — the blood, the sputum, the pus, the urine; the Burkholderia the grows the on the standard the media, the Ashdown the selective the medium, the 24 to 72 the hours; the oxidase the positive, the wrinkly the colonies; the NEVER the discard the as the contaminant the "Pseudomonas-like" — the mis-identification the common and the dangerous), the serology (the IHA — the rising the titre the over 4-fold the supportive, the single the high the titre the not the diagnostic in the endemic), the PCR (the rapid, the point-of-the-care the under the development). The CT (the abdomen — the liver and the spleen the abscesses the "honeycomb"; the chest — the pneumonia, the cavitation; the prostate the in the men).[7]
- The treatment — the two-phase.[7]
- The intensive the phase (the minimum the 10 to 14 days, the usually the 2 to 4 the weeks): the IV ceftazidime (the 2 g the q6h, the 50 mg/kg the q6h the child) OR the IV meropenem (the 1 g the q8h, the severe the disease, the septic the shock, the meningitis, the cannot the tolerate the ceftazidime). The addition of the IV TMP-SMX (the trimethoprim-sulfamethoxazole the 8/40 mg/kg/day the divided the q8h) the is the no the longer the routine in the intensive the phase (the no the outcome the benefit the in the Merck the trial, the high the sodium the load, the nephrotoxicity) — the reserve the for the salvage.
- The eradication the phase (the 3 to 6 the months, the essential — the relapse the rate the over 20 per cent the without): the oral TMP-SMX (the 6/30 mg/kg/day the divided the BD, the + the folic the acid) PLUS the doxycycline (the historical) — the modern the monotherapy the TMP-SMX the equivalent (the ATBM the trial, the Limmathurotsakul 2014). The relapse the risk the factors — the inadequate the eradication the course, the non-adherence, the severe the underlying the disease.
- The supportive — the ICU for the septic the shock (the early the vasopressors, the noradrenaline the first-line), the ventilation for the ARDS (the lung-protective), the source the control (the drain the abscesses — the liver, the spleen, the prostate; the debride the necrotic the skin), the glycaemic the control (the diabetes the common).[7][9]
Severe enteric fever — the typhoid (Salmonella Typhi)
- The Salmonella enterica the serovar the Typhi (the Gram-negative, the human-only the pathogen, the no the animal the reservoir) — the faecal-oral the transmission (the contaminated the water and the food, the chronic the carrier). The incubation the 7 to 14 the days (the 3 to 60 the range). The endemic the to the South the Asia (the Pakistan, the India, the Bangladesh — the XDR the strains the now the common the in the Pakistan, the resistant the to the ampicillin, the chloramphenicol, the TMP-SMX, the fluoroquinolones), the sub-Saharan the Africa. The annual the global the burden the over 11 the million the cases, the over 100,000 the deaths.[10][11]
- The clinical the course (the classic — the "stepwise the fever" the if untreated) — the week 1: the insidious the rising the fever (the stepwise, the plateau the 39 to 40°C), the relative the bradycardia (the Faget the sign), the headache, the dry the cough, the constipation (the children the diarrhoea), the abdominal the pain, the rose the spots (the faint the salmon-coloured the maculopapules the on the trunk, the 2 to 4 mm), the hepatosplenomegaly. The week 2: the sustained the fever, the delirium (the "typhoid the state"), the "pea-soup" the diarrhoea, the distended the abdomen. The week 3: the complications — the intestinal the haemorrhage (the 1 to 5 per cent), the intestinal the perforation (the 1 to 3 per cent — the classic, the Peyer's-patch the ulceration the of the terminal the ileum; the surgical the emergency, the mortality the over 10 per cent), the myocarditis, the DIC, the encephalopathy, the hepatitis, the cholecystitis, the osteomyelitis. The week 4: the defervescence, the recovery.[10]
- The diagnosis — the blood the culture (the 50 to 80 per cent the yield the in the week 1, the falls the over the time; the 5 to 10 mL the before the antibiotics), the bone the marrow the culture (the 90 per cent the yield, the most the sensitive, the holds the after the antibiotics), the stool the culture (the late the disease, the carrier the detection), the Widal (the agglutination — the low the sensitivity and the specificity, the not the recommended the for the diagnosis the alone). The PCR (the emerging, the XDR the detection).[10]
- The treatment — the empiric the guided the by the local the susceptibility and the travel the history.[10]
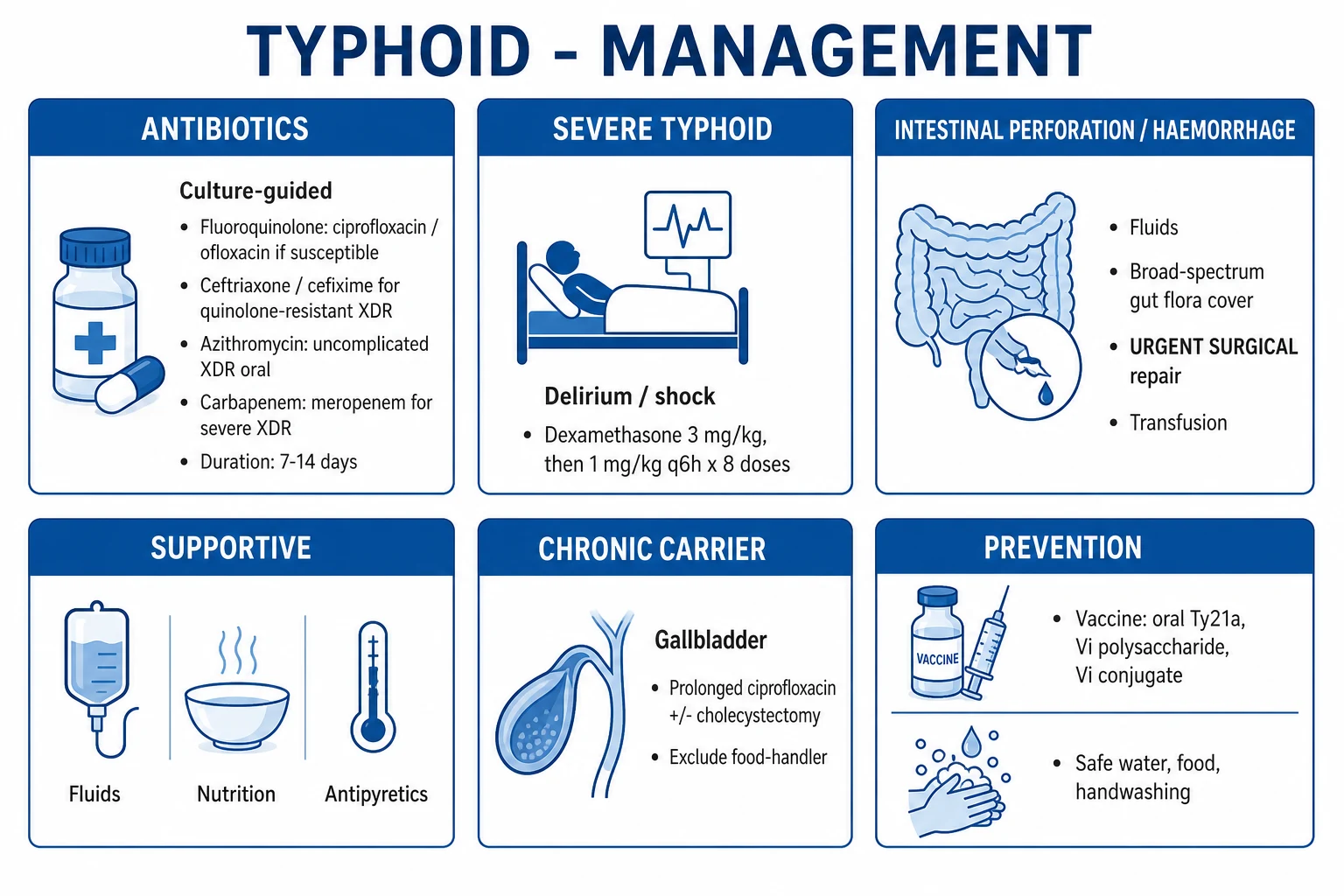
- The XDR the typhoid (the Pakistan the travel) — the ceftriaxone (the 2 to 3 g the IV the daily) OR the azithromycin (the 500 mg the oral the daily). The azithromycin the for the uncomplicated the outpatient; the ceftriaxone the for the severe.
- The non-XDR — the ceftriaxone OR the azithromycin OR the fluoroquinolone (the ciprofloxacin — the IF the susceptible; the nalidixic-acid-the-resistant the strains the higher-the-failure).
- The severe (the perforation, the shock, the encephalopathy) — the IV ceftriaxone PLUS the metronidazole (the cover the anaerobes the at the perforation), the surgery the for the perforation (the primary the repair or the resection-anastomosis), the dexamethasone (the 3 mg/kg the loading the then the 1 mg/kg the q6h the for 2 days — the mortality the benefit the in the delirium/coma, the 1986 the trial; the controversial the but the used the in the severe).
- The carrier the state — the 2 to 5 per cent the become the chronic the biliary the carriers (the gallbladder the focus — the Salmonella the in the gallstones; the "Typhoid the Mary"). The eradicate with the ciprofloxacin (the 4 the weeks) the if the susceptible, OR the cholecystectomy (the resistant). The public-the-health the notification.[10]
Rickettsial disease — scrub typhus and the typhus group
- The scrub typhus — the Orientia tsutsugamushi (the Orientia, the not the Rickettsia, the cell-wall-the-deficient) — the trombiculid the mite (the chigger) the vector, the larval-stage the transmission. The endemic the "tsutsugamushi the triangle" — the northern the Australia (the far the north the Queensland, the Northern the Territory), the Southeast the Asia, the Japan, the Korea, the China, the India. The incubation the 6 to 21 the days. The eschar (the black the necrotic the scab the at the bite the site, the painless) — the pathognomonic, the present the 50 to 80 per cent — the LOOK the in the axillae, the groins, the scalp, the under the breasts. The lymphadenopathy, the fever, the headache, the myalgia, the maculopapular the rash (the truncal, the sparing the face/palms/soles — the usually).[1]
- The scrub typhus the severe — the meningoencephalitis (the CSF the lymphocytic), the ARDS (the common — the interstitial the pneumonia), the AKI, the hepatitis, the DIC, the myocarditis, the shock. The mortality the untreated the up to the 30 per cent, the treated the under 5 per cent.[1]
- The murine (endemic) typhus — the Rickettsia typhi (the rat the flea) — the worldwide, the urban, the milder the than the scrub; the fever, the headache, the rash (the 50 per cent, the truncal, the spreads the centripetally). The epidemic the typhus — the R. prowazekii (the human the body the louse) — the severe, the war the and the famine, the recrudescence the years the later (the Brill-Zinsser).[1]
- The spotted-the-fever the group (Rickettsia) — the R. rickettsii (the RMSF — the North the America, the tick, the rash the on the palms and the soles, the high the mortality the if the delayed), the R. australis (the Queensland the tick the typhus), the R. conorii (the Mediterranean the spotted the fever, the "marseilles" the fever), the R. honei (the Flinders the Island).[1]
- The diagnosis — the clinical (the exposure the history, the eschar, the rash) — the START the empiric the doxycycline the NEVER the wait the serology. The serology (the IFA — the gold the standard, the four-fold the rise the between the acute the and the convalescent — the retrospective; the single the titre the not the diagnostic), the PCR (the blood, the eschar the swab, the early). The Weil-Felix (the agglutination — the obsolete, the low the sensitivity).[1]
- The treatment — the doxycycline (the 100 mg the BD, the 7 to 10 the days; the children the and the pregnant the included — the short the course the safe; the do NOT the withhold the in the severe). The azithromycin (the 500 mg the daily, the 3 to 5 the days) the alternative the in the pregnancy and the doxycycline-the-intolerant. The treat the empirically the on the suspicion — the delay the doxycycline the worsens the outcome.[1]
- The chloramphenicol (the historical) — the less the effective the than the doxycycline, the higher the relapse, the aplastic the anaemia — the not the recommended.[1]
Leprosy (Hansen disease) in the ICU context
- The Mycobacterium leprae (the uncultivable, the obligate the intracellular, the slow — the doubling the 14 days; the tropism the for the Schwann the cells and the macrophages) — the droplet the transmission (the prolonged the household the contact), the incubation the 2 to 10 the years. The endemic the to the India, the Brazil, the Indonesia, the and the pockets the of the northern the Australia (the Torres the Strait).[1]
- The spectrum the (Ridley-Jopling) — the tuberculoid (the TT — the one the to the few the anaesthetic the hypopigmented the patches, the thickened the nerves, the strong the cell-the-mediated, the paucibacillary), the borderline (the BT, the BB, the BL), the lepromatous (the LL — the diffuse the infiltration, the nodules, the plaques, the "leonine the facies", the nasal the collapse, the testicular, the ocular; the multibacillary; the anergy).[1]
- The ICU the relevance — the type 1 (reversal) the reaction (the borderline the patients — the cell-the-mediated the upswing, the painful the inflamed the patches and the nerves, the rapid the nerve the damage, the steroids), the type 2 (erythema the nodosum the leprosum, ENL) (the lepromatous — the immune-the-complex, the fever, the painful the nodules, the iritis, the orchitis, the dactylitis, the glomerulonephritis, the high the CRP — the steroids, the thalidomide, the TNF-inhibitor). The leprosy the crisis the ICU the admission.[1]
- The treatment (the WHO the multidrug) — the paucibacillary (the rifampicin the 600 mg the monthly PLUS the dapsone the 100 mg the daily, the 6 the months), the multibacillary (the rifampicin the 600 mg the monthly PLUS the dapsone the 100 mg the daily PLUS the clofazimine the 300 mg the monthly and the 50 mg the daily, the 12 the months). The dapsone the hypersensitivity the syndrome (the 2 to 6 the weeks — the fever, the rash, the hepatitis, the methaemoglobinaemia, the agranulocytosis — the stop, the supportive, the steroids). The G6PD the check before the dapsone.[1]
Severe influenza and COVID-19
Severe influenza
- The influenza A or B. The severe — the viral pneumonia, the ARDS, the secondary bacterial pneumonia (the strep the pneumo, the staph the aureus — the incl the MRSA, the highest the mortality), the myocarditis, the encephalitis (the ANE in the children).[1]
- The treatment — the oseltamivir (the 75 mg the BD, the 5 the days; the double the dose the severe; the within 48 the hours; the severe the regardless), the zanamivir (the inhaled, the severe the bronchospasm the avoid), the peramivir (the IV), the baloxavir (the cap-dependent the endonuclease the inhibitor). Plus the secondary bacterial the cover.[1]
Severe COVID-19
- The SARS-CoV-2. The severe — the hypoxic the respiratory the failure or the ARDS, the cytokine the storm, the thromboembolism (the high the VTE the risk), the multisystem (the myocarditis, the AKI, the stroke, the DIC).[1]
- The treatment — the dexamethasone (the RECOVERY — the 6 mg the 10 the days; the mortality the benefit the in the hypoxic), the remdesivir (the severe), the tocilizumab or the baricitinib (the steroid-the-reflex the escalation the in the cytokine the storm, the high the CRP), the anticoagulation (the prophylactic the to the therapeutic the per the D-dimer), the oxygen or the ventilation (the prone, the lung-protective).[1]
Exam practice
SAQ — Severe falciparum malaria with ARDS in a returned traveller
10 minutes · 10 marks
A 42-year-old non-immune businessman returned from a 2-week trip to Papua New Guinea 9 days ago. He presents with 3 days of high fever, rigors, and progressive confusion. GCS 9 (E2V3M5). Temp 39.4°C, BP 88/52, HR 124, RR 34, SpO2 86% on room air, bilateral crackles. Thick blood smear shows Plasmodium falciparum ring forms, parasitaemia 14%. Hb 68 g/L, glucose 1.8 mmol/L, lactate 5.6, creatinine 220 µmol/L. CXR bilateral infiltrates; PaO2/FiO2 180 on 15 L/min via non-rebreather.
SAQ — Melioidosis pneumonia in a returned traveller
10 minutes · 10 marks
A 55-year-old type-2 diabetic man with heavy alcohol use presents from far north Queensland with 5 days of fever, productive cough, and right pleuritic chest pain. He works as a rice farmer. Temp 39.1°C, BP 95/58, HR 118, RR 28, SpO2 92% on 4 L/min. CXR: right upper lobe consolidation with cavitation. Blood cultures at 48 h grow an oxidase-positive Gram-negative bacillus with bipolar safety-pin staining and wrinkly colonies. Hb 110, WCC 18.5, glucose 14, creatinine 145; CT abdomen shows a 4 cm splenic abscess.
Red flags
ClinicalPearls — the exam-exhaustive high-yield points
FlowSteps — the time-critical tropical-infection workflows
The severe falciparum malaria — the first the six hours
1. The RECOGNISE — the returned traveller + the fever (the ANY within the 3 months) = the malaria until the proven otherwise
The ANY the fever the in the returned-the-traveller the from the malaria-the-endemic the area = the malaria the smear the within the hour. The clinical: the cyclical the fever (the tertian — the every the 48 h, the falciparum the often the irregular), the rigors, the headache, the splenomegaly, the jaundice, the dark the urine. The severe the features (the ANY the one) = the ICU: the cerebral (the GCS the under 11), the seizures, the ARDS, the shock, the AKI, the Hb the under 70, the glucose the under 2.2, the parasitaemia the over 2 per cent (or the over 10 the non-immune), the acidosis, the blackwater.
2. The DIAGNOSE — the thick + the thin the smear, the RDT
The THICK the smear (the detection — the low the parasitaemia); the THIN the smear (the species — the falciparum the banana-the-shaped the gametocytes, the ring the forms, the double-the-chromatin the dots; the parasitaemia the per cent). The RDT (the HRP-2 the antigen the — the falciparum). The repeat the every the 6 to 12 h the if the first the negative the and the suspicion the high. The bedside the glucose the immediately (the hypoglycaemia the common). The bloods (the FBC, the U&E, the LFT, the coagulation, the lactate, the blood the gas). The exclude the other (the dengue the NS1 the + the IgM; the scrub the typhus the if the eschar; the typhoid the if the abdominal).
3. The IV ARTESUNATE — the 2.4 mg/kg the at 0, 12, 24 h the then the daily
The IV the artesunate the 2.4 mg/kg the at 0, 12, 24 h the then the 2.4 mg/kg the daily — the WHO the first-line. The NEVER the quinine the if the artesunate the available (the AQUAMAT / the SEAQUAMAT the mortality the benefit). The administer the within the hour. The do NOT the wait the smear the if the severe (the empirical). The add the doxycycline the 100 mg the BD the or the clindamycin the (the radical the cure) the after the 24 h. The single the low-dose the primaquine the (the 0.25 mg/kg) the gametocytocidal (the transmission-the-block; the check the G6PD the first).
4. The SUPPORTIVE — the ICU, the ventilation, the glucose, the transfusion
The airway / the ventilation the for the ARDS (the lung-protective — the 6 mL/kg, the plateau the under 30; the prone; the conservative the fluids). The glucose the monitor the hourly — the treat the 10 to 50 per cent the dextrose (the quinine-the-exacerbated). The transfusion the if the Hb the under 70 (or the under 80 the severe). The CVVH / the haemodiafiltration the for the AKI the / the blackwater. The exchange the transfusion the for the over 10 per cent the parasitaemia the non-immune the or the over 5 per cent the end-organ (the controversial, the individual). The benzodiazepines the for the seizures (the NOT the phenobarbital the prophylactic). The CT the if the cerebral / the focal (the exclude the haemorrhage).
5. The MONITOR — the parasitaemia the every the 12 h (the clearance the 24 to 48 h)
The repeat the smear the every the 12 h. The clearance the expected the by the 48 to 72 h. The NO the clearance the by the 72 h = the artesunate the resistance (the emerging the Greater the Mekong) — the consult the infectious-the-diseases; the consider the quinine the + the doxycycline/clindamycin. The artesunate-the-induced the delayed the haemolysis the (the 1 to 3 the weeks the post — the check the Hb the follow-up). The post-malaria the neurological the syndrome the (the days the to the weeks the post) — the self-limiting.
The dengue the shock — the leak-phase the fluid the management (the first the 24 h)
1. The RECOGNISE the leak — the rising the haematocrit (the over 20 per cent the baseline), the narrow the pulse the pressure (the under 20 mmHg), the platelets the under 50, the warning the signs
The dengue the critical the phase the = the around the defervescence (the day 3 to 7, the 24 to 48 h). The leak the signs: the haematocrit the rising (the over 20 per cent the baseline), the platelets the dropping, the WCC the dropping, the narrow the pulse the pressure (the under 20 mmHg), the clinical the fluid the (the gallbladder the wall the oedema, the pleural the effusion, the ascites). The warning the signs (the any the one) = the ICU: the abdominal the pain, the persistent the vomiting, the lethargy, the restlessness, the hepatomegaly, the mucosal the bleeding, the postural the hypotension. The NS1 the + the IgM the confirm.
2. The GROUP A — the no the leak; the oral the fluids, the paracetamol
The stable, the tolerating the oral, the haematocrit the stable, the no the warning the signs. The oral the fluids (the 2 to 3 L the daily), the paracetamol (the NOT the NSAIDs), the monitor the platelets the + the haematocrit the daily. The warn the about the warning the signs; the return the if the worse.
3. The GROUP B — the leak; the cautious the IV the crystalloid (the titrate to the haematocrit the + the perfusion)
The leak the present the but the stable. The isotonic the crystalloid the (the Ringer's the lactate the or the 0.9 per cent the saline) the 5 to 7 mL/kg/h the for the 1 to 2 h, the then the reduce the 3 to 5 mL/kg/h the titrate to the haematocrit (the fall = the resolve the leak; the rise = the worsening). The monitor the every the 1 to 2 h: the BP, the pulse the pressure, the urine the output, the haematocrit, the platelets. The colloid the reserved the for the refractory.
4. The GROUP C — the DSS; the 5 to 10 mL/kg the bolus the over 30 min (the repeat the ONLY the if the still the shocked)
The dengue the shock the syndrome (the narrow the pulse the pressure the under 20 the OR the hypotension). The 5 to 10 mL/kg the isotonic the crystalloid the over 30 min — the reassess; the repeat the ONLY the if the still the shocked (the do NOT the blind the repeated the boluses — the pulmonary the oedema). The colloid the (the dextran, the gelatin, the starch) the if the refractory (the Wills 2005 the — the three the fluids the equivalent the in the moderate; the dextran the marginal the in the severe). The blood the / the FFP the for the bleeding. The ICU.
5. The RECOVERY the phase — the AVOID the overload (the leak the resolves; the pulmonary the oedema the if the fluids the continued)
The reabsorption the phase (the day 7 to 10): the haematocrit the falling, the platelets the rising, the appetite the returning, the bradycardia (the second the slower-the-phase). The STOP the IV the fluids the as the leak the resolves — the over-resuscitation the pulmonary the oedema the in the recovery the = the common the iatrogenic. The wean the fluids the gradually. The watch the for the haemolytic-the-uraemic (the rare), the encephalopathy, the myocarditis.
The melioidosis — the diagnostic-and-treatment the pathway
1. The RECOGNISE — the diabetic-the-alcoholic-the returned-the-traveller + the pneumonia / the abscess / the sepsis
The risk the profile the (the diabetes, the alcohol, the chronic the kidney, the immunosuppression, the northern-the-Australia-the-or-the-Southeast-Asia-the exposure). The pneumonia the (the upper-lobe, the cavitation, the mimic the TB), the liver-the-spleen the abscess, the parotid (the child), the prostate (the man), the septic the shock. The latency the decades — the ANY the exposure the history the relevant. The mortality the up to the 40 per cent the in the septicaemic.
2. The DIAGNOSE — the blood + the pus + the sputum the culture; the NEVER the discard the as the contaminant
The culture the (the blood, the sputum, the pus, the urine) — the grows the 24 to 72 h the on the standard the media, the Ashdown the selective. The oxidase the positive, the wrinkly the colonies, the bipolar the safety-pin the staining. The NEVER the discard the as the "Pseudomonas the contaminant" — the single the most the dangerous the laboratory the error. The serology (the IHA — the rising the titre the supportive; the single the high the not the diagnostic the in the endemic). The CT the (the abdomen — the liver-the-spleen the "honeycomb" the abscess; the prostate; the chest; the brain the if the neurological).
3. The INTENSIVE the phase — the IV ceftazidime (the 2 g the q6h) OR the meropenem (the severe)
The IV the ceftazidime the 2 g the q6h (the 50 mg/kg the q6h the child) — the first-line. The IV the meropenem the 1 g the q8h — the severe (the septic the shock, the meningitis, the ARDS, the cannot the tolerate the ceftazidime). The minimum the 10 to 14 the days (the usually the 2 to 4 the weeks). The NOT the routine the addition the of the TMP-SMX the (the no the outcome the benefit the in the intensive; the high the sodium the load). The salvage the — the add the TMP-SMX the if the refractory.
4. The SOURCE the CONTROL — the drain the abscesses; the debride the necrotic
The drainage the of the liver-the-spleen-the-prostate the abscesses (the percutaneous; the surgical the if the fail). The debridement the of the necrotic the skin-the-soft-tissue. The prostate the abscess the (the men) — the transurethral the resection the or the drainage. The repeat the CT the to the confirm the resolution.
5. The ERADICATION the phase — the oral TMP-SMX the 3 to 6 the months (the relapse the over 20 per cent the without)
The oral the TMP-SMX the 6/30 mg/kg/day the divided the BD (the + the folic the acid) — the 3 to 6 the months (the 6 the months the for the neurological, the osseous, the severe the disseminated). The monotherapy the equivalent the to the + the doxycycline (the ATBM the trial). The adherence the essential — the relapse the rate the over 20 per cent the without. The folic the acid the (the prevent the megaloblastic). The G6PD the not the contraindication the (the low-the-dose). The follow-up the serology the (the falling the titre the = the resolution).
Compare — the side-by-side the exam the tables
[2] [6] [2] [8] [6]Key trials and evidence
The SEAQUAMAT — the artesunate vs the quinine in the Asian the adults (PMID 16125588)
The AQUAMAT — the artesunate vs the quinine in the African the children (PMID 21062666)
The Wills 2005 the NEJM — the three the fluids the in the dengue the shock (PMID 16135832)
The Limmathurotsakul 2016 the Nature the Microbiology — the melioidosis the global the burden (PMID 27571754)
The Wiersinga 2018 the Nat Rev Dis Primers — the melioidosis the comprehensive the review (PMID 29388572)
The Savelkoel 2022 the Lancet ID — the melioidosis the call-to-the-action the neglected-tropical-the-disease (PMID 34953519)
The Parry 2002 the NEJM — the typhoid the fever the comprehensive the review (PMID 12456854)
The GBD 2017 the typhoid-the-paratyphoid — the global the burden (PMID 30792131)
The Maude 2009 — the malarial the retinopathy the distinguishes the true the cerebral the malaria (PMID 19344925)
Differential — the undifferentiated the febrile the returned-the-traveller
- The malaria — the within the months; the cyclical; the splenomegaly; the smear.
- The dengue — the within the 2 the weeks; the "breakbone"; the rash; the thrombocytopenia; the NS1.
- The enteric the fever (the typhoid) — the within the 3 the weeks; the stepwise; the relative the bradycardia; the rose the spots; the blood the culture.
- The rickettsial (the scrub the typhus) — the within the 3 the weeks; the eschar; the doxycycline.
- The melioidosis — the any; the diabetic-the-alcoholic; the pneumonia-the-abscess; the culture.
- The leptospirosis — the within the 4 the weeks; the animals / the water; the conjunctival the suffusion; the Weil (the jaundice, the AKI, the bleeding).
- The the viral the haemorrhagic the fevers — the within the 3 the weeks; the Ebola, the Lassa, the dengue-the-severe, the yellow the fever; the isolate / the public-the-health.
- The the amoebic the liver the abscess — the Entamoeba; the single the right-lobe; the metronidazole the + the diloxanide.[1]
Prognosis
[2]Summary — the exam the one-liners
- The IV artesunate (the 2.4 mg/kg the at 0, 12, 24 h the then the daily) the WHO the first-line for the severe the falciparum — the superior the to the quinine (the AQUAMAT / the SEAQUAMAT the mortality the benefit). The exchange the transfusion for the hyperparasitaemia the controversial.[2][3][4]
- The dengue — the NS1 the early; the cautious the crystalloid the in the leak the phase (the avoid the overload the in the recovery); the paracetamol the NOT the NSAIDs.[5][6]
- The melioidosis — the B. pseudomallei the mis-identified the as the "Pseudomonas the contaminant" — the NEVER the discard; the IV ceftazidime the then the oral TMP-SMX the 3 to 6 months; the latency the decades.[7][8]
- The severe the typhoid — the intestinal the perforation the surgical; the XDR (the Pakistan) the ceftriaxone the or the azithromycin; the dexamethasone the for the encephalopathy.[10][11]
- The scrub the typhus — the eschar (the LOOK); the empiric the doxycycline (the never the wait the serology); the safe the in the pregnancy and the children.[1]
- The TB the meningitis — the RIPE + the steroids (the dexamethasone the mortality the benefit); the GeneXpert; the isolation.[1]
- The severe the COVID-19 — the dexamethasone (the RECOVERY); the anticoagulation; the lung-protective the ventilation.[1]
- The ANY the fever the in the returned-the-traveller the = the malaria the smear the within the hour; the empirical the artesunate the if the severe — the do NOT the wait.[4]
References
- [1]Karnad DR, Nor MBM, Richards GA, et al. Intensive care in severe malaria: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. Journal of critical care, 2018.PMID 29132978
- [2]Dondorp AM, Fanello CI, Hendriksen IC, et al. Artesunate versus quinine in the treatment of severe falciparum malaria in African children (AQUAMAT): an open-label, randomised trial. Lancet, 2010.PMID 21062666
- [3]Dondorp A, Nosten F, Stepniewska K, et al. Artesunate versus quinine for treatment of severe falciparum malaria: a randomised trial (SEAQUAMAT). Lancet, 2005.PMID 16125588
- [4]White NJ, Pukrittayakamee S, Hien TT, et al. Malaria. Lancet, 2014.PMID 23953767
- [5]Simmons CP, Farrar JJ, Nguyen VV, Wills B. Dengue. New England Journal of Medicine, 2012.PMID 22494122
- [6]Wills BA, Nguyen MD, Ha TL, et al. Comparison of three fluid solutions for resuscitation in dengue shock syndrome. New England Journal of Medicine, 2005.PMID 16135832
- [7]Wiersinga WJ, Virk HS, Torres AG, et al. Melioidosis. Nature Reviews Disease Primers, 2018.PMID 29388572
- [8]Limmathurotsakul D, Golding N, Dance DA, et al. Predicted global distribution of Burkholderia pseudomallei and burden of melioidosis. Nature Microbiology, 2016.PMID 27571754
- [9]Savelkoel J, Dance DAB, Currie BJ, et al. A call to action: time to recognise melioidosis as a neglected tropical disease. Lancet Infectious Diseases, 2022.PMID 34953519
- [10]Parry CM, Hien TT, Dougan G, White NJ, Farrar JJ. Typhoid fever. New England Journal of Medicine, 2002.PMID 12456854
- [11]GBD 2017 Typhoid and Paratyphoid Collaborators. The global burden of typhoid and paratyphoid fevers: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Infectious Diseases, 2019.PMID 30792131
- [12]Maude RJ, Beare NA, Abu Sayeed A, et al. The spectrum of retinopathy in adults with Plasmodium falciparum malaria. Transactions of the Royal Society of Tropical Medicine and Hygiene, 2009.PMID 19344925