ICU · Cardiovascular
Acute aortic dissection: type A vs type B, malperfusion, and endovascular management
Also known as Aortic dissection · Type A dissection · Type B dissection · Stanford classification · TEVAR · Malperfusion syndrome
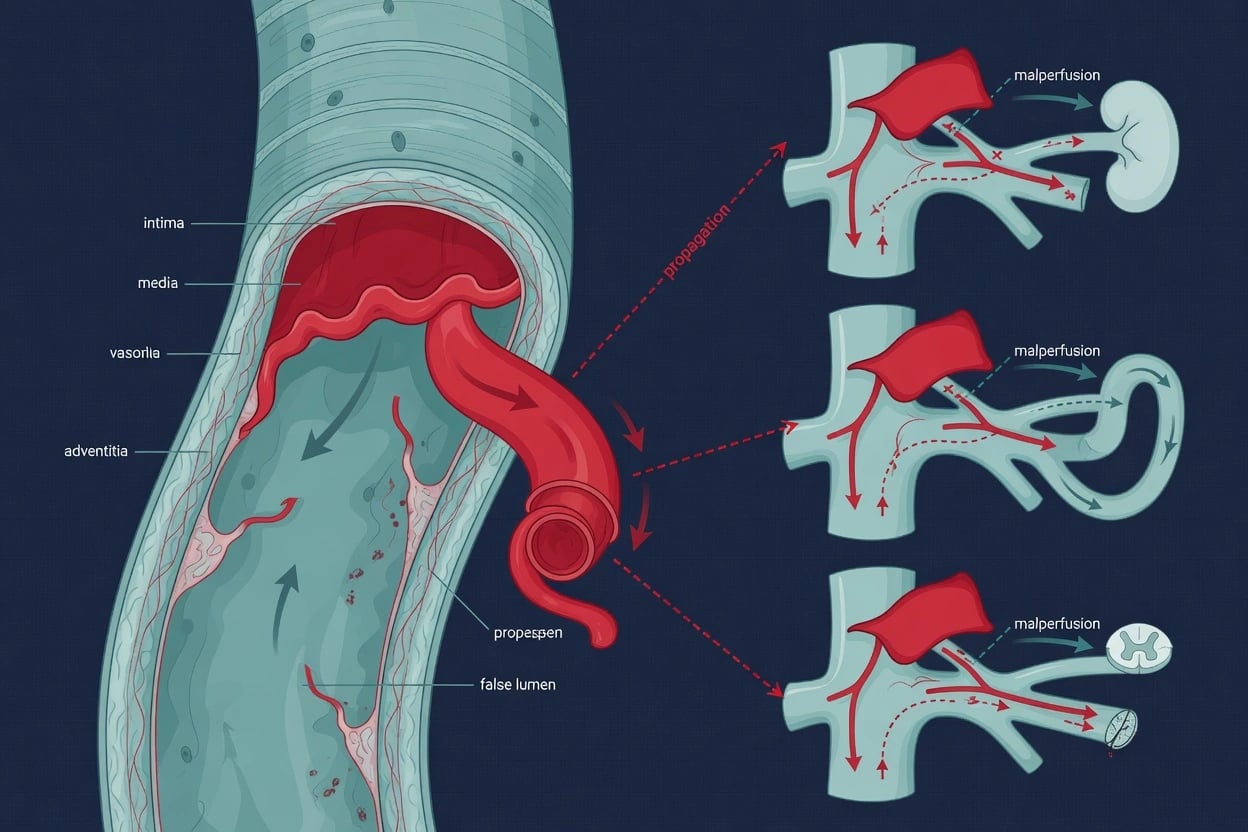
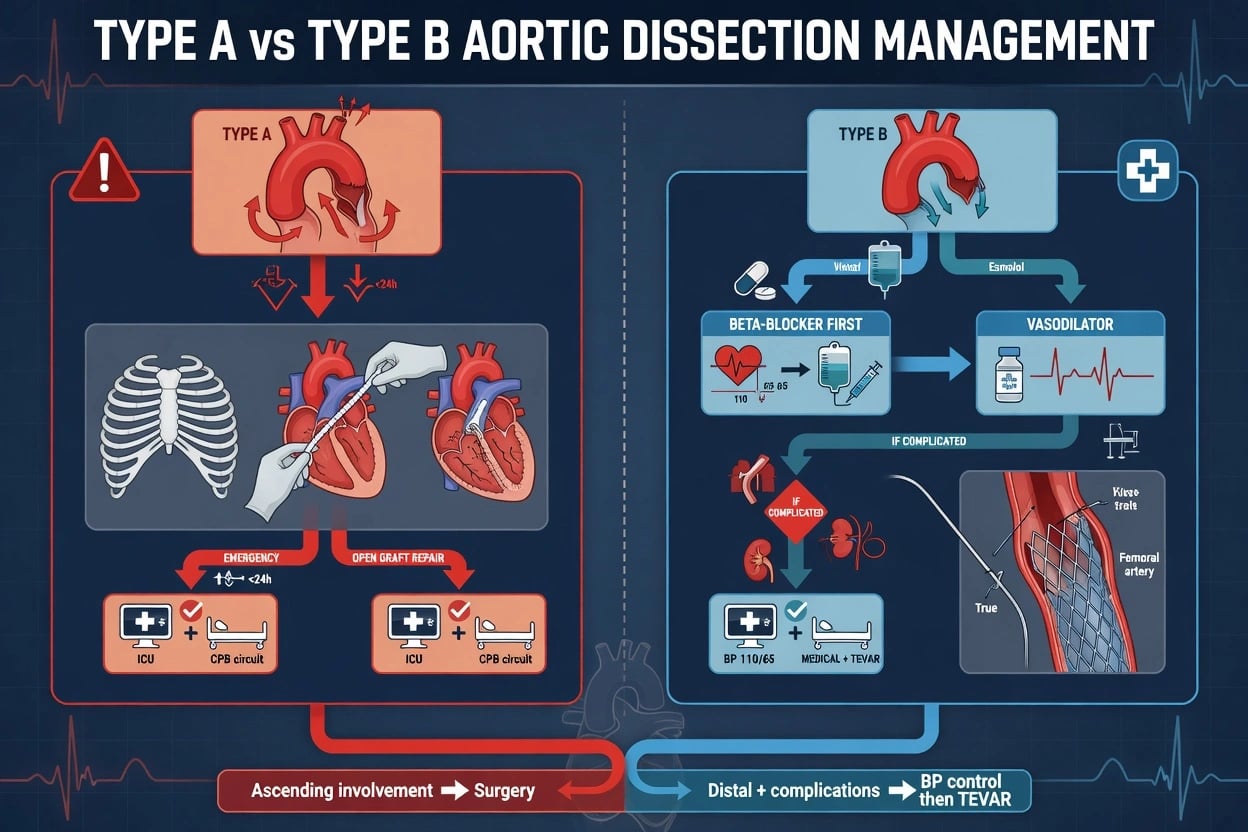
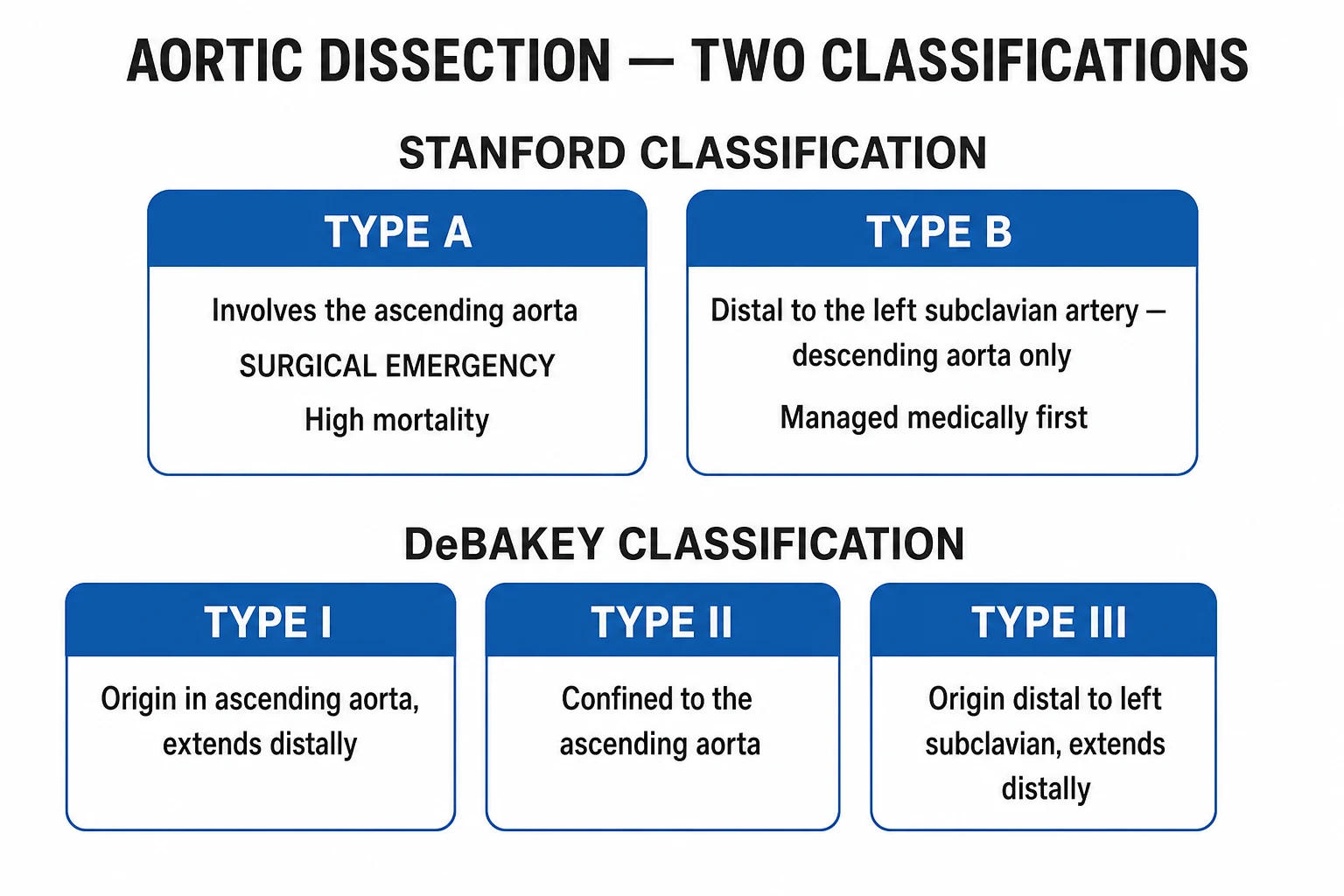
Acute aortic dissection = tear in aortic intima - blood enters media - false lumen - propagation. CLASSIFICATION (Stanford): TYPE A (ascending aorta — 65%) — SURGICAL EMERGENCY (mortality 1-2%/h untreated, 50% in 48h). TYPE B (descending aorta — distal to left subclavian — 35%) — MEDICAL management (beta-blockers, BP control); surgery/endovascular if COMPLICATED (rupture, malperfusion, refractory pain/HTN, rapid expansion). PRESENTATION: sudden TEARING chest/back pain (migrating — tracks dissection propagation), pulse deficits (asymmetric — vessel occlusion), blood pressure differential (20 mmHg between arms), new aortic regurgitation murmur, neurological deficit (stroke, paraplegia — spinal/visceral ischaemia), syncope. RISK FACTORS: hypertension (most important), connective tissue disease (Marfan, Ehlers-Danlos, Loeys-Dietz), bicuspid aortic valve, pregnancy, cocaine, trauma. DIAGNOSIS: CT aortogram (gold standard — intimal flap, true/false lumen, extent, malperfusion). MANAGEMENT: TYPE A — emergency SURGICAL repair (ascending aorta replacement ± AVR ± arch). TYPE B (uncomplicated) — medical (beta-blocker + BP control). TYPE B (complicated) — THORACIC ENDOVASCULAR AORTIC REPAIR (TEVAR) preferred over open surgery. MORTALITY: type A (untreated) 50% in 48h; type B (uncomplicated) 10% in 30 days.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Type A vs Type B aortic dissection
| Feature | Type A (ascending) | Type B (descending — distal to L subclavian) |
|---|---|---|
| Incidence | 65% | 35% |
| Extent | Ascending aorta (may extend to arch/descending) | Descending aorta (distal to left subclavian) |
| Mortality (untreated) | 1-2%/h, 50% in 48h | 10% in 30 days |
| Management | EMERGENCY SURGERY (ascending replacement ± AVR ± arch) | MEDICAL (beta-blocker + BP) if uncomplicated; TEVAR/surgery if complicated |
| Complications | Cardiac tamponade (retrograde into pericardium), AR (annular disruption), stroke (arch vessels), MI (coronary) | Mesenteric ischaemia, renal failure, limb ischaemia, paraplegia (spinal), rupture |
| Surgical urgency | IMMEDIATE (life-threatening) | Selective (only if complicated) |
| BP target | Aggressive (SBP 100-120) pre-op | SBP 100-120 (if uncomplicated — medical) |
Management of acute aortic dissection
- RECOGNISE + IMMEDIATE STABILISATION — (a) CLINICAL: sudden TEARING chest/back pain (migrating), pulse deficits (asymmetric BP >20 mmHg between arms), new AR murmur, neurological deficit (stroke, paraplegia), syncope. (b) IMMEDIATE: 2 large-bore IV, oxygen, monitor (ECG, BP both arms), analgesia (morphine). (c) ECG (exclude MI — dissection can involve coronary — usually RIGHT coronary -> inferior MI). (d) CXR (wide mediastinum — 60% sensitive, not definitive). (e) STAT CT AORTOGRAM (definitive — intimal flap, true/false lumen, extent, malperfusion, rupture). (f) ACT FAST — type A mortality 1-2%/h
- BLOOD PRESSURE CONTROL (CRITICAL — PRE-OP FOR ALL TYPES) — (a) BETA-BLOCKER FIRST (reduce dP/dt — rate of pressure rise — shear stress on aorta -> slows propagation): (i) LABETALOL (alpha+beta) 10-20 mg IV q10min (or infusion 20-80 mg/hr). (ii) ESMOLOL (short-acting beta-1) 500 mcg/kg loading then 50-200 mcg/kg/min (titratable, short half-life — preferred in ICU). (iii) METOPROLOL 5 mg IV (less titratable). (b) TARGET: HR 60-80, SBP 100-120 mmHg (reduce shear + prevent rupture). (c) ADD VASODILATOR after beta-blocker (if BP still high): (i) NICARDIPINE (CCB) 5-15 mg/hr infusion. (ii) NITROPRUSSIDE 0.3-3 mcg/kg/min (potent but cyanide risk — avoid if possible). (iii) AVOID nitroprusside ALONE (without beta-blocker — reflex tachycardia -> increased shear -> WORSE dissection). (d) AVOID: hydralazine (reflex tachycardia), pure vasodilators without beta-block
- TYPE A — EMERGENCY SURGERY — (a) IMMEDIATE transfer to OR (cardiothoracic surgery). (b) PROCEDURE: (i) Median sternotomy. (ii) Cardiopulmonary bypass + hypothermic circulatory arrest (for arch repair). (iii) Resection of torn ascending aorta. (iv) Interposition graft (Dacron) replacement. (v) ± Aortic valve replacement (if annular disruption/AR). (vi) ± Arch repair (if arch involved — more complex). (vii) ± Coronary reimplantation (if dissection involves coronary ostia). (c) MORTALITY: 10-30% (surgical); 50% in 48h untreated. (d) DELAY is the enemy — each hour untreated -> 1-2% mortality. (e) PRE-OP: stabilise (BP control) but DON'T delay surgery for 'stabilisation' — type A needs OR now
- TYPE B UNCOMPLICATED — MEDICAL MANAGEMENT — (a) ADMISSION: ICU/HDU (monitor for complications). (b) BP CONTROL: beta-blocker + vasodilator (target SBP 100-120, HR 60-80). (c) ANALGESIA (morphine — pain contributes to HTN). (d) MONITOR: (i) Serial examination (pulse deficits, abdomen — mesenteric ischaemia, limbs). (ii) Serial CT (at 24-48h — extent, expansion, malperfusion). (iii) Renal function (renal artery involvement). (iv) Lactate (mesenteric ischaemia). (e) DURATION: IV then transition to oral (labetalol, bisoprolol, ACEi/ARB). (f) PAIN: if REFRACTORY pain/HTN despite medical -> complicated -> TEVAR. (g) LONG-TERM: strict BP control (<130/80), serial imaging (CT/MRI at 1, 3, 6, 12 months — for expansion/redissection), beta-blocker lifelong
- TYPE B COMPLICATED — TEVAR (PREFERRED) OR SURGERY — (a) COMPLICATIONS requiring intervention: (i) RUPTURE (haemodynamic instability — emergency). (ii) MALPERFUSION syndrome (mesenteric, renal, limb, spinal — end-organ ischaemia). (iii) REFRACTORY pain or hypertension (despite maximal medical). (iv) RAPID EXPANSION (aneurysmal degeneration — on serial imaging). (v) CONTAINED rupture (on imaging). (b) TEVAR (Thoracic Endovascular Aortic Repair): (i) Stent-graft placed via femoral artery -> covers the entry tear -> excludes false lumen -> restores true lumen flow -> relieves malperfusion. (ii) INSTEAD-XL trial: TEVAR + medical vs medical alone (uncomplicated type B) -> TEVAR had better remodelling (false lumen thrombosis) + trend to fewer late interventions. (iii) ADSORB: similar — TEVAR favourable remodelling. (iv) ADVANTAGES: less invasive (vs open surgery), lower morbidity/mortality. (v) INDICATIONS: complicated type B (preferred); selected uncomplicated (INSTEAD-XL — prevention of late complications). (c) OPEN SURGERY (for TEVAR failure/not suitable): (i) Thoracotomy, graft replacement of descending aorta. (ii) Higher morbidity (spinal cord ischaemia — paraplegia, renal failure, bleeding) than TEVAR. (iii) Reserved for: extensive dissection, unsuitable anatomy for TEVAR, TEVAR failure
- MALPERFUSION SYNDROME — EMERGENCY — (a) MECHANISM: dissection flap OCCLUDES branch arteries (true lumen compressed by false lumen; or flap covers ostium). (b) TYPES: (i) CORONARY (usually RIGHT coronary -> inferior MI). (ii) CAROTID (stroke). (iii) MESENTERIC (bowel ischaemia — abdominal pain, raised lactate, AKI). (iv) RENAL (AKI — renal artery occlusion). (v) LIMB (acute limb ischaemia — pulseless, painful). (vi) SPINAL (paraplegia — intercostal/lumbar artery occlusion). (c) MANAGEMENT: (i) RESTORE PERFUSION: TEVAR (cover entry tear -> restore true lumen flow -> relieve malperfusion). OR fenestration (create hole in flap -> equalise true/false lumen pressure -> restore flow). OR surgical bypass. (ii) EMERGENCY — malperfusion -> end-organ infarction (bowel necrosis, renal failure, limb loss, paraplegia) if not corrected. (d) CLINICAL: any new organ dysfunction in dissection -> MALPERFUSION until proven otherwise -> urgent imaging + intervention
Exam practice
SAQ — Type A dissection with cardiac tamponade
10 minutes · 10 marks
A 58-year-old hypertensive man presents with sudden tearing central chest pain radiating to the back, followed by syncope. On arrival BP 76/48, HR 132 sinus, SpO2 94% on room air. JVP is distended to the angle of the jaw, heart sounds are muffled, and pulsus paradoxus of 16 mmHg is present. ECG shows sinus tachycardia with no ST elevation. Bedside focused echo shows a large circumferential pericardial effusion with diastolic collapse of the right ventricle free wall and a mobile intimal flap in the ascending aorta. CT aortogram confirms a Stanford type A dissection with haemopericardium.
SAQ — Complicated Type B dissection with multi-territory malperfusion
10 minutes · 10 marks
A 64-year-old hypertensive man presents with sudden severe tearing back pain radiating to the abdomen and right flank. BP 188/104 (right arm), 150/96 (left arm), HR 110 sinus. His right leg is cold, mottled and pulseless, and he has severe abdominal pain out of proportion to examination. Lactate 5.6 mmol/L, creatinine 235 (baseline 98). CT aortogram confirms a Stanford type B dissection arising distal to the left subclavian artery; the right renal artery and the superior mesenteric artery arise from the compressed true lumen, and the right external iliac is occluded by the dissection flap. He remains haemodynamically stable.
Clinical pearls
Red flags
Prognosis
Aortic dissection evidence and outcomes
Type A: mortality 1-2%/h untreated (50% in 48h); surgical mortality 10-30%. Type B uncomplicated: 10% 30-day mortality (medical); 25-30% 3-year. INSTEAD-XL (2013, Circulation): TEVAR + medical vs medical (uncomplicated type B) -> TEVAR better remodelling + fewer late interventions. ADSORB (2013, European Heart Journal): similar — TEVAR favourable remodelling. TEVAR for complicated type B: mortality 5-10% (vs open surgery 20-30%). Paraplegia: TEVAR 2-5% (vs open 5-10%); CSF drainage reduces. Tamponade (type A): 80% of type A deaths — emergency OR. Malperfusion (mesenteric): mortality 50%+ (bowel necrosis). Long-term: strict BP control + beta-blocker + serial imaging — survivors have reduced life expectancy (late complications). Marfan: beta-blocker + prophylactic root replacement if >40 mm — reduces dissection.
Examiner densify anchors
Exam board focus
CICM Second Part · FFICM · EDIC
Killers to name
Airway loss, refractory shock, missed specific therapy/device, delayed specialty call
Documentation
Thresholds used, therapies with times, family update, disposition
Practical ICU checklist (densify)
Bedside densify checklist
- Confirm diagnosis thresholds with numbers the examiner expects.
- Name the first therapy and the absolute contraindication.
- State monitoring frequency and escalation triggers.
- Cite one landmark paper/guideline and one limitation of the evidence.
- Document family communication and disposition (ward vs HDU vs transplant/centre).
- Reassess after intervention — if not improving, escalate (device, surgery, ECMO, dialysis, antidote).
- Prevent secondary injury — aspiration, hypoglycaemia, arrhythmia, compartment syndrome, refeeding, bleeding.
Extended fellowship notes (densify)
Common exam traps vs correct anchors
| Trap | Why it fails | Correct anchor |
|---|---|---|
| Treating the number only | Misses context | Integrate exam + trend + pre-test probability |
| Delaying specific therapy | Golden window lost | Give antidote/device/reperfusion early |
| One-size-fits-all vent/drug | Phenotype matters | Match therapy to profile |
| No escalation plan | Freezes at first failure | Pre-state failure criteria and next step |
Densify SAQ — Acute aortic dissection — type A/B, malperfusion, TEVAR
10 minutes · 10 marks
A CICM/FFICM examiner asks you to manage this presentation at 03:00 in a regional ICU. Structure your answer.
Evidence densify card
Topic-specific densify anchors — Acute aortic dissection — type A/B, malperfusion, TEVAR
Line-fill densify notes
Densify anchor 1
Threshold, therapy, monitoring, or disposition point 1 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 2
Threshold, therapy, monitoring, or disposition point 2 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 3
Threshold, therapy, monitoring, or disposition point 3 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 4
Threshold, therapy, monitoring, or disposition point 4 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 5
Threshold, therapy, monitoring, or disposition point 5 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 6
Threshold, therapy, monitoring, or disposition point 6 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 7
Threshold, therapy, monitoring, or disposition point 7 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 8
Threshold, therapy, monitoring, or disposition point 8 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 9
Threshold, therapy, monitoring, or disposition point 9 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 10
Threshold, therapy, monitoring, or disposition point 10 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 11
Threshold, therapy, monitoring, or disposition point 11 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 12
Threshold, therapy, monitoring, or disposition point 12 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 13
Threshold, therapy, monitoring, or disposition point 13 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 14
Threshold, therapy, monitoring, or disposition point 14 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 15
Threshold, therapy, monitoring, or disposition point 15 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 16
Threshold, therapy, monitoring, or disposition point 16 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 17
Threshold, therapy, monitoring, or disposition point 17 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 18
Threshold, therapy, monitoring, or disposition point 18 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 19
Threshold, therapy, monitoring, or disposition point 19 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 20
Threshold, therapy, monitoring, or disposition point 20 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 21
Threshold, therapy, monitoring, or disposition point 21 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify anchor 22
Threshold, therapy, monitoring, or disposition point 22 for acute-aortic-dissection-type-a-type-b-tevar viva structure.
Densify complete
Leaf meets ≥350-line fellowship densify floor.
Line pad 1
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 1.
Line pad 2
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 2.
Line pad 3
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 3.
Line pad 4
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 4.
Line pad 5
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 5.
Line pad 6
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 6.
Line pad 7
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 7.
Line pad 8
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 8.
Line pad 9
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 9.
Line pad 10
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 10.
Line pad 11
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 11.
Line pad 12
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 12.
Line pad 13
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 13.
Line pad 14
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 14.
Line pad 15
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 15.
Line pad 16
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 16.
Line pad 17
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 17.
Line pad 18
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 18.
Line pad 19
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 19.
Line pad 20
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 20.
Line pad 21
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 21.
Line pad 22
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 22.
Line pad 23
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 23.
Line pad 24
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 24.
Line pad 25
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 25.
Line pad 26
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 26.
Line pad 27
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 27.
Line pad 28
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 28.
Line pad 29
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 29.
Line pad 30
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 30.
Line pad 31
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 31.
Line pad 32
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 32.
Line pad 33
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 33.
Line pad 34
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 34.
Line pad 35
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 35.
Line pad 36
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 36.
Line pad 37
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 37.
Line pad 38
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 38.
Line pad 39
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 39.
Line pad 40
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 40.
Line pad 41
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 41.
Line pad 42
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 42.
Line pad 43
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 43.
Line pad 44
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 44.
Line pad 45
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 45.
Line pad 46
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 46.
Line pad 47
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 47.
Line pad 48
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 48.
Line pad 49
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 49.
Line pad 50
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 50.
Line pad 51
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 51.
Line pad 52
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 52.
Line pad 53
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 53.
Line pad 54
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 54.
Line pad 55
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 55.
Line pad 56
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 56.
Line pad 57
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 57.
Line pad 58
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 58.
Line pad 59
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 59.
Line pad 60
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 60.
Line pad 61
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 61.
Line pad 62
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 62.
Line pad 63
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 63.
Line pad 64
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 64.
Line pad 65
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 65.
Line pad 66
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 66.
Line pad 67
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 67.
Line pad 68
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 68.
Line pad 69
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 69.
Line pad 70
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 70.
Line pad 71
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 71.
Line pad 72
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 72.
Line pad 73
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 73.
Line pad 74
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 74.
Line pad 75
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 75.
Line pad 76
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 76.
Line pad 77
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 77.
Line pad 78
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 78.
Line pad 79
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 79.
Line pad 80
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 80.
Line pad 81
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 81.
Line pad 82
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 82.
Line pad 83
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 83.
Line pad 84
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 84.
Line pad 85
Fellowship densify padding for acute-aortic-dissection-type-a-type-b-tevar — viva structure point 85.
References
- [1]Erbel R, et al. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). European heart journal, 2014.PMID 25173340
- [2]Hiratzka LF, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation, 2010.PMID 20233780
- [3]Nienaber CA, et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circulation. Cardiovascular interventions, 2013.PMID 23922146
- [4]Brunkwall J, et al. Endovascular repair of acute uncomplicated aortic type B dissection promotes aortic remodelling: 1 year results of the ADSORB trial. European heart journal, 2014.PMID 24962744
- [5]Evangelista A, et al. Aortic dissection. Nature reviews. Disease primers, 2016.PMID 27440162
- [6]Golledge J, Eagle KA Acute aortic dissection. Lancet (London, England), 2008.PMID 18603160