ICU · Cardiovascular
Acute aortic dissection and acute aortic syndrome
Also known as Stanford type A and type B dissection · Acute aortic syndrome · Aortic intramural haematoma (IMH) · Penetrating atherosclerotic ulcer (PAU) · TEVAR (thoracic endovascular aortic repair) · Malperfusion syndrome
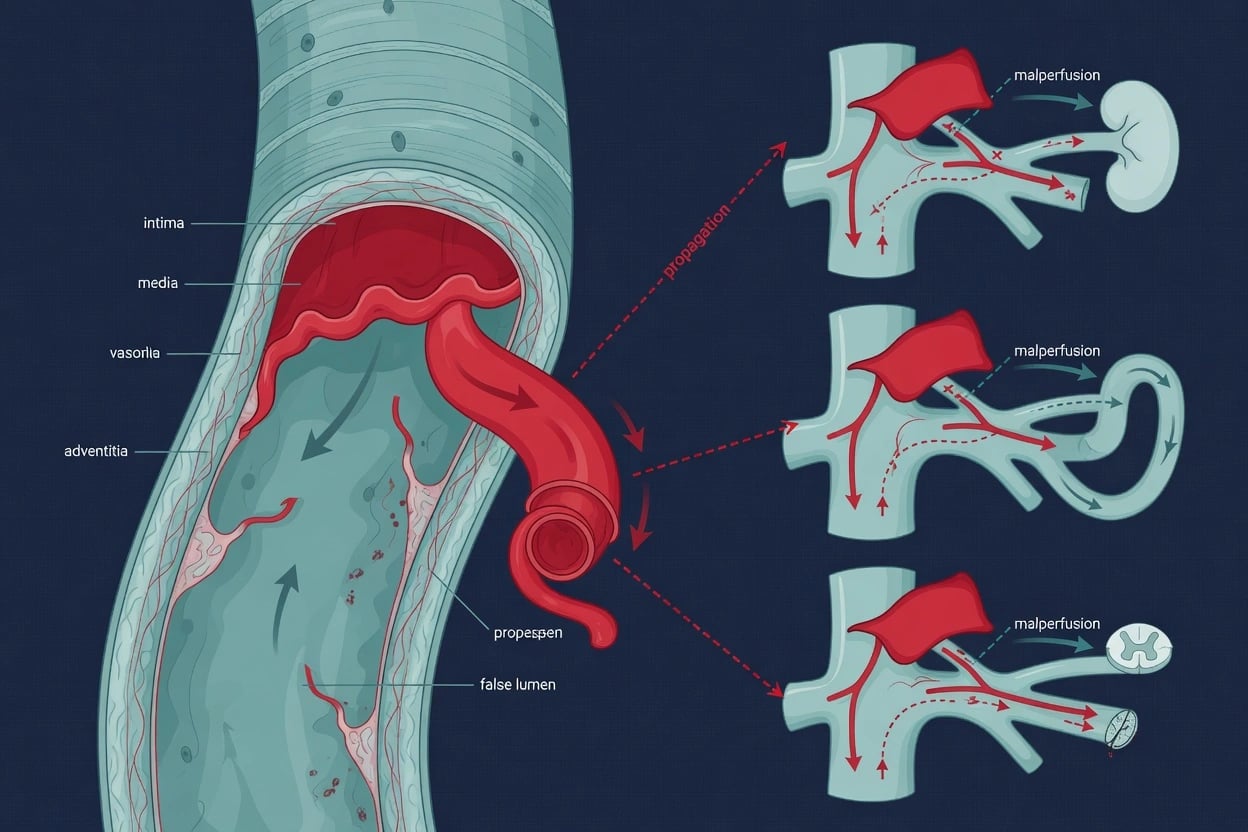
Acute aortic dissection is a tear in the aortic intima allowing blood to enter the media, creating a false lumen. Stanford classification: Type A involves the ascending aorta (surgical emergency — mortality 1-2%/h, surgical repair). Type B involves only the descending aorta (medical management — BP control, TEVAR for complicated). Presentation: tearing chest/back pain, pulse deficit, BP differential (20 mmHg between arms), widened mediastinum on CXR, new aortic regurgitation murmur, neurological deficit, syncope. Diagnosis: CT angiography (gold standard — intimal flap, true/false lumen), transoesophageal echo in the unstable patient, CXR widened mediastinum as a clue. Management: Type A = emergency surgery (BP control first — beta-blocker before vasodilator, target SBP 100-120 HR 60-80); Type B = medical (IV beta-blocker first — labetalol/esmolol — reduce dP/dt, target SBP 100-120), TEVAR if complicated (malperfusion, rupture, rapid expansion — ADSORB/INSTEAD trials). Acute aortic syndrome also includes intramural haematoma (IMH) and penetrating atherosclerotic ulcer (PAU). Complications: malperfusion (coronary/cerebral/mesenteric/renal/spinal), cardiac tamponade, rupture. DeBakey classification refines anatomy (I = ascending + beyond, II = ascending only, III = descending only).
On this page & tools
Your progress
Saved locally on this device.
5 MCQs with explanations
Target exams
Red flags

Classification
Stanford classification of aortic dissection (click each)
Descending aorta only
Dissection distal to the left subclavian artery (descending thoracic ± abdominal aorta). Does NOT involve ascending aorta. MEDICAL management first (BP control). TEVAR if complicated: malperfusion (renal, mesenteric, limb ischaemia), rupture, rapid expansion, refractory pain, or persistent hypertension.
DeBakey classification
DeBakey I
Ascending + beyond
- Intimal tear in the ascending aorta, dissection propagates distally through the aortic arch into the descending and abdominal aorta
- Involves the ENTIRE aorta. Maps to Stanford Type A.
- Most lethal variant — requires emergency open repair.
- Typical of young Marfan patients with annuloaortic ectasia.
DeBakey II
Ascending only
- Dissection confined to the ascending aorta (does NOT pass the innominate artery).
- Maps to Stanford Type A. Common in elderly hypertensive patients with a localised tear.
- Surgical management identical to DeBakey I: open graft replacement ± valve.
DeBakey IIIa
Descending thoracic only
- Tear distal to the left subclavian, dissection confined to the descending thoracic aorta (above the diaphragm).
- Maps to Stanford Type B. Medical management; TEVAR if complicated.
- Best long-term prognosis of the three.
DeBakey IIIb
Descending + abdominal
- Tear distal to the left subclavian, dissection extends below the diaphragm into the abdominal aorta and iliacs.
- Maps to Stanford Type B. Higher risk of visceral/renal malperfusion.
- Most likely variant to need fenestration or branch-vessel stenting.
Epidemiology and the IRAD dataset
[6] [7] [8]Aortic dissection by the numbers (IRAD, 17-year trends)
Acute aortic syndrome
Classic dissection
Intimal tear + false lumen
- Tear in intima allows blood to enter media, splitting it
- True lumen (smaller, flows normally) vs false lumen (larger, static/thrombosed)
- Most common form of acute aortic syndrome
- Risk factors: hypertension (#1), age, male, Marfan syndrome, bicuspid aortic valve, pregnancy, cocaine
Intramural haematoma (IMH)
Bleeding within media, no tear
- Vasa vasorum rupture within the aortic wall (no intimal tear, no false lumen flow)
- Can progress to frank dissection or rupture
- Management: same as classic dissection (Type A = surgery, Type B = medical)
- More likely to regress spontaneously than classic dissection
Penetrating atherosclerotic ulcer (PAU)
Ulcer through intima into media
- Atherosclerotic plaque ulcerates through intima into media
- Can form pseudoaneurysm or progress to dissection/rupture
- Usually in elderly patients with severe atherosclerosis
- Management: medical if asymptomatic; intervention if symptomatic, expanding, or ruptured
Diagnosis
Clinical presentation
[1]Imaging
CT angiography (CTA)
Gold standard — first-line
- Sensitivity and specificity >98%
- Shows intimal flap, true and false lumen, entry/exit tears
- Identifies branch vessel involvement (coronaries, carotids, renals, mesenteric)
- Identifies complications: tamponade, rupture, malperfusion
- Fast, widely available
Transoesophageal echo (TOE)
If haemodynamically unstable
- Bedside — useful if patient too unstable for CT
- Excellent for ascending aorta and aortic valve (assess AR)
- Can be done in theatre while preparing for surgery
- Cannot visualise the entire aorta (blind spots in distal descending)
D-dimer
Rule OUT (not rule in)
- D-dimer <500 ng/mL effectively rules out dissection (sensitivity ~97%)
- Useful in LOW-RISK patients to avoid unnecessary CTA
- D-dimer is elevated in MANY conditions (PE, sepsis, trauma, malignancy) — not specific
- ADAPT trial: D-dimer-based algorithm safely reduced CTA use by ~30%
Differential diagnosis [1]
Acute coronary syndrome
Builds up, pressure-like
- Pain crescendos over minutes and is pressure-like rather than tearing/ripping.
- ECG shows ischaemic changes (BUT inferior STEMI can be the *presentation* of a Type A dissection involving the RCA — always check for pulse/BP differential).
- Troponin rises; D-dimer is not a useful discriminator (raised in both).
- Pearl: give antiplatelets/heparin/fibrinolytics only after excluding dissection when pain is atypical or there is a BP differential.
Pulmonary embolism
Pleuritic, dyspnoea
- Sudden pleuritic pain, dyspnoea, hypoxia; D-dimer raised in both.
- No BP differential or pulse deficit; CTPA shows clot, not a flap.
- Right heart strain on echo (McConnell sign) supports PE.
Tension pneumothorax
Unilateral, tracheal deviation
- Sudden dyspnoea + chest pain, hypoxia, hypotension, unilateral hyper-resonance and absent breath sounds.
- CXR (or US) is diagnostic; no mediastinal flap on imaging.
Pericarditis / myocarditis
Positional, pleuritic
- Positional pain relieved by sitting forward; diffuse ST elevation; no mediastinal widening.
- Tamponade physiology can mimic dissection with tamponade — echo distinguishes.
Oesophageal rupture (Boerhaave)
Post-emesis
- Sudden chest pain after vomiting; left pleural effusion, subcutaneous emphysema.
- CT/contrast oesophagram confirms; oesophageal tear not aortic flap.
Musculoskeletal / aortic aneurysm leak
Non-dissecting
- Aortic aneurysm without dissection can cause severe back pain; CTA distinguishes.
- Always image the aorta when "torn muscle" pain is sudden and maximal at onset in a hypertensive patient.
Type A vs Type B at a glance
Type A
Ascending aorta — surgical emergency
- Mortality 1–2% per hour untreated — in-hospital mortality 22–30% even with surgery.
- Presentation: tearing chest pain radiating to the back/syncope/new AR murmur/pulse deficit; ~10% present in syncope.
- Complications: acute AR, coronary occlusion (RCA → inferior STEMI), tamponade, stroke.
- Management: emergency open repair (graft ± valve ± Bentall); pericardiocentesis only if pre-arrest.
Type B
Descending aorta — medical first
- 30-day mortality ~10% (uncomplicated) rising to ~30% when complicated.
- Presentation: tearing back/abdominal pain; mesenteric/renal/limb malperfusion signs.
- Management: IV beta-blocker FIRST then vasodilator; SBP 100–120, HR 60–80.
- TEVAR for complicated (malperfusion, rupture, rapid expansion, refractory pain/HTN); consider TEVAR in select uncomplicated high-risk (INSTEAD-XL, ADSORB).
Management

Type A — surgical emergency
Type A dissection management
Immediate surgical referral
Type A dissection is a SURGICAL EMERGENCY. Mortality 1-2% per hour untreated. Contact cardiothoracic surgery immediately. Do NOT delay for extensive workup — CTA to confirm, then to theatre.
Medical management WHILE awaiting surgery
Start IV beta-blocker: labetalol (20 mg IV bolus, then 20-80 mg every 10 min, or infusion 1-2 mg/min) or esmolol (loading 500 mcg/kg over 1 min, then 50-200 mcg/kg/min). Target: SBP 100-120, HR 60-80. Then add vasodilator if needed (IV nitroprusside or nicardipine). NEVER give vasodilator alone before beta-blocker — reflex tachycardia increases shear stress.
Surgical repair
Resection of the intimal tear + interposition graft (Dacron) of the ascending aorta ± aortic valve repair/replacement ± coronary reimplantation (Bentall procedure if root involved). Goal: obliterate the false lumen, restore true lumen flow.
Manage complications
Cardiac tamponade: pericardiocentesis ONLY if imminent arrest (risk of rebleeding — prefer rapid surgical approach). Coronary occlusion (usually RCA): revascularise at surgery. Acute aortic regurgitation: valve repair/replacement. Stroke: may be haemorrhagic (anticoagulation from bypass) — individualised approach.
Type B — medical first-line
Type B dissection management
Beta-blocker FIRST (reduce dP/dt)
IV labetalol: 20 mg bolus, then 20-80 mg every 10 min (max 300 mg), or infusion 1-2 mg/min titrated. OR esmolol: 500 mcg/kg loading over 1 min, then 50-200 mcg/kg/min infusion. Target: HR 60-80 bpm FIRST. Reducing heart rate reduces the rate of pressure rise (dP/dt) and shear stress on the aortic wall.
Add vasodilator (after beta-blockade)
If SBP still >120 after achieving HR 60-80, add IV vasodilator: sodium nitroprusside (0.3-3 mcg/kg/min) OR nicardipine (5-15 mg/h) OR nitroglycerin. Target SBP 100-120. NEVER give vasodilator before beta-blocker — reflex tachycardia increases shear stress and can extend the dissection.
Assess for complications
COMPLICATED Type B = any of: malperfusion syndrome (renal/mesenteric/limb ischaemia), rupture (haemothorax, mediastinal haematoma), rapid expansion (>10 mm), refractory pain/hypertension, spinal cord ischaemia. Complicated Type B = indication for TEVAR (thoracic endovascular aortic repair).
TEVAR for complicated Type B
Cover the primary entry tear with a stent graft. Restores true lumen flow, depressurises false lumen, promotes thrombosis of false lumen. Also used prophylactically in high-risk uncomplicated Type B (INSTEAD-XL trial: TEVAR + optimal medical therapy vs medical alone → improved 5-year survival and aorta-specific survival).
Malperfusion syndrome — fenestration
If branch vessels are occluded by the dissection flap (dynamic obstruction from true lumen collapse or static obstruction from flap covering the ostium): percutaneous fenestration (creating a window in the flap to equalise pressures between true and false lumens) ± branch vessel stenting. This restores blood flow to compromised organs.
Malperfusion syndrome
Coronary
Usually right coronary
- Dissection flap covers coronary ostium (usually right coronary — RCA)
- Presents as inferior STEMI in the context of dissection
- Management: surgical repair of the dissection will restore coronary flow
- Do NOT stent the coronary without fixing the dissection
Mesenteric
Bowel ischaemia
- Dissection flap covers superior mesenteric artery (SMA) ostium
- Presents as severe abdominal pain out of proportion to examination
- Lactate rising, metabolic acidosis
- Management: urgent fenestration/SMA stenting, exploratory laparotomy
Renal
AKI from renal artery occlusion
- Dissection flap covers renal artery ostium
- Presents as AKI, refractory hypertension (renin release from ischaemic kidney)
- Management: fenestration or renal artery stenting
Spinal cord
Paraplegia
- Dissection occludes intercostal/lumbar arteries feeding the artery of Adamkiewicz
- Presents as sudden paraplegia, loss of sensation below level
- Management: CSF drainage (to improve spinal cord perfusion pressure), augment MAP
Anaesthetic considerations for emergency Type A repair [1]
Induction and bypass for Type A — avoid propagation of the dissection
Pre-induction
Two large-bore IVs + arterial line (femoral or the arm with the HIGHER pressure — the lower-pressure arm may be reading a compromised subclavian). Pre-oxygenase. Maintain SBP 100–120 and HR 60–80 with IV beta-blocker ± vasodilator BEFORE induction; resuscitate volume if hypovolaemic.
Induction
Modified rapid-sequence with agents that blunt the sympathetic surge: fentanyl/sufentanil + propofol or etomidate; rocuronium or suxamethonium. AVOID ketamine (raises BP and dP/dt) and avoid coughing/bucking — these cause shear-stress spikes that extend the flap. Have an esmolol/nitroprusside infusion running to blunt the pressor response to laryngoscopy.
Vascular access & monitoring
Femoral arterial line preferred (radial may read a dissected subclavian). Central access for vasoactive infusions. TOE probe placed once anaesthetised to confirm entry tear, AR, tamponade, and coronary involvement.
Cardiopulmonary bypass
Arterial cannulation strategy depends on the tear — axillary/femoral artery. Deep hypothermic circulatory arrest (DHCA, 18–22°C) is used when the arch is involved, to allow open distal anastomosis and protect the brain. Selective antegrade cerebral perfusion (SACP) is now standard adjunct.
Coagulopathy
Expect massive transfusion. Cell salvage, rapid-infusion system, and a massive-haemorrhage protocol should be active. Correct hypofibrinogenaemia (cryoprecipitate/fibrinogen concentrate) and thrombocytopenia early — bypass + hypothermia + long clamp time = severe coagulopathy.
Post-bypass / ICU
Re-warm fully; reverse heparin with protamine. Watch for re-bleeding, tamponade, and spinal/visceral malperfusion. Maintain MAP >80 mmHg to protect the spinal cord (and CSF drain if long-segment repair). Glucose, temperature, and lactate surveillance for ongoing malperfusion.
TEVAR: technique, indications and complications
Indications (complicated Type B)
TEVAR is standard
- Rupture or impending rupture (haemothorax, mediastinal haematoma).
- Malperfusion syndrome (renal, mesenteric, limb, spinal) — TEVAR ± fenestration.
- Rapid expansion (>10 mm/yr) or aneurysmal degeneration of the false lumen.
- Refractory pain or refractory hypertension despite maximal medical therapy.
Selected uncomplicated Type B
Prophylactic TEVAR — evidence-based
- INSTEAD-XL (2013): TEVAR + OMT vs OMT alone → improved 5-year aorta-specific survival and delayed progression.
- ADSORB (2014): in acute (<14 days) uncomplicated Type B, TEVAR promoted false-lumen thrombosis and aortic remodelling at 1 year.
- Caveat: both trials are modest in size; guidelines reserve prophylactic TEVAR for high-risk anatomy (entry tear >10 mm, total aortic diameter >40 mm, false lumen diameter >22 mm).
- Not for everyone: best in young, fit patients with favourable landing zones.
Technical principles
Cover the entry tear
- Stent-graft covers the primary entry tear → restores true-lumen flow, depressurises false lumen, promotes false-lumen thrombosis.
- Requires a proximal landing zone of ≥20 mm healthy aorta distal to the left subclavian; may need left carotid–subclavian bypass.
- Distal extension may compromise segmental arteries → spinal cord ischaemia.
- Use intravascular ultrasound (IVUS) and aortography to confirm true-lumen wire position.
TEVAR complications
Know these for the exam
- Spinal cord ischaemia/paraplegia (1–5%) — mitigated by CSF drainage and permissive hypertension.
- Stroke (2–8%) from wire/catheter manipulation in the arch or coverage of the left subclavian.
- Endoleak (Type I most important) → persistent pressurisation of false lumen.
- Retrograde Type A dissection (rare but catastrophic) — the stent itself creates a new entry tear.
- Access-site injury (iliac/femoral rupture) — stiff large-bore sheaths in atherosclerotic vessels.
INSTEAD (Nienaber 2009) and INSTEAD-XL (2013)
Circulation 2009 / Circ Cardiovasc Interv 2013
Randomised, multicentre, chronic (>2 weeks) uncomplicated Type B dissection: TEVAR + optimal medical therapy vs medical therapy alone; long-term follow-up at 5 years (INSTEAD-XL)
Key finding
INSTEAD (1 yr): no difference in all-cause mortality (TEVAR not worse). INSTEAD-XL (5 yr): aorta-specific mortality 0% (TEVAR+OMT) vs 7% (OMT alone) and improved aortic remodelling (false-lumen thrombosis).
Practice change
TEVAR is safe and improves long-term aorta-specific outcomes in selected chronic uncomplicated Type B — but does not change all-cause mortality
ADSORB (Brunkwall 2014)
Eur J Vasc Endovasc Surg 2014
Randomised European multicentre trial, 61 patients with acute (<14 days) UNCOMPLICATED Type B dissection: TEVAR + OMT vs OMT alone; primary endpoint false-lumen thrombosis at 1 year
Key finding
TEVAR promoted false-lumen thrombosis (55.6% vs 0% complete thrombosis) and favourable aortic remodelling at 1 year. No mortality difference; paraplegia ~3% in the TEVAR arm.
Practice change
Acute uncomplicated Type B remodels better with TEVAR, but no survival advantage — medical therapy remains default; TEVAR reserved for high-risk features
IRAD (Hagan 2000; Pape 2015)
JAMA 2000 / JACC 2015
International Registry of Acute Aortic Dissection — >4500 enrolled patients across 30+ centres; 17-year trends paper (Pape 2015) tracked presentation, management and outcomes
Key finding
Over 17 years, Type A in-hospital mortality fell modestly; CT angiography became the dominant diagnostic modality (>90%); the use of cerebral protection and TEVAR increased; hospital mortality for complicated Type B remains ~30%.
Practice change
Established CTA as the default diagnostic test and quantified the natural history that underpins all modern guidelines
Long-term surveillance and follow-up
[1] [12]Genetic aortopathies and pregnancy
Marfan syndrome
FBN1 mutation
- Most common heritable cause of dissection; annuloaortic ectasia → root aneurysm → Type A.
- Elective root replacement when aortic root >50 mm (or >45 mm with risk factors).
- Pregnancy: risk rises sharply when root >40 mm — beta-blocker throughout, consider prophylactic root repair before conception.
Loeys-Dietz syndrome
TGFBR1/2 / SMAD3
- Aggressive, tortuous arterial disease; dissection at smaller aortic diameters (>42 mm threshold for repair).
- Widely disseminated arterial aneurysms — image from skull to pelvis.
- Pregnancy: high maternal risk — multidisciplinary aortopathy clinic essential.
Vascular Ehlers-Danlos (vEDS)
COL3A1 mutation
- Fragile arteries and viscera; dissection/rupture at small diameter; catastrophic bowel/uterine rupture.
- Avoid angiography/invasive procedures where possible; celiprolol is the disease-modifying drug.
- Pregnancy-associated rupture mortality is very high.
Bicuspid aortic valve (BAV)
Most common congenital cardiac lesion
- Associated with ascending aortic aneurysm and dissection independent of valve haemodynamics.
- Image the aorta in every BAV patient; repair when ascending diameter >55 mm (or >50 mm with risk factors, >45 mm at time of valve surgery).
- Familial — screen first-degree relatives.
Pregnancy-related dissection
Third trimester / peripartum
- Aortic dissection is responsible for a disproportionate share of maternal cardiac deaths; most occur in the third trimester or post-partum.
- Highest risk: Marfan with root >40 mm, prior dissection, bicuspid valve with dilated aorta, Turner syndrome.
- Manage BP aggressively; Type A → emergency caesarean + cardiac surgery; Type B → medical ± TEVAR.
Prognosis
Aortic dissection outcomes
Exam practice
SAQ — Type B aortic dissection with malperfusion
10 minutes · 10 marks
A 68-year-old hypertensive man presents with sudden severe tearing back pain radiating to the abdomen. BP 180/100 (right arm), 148/90 (left arm). CXR shows widened mediastinum. CT angiography confirms aortic dissection originating distal to the left subclavian artery, extending to the iliac bifurcation. The left renal artery arises from the false lumen. Creatinine 180 (baseline 90). Lactate 4.2. Severe abdominal pain.
Clinical pearls
Red flags
References
- [1]Isselbacher EM, Preventza O, Hamilton Black I, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines Circulation, 2022.PMID 36322642
- [2]Pape LA, Awais M, Woznicki EM, et al. Type A Aortic Dissection-Experience Over 5 Decades: JACC Historical Breakthroughs in Perspective J Am Coll Cardiol, 2020.PMID 33004136
- [3]Nautiyal A, Ather S, Swaminathan K, et al. Hemodynamic Safety of Continuous Infusion Labetalol Versus Esmolol Combination Therapies for Type B Aortic Dissections J Pharm Pract, 2021.PMID 32552306
- [4]Nienaber CA, Kische S, Rousseau H, et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial Circ Cardiovasc Interv, 2013.PMID 23922146
- [5]Mestres CA, et al. [Acute Aortic Dissection with Visceral Malperfusion Syndrome] Kyobu Geka, 2023.PMID 38056838
- [6]Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease JAMA, 2000.PMID 10685714
- [7]Pape LA, Awais M, Woznicki EM, et al. Presentation, Diagnosis, and Outcomes of Acute Aortic Dissection: 17-Year Trends From the International Registry of Acute Aortic Dissection J Am Coll Cardiol, 2015.PMID 26205591
- [8]Golledge J, Eagle KA. Acute aortic dissection Lancet, 2008.PMID 18603160
- [9]Nienaber CA, Kische S, Akin I, et al. Randomized comparison of strategies for type B aortic dissection: the INvestigation of STEnt Grafts in Aortic Dissection (INSTEAD) trial Circulation, 2009.PMID 19996018
- [10]Brunkwall J, Kasprzak P, Verhoeven E, et al. Endovascular repair of acute uncomplicated aortic type B dissection promotes aortic remodelling: 1 year results of the ADSORB trial Eur J Vasc Endovasc Surg, 2014.PMID 24962744
- [11]Brunkwall J, Lammer J, Verhoeven E, et al. ADSORB: a study on the efficacy of endovascular grafting in uncomplicated acute dissection of the descending aorta Eur J Vasc Endovasc Surg, 2012.PMID 22575291
- [12]Kasprzak PM, Gallis K, Cucuruz B, et al. Predictors of aortic growth in uncomplicated type B aortic dissection from the Acute Dissection Stent Grafting or Best Medical Treatment (ADSORB) database J Vasc Surg, 2017.PMID 27876516
- [13]Nienaber CA, Kische S, Ince H, et al. Strategies for subacute/chronic type B aortic dissection: the Investigation Of Stent Grafts in Patients with type B Aortic Dissection (INSTEAD) trial 1-year outcome J Thorac Cardiovasc Surg, 2010.PMID 21092774