ICU · Cardiovascular
Infective endocarditis in the ICU
Also known as Infective endocarditis (IE) · Bacterial endocarditis · Subacute bacterial endocarditis (SBE) · Duke criteria · Valvular vegetation · Embolic phenomena · Native valve endocarditis · Prosthetic valve endocarditis
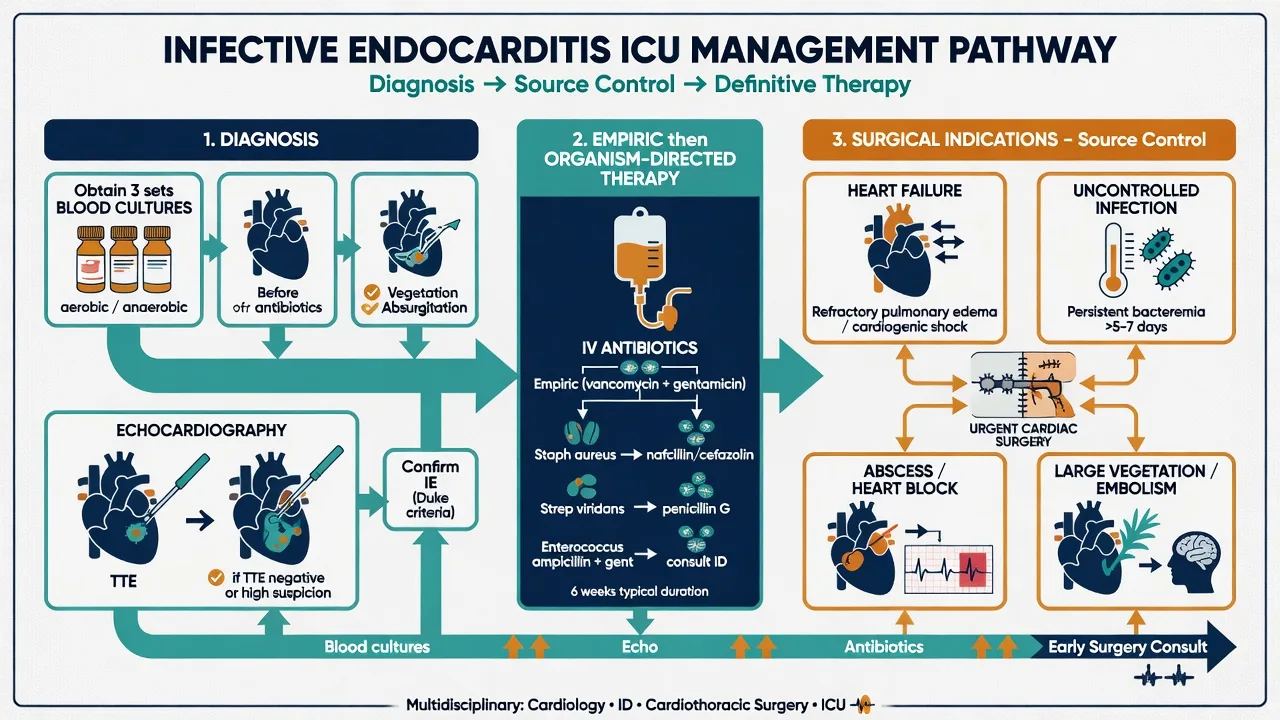
Infective endocarditis (IE) is microbial infection of the endocardial surface (usually heart valves). ICU admission for: septic shock, heart failure from valvular destruction, embolic stroke, conduction abnormalities. Diagnosis: modified Duke criteria (blood cultures + echocardiography). Organisms: S. aureus (1 overall — acute, aggressive), viridans streptococci (subacute — dental source, 1 in community-acquired native valve), Enterococcus (genitourinary source), HACEK, culture-negative (Coxiella, Bartonella, fungi — Candida), fungi (Candida — large vegetations, IVDU/prolonged lines). Treatment: prolonged IV antibiotics (4-6 weeks), organism-specific. Empiric: vancomycin + gentamicin + cefepime for severe/septic shock; definitive — penicillin/ceftriaxone for strep, nafcillin/oxacillin (flucloxacillin) for MSSA, vancomycin for MRSA. Surgery indications: heart failure from valvular destruction (1), uncontrolled infection, large mobile vegetation with embolism, perivalvular extension (abscess), prosthetic valve dehiscence.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Why does IE come to the ICU?
Infective endocarditis reaches critical care through four principal pathways, and recognising which dominates changes the whole management plan:[1]
- Septic shock — uncontrolled bacteraemia (often S. aureus) with vasopressor requirement and multi-organ dysfunction.
- Acute heart failure — sudden severe valvular regurgitation from leaflet destruction or chordal rupture → pulmonary oedema / cardiogenic shock (the leading indication for surgical referral).[6]
- Embolic stroke — vegetation fragments embolise to the brain (20-40% of left-sided IE); may present as ischaemic or haemorrhagic stroke.
- Conduction disease / arrhythmia — perivalvular aortic root abscess extending into the septum → new AV block, fascicular block, or ventricular arrhythmia.[2]
Mortality overall is 15-25% and has barely improved in two decades despite better antibiotics and surgery; the patients who die usually die of heart failure, neurologic complications, or uncontrolled sepsis rather than antimicrobial failure.[5]
Modified Duke criteria
[1] [2]Interpreting the Duke criteria — exam traps
The modified Duke criteria (Li 2000, the universally adopted update of the original 1994 Duke schema) classify a case as definite, possible, or rejected. Three categories are easy to confuse on viva:[4]
- Definite IE = (a) pathological criteria (organisms/lesions in vegetation or abscess at surgery or autopsy), OR (b) 2 major clinical criteria, OR (c) 1 major + 3 minor, OR (d) 5 minor.
- Possible IE = 1 major + 1 minor, OR 3 minor. "Possible" is NOT a licence to ignore — it still mandates treatment and repeat imaging.
- Rejected = firm alternative diagnosis, OR resolution of the syndrome with ≤4 days of antibiotics, OR no pathologic evidence of IE at surgery/autopsy. [1]
A single positive blood culture for coagulase-negative staphylococci does not count as a major criterion — the typical organisms must come from two separate cultures (or a single positive for Coxiella burnetii with anti-phase I IgG titre >1:800, which is itself a major criterion).[1]
Common organisms
Native valve
Community-acquired
- Staphylococcus aureus (#1 overall — acute, aggressive)
- Viridans streptococci (subacute — dental source)
- Enterococcus (genitourinary source)
- Coagulase-negative staph (less common in native valves)
- Culture-negative: Coxiella burnetii, Bartonella, HACEK group
Prosthetic valve / IV drug user
Special populations
- Prosthetic valve: coagulase-negative staph (early <2mo), S. aureus, Enterococcus, fungi
- IV drug user: S. aureus (right-sided — tricuspid valve), Pseudomonas, Candida
- Healthcare-associated: S. aureus (including MRSA), Enterococcus, coagulase-negative staph
Organism deep-dive — epidemiology, source, behaviour, mortality
The organism shapes everything that follows: the empiric regimen, the surgical threshold, and the prognosis. The ICE-PCS (over 2,700 cases) established the modern epidemiology.[5]
Viridans streptococci
#1 community native-valve organism
- ~30% of all IE; S. sanguis, S. mitis, S. mutans, S. salivarius
- Source: oral flora — poor dentition, dental procedures, bacteraemia from chewing
- Subacute (weeks-months); usually on previously damaged native valves
- Highly penicillin-sensitive (most); excellent prognosis (5-10% mortality)
- Treatment: penicillin G or ceftriaxone x 4 weeks (2 weeks if + gentamicin and pen MIC <0.12)
Staphylococcus aureus
#1 overall — acute, aggressive
- ~30% of all IE; highest mortality (25-40%)
- Can infect NORMAL valves (unlike viridans strep); acute presentation (days)
- Sources: skin — IV cannulae, IVDU, skin/soft tissue infection; healthcare-associated
- Highest embolic rate; metastatic infection (vertebral osteomyelitis, epidural abscess, septic arthritis)
- MRSA: vancomycin 6 weeks (target trough 15-20); MSSA: flucloxacillin/nafcillin 4-6 weeks
Enterococcus
GI/GU source
- ~10% of IE; E. faecalis (most), E. faecium
- Source: genitourinary and GI tract — urinary catheters, instrumentation, bowel surgery
- Often elderly, nosocomial; may be vancomycin-resistant (VRE)
- Treatment: ampicillin + gentamicin (or ceftriaxone) x 4-6 weeks; VRE → daptomycin/linezolid
Streptococcus gallolyticus (bovis)
GI — colonoscopy mandatory
- 5-10% of IE; strongly associated with colonic pathology (polyps, carcinoma)
- Any S. gallolyticus IE → colonoscopy MANDATORY after recovery to find/exclude colon cancer
- Treatment as for penicillin-sensitive streptococci (4 weeks)
HACEK group
Oropharyngeal, slow-growing
- Haemophilus, Aggregatibacter, Cardiobacterium, Eikenella, Kingella — 2-5% of IE
- Oropharyngeal flora; slow-growing — may need prolonged incubation (historically culture-negative)
- Tend to form large vegetations with high embolic rate
- Treatment: ceftriaxone 2g/day x 4 weeks; modern labs now culture them readily
Fungi
Candida — large vegetations, IVDU
- <2% but devastating; Candida (most common fungal IE), then Aspergillus
- Risk: IVDU, prolonged antibiotics, indwelling central lines, immunocompromise
- Large friable vegetations, very high embolic rate, poor prognosis (30-50% mortality)
- SURGICAL valve replacement mandatory + prolonged antifungal (liposomal amphotericin B ± flucytosine, then long-term fluconazole suppression)
Culture-negative IE
Prior antibiotics / fastidious organisms
- 5-10% of IE; causes: prior antibiotics (most common), Coxiella burnetii, Bartonella, Brucella, Tropheryma whipplei, fungi
- Send serology (Coxiella phase I/II IgG, Bartonella) and PCR; hold/special media
- Coxiella: single positive blood culture + anti-phase I IgG >1:800 = MAJOR Duke criterion
- Treatment: empiric broad cover; tailor once organism/serology returns
Coagulase-negative staph
Prosthetic valve (early)
- ~5% overall but dominant in EARLY prosthetic valve IE (<2 months post-implant)
- S. epidermidis — perioperative contamination → biofilm on prosthetic material
- Almost always requires surgery + rifampicin (penetrates biofilm) + vancomycin x >=6 weeks
Diagnosis — cultures and echocardiography
Blood cultures — the non-negotiable first step
Blood culture protocol before antibiotics
THREE sets from DIFFERENT venepuncture sites
Draw 3 sets (aerobic + anaerobic bottles each) from 3 separate sites, spaced ~30 minutes apart. Volume is the key determinant of yield — 20 mL per set (10 mL per bottle) in adults. Paediatric bottles for small children.
BEFORE antibiotics — if at all possible
Prior antibiotics are the leading cause of culture-negative IE. If already given, stop them (if safe) and repeat cultures over several days; consider specialised media and resin-containing bottles to neutralise antibiotics.
Septic patient — do NOT delay >1 hour
In septic shock, draw cultures then start empiric antibiotics within the first hour. Yield remains ~95% if cultures drawn within 24h of antibiotic start; falls sharply thereafter.
Persistent bacteraemia is itself diagnostic
A typical organism in cultures drawn >12 hours apart, OR a majority of >3 cultures positive, satisfies the major microbiological criterion — it is NOT just "line infection" until echo excludes IE.
Echocardiography — TTE vs TOE
TTE (transthoracic)
First-line screening
- Sensitivity ~50-60% native valve, ~20-40% prosthetic valve
- Detects vegetations >6 mm; misses small vegetations, abscess, prosthetic vegetations
- Bedside, non-invasive — useful for screening and for haemodynamic assessment of regurgitation
- A positive TTE still mandates TOE (to define complications)
TOE (transoesophageal)
Definitive — do for ALL suspected IE
- Sensitivity 90-100% native valve, 85-95% prosthetic valve
- Detects vegetations >3 mm; visualises abscess, fistula, leaflet perforation, dehiscence
- ALWAYS do TOE if IE suspected — even if TTE positive (to assess complications and extent)
- Repeat TOE after 5-7 days if clinical deterioration, new murmur, or persistent fever
Antibiotic treatment
IE antibiotic therapy
Empiric therapy (while awaiting cultures)
Vancomycin (covers MRSA) + gentamicin ± cefepime (if Gram-negative risk). Start after 3 sets of blood cultures from different sites. Do NOT delay antibiotics if patient is septic.
S. aureus (native valve)
Flucloxacillin 2g IV Q4H x 4-6 weeks (if MSSA). If MRSA: vancomycin (trough 15-20). Add gentamicin for first 3-5 days (synergy) — controversial, some guidelines no longer recommend routine gentamicin for S. aureus (nephrotoxicity without clear benefit). Monitor drug levels, renal function.
Viridans streptococci
Penicillin G or ceftriaxone x 4 weeks (2 weeks if + gentamicin and Pen MIC <0.12). Most streptococci are highly susceptible. Duration depends on MIC.
Enterococcus
Ampicillin + gentamicin (or ceftriaxone) x 4-6 weeks. Check susceptibility — VRE may need linezolid or daptomycin. Monitor for nephrotoxicity from gentamicin.
Duration: 4-6 weeks generally
S. aureus native valve: 4-6 weeks. Prosthetic valve: >=6 weeks. Viridans streptococci: 2-4 weeks (depending on regimen). Enterococcus: 4-6 weeks. Culture-negative: 4-6 weeks. Fungal: surgical valve replacement + prolonged antifungal.
Empiric therapy by clinical scenario
The empiric regimen is dictated by the likely organism, which in turn follows the clinical context:[1][2]
Native valve, community-acquired
Low MRSA risk
- Likely: viridans strep, S. aureus (MSSA), enterococcus, HACEK
- Ampicillin-sulbactam + gentamicin OR ceftriaxone + gentamicin (penicillin-allergic)
- Add vancomycin if MRSA suspected or severe/bacteraemic
Severe sepsis / septic shock
Broadest empiric cover
- Vancomycin + gentamicin + cefepime (or piperacillin-tazobactam)
- Covers MRSA, strep, enterococcus, HACEK, Gram-negatives including Pseudomonas
- De-escalate immediately on organism identification — prolonged broad therapy drives resistance and nephrotoxicity
Prosthetic valve (<12 months)
Biofilm / CoNS
- Vancomycin + gentamicin + rifampicin (900 mg/day)
- Rifampicin penetrates the biofilm on prosthetic material — essential; start AFTER 3-5 days of vancomycin/gentamicin (reduces bacterial load first to prevent rapid rifampicin resistance)
IV drug user
Right-sided, MRSA common
- Vancomycin + gentamicin (covers MRSA — most common in IVDU)
- Switch to flucloxacillin/nafcillin if MSSA confirmed (superior to vancomycin for MSSA)
- Add addiction-treatment referral — without it, recurrence is ~40% at 1 year
Definitive therapy by organism — the directed regimens
Once the organism and susceptibilities return, therapy is narrowed. Vancomycin is inferior to beta-lactams for MSSA endocarditis (slower clearance, higher failure/mortality) — always de-escalate MSSA to flucloxacillin/nafcillin.[8]
Viridans strep / S. gallolyticus (Pen MIC <0.12)
Highly susceptible
- Penicillin G 12-18 MU/day IV x 4 weeks, OR ceftriaxone 2g/day x 4 weeks
- Short course: 2 weeks if penicillin + gentamicin synergy (Pen MIC <0.12)
- Relatively resistant (MIC >0.12-0.5): penicillin x 4 weeks + gentamicin first 2 weeks
MSSA (native valve)
Beta-lactam superior
- Flucloxacillin/nafcillin/oxacillin 12g/day (2g Q4H) x 4-6 weeks
- Gentamicin synergy (first 3-5 days) controversial — no clear benefit, adds nephrotoxicity
- Vancomycin is a POOR substitute if beta-lactam tolerated — higher failure rate
MRSA
Vancomycin / daptomycin
- Vancomycin x 6 weeks (trough 15-20 mcg/mL; AUC/MIC monitoring preferred)
- Daptomycin 6-10 mg/kg/day if vancomycin MIC >1.5 or vancomycin failure/intolerance
- Rifampicin + gentamicin NOT routinely for native-valve MRSA (no benefit, toxicity)
Enterococcus (ampicillin-susceptible)
Synergy required
- Ampicillin + gentamicin (or ceftriaxone) x 4-6 weeks
- Ampicillin + ceftriaxone is an alternative synergy regimen (less nephrotoxic than gentamicin)
- VRE: daptomycin or linezolid (linezolid — watch myelosuppression, neuropathy)
HACEK
Beta-lactam
- Ceftriaxone 2g/day IV x 4 weeks (now routinely culturable)
Fungal (Candida)
Surgery + antifungal
- Surgical valve replacement MANDATORY + liposomal amphotericin B ± flucytosine, then lifelong/suppressive fluconazole
- Medical cure alone essentially never occurs
Surgery indications
[1]Surgical timing — evidence and urgency
About 40-50% of patients with IE undergo surgery during the index admission. The decision and its timing are the single highest-yield viva topic in endocarditis.[6]
Heart failure from acute AR/MR
EMERGENCY (<24-48h)
- The #1 surgical indication; ~60-70% of surgical IE
- Medical management alone: 50-70% mortality; early surgery reduces to 10-15%
- Do NOT wait for the antibiotic course — heart failure kills first
- ESC Class I, Level B
Uncontrolled infection
URGENT (days)
- Persistent bacteraemia/fever >5-7 days despite appropriate antibiotics = source uncontrolled
- Fungi, multiresistant organisms, S. aureus prosthetic valve — surgery almost always
Perivalvular extension (abscess)
URGENT — surgical emergency
- Aortic annular abscess → septal extension → AV block; progresses to fistula/perforation
- New heart block in aortic valve IE = abscess until proven otherwise
- Temporary pacing + urgent surgical debridement + valve replacement
Large mobile vegetation with emboli
URGENT
- >10 mm mobile vegetation AND prior embolic event — early surgery to prevent stroke
- >15 mm vegetation even without embolism (ESC Class IIb) — consider surgery
- Embolic risk is highest in the first 2 weeks; each day with a large vegetation = stroke risk
Prosthetic valve IE (early, <2 months)
Almost always surgical
- CoNS biofilm cannot be eradicated by antibiotics alone — rifampicin helps but surgery definitive
- Dehiscence, abscess, or S. aureus → surgery
Prosthetic valve dehiscence
URGENT
- New partial dehiscence on echo = active perivalvular infection — major Duke criterion
- Often with perivalvular leak and haemodynamic compromise → early surgery
Special situations
Prosthetic valve endocarditis — early vs late
Prosthetic valve endocarditis (PVE) carries roughly double the mortality of native-valve IE. Early PVE (commonly defined as <12 months, with <2 months the highest-risk window) reflects perioperative contamination; late PVE resembles community native-valve IE.[10]
Early PVE (<12 months)
Biofilm, CoNS
- Most common organism: coagulase-negative staph (S. epidermidis) from perioperative contamination
- Biofilm on prosthetic material — antibiotics cannot penetrate; only rifampicin does
- Abscess rate 40-60%; almost always requires surgery
- Mortality 20-40%
Late PVE (>12 months)
Resembles native-valve IE
- Same organisms as native-valve IE — viridans strep, S. aureus, enterococcus
- Transient bacteraemia (dental, GI/GU) seeding the sewing ring or valve thrombus
- Surgery case-by-case (apply native-valve criteria); mortality 15-25%
Right-sided endocarditis (IVDU) — the distinct entity
Right-sided (tricuspid) IE in people who inject drugs is a separate disease: a younger population, S. aureus in 60-70%, and a fundamentally different clinical picture because emboli go to the lung, not the brain.[7]
Right-sided (tricuspid) IE
IVDU population
- Population: IV drug users; also pacemaker/ICD leads, long-term central lines
- Organism: S. aureus 60-70% (skin/injection site)
- Presentation: SEPTIC PULMONARY EMBOLI — fever, pleuritic chest pain, cavitating lung lesions, haemoptysis (emboli to LUNGS, not brain/spleen)
- Surgery rarely needed; better prognosis (5-10% mortality) unless septic shock
- Antibiotics: 4-6 weeks (flucloxacillin MSSA; vancomycin MRSA); 2-week regimens possible in selected uncomplicated IVDU cases
- Addiction treatment ESSENTIAL — recurrence ~40% at 1 year without it
Left-sided (aortic/mitral) IE
Older, damaged valves
- Population: age >60, damaged valves (rheumatic, degenerative, prosthetic)
- Organisms: viridans strep 30%, S. aureus 30%, enterococcus 10%
- Presentation: SYSTEMIC emboli — stroke, splenic/renal/mesenteric infarct, femoral embolus
- Surgery commonly needed (40-50%); mortality 15-25%
Culture-negative endocarditis
Culture-negative IE (5-10%) is most often due to antibiotics given before cultures — not an exotic organism. When fastidious organisms are responsible, serology and PCR make the diagnosis.[4]
Prior antibiotics
Most common cause
- Account for the majority of culture-negative cases
- Stop antibiotics if safe, repeat cultures over days; use resin/antibiotic-neutralising bottles
Coxiella burnetii (Q fever)
Serology = major criterion
- Single positive blood culture + anti-phase I IgG >1:800 = MAJOR Duke criterion
- Often on prosthetic valves; chronic Q fever IE — treat with doxycycline + hydroxychloroquine >=18 months
Bartonella
Homeless, alcoholism, lice
- B. henselae (cats), B. quintana (body lice); large vegetations
- Diagnose by serology/PCR; treat with doxycycline + gentamicin (or ceftriaxone)
Other fastidious
Brucella, Tropheryma, fungi
- Brucella (unpasteurised dairy), Tropheryma whipplei, Aspergillus
- Send serology + PCR + special media; involve microbiology early
Complications of endocarditis
Embolic risk — prediction and prevention
Symptomatic embolism occurs in 20-40% of left-sided IE and is highest in the first 2 weeks. The Hubert risk calculator (French cohort) stratifies embolic risk and helps triage early surgery.[9]
High embolic-risk predictors
Favours early surgery
- Vegetation size >10 mm AND prior embolic event — early surgery (Class IIa)
- Vegetation >15 mm regardless of embolism (Class IIb)
- Staphylococcus aureus organism — higher embolic rate
- Mitral valve location (vs aortic) — higher embolic rate
- Increasing vegetation size on serial imaging, mobile vegetation
Embolic destinations
Left vs right sided
- Left-sided: brain (stroke — 20-40%), spleen, kidney, mesentery, coronaries, limb
- Right-sided/tricuspid: lungs (septic pulmonary emboli, cavitation, empyema)
- Mycotic aneurysm — intracranial (may rupture → haemorrhagic stroke), mesenteric, aortic
Neurologic complications
Neurologic events are the most feared complication and the principal reason surgery gets delayed.[1]
Ischaemic stroke (embolic)
Most common
- Vegetation fragment → cerebral artery occlusion
- Do NOT thrombolyse — high risk of haemorrhagic transformation of the septic infarct
- Surgery can proceed if no coma and no large haemorrhage; ideally delay ~2 weeks if heart failure allows
Haemorrhagic stroke
Delay surgery 3-4 weeks
- Usually haemorrhagic transformation of a septic embolic infarct, OR ruptured mycotic aneurysm
- Delay elective surgery 3-4 weeks if haemodynamically possible; stop/reverse anticoagulation
- EXCEPTION: if heart failure mandates immediate surgery, operate despite the bleed
Mycotic aneurysm
Intracranial — neurosurgery
- Infectious arteritis of the vessel wall; intracranial (most dangerous), mesenteric, aortic
- Rupture risk high; CT/MR angiography if headache/focal deficit; neurosurgical/endovascular input
Cardiac complications
Heart failure
#1 cause of death
- Acute valvular regurgitation (aortic, mitral) from leaflet destruction/chordal rupture
- Strongest predictor of mortality; mandates early surgery
Perivalvular extension
Abscess/fistula
- Aortic root abscess → septum → AV block (new conduction abnormality = abscess)
- Echo: thickening around the annulus, echo-free space, prosthetic dehiscence; surgical emergency
Conduction disease
New AV block
- New first-degree / higher AV block in aortic valve IE = abscess extending into septum
- Continuous ECG monitoring; temporary pacing; urgent surgery
Pericarditis / tamponade
Rare but critical
- Septic pericarditis from annular abscess rupture into pericardium, or mycotic aneurysm leak
- Tamponade physiology — emergency drainage + surgery
Prognosis
By organism
Best → worst
- Viridans strep (native): 5-10% (best)
- IVDU tricuspid S. aureus: 5-10%
- Enterococcus: 15-25%
- S. aureus native valve: 25-40% (most aggressive)
- Early prosthetic valve (CoNS): 20-40%
- Fungal IE: 30-50% (worst)
By complication
Modifiers of mortality
- Heart failure (no surgery): 50-70% → early surgery reduces to 10-15%
- Embolic stroke: adds 5-10% to baseline mortality
- Perivalvular abscess, prosthetic valve, elderly, healthcare-associated acquisition: worse
- Overall: 15-25% — unchanged in 20 years despite better antibiotics and surgery
Exam practice
SAQ — Native valve endocarditis with embolic stroke
10 minutes · 10 marks
A 58-year-old man with a bicuspid aortic valve presents to the ED with 10 days of fever, night sweats and a new diastolic murmur. Three sets of blood cultures grow Streptococcus sanguis (viridans streptococci). Transthoracic echo shows a 14 mm mobile aortic valve vegetation. Twelve hours after admission he develops acute right-sided weakness and aphasia; CT brain confirms an acute left MCA territory ischaemic infarct with no haemorrhage. BP 165/90, HR 96 sinus, SpO2 98%. GCS E4V3M6.
SAQ — Prosthetic valve endocarditis with acute heart failure
10 minutes · 10 marks
A 67-year-old woman is admitted 5 weeks after a bioprosthetic aortic valve replacement with 2 weeks of fever, dyspnoea and constitutional symptoms. Examination: JVP to the earlobes, bilateral crackles to mid-zones, a loud pansystolic murmur at the left sternal edge, and a new early diastolic murmur. Three blood cultures grow Staphylococcus epidermidis (coagulase-negative staph). CT chest shows pulmonary oedema. TOE demonstrates a peri-valvular abscess, partial prosthetic dehiscence with severe regurgitation, and PR interval prolongation to 320 ms on telemetry.
Clinical pearls
Key trials and evidence
ESC 2015 Guidelines — the global management standard (PMID 26320109)
Source
European Society of Cardiology — clinical practice guidelines (Habib et al.)
Diagnosis
Modified Duke criteria — 2 major, or 1 major + 3 minor, or 5 minor for definite IE
Imaging
TOE preferred over TTE — higher sensitivity for vegetations, abscess, prosthetic assessment
Surgery
Indicated for heart failure (early), uncontrolled infection, large mobile vegetations (>10mm with emboli, >15mm regardless), perivalvular extension, prosthetic valve IE
Antibiotics
4-6 weeks IV, organism-specific; gentamicin synergy for enterococci/streptococci; rifampicin for staphylococcal prosthetic valve IE
Bottom line
The definitive IE management guideline — modified Duke criteria + TOE + organism-specific antibiotics + early surgery for heart failure
AHA 2015 Scientific Statement — the US companion (PMID 26373316)
Source
American Heart Association — Baddour et al., Circulation
Key principle 1
TOE for ALL suspected IE (even if TTE positive) — to assess complications
Key principle 2
S. aureus bacteraemia → echocardiography mandatory (TOE preferred)
Key principle 3
Surgery in 40-50% of IE; heart failure is the #1 indication
Key principle 4
Prophylaxis limited to highest-risk patients (prosthetic valves, prior IE, complex congenital, transplant valvulopathy)
Bottom line
Comprehensive US guidance — emphasises TOE, S. aureus, early surgery, and restricted prophylaxis
ICE-PCS — modern IE epidemiology (PMID 19273776)
Source
International Collaboration on Endocarditis — Prospective Cohort Study (Murdoch et al., Arch Intern Med 2009)
Design
Prospective multinational cohort — >2,700 definite IE cases from 25 centres
Top organisms
Staph aureus (~31%, now #1), viridans streptococci (~17%), enterococci (~11%), CoNS (~11%), HACEK (~2%)
Key findings
S. aureus overtook viridans strep as the leading organism; ~half of cases had health-care-associated acquisition; native-valve IE still most common
Bottom line
Established the contemporary epidemiology: S. aureus dominance, healthcare-associated burden, and the persistent 15-25% mortality
Chirouze — early surgery in S. aureus prosthetic valve IE (PMID 25389255)
Source
ICE-PCS analysis — Chirouze et al., Clinical Infectious Diseases 2015
Question
Does early valve surgery improve survival in S. aureus prosthetic valve endocarditis?
Population
S. aureus prosthetic valve IE — historically near-uniform mortality with medical therapy alone
Finding
Early surgery was associated with markedly reduced 1-year mortality vs conventional medical management
Bottom line
S. aureus prosthetic valve IE should prompt early surgical referral — medical therapy alone usually fails (biofilm + aggressive organism)
Kang — timing of surgery in IE (PMID 26285598)
Source
Kang DH et al., Heart 2015 (and the preceding NEJM RCT of early surgery for NVE with large vegetations)
Question
Does early surgery reduce embolism in IE with large (>10mm) vegetations?
Design
Randomised and observational analyses of early vs delayed surgery
Finding
Early surgery reduced the composite of embolic events and death, particularly when vegetations were >10mm and mobile
Bottom line
Early surgery for large mobile vegetations (especially with prior emboli) prevents stroke — the basis of the ESC >10mm/>15mm thresholds
Hubert — embolic risk calculator (PMID 23906859)
Source
Hubert S et al., JACC 2013 — French multicentre cohort
Aim
Construct and validate a risk calculator for symptomatic embolism in IE
Predictors
Vegetation size, mobility, Staphylococcus aureus, mitral location, prior embolism
Use
Stratifies patients in whom early surgery to prevent embolism is justified vs those in whom it is not
Bottom line
Provides the evidence base for individualised surgical decision-making on embolic grounds
Pericàs — vancomycin MIC and MSSA IE outcomes (PMID 28159672)
Source
Pericàs JM et al., Clinical Microbiology and Infection 2017 — ICE-PCS analysis
Question
Does vancomycin MIC affect outcome when vancomycin is used for MSSA endocarditis?
Finding
Higher vancomycin MIC and vancomycin use (vs beta-lactam) were associated with worse outcomes in MSSA IE
Bottom line
Reinforces that beta-lactams (flucloxacillin/nafcillin) are superior to vancomycin for MSSA — reserve vancomycin for MRSA and beta-lactam allergy
Red flags
References
- [1]Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM) Eur Heart J, 2015.PMID 26320109
- [2]Baddour LM, Wilson WR, Bayer AS, et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association Circulation, 2015.PMID 26373316
- [3]Chirouze C, Alla F, Fowler VG Jr, et al. Impact of early valve surgery on outcome of Staphylococcus aureus prosthetic valve infective endocarditis: analysis in the International Collaboration of Endocarditis-Prospective Cohort Study Clin Infect Dis, 2015.PMID 25389255
- [4]Li JS, Sexton DJ, Mick N, et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis Clin Infect Dis, 2000.PMID 10770721
- [5]Murdoch DR, Corey GR, Hoen B, et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study Arch Intern Med, 2009.PMID 19273776
- [6]Kang DH, Kim YJ, Kim SH, et al. Timing of surgery in infective endocarditis Heart, 2015.PMID 26285598
- [7]Pericàs JM, Llopis J, Cervera C, et al. Prospective Cohort Study of Infective Endocarditis in People Who Inject Drugs J Am Coll Cardiol, 2021.PMID 33538252
- [8]Pericàs JM, Messina JA, Garcés C, et al. Influence of vancomycin minimum inhibitory concentration on the outcome of methicillin-susceptible Staphylococcus aureus left-sided infective endocarditis treated with antistaphylococcal β-lactam antibiotics: a prospective cohort study by the International Collaboration on Endocarditis Clin Microbiol Infect, 2017.PMID 28159672
- [9]Hubert S, Thuny F, Resseguier N, et al. Prediction of symptomatic embolism in infective endocarditis: construction and validation of a risk calculator in a multicenter cohort J Am Coll Cardiol, 2013.PMID 23906859
- [10]Lalani T, Kanafani ZA, Chu VH, et al. Prosthetic valve endocarditis due to coagulase-negative staphylococci: findings from the International Collaboration on Endocarditis Merged Database Eur J Clin Microbiol Infect Dis, 2006.PMID 16767483