ICU · cardiovascular
Acute severe valvular emergencies — critical aortic stenosis, acute mitral regurgitation, acute aortic regurgitation (comprehensive ICU management)
Also known as Critical aortic stenosis · Acute mitral regurgitation · Acute aortic regurgitation · Papillary muscle rupture · Acute MR · Acute AR · Valvular cardiogenic shock · Balloon aortic valvuloplasty · BAV · TAVI · TAVR · Transcatheter aortic valve implantation · Surgical aortic valve replacement · SAVR · PARTNER 3 · Evolut Low Risk · Prosthetic valve thrombosis · Paravalvular leak · MitraClip · TEER · Flail leaflet · Aortic stenosis symptom triad · AS syncope angina heart failure
Acute valvular emergencies present as cardiogenic shock, flash pulmonary oedema, syncope, or cardiac arrest, and they are defined by THREE NATIVE-VALVE LESIONS plus prosthetic valve failure. (1) CRITICAL AORTIC STENOSIS (AVA <1.0 cm², mean gradient >40 mmHg, peak velocity >4 m/s; critical/shock when AVA ~0.6 and gradient ~50): a FIXED LV outflow obstruction with a stiff hypertrophied ventricle that is PRELOAD-, AFTERLOAD- and ATRIAL-KICK dependent. The AS symptom triad is ANGINA (5-yr survival), SYNCOPE (3-yr), HEART FAILURE (2-yr) — prognosis without AVR is dismal. Haemodynamic goal: SLOW heart rate (60-80, long diastolic filling time), HIGH SVR (noradrenaline — never vasodilate), ADEQUATE PRELOAD (cautious diuresis only), and MAINTAIN SINUS RHYTHM (AF is devastating — synchronised DC cardioversion if unstable). AVOID nitrates/GTN, ACEi/ARB, high-dose beta-blockers, and over-diuresis. Definitive therapy is AORTIC VALVE REPLACEMENT (surgical AVR or TAVI); balloon aortic valvuloplasty (BAV) or VA-ECMO bridge the unstable patient. (2) ACUTE MITRAL REGURGITATION (papillary muscle rupture 2-7 days post-inferior MI, chordal rupture, endocarditis, trauma): sudden volume overload of a small non-compliant LA - flash pulmonary oedema + shock; the murmur may be SOFT or ABSENT (rapid LA pressure equalisation) — never be reassured by a quiet chest. Echo (flail leaflet, eccentric jet) is diagnostic. Haemodynamic goal: LOW SVR/afterload reduction (nitroprusside; IABP gives mechanical unloading) + inotrope (dobutamine/milrinone); definitive therapy is URGENT MV repair/replacement, or MitraClip (TEER) in the prohibitive-surgical-risk patient. (3) ACUTE AORTIC REGURGITATION (Type A dissection, endocarditis, trauma): diastolic run-off into a non-compliant LV - rapidly rising LVEDP - acute pulmonary oedema + shock; the wide pulse pressure, water-hammer pulse and Austin-Flint murmur of CHRONIC AR are usually ABSENT in acute AR (LV has not adapted; pulse pressure may be normal, murmur SHORT). Haemodynamic goal: LOW SVR + HIGH HEART RATE (tachycardia is protective — shorter diastole = less regurgitation) + vasopressor (noradrenaline to raise diastolic/coronary perfusion); AVOID pure beta-blockers in isolated acute AR (abolishes the compensatory tachycardia) and AVOID IABP (diastolic augmentation WORSENS the regurgitant volume) — except that in Type A dissection WITH AR, beta-blockers ARE first-line (to reduce dp/dt shear) and the AR is corrected by emergency surgery. Definitive therapy is URGENT SURGICAL AVR. (4) PROSTHETIC VALVE DYSFUNCTION: thrombosis (mechanical valve — obstructive: rtPA/systemic thrombolysis or surgery; non-obstructive: heparin ± lysis), pannus, dehiscence (paravalvular leak), structural deterioration (bioprosthesis), and prosthetic endocarditis — any unexplained shock/pulmonary oedema in a prosthetic-valve patient demands urgent echo (± fluoroscopy for leaflet motion). In ALL acute valvular emergencies the ECHOCARDIOGRAM is diagnostic and must be obtained EARLY; standard 'heart failure' therapy (nitrates, aggressive diuresis, IABP, negative inotropes) can be CATASTROPHIC if applied without knowing the lesion.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview and definition

Acute severe valvular emergencies are a group of mechanical, surgically-correctable catastrophes in which a native or prosthetic valve fails suddenly, producing flash pulmonary oedema, cardiogenic shock, syncope, or cardiac arrest. They are united by one principle that overrides all others: you cannot manage these with generic 'heart failure' therapy. The haemodynamic support that saves a warm-wet dilated-cardiomyopathy patient — nitrates, aggressive diuresis, afterload reduction, an intra-aortic balloon pump — can kill a patient with critical aortic stenosis or acute aortic regurgitation within minutes. The lesion must be identified by echocardiography early, and the haemodynamic strategy must be tailored to the specific valve.[4][5]
The AHA/ACC and ESC/EACTS valvular guidelines frame the decision-making around (a) confirming severity by echocardiography, (b) stabilising haemodynamics in a lesion-specific way as a bridge, and (c) proceeding to definitive mechanical correction — valve replacement or repair, transcatheter or surgical — by a multidisciplinary heart team, because no pharmacological regimen cures a structural valve lesion.[4][5]
[3]The haemodynamic doctrine — why each valve has a non-negotiable strategy
The single most important concept in valvular emergencies is that each lesion dictates a unique haemodynamic goal, and violating that goal is the commonest cause of iatrogenic collapse. The logic derives from the pressure-volume relationship and the compliance of the receiving chamber.[4]
Critical AS — the ventricle is starved of preload and afterload. The stenotic valve is a fixed obstruction: stroke volume cannot rise to compensate, so cardiac output is rate-dependent and the hypertrophied, stiff LV sits on the steep portion of the Starling curve. It therefore needs high preload (to maintain filling pressure across the stiff ventricle), high afterload/SVR (vasodilation drops diastolic pressure, stealing subendocardial coronary perfusion and collapsing the Starling curve), a slow rate with a long diastolic filling time (the stiff LV fills slowly; tachycardia abbreviates filling), and sinus rhythm with atrial kick (atrial contraction contributes 30-40% of LV filling in the non-compliant ventricle, versus 15-20% normally). Loss of any of these — a vasodilator, a diuretic, an episode of AF — can precipitate irreversible cardiogenic shock.[5]
Acute MR — the ventricle has a low-impedance escape route. The regurgitant orifice lets blood escape backwards into the LA during systole, so forward stroke volume is exquisitely sensitive to afterload: the lower the systemic vascular resistance, the greater the fraction of stroke volume that goes forward into the aorta rather than backwards into the LA. The strategy is therefore afterload reduction (nitroprusside; the IABP provides mechanical systolic unloading) plus inotropic support to maintain forward output, as a bridge to urgent surgical or percutaneous correction.[3]
Acute AR — the ventricle is drowning in diastolic run-off. In diastole, blood runs back from the aorta into the LV through the incompetent valve, so the therapeutic aim is to shorten diastole (a faster heart rate means less time per beat for regurgitation) and to support the diastolic pressure (coronary perfusion happens in diastole and is threatened by the run-off). A pure beta-blocker abolishes the protective tachycardia; an IABP, which augments diastolic pressure, worsens the regurgitant volume. The exception is Type A dissection with AR, where reducing the aortic dp/dt (shear stress) with a beta-blocker is the priority because it limits propagation and rupture, and the regurgitation is corrected at emergency surgery.[4]
[3]Critical aortic stenosis — the fixed-obstruction emergency
Definition and severity. Severe AS is defined echocardiographically as an aortic valve area (AVA) <1.0 cm² (or <0.6 cm²/m² indexed), a mean transaortic gradient >40 mmHg, and a peak jet velocity >4.0 m/s; a dimensionless index <0.25 supports the diagnosis. Critical AS — the patient in or near cardiogenic shock — typically has an AVA ~0.6 cm² and a mean gradient ~50 mmHg. When flow is low (low-flow low-gradient AS, e.g. LVEF <40%), dobutamine stress echocardiography distinguishes true-severe (gradient rises with flow) from pseudo-severe AS, and identifies lack of contractile reserve (a marker of high perioperative risk).[5]
The symptom triad and prognosis. Symptomatic severe AS carries a grim prognosis that the intensivist must respect: angina (median survival ~5 years without AVR — from LV hypertrophy, high wall stress, and compressed subendocardial vasculature, even without epicardial coronary disease), syncope (~3 years — exertional, because the fixed cardiac output cannot rise with demand), and heart failure (~2 years — initially diastolic from the stiff LV, then systolic as the ventricle decompensates). Once symptoms appear, median survival without AVR is only 2-3 years, and critical AS in cardiogenic shock has near-100% mortality without valve replacement. The ICU presentation is most often decompensated heart failure or cardiogenic shock in a patient with known (or previously undiagnosed) AS.[5]
Clinical features. A slow-rising, low-volume pulse (pulsus parvus et tardus) with a narrow pulse pressure; a harsh crescendo-decrescendo ejection systolic murmur radiating to the carotids, with a soft or absent A2 (paradoxical splitting), an ejection click (in mobile bicuspid valves), and a thrusting but non-displaced apex beat (concentric hypertrophy). ECG shows LV hypertrophy with strain and often left anterior hemiblock or LBBB. The chest X-ray may be normal or show cardiomegaly and pulmonary venous congestion. Echo is diagnostic and indispensable.[3]
Acute mitral regurgitation — the low-impedance-escape emergency
Pathophysiology. Acute MR dumps a large regurgitant volume into a small, non-compliant left atrium that has not had time to adapt (unlike chronic MR, where the LA and LV dilate and accommodate the volume). The acute LA pressure spike is transmitted directly to the pulmonary veins and capillaries, producing flash pulmonary oedema, and forward cardiac output falls, producing cardiogenic shock. Two features are counter-intuitive and frequently missed: the murmur may be soft or absent (because the LA pressure rises so rapidly it equalises with LV systolic pressure, abolishing the gradient that generates the murmur), and the patient can deteriorate from a salvageable lesion to arrest in hours.[3]
Causes. (a) Papillary muscle rupture — classically 2-7 days after an inferior MI; the posteromedial papillary muscle is vulnerable because it has a single blood supply (right coronary/PDA), unlike the anterolateral muscle (dual supply from LAD and circumflex). (b) Chordal rupture — myxomatous degeneration (mitral valve prolapse), connective tissue disease, trauma. (c) Infective endocarditis — destructive leaflet perforation or chordal involvement. (d) Ischaemic papillary muscle dysfunction — transient, may resolve with revascularisation. (e) Iatrogenic — post-MV surgery, post-balloon valvuloplasty. (f) Blunt chest trauma.[3]
Clinical features. Sudden onset of severe dyspnoea, orthopnoea, pink frothy sputum, hypoxaemia, and shock, often in the context of recent MI, known valve disease, or sepsis (endocarditis). A pansystolic murmur at the apex radiating to the axilla is classic, BUT in acute MR it may be soft, early, decrescendo, or entirely absent — the absence of a murmur must never reassure you. A hyperdynamic, displaced apex (if chronic MR coexists) and signs of the underlying cause (e.g. recent infarct, stigmata of endocarditis) may be present. Echo is diagnostic — it demonstrates the mechanism (flail leaflet, ruptured papillary muscle head, prolapse, vegetation), the regurgitant jet (colour Doppler, often eccentric and wall-impinging), and the haemodynamic severity (vena contracta, effective regurgitant orifice area, pulmonary vein systolic flow reversal, elevated pulmonary artery pressure). Transoesophageal echo (TOE) gives superior detail for surgical planning.[3]
Acute aortic regurgitation — the diastolic run-off emergency
Pathophysiology. In acute AR, the incompetent aortic valve allows blood to run back from the aorta into the LV during diastole. Because the LV has not had time to dilate and adapt (unlike chronic AR, where the ventricle becomes large and compliant), the sudden regurgitant volume rapidly raises LV end-diastolic pressure (LVEDP), which is transmitted to the LA and pulmonary veins, producing acute pulmonary oedema and shock. The diastolic run-off also lowers aortic diastolic pressure, threatening coronary perfusion (which occurs in diastole) and producing subendocardial ischaemia. Crucially, the classic signs of chronic AR — wide pulse pressure, bounding water-hammer pulse, Corrigan's sign, Austin-Flint murmur — are usually ABSENT in acute AR, because the LV cannot accommodate the volume and LVEDP equalises with aortic diastolic pressure early in diastole, truncating the run-off. The murmur is typically short, early diastolic, and decrescendo rather than the long, blowing diastolic murmur of chronic AR; the pulse pressure may be normal.[3][4]
Causes. (a) Acute Type A aortic dissection — the dissection flap tears or dilates the annulus, prolapses through the valve, or detaches a leaflet, causing acute AR. (b) Infective endocarditis — leaflet destruction, perforation, or vegetation preventing coaptation. (c) Blunt chest trauma — leaflet tear. (d) Prosthetic valve failure (see below). (e) Rupture of a sinus of Valsalva. The two dominant causes the intensivist must always consider are dissection (a surgical emergency in its own right) and endocarditis.[4]
Clinical features. Sudden severe dyspnoea, pulmonary oedema, hypotension, and shock, often with chest/back pain (dissection) or constitutional/embolic features (endocarditis). An early diastolic decrescendo murmur at the left sternal edge (Erbs point) with the patient sitting forward in held expiration is characteristic but may be short and easily missed; a soft S1 and an S3 are common. Signs of the cause (blood-pressure differential between arms, widened mediastinum on chest X-ray, new conduction block from aortic-root abscess) should be sought. Echo is diagnostic — colour and continuous-wave Doppler show the regurgitant jet, a short pressure half-time (reflecting rapid diastolic pressure equalisation), and premature mitral valve closure (the high LVEDP pushes the mitral valve closed before systole, a sign of severe acute AR).[3]
Prosthetic valve dysfunction — the hidden catastrophe
Any patient with a prosthetic heart valve who presents with unexplained shock, pulmonary oedema, syncope, an embolic event, or new murmur has prosthetic valve dysfunction until proven otherwise. The diagnosis is urgent echo (often combined with fluoroscopy to assess mechanical leaflet motion), and the management is lesion-specific.[5][6]
(a) Prosthetic valve thrombosis — most often a mechanical valve with inadequate anticoagulation. It may be obstructive (thrombus prevents opening/closing -> acute stenosis or regurgitation -> shock) or non-obstructive (smaller thrombus, often presenting with embolism). Diagnosis: echo (immobile/abnormally moving leaflet, raised transprosthetic gradient, reduced effective orifice area) and fluoroscopy (restricted leaflet motion); the distinction between thrombus and pannus (fibrous ingrowth) may require CT. Treatment of obstructive thrombosis: surgery (high-risk but definitive) or thrombolysis (e.g. slow infusion of rtPA / alteplase, or streptokinase) — the choice depends on surgical risk, clot burden, thrombolysis contraindications, and valve location (left-sided thrombolysis carries a stroke/embolism risk). Non-obstructive thrombosis is usually managed with intensified heparin ± lysis.[6]
(b) Paravalvular leak / dehiscence — the prosthetic valve partially separates from the annulus (from endocarditis with annular destruction, suture failure, or degeneration), producing a paravalvular regurgitant jet that can cause haemolysis, heart failure, or shock. Diagnosis by echo (± TOE); treatment ranges from conservative management of small stable leaks to percutaneous closure (occluder devices) or surgical re-operation for large/dehiscent leaks.
[6](c) Structural valve deterioration — bioprosthetic valves degenerate over years (calcification, tear, perforation) producing stenosis or regurgitation; this may decompensate acutely. Echo defines the mechanism; valve-in-valve TAVI is increasingly an option for failed surgical bioprostheses, alongside redo surgery.[6]
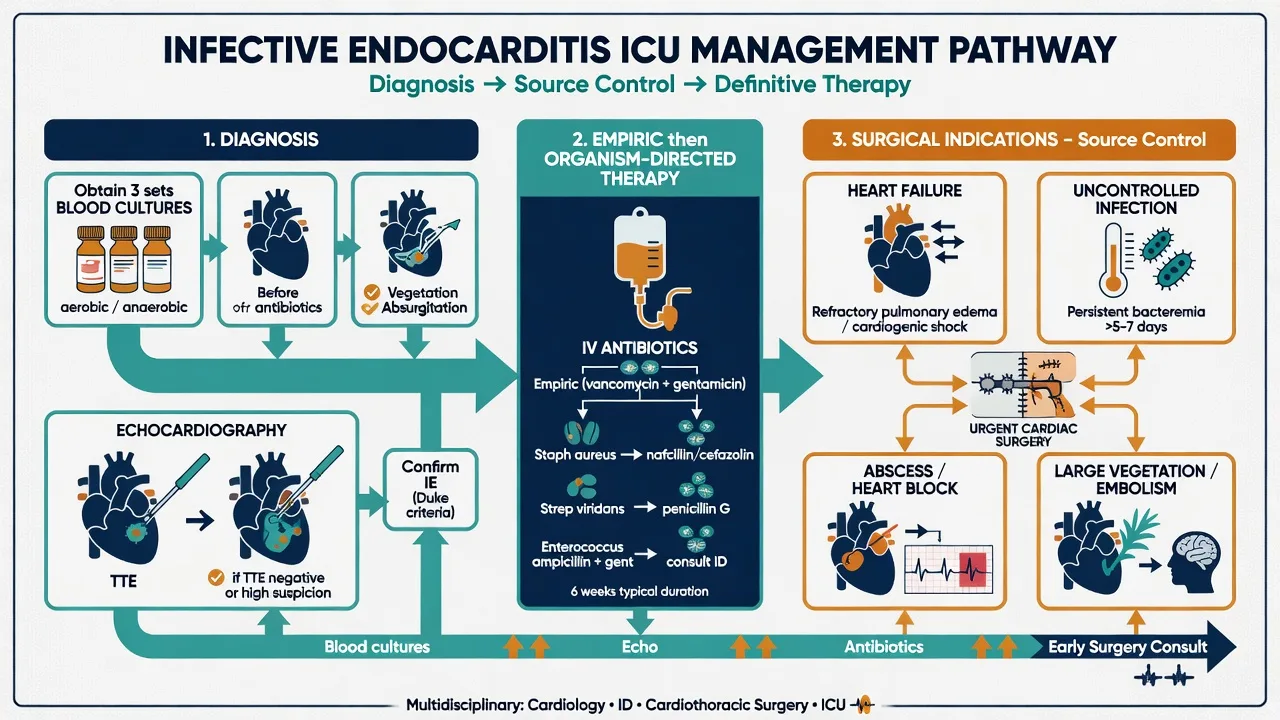
(d) Prosthetic valve endocarditis — carries a higher mortality than native-valve endocarditis because of the potential for annular/paravalvular abscess, conduction block, and destructive regurgitation. Diagnosis follows modified Duke criteria with TOE (more sensitive than TTE for prosthetic valves and complications). Early surgery is indicated for heart failure, uncontrolled infection, abscess/conduction block, and large vegetations with embolic risk.[4]
Comparison tables
[3] [1] [1]Clinical pearls
Red flags
Prognosis
Valvular emergency evidence and outcomes
Outcomes. Critical AS in cardiogenic shock has near-100% mortality without valve replacement; AVR (surgical or TAVI) transforms prognosis, with low-risk TAVI and SAVR now both showing excellent outcomes (PARTNER 3, Evolut Low Risk). Acute MR from papillary muscle rupture carries mortality approaching 100% without surgery; urgent MV repair/replacement achieves survival of roughly 70-90% (worse in ischaemic/ endocarditic aetiologies). Acute severe AR from Type A dissection or destructive endocarditis is lethal without urgent surgical AVR — dissection mortality rises ~1-2% per hour untreated. Prosthetic valve thrombosis managed by prompt surgery or thrombolysis has a guarded but salvageable prognosis; delay is the enemy. Across all four lesions the determinants of survival are early echocardiographic diagnosis, a lesion-specific haemodynamic bridge, and rapid definitive mechanical correction by the heart team — prolonged pharmacological support without a definitive plan signals futility.[4][5]
Exam SAQ — densified leaf
10 minutes · 10 marks
In structured CICM/FFICM style: (1) define the core entity in one sentence; (2) list three immediate ICU priorities; (3) state two investigations that change management; (4) name one evidence landmark or guideline anchor; (5) give one fatal exam trap.
Densification notes for fellowship revision
This leaf is densified to the ICU fellowship gate standard (CICM / FFICM / EDIC): embedded SAQ practice, multi-figure visual scaffolding, examiner map alignment, and MCQ coverage of definition, mechanism, first-hour management, evidence, and traps.
[5]- Revision checkpoint 1: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 2: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 3: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 4: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 5: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 6: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 7: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Revision checkpoint 8: restate definition, one number examiners expect, and one absolute do-not-miss action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
- Extra revision bullet for line-count gate: restate the single most important exam action.
References
- [1]Mack MJ, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med, 2019.PMID 30883058
- [2]Popma JJ, et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med, 2019.PMID 30883053
- [3]Lancellotti P, et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 1: aortic and pulmonary regurgitation (native valve disease). Eur J Echocardiogr, 2010.PMID 20375260
- [4]Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC), et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J, 2012.PMID 22922415
- [5]Nishimura RA, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol, 2014.PMID 24603191
- [6]Abbas AE, et al. Hemodynamic principles of prosthetic aortic valve evaluation in the transcatheter aortic valve replacement era. Echocardiography, 2020.PMID 32362021