ICU · Endocrine
Hypoglycaemia in the ICU
Also known as Hypoglycaemia · Hypoglycaemic coma · Insulin overdose · Neuroglycopenia · Whipple triad · Sulfonylurea overdose · Octreotide · Insulinoma · Hypoglycaemia-associated autonomic failure · Insulin autoimmunity (Hirata syndrome)
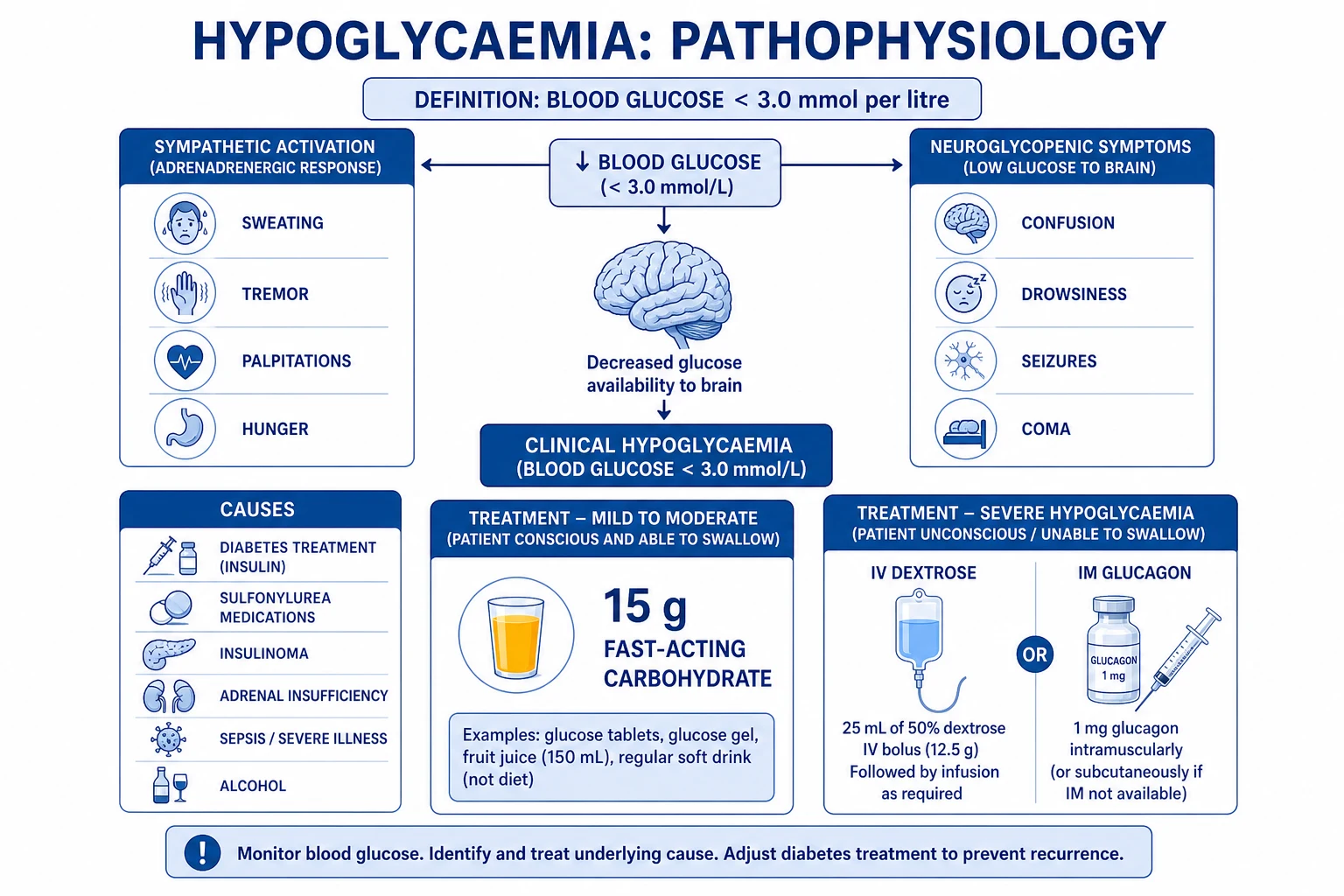
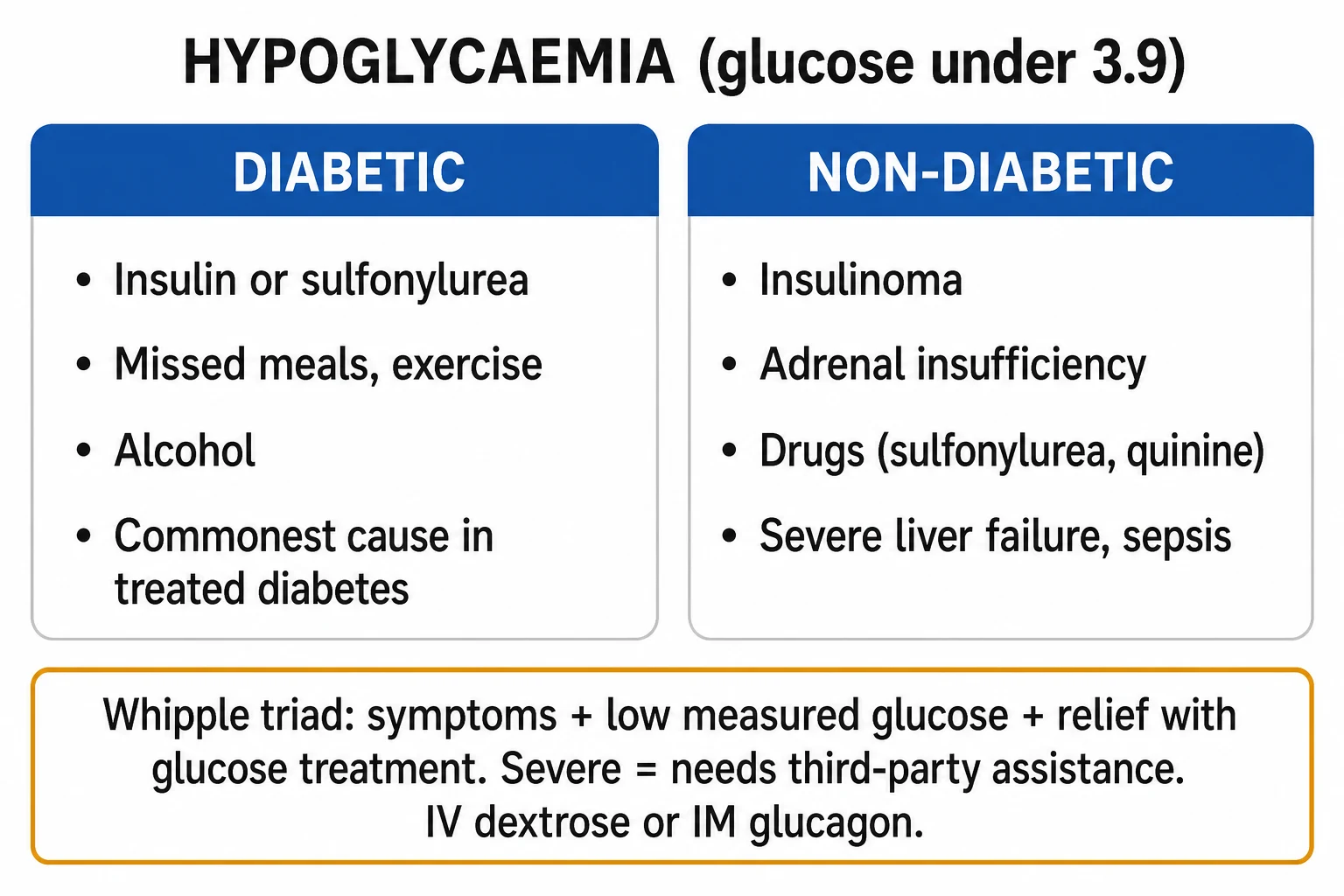
Hypoglycaemia (plasma glucose <3.9 mmol/L / 70 mg/dL with symptoms; severe <2.2 mmol/L / 40 mg/dL with altered consciousness requiring assistance) is common in ICU and independently associated with increased mortality. The brain is an obligate glucose consumer (~100 g/day) and cannot store it, so profound or prolonged hypoglycaemia causes neuronal death. Causes in ICU: insulin (iatrogenic sliding-scale/DKA–HHS errors, exogenous overdose — the single most common), sulfonylureas (prolonged recurrent hypoglycaemia — add octreotide), insulinoma, sepsis (increased utilisation + impaired gluconeogenesis), hepatic failure, renal failure (reduced insulin clearance), adrenal insufficiency, malaria/quinine, alcohol, and post-bariatric dumping. The counterregulatory response (glucagon, adrenaline, cortisol, growth hormone) is blunted in critical illness and diabetes. Whipple's triad defines true hypoglycaemia. Management: conscious — 15 g fast carbohydrate, recheck in 15 min (15-15 rule); unconscious — IV dextrose (50% 25–50 mL via a large vein, or 10% infusion); IM glucagon 1 mg if no IV access (ineffective with depleted glycogen — liver failure, alcohol, starvation, and counterproductive in sulfonylurea overdose); octreotide for sulfonylurea; hydrocortisone for adrenal insufficiency; thiamine before glucose in alcoholics. NICE-SUGAR: target glucose 6–10 mmol/L — tight control (4.4–6.1) caused more severe hypoglycaemia and higher mortality.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview & definition
Hypoglycaemia is a plasma glucose low enough to cause symptoms and/or signs.[8] The American Diabetes Association / Endocrine Society workgroup classifies it by severity:[8]
- Level 1 (mild): glucose <3.9 mmol/L (70 mg/dL) — autonomic symptoms, patient self-treats.
- Level 2 (moderate): glucose <3.0 mmol/L (54 mg/dL) — autonomic + early neuroglycopenic symptoms; intervention required, but patient may still self-treat.
- Level 3 (severe): glucose <2.2 mmol/L (40 mg/dL) with altered consciousness / seizure / coma requiring assistance — a medical emergency; the patient cannot self-treat. In the ICU, severe hypoglycaemia is independently associated with a 2–6-fold increase in mortality.[2][5]
The brain is an obligate glucose consumer (≈100 g/day) and stores no glycogen, so profound or prolonged hypoglycaemia → energy failure → neuronal death (hippocampus and cerebral cortex most vulnerable).[2]
Whipple's triad — defining true hypoglycaemia
Before investigating spontaneous hypoglycaemia (insulinoma etc.), all three elements must be documented:[8]
- Symptoms/signs consistent with hypoglycaemia (autonomic and/or neuroglycopenic).
- A low plasma glucose measured at the time of symptoms (laboratory confirmation, not just fingerprick).
- Relief of symptoms when the glucose is raised.[6]
Without the triad, "low" readings may be artefactual (sample from a line carrying dextrose, faulty strip, delays in processing — in-vitro glycolysis in leukaemia with very high white-cell count gives spuriously low glucose).[1]
[7]Causes in ICU

Treatment-related
Most common
- Insulin (sliding scale errors, DKA treatment — insulin dose too high)
- Sulfonylureas (gliclazide, glipizide — stimulate insulin secretion)
- Insulinoma (rare — fasting hypoglycaemia with high insulin + C-peptide)
- SGLT2 inhibitors (can cause euglycaemic DKA)
Critical illness
Organ dysfunction
- Sepsis (increased glucose utilisation, impaired gluconeogenesis)
- Liver failure (impaired gluconeogenesis and glycogen stores)
- Renal failure (reduced insulin clearance, reduced gluconeogenesis)
- Adrenal insufficiency (impaired gluconeogenesis — check cortisol)
- Malaria (especially severe falciparum — quinine-induced)
Drugs
Iatrogenic/toxic
- Beta-blockers (mask autonomic symptoms — no sweating/tremor)
- Quinine (stimulates insulin secretion — especially in malaria)
- Pentamidine (toxic to beta cells — initial hypoglycaemia then diabetes)
- Alcohol (inhibits gluconeogenesis)
- Salicylates (high dose)
Pathophysiology — the counterregulatory response
Glucose homeostasis relies on a coordinated endocrine response that the normal brain mounts as glucose falls. Four hormones defend plasma glucose, in this order:[2][6]
Glucagon
First responder (~3.6 mmol/L)
- Pancreatic α-cell peptide → hepatic glycogenolysis + gluconeogenesis
- Fast (5–20 min), raises glucose ~2–4 mmol/L
- Basis for IM glucagon therapy
- FAILED in: depleted glycogen (liver failure, alcohol, starvation, anorexia); blunted in critical illness and long-standing diabetes
Adrenaline (epinephrine)
Second wave (~3.4 mmol/L)
- Adrenal medulla → glycogenolysis, gluconeogenesis, lipolysis, inhibits insulin, stimulates glucagon
- Generates the autonomic symptoms (sweating, tremor, palpitations)
- MASKED by beta-blockers and blunted after repeated hypoglycaemia (HAAF)
Cortisol
Delayed, sustained (~3.2 mmol/L)
- HPA axis → permissive for gluconeogenesis, antagonises insulin
- Acts over hours — sustains recovery and prevents recurrence
- FAILED in adrenal insufficiency (CIRCI) → recurrent hypoglycaemia; give hydrocortisone
Growth hormone
Slow, late (~3.0 mmol/L)
- Antagonises insulin, mobilises free fatty acids (alternative fuel)
- Important for prolonged defence; suppressed in prolonged critical illness
Two key failure modes in the ICU:[3]
- Critical illness attenuates counterregulation. Glucagon and adrenaline responses are blunted within days; the cortisol axis (CIRCI) frequently fails, so recurrent hypoglycaemia in a septic/shocked patient should prompt a random cortisol and empirical hydrocortisone.[6]
- Hypoglycaemia-associated autonomic failure (HAAF) in diabetes. Each antecedent hypoglycaemic episode lowers the glycaemic threshold for the next counterregulatory response — the patient loses autonomic warning symptoms and swings straight from euglycaemia into neuroglycopenia ("hypoglycaemia unawareness"). This is the central mechanism by which tight glucose control in ICU becomes dangerous.[2]
Symptoms
Hypoglycaemia symptom progression
Autonomic (3.5-3.9 mmol/L)
Sympathetic activation: sweating, tremor, palpitations, hunger, anxiety, piloerection. These are WARNING symptoms — patient may self-treat (eat/drink). CAUTION: beta-blockers mask these symptoms. Also: patients with recurrent hypoglycaemia develop hypoglycaemia unawareness (loss of autonomic warning).
Neuroglycopenic (<3.5 mmol/L)
Brain deprived of glucose: confusion, irritability, slurred speech, visual disturbance, weakness, ataxia. May mimic alcohol intoxication or stroke. Then: drowsiness → seizures → coma. Severe (<2.2 mmol/L): irreversible neuronal death (glucose is the brain only energy source under normal conditions).
Severe (<2.2 mmol/L)
Coma, seizures, permanent brain injury. EEG: slow waves then flat. Neuronal death occurs because brain cannot use alternative fuels (ketones, lactate) quickly enough. This is a MEDICAL EMERGENCY — treat immediately.
ICU causes — the expanded differential
Excess insulin (exogenous)
C-peptide LOW
- Sliding-scale / infusion error, DKA–HHS over-treatment, wrong pump rate
- Deliberate self-harm (non-diabetic nurses/patients, factitious)
- Insulin + LOW/undetectable C-peptide + low β-hydroxybutyrate
- Long-acting analogues (glargine, detemir, degludec) → prolonged effect, observe 24 h+
Insulin secretagogues
C-peptide HIGH
- Sulfonylureas (glibenclamide, gliclazide, glipizide, glimepiride) — prolonged, recurrent; add octreotide
- Quinine, quinolones, pentamidine — β-cell toxins / insulin releasers
- Insulin + HIGH C-peptide + HIGH proinsulin; drug confirmed on urine/plasma sulfonylurea screen
Endogenous hyperinsulinism
C-peptide HIGH
- Insulinoma — neuroglycopenia in fasted state; 72-h fast diagnostic
- Non-insulinoma pancreatogenous hypoglycaemia (NIPHS) / nesidioblastosis
- Autoimmune insulin syndrome (Hirata) — anti-insulin antibodies; postprandial hypoglycaemia
Critical illness
Multi-factorial
- Sepsis — cytokine-driven glucose utilisation + impaired hepatic output
- Liver failure — loss of gluconeogenesis + glycogen
- Renal failure — reduced insulin clearance + loss of renal gluconeogenesis
- Adrenal insufficiency / CIRCI — cortisol deficiency; check cortisol
- Severe burns, large tumour burden, refeeding syndrome
Drugs & toxins
Mechanism varies
- Beta-blockers — mask adrenergic warning + impair gluconeogenesis
- Alcohol — blocks gluconeogenesis (NADH/NAD+ shift); coexists with starvation
- ACE inhibitors, salicylates, disopyramide, trimethoprim-sulfamethoxazole
- Drug–drug: fluoroquinolones + sulfonylureas
Post-bariatric / surgical
Postprandial
- Late dumping after Roux-en-Y gastric bypass — exaggerated GLP-1 → hyperinsulinaemia
- Nesidioblastosis / islet hyperplasia — 1–3 h post-meal hypoglycaemia
- Manage with small low-CHO meals, acarbose, diazoxide; rarely partial pancreatectomy
Non-islet cell tumour
Insulin LOW
- Large retroperitoneal/pleural sarcoma, hepatoma — secrete "big" IGF-II
- Suppresses GH → low IGF-I → low insulin and ketones despite hypoglycaemia
- Treat with glucose + glucocorticoids (restore GH/IGF axis) + tumour debulking
Management
Hypoglycaemia treatment protocol
Check glucose (fingerprick at bedside)
Check glucose in ANY patient with: altered mental status, seizure, coma, syncope, or unexplained symptoms. Do NOT assume intoxication or stroke without checking glucose first. Fingerprick glucose takes 5 seconds — no excuse to miss hypoglycaemia. In shock/vasoconstriction, confirm a borderline reading with an arterial or laboratory sample.
If conscious and can swallow
Oral glucose (15-20 g fast-acting carbohydrate): glucose tablets, Lucozade, fruit juice, glucose gel (Hypostop). Recheck glucose in 15 min. If still low: repeat. Then give longer-acting carbohydrate (toast, biscuit) to prevent recurrence.
If unconscious or cannot swallow
IV dextrose: 50% dextrose 25-50 mL (12.5-25 g) IV rapidly via large vein. Caution: 50% is viscous and irritant — use central line if possible, or use 10% dextrose 100-200 mL. Recheck glucose in 10-15 min. If still low: repeat. Then start 10% dextrose infusion (50-100 mL/h) to prevent recurrence.
If IV access not available
IM glucagon 1 mg (stimulates hepatic glycogenolysis — releases stored glucose). Works within 10-15 min. Caution: does NOT work if: liver failure (no glycogen stores), chronic alcoholism (depleted glycogen). Must follow with oral/IV glucose once conscious (glucagon effect is transient).
Sulfonylurea overdose
Sulfonylureas stimulate insulin secretion — hypoglycaemia is prolonged and recurrent. IV dextrose alone is insufficient (insulin continues to be secreted). Add: octreotide 50-100 mcg SC Q8H (somatostatin analogue — inhibits insulin secretion). Monitor for 24-48h (long half-life of sulfonylureas).
Identify and treat cause
Review: insulin/sulfonylurea doses, renal function, liver function, sepsis. Check cortisol if adrenal insufficiency suspected (hypotension + recurrent hypoglycaemia). Adjust insulin regimen. Consider continuous glucose monitoring if recurrent episodes. NICE-SUGAR: target 6-10 mmol/L — avoid both hypo- and hyperglycaemia.
The 15-15 rule (mild–moderate hypoglycaemia, conscious patient)
The ADA-endorsed outpatient/community rule generalises to the awake ICU patient who can swallow safely:[8]
- 15 g fast-acting carbohydrate — 4 glucose tablets (4 g each), 150–200 mL fruit juice or non-diet soft drink, 1 tube glucose gel, or 1 tablespoon sugar/honey. Avoid chocolate/fats (slow absorption) and overtreatment (rebound hyperglycaemia).
- Recheck capillary glucose at 15 min.
- If still <3.9 mmol/L → repeat the 15 g.
- Once recovered (≥4.0 mmol/L and symptom-free) and the next meal is >1 h away, give a long-acting carbohydrate + protein snack (bread, biscuit, milk) to prevent recurrence.[1]
ICU caveats to the 15-15 rule: an impaired-consciousness or recently-extubated patient may aspirate oral glucose gel — use IV dextrose instead. Do not give oral fluids to a patient lying flat or with a reduced GCS.[1]
Severe hypoglycaemia (altered consciousness) — ICU pharmacology
IV dextrose (first-line)
Immediate, reliable
- 50% dextrose 25–50 mL (12.5–25 g) via LARGE peripheral vein or central line over 2–3 min
- Response in 5–10 min; recheck at 10–15 min and repeat if needed
- ALTERNATIVES: 10% dextrose 100–200 mL over 10–15 min (less irritant, more volume); 10% infusion 50–100 mL/h for maintenance
- CAUTION: 50% is hypertonic (osmolarity 2520 mOsm/L) — extravasation causes tissue necrosis; flush well, dilute to ≤10–20% in small peripheral veins
IM glucagon
No IV access
- 1 mg IM/SC → hepatic glycogenolysis; works in 10–15 min
- INEFFECTIVE with depleted glycogen: liver failure, alcoholism, starvation, anorexia, sepsis
- Counter-productive in sulfonylurea overdose (stimulates further insulin secretion)
- Transient effect — must follow with oral/IV dextrose once conscious; can cause vomiting (aspiration risk in obtunded patient)
Octreotide
Sulfonylurea overdose
- Somatostatin analogue; 50–100 µg SC q8h (or 25–50 µg/h IV infusion)
- Inhibits pancreatic insulin release — the definitive antidote for sulfonylurea hypoglycaemia
- Give WITH dextrose (dextrose alone provokes rebound insulin release)
- Continue 24–72 h — glibenclamide half-life up to 24–72 h, especially in renal failure
Hydrocortisone
Adrenal insufficiency
- 100 mg IV stat then 50 mg q6h (or 200 mg/24 h infusion)
- Indicated when cortisol deficient (CIRCI) — recurrent hypoglycaemia + vasopressor-dependent shock
- Restores gluconeogenesis; effect over hours, not minutes — give WITH dextrose
- Check a random cortisol and short Synacthen test, but do NOT delay treatment
Thiamine
Before glucose in alcoholics
- 100–300 mg IV BEFORE the dextrose load in any alcoholic/malnourished patient
- Prevents precipitation of Wernicke encephalopathy (thiamine is a glycolysis cofactor depleted by the glucose load)
- Empirical — do not wait for confirmation
Diazoxide
Where octreotide unavailable
- Opens β-cell K-ATP channel → inhibits insulin release
- 300 mg loading then 100–200 mg q4–6h PO/NG (or 1–3 mg/kg)
- Alternative/adjunct to octreotide in refractory sulfonylurea or insulinoma hypoglycaemia
- Side-effects: hypotension, sodium/water retention (give with a diuretic)
Refractory / recurrent hypoglycaemia in ICU
Approach when hypoglycaemia keeps recurring
Secure a continuous dextrose supply
10% dextrose infusion titrated to keep glucose 6–10 mmol/L; if refractory, escalate to 20% or 50% via central line, or add enteral feed. Do NOT chase with boluses alone — establish a basal supply.
Reconsider the cause — take blood DURING the hypoglycaemic spell
Draw: insulin, C-peptide, proinsulin, β-hydroxybutyrate, cortisol, GH, sulfonylurea screen, lactate, ammonia, blood alcohol, and free insulin/IGF-II if a tumour is suspected. The "critical sample" during a true spell is the single most informative test.
Apply mechanism-specific therapy
Sulfonylurea → octreotide 50–100 µg SC q8h. Insulinoma → diazoxide + dextrose; definitive = surgical resection. Adrenal insufficiency → hydrocortisone 100 mg IV. Non-islet cell tumour (big-IGF-II) → glucocorticoids + tumour debulking/radiotherapy. Autoimmune insulin syndrome → glucocorticoids/plasmapheresis.
Switch to subcutaneous continuous glucose monitoring
Interstitial sensors trend glucose every 1–5 min with low alarms; useful in recurrent episodes. Confirm borderline readings with arterial/lab glucose — sensors lag and read falsely low in shock/peripheral oedema.
Diagnostic workup of spontaneous (non-iatrogenic) hypoglycaemia
Investigating insulinoma and other spontaneous causes
Confirm Whipple triad
Symptoms + documented low glucose + relief with glucose — all three. Without it, do not over-investigate a single borderline reading (consider sample/processing artefact).
Prolonged (72-h) supervised fast
The gold standard for insulinoma. Stop when symptomatic AND glucose <2.5 mmol/L (or 72 h elapsed). Draw the critical sample (insulin, C-peptide, proinsulin, β-hydroxybutyrate, sulfonylurea screen) then terminate with IV dextrose.
Interpret the critical sample
INAPPROPRIATELY HIGH insulin (>3 µU/mL) + HIGH C-peptide + HIGH proinsulin + LOW β-hydroxybutyrate during hypoglycaemia = endogenous hyperinsulinism (insulinoma or sulfonylurea). LOW C-peptide = exogenous insulin. LOW insulin + LOW ketones + low glucose = non-islet cell tumour (big-IGF-II).
Sulfonylurea screen
Urine/plasma assay — distinguishes sulfonylurea overdose (also high C-peptide) from insulinoma. Essential: a "first-fit" hypoglycaemia workup excludes sulfonylurea before concluding insulinoma.
Localise an insulinoma
CT/MRI pancreas first; if negative, endoscopic ultrasound ± arterial calcium stimulation with hepatic venous insulin sampling; intra-operative ultrasound at surgery. >90% are solitary, benign, <2 cm.
Post-bariatric (late dumping) hypoglycaemia
After Roux-en-Y gastric bypass, rapid gastric emptying delivers nutrient to the distal small bowel → exaggerated GLP-1 and incretin release → hyperinsulinaemia. Neuroglycopenia occurs 1–3 h postprandially, rarely with fasting.[6]
- Diagnosis: mixed-meal test (not 72-h fast) with glucose + insulin during symptoms; exclude insulinoma (C-peptide high in both — history of bypass + postprandial timing is key).
- Management ladder: (1) small, frequent low-glycaemic-index / low-carbohydrate meals, avoid liquid calories; (2) acarbose (α-glucosidase inhibitor) blunts the post-meal glucose/insulin surge; (3) diazoxide or octreotide to suppress insulin; (4) continuous glucose monitoring; (5) rarely, partial pancreatectomy for refractory nesidioblastosis.[7]
Malaria- and quinine-associated hypoglycaemia
Severe Plasmodium falciparum malaria causes hypoglycaemia by three overlapping mechanisms: (a) parasite glucose consumption, (b) impaired hepatic gluconeogenesis, and (c) quinine-stimulated β-cell insulin release.[6]
- Pregnancy is especially susceptible (hyperinsulinaemia of pregnancy + quinine sensitivity) — quinine-induced hypoglycaemia is a leading cause of death in severe malaria in pregnancy.
- Artemisinin derivatives (artesunate) cause less hypoglycaemia than quinine and are first-line.
- Treat with IV dextrose; monitor frequently; consider octreotide if quinine-driven insulin release is persistent.[6]
NICE-SUGAR trial
NICE-SUGAR (NEJM 2009)
Multicentre RCT: 6104 critically ill patients
Population: Adult ICU patients expected to stay >3 days
Key finding
Intensive control had HIGHER mortality (27.5% vs 24.9%, p=0.02). More episodes of SEVERE hypoglycaemia (<2.2 mmol/L): 6.8% vs 0.5%.
Practice change
Moderate glucose control (target 6-10 mmol/L) is preferred. Intensive control (4.4-6.1) causes more hypoglycaemia and increases mortality. Hypoglycaemia is dangerous.
The evidence base for ICU glucose control
Leuven I — Surgical ICU (2001)
van den Berghe, NEJM
- 1548 post-op surgical ICU patients; intensive insulin (4.4–6.1) vs conventional (10–11.1)
- RESULT: intensive therapy REDUCED mortality (4.6% vs 8.0%) — mainly long-stay and septic patients
- Spawned the "tight glycaemic control" era; CAVEATS: single centre, predominantly cardiac surgery, early enteral feeding
Leuven II — Medical ICU (2006)
van den Berghe, NEJM
- 1200 medical ICU patients; same targets
- RESULT: NO overall mortality benefit; fewer morbidity outcomes but more hypoglycaemia
- Suggested the surgical benefit did not generalise to medical ICU
NICE-SUGAR (2009)
Finfer, NEJM
- 6104 mixed ICU patients; intensive (4.4–6.1) vs conventional (<10)
- RESULT: intensive control INCREASED 90-day mortality (27.5% vs 24.9%) and severe hypoglycaemia 6.8% vs 0.5%
- Established the modern target: 6–10 mmol/L
Finfer 2012 — Hypoglycaemia & death
NEJM
- NICE-SUGAR cohort analysis of 6026 patients
- RESULT: severe hypoglycaemia (<2.2) independently associated with mortality (OR ≈ 1.4–2.3 dose-dependent)
- Association yes, causation not proven — hypoglycaemia marks illness severity AND may directly harm
ICU glycaemic target — synthesis
The current consensus target in most adult ICUs is glucose 6–10 mmol/L (108–180 mg/dL), avoiding both hypoglycaemia and marked hyperglycaemia (>10–12 mmol/L).[1][5]
- Avoid hypoglycaemia above all — severe hypoglycaemia (<2.2) is the strongest glucose-related predictor of death.
- Use IV insulin infusions (not sliding-scale boluses alone) for unstable patients; titrate to a written protocol with q1–2h glucose checks.
- Feeding matters: adequate enteral nutrition reduces hypoglycaemia risk on an insulin infusion; suddenly stopping feed is a classic ICU precipitant of hypoglycaemia (continue insulin briefly or reduce insulin when feed is held).
- Renal failure, liver failure, sepsis, and shock lower insulin requirement — re-titrate daily and after any change in organ support.[3]
SAQ — Severe hypoglycaemia presenting with generalised seizure in a type 1 diabetic
10 minutes · 10 marks
A 34-year-old woman with type 1 diabetes (on a basal-bolus regimen: glargine 22 units nocte, aspart 6–8 units with meals) is brought to the emergency department by ambulance after a generalised tonic-clonic seizure at home. Her partner reports she skipped dinner after a busy shift and her insulin pump was found disconnected. On arrival: GCS 9 (E2V3M4), HR 112, BP 104/68, RR 22, SpO2 97 percent on room air, afebrile, still post-ictal. Fingerprick glucose reads 'LOW' (below 1.1 mmol/L on the meter); laboratory glucose confirms 1.0 mmol/L. The team is preparing to manage her.
SAQ — Sulfonylurea overdose with recurrent hypoglycaemia in an elderly patient
10 minutes · 10 marks
A 78-year-old man with type 2 diabetes, CKD stage 4 (eGFR 22 mL/min/1.73 m2) and depression is brought in after a deliberate overdose of glibenclamide 5 mg — he has taken approximately 20 tablets (100 mg) 6 hours ago. On arrival he is drowsy (GCS 12), sweaty, and tremulous; fingerprick glucose is 1.6 mmol/L. The team gives 25 g of 50 percent dextrose IV and the glucose rises to 9.2 mmol/L, but 90 minutes later it has fallen to 1.9 mmol/L with recurrence of confusion. You are asked to take over his management.
Clinical pearls
Red flags
[3]References
- [1]The NICE-SUGAR Study Investigators; Finfer S, Chittock DR, Su SY, et al. Intensive versus conventional glucose control in critically ill patients. New England Journal of Medicine, 2009.PMID 19318384
- [2]Cryer PE. Individualized glycemic goals and an expanded classification of severe hypoglycemia in diabetes. Diabetes Care, 2017.PMID 29162584
- [3]van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients (Leuven surgical ICU trial). New England Journal of Medicine, 2001.PMID 11794168
- [4]van den Berghe G, Wilmer A, Hermans G, et al. Intensive insulin therapy in the medical ICU (Leuven medical ICU trial). New England Journal of Medicine, 2006.PMID 16452557
- [5]The NICE-SUGAR Study Investigators; Finfer S, Liu B, Chittock DR, et al. Hypoglycemia and risk of death in critically ill patients. New England Journal of Medicine, 2012.PMID 22992074
- [6]Umpierrez G, Korytkowski M. Diabetic emergencies — ketoacidosis, hyperglycaemic hyperosmolar state and hypoglycaemia. Nature Reviews Endocrinology, 2016.PMID 26893262
- [7]Lheureux PE, Zahir S, Penaloza A, Gris M. Bench-to-bedside review: Antidotal treatment of sulfonylurea-induced hypoglycaemia with octreotide. Critical Care, 2005.PMID 16356235
- [8]Seaquist ER, Anderson J, Childs B, et al. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and The Endocrine Society. Diabetes Care, 2013.PMID 23589542