ICU · Environmental emergencies
Heat Stroke & Heat Illness
Also known as Heat stroke · Heat exhaustion · Heat illness · Exertional heat stroke · Classic heat stroke · Hyperthermia · Rapid cooling
The heat stroke — the core temperature above 40 degrees C with the CNS dysfunction (the confusion, the seizure, the coma). The two types (the classic — the elderly, the drugs; the exertional — the young, the athletes). The thermoregulatory failure → the multi-organ (the CNS, the cardiac, the liver, the renal, the DIC). The RAPID cooling (the priority — the ice-water immersion the fastest; the evaporative the practical). The NOT the antipyretics (the central set-point normal). The benzodiazepine for the shivering. The mortality 10 to 50 per cent.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
The heat stroke — the core temperature above 40 degrees C with the CNS dysfunction. The thermoregulatory failure → the multi-organ (the CNS, the cardiac, the liver, the renal, the DIC). The mortality 10 to 50 per cent (the delay → the higher). The RAPID cooling the priority.[1][1]

The two types
- The classic (non-exertional) — the elderly, the comorbid, the drugs (the anticholinergics, the diuretics, the beta-blockers, the antipsychotics), the poor ventilation (the heatwave, the enclosed). The anhidrosis (the dry/hot skin).[1][2][1]
- The exertional — the young, the athletes, the military, the labourers. The exertion in the heat → the thermogenesis exceeds the dissipation. The sweating (the skin may be wet). The rhabdomyolysis more common.[1][2]
The clinical
- The hyperthermia (the core above 40).[1]
- The CNS — the confusion, the agitation, the ataxia, the seizure, the coma (the hallmark — distinguishes from the heat exhaustion).[1][1]
- The cardiovascular — the tachycardia, the hypotension, the distributive shock.[1][1]
- The multi-organ — the AKI, the liver failure (the transaminitis, the coagulopathy), the rhabdomyolysis, the DIC.[1][1]
The management — rapid cooling
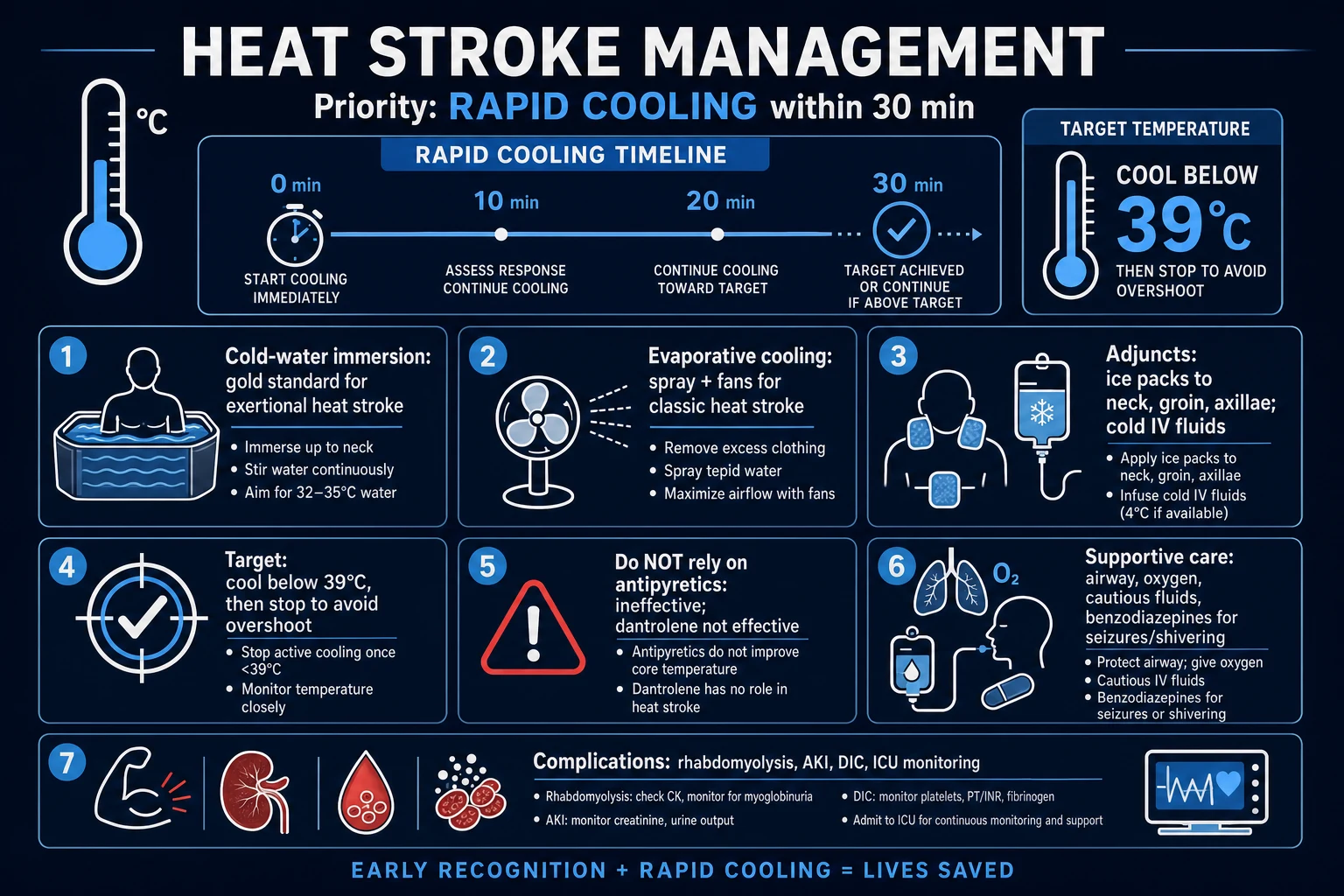
1. The rapid cooling (the priority).[1][2][1]
- The ice-water immersion (the gold standard for the exertional — the fastest cooling rate, about 0.15 degrees C/min).[1]
- The evaporative cooling (the practical ICU — the misting the body with the lukewarm the water + the continuous the fanning; about 0.1 degrees C/min).[1]
- The cold IV fluids (the 30 mL/kg the balanced the crystalloid at the 4 degrees C).[1]
- The cooling blankets (the gel pads, the Arctic Sun), the ice packs (the groin, the axillae, the neck).[1][1]
- The target: below 39 degrees C, then the stop the active (the avoid the over-shoot the hypothermia).[1]
2. The NOT the antipyretics.[1]
- The paracetamol / the NSAID the INEFFECTIVE (the central the hypothalamic the set-point is the normal in the heat stroke — the not the pyrogen-driven).[1]
- For the shivering (the shivering generates the heat — the defeats the cooling), the agitation, the seizures. The NOT the antipyretics; the NOT the dantrolene (the not the true the MH).[1][1]
- The aggressive (the shock, the dehydration, the rhabdomyolysis → the AKI). The balanced crystalloid. The titrate to the haemodynamics + the urine output.[1]
5. The multi-organ support.[1][1]
- The vasopressor (the noradrenaline) for the shock. The lung-protective ventilation if the ARDS. The renal replacement if the AKI. The correction of the electrolyte (the potassium, the phosphate). The FFP / the cryoprecipitate for the DIC.[1][1]
Prognosis
The mortality 10 to 50 per cent (the delay → the higher). The multi-organ failure (the liver, the renal, the DIC) the worse. The prompt cooling (the within 30 min → the below 39) the reduces dramatically.[1][2][1]
Red flags
The classic vs the exertional — the two types in detail
The two subtypes of the heat stroke — the same endpoint (the core above 40 + the CNS dysfunction + the multi-organ), the different the mechanism + the patient + the prognosis.[1][3][4]
The classic (the non-exertional)
The classic — the elderly, the chronic the disease (the cardiopulmonary, the renal, the diabetes, the dementia), the drugs (the anticholinergics, the diuretics, the beta-blockers, the antipsychotics, the antihistamines), the poor the ventilation / the no air-conditioning, the social isolation, the enclosed (the upstairs the apartment, the locked-in the car). The epidemic during the heatwave (the 2003 the European the heatwave — the 70,000 the dead; the 1995 the Chicago; the 2022 the Europe). The thermoregulatory the FAILURE (the impaired the dissipation) → often the anhidrosis (the dry / the hot the skin). The insidious (the days). The mortality the HIGH (the 10 to 50 per cent).[3][4][6]
The drug the list — why the elderly the vulnerable. The anticholinergics (the tricyclics, the oxybutynin, the antihistamines) the block the sweating. The diuretics the dehydrate. The beta-blockers the reduce the cardiac the output + the blunt the tachycardic the response. The antipsychotics (the phenothiazines) the impair the hypothalamic the regulation + the block the sweating. The stimulants (the MDMA, the cocaine, the amphetamines) the increase the heat the production. The alcohol the vasodilates (the heat the loss) BUT the impairs the judgement + the dehydration.[1][4]
The exertional
The exertional — the young, the fit (the athletes, the military the recruits, the miners, the firefighters, the labourers). The intense the exertion in the hot / the humid → the heat the PRODUCTION exceeds the dissipation. The sporadic (the individual). The sudden (the hours). The sweating usually the PRESENT (the profuse — the skin the wet). The rhabdomyolysis, the DIC, the AKI, the lactic the acidosis the more the severe. The mortality the LOW (the below 5 per cent) IF the rapid the cooling.[1][3][5]
The 'sweating present' the pearl. The presence of the sweating + the wet the skin does NOT the exclude the heat stroke (the common the exam the trap). The exertional the heat stroke the typically the sweaty. The classic the often the dry (the anhidrosis). The anhidrosis is NOT the required for the diagnosis — the CNS the dysfunction + the core above 40 is the required.[3][4]
The classic vs the exertional — the exam the favourite
| The feature | The classic (the non-exertional) | The exertional |
|---|---|---|
| The patient | The elderly, the chronic the disease, the psychiatric the meds | The young, the fit (the athlete, the military, the miner) |
| The context | The heatwave, the no air-conditioning, the poor the ventilation | The intense the exertion in the hot / the humid |
| The epidemiology | The EPIDEMIC (the mass during the heatwave) | The sporadic (the individual) |
| The onset | The insidious (the days) | The sudden (the hours) during / after the exertion |
| The mechanism | The impaired the DISSIPATION (the thermoregulatory the failure) | The overwhelming the PRODUCTION the greater than the dissipation |
| The sweating | The often the ABSENT (the anhidrosis — the dry) | The usually the PRESENT (the profuse — the wet) |
| The temperature | The 40 to 41 degrees C | The often the very the high (the above 42) |
| The rhabdomyolysis | The mild to moderate | The common + the SEVERE (the CK the above 10,000) |
| The DIC | The variable | The common, the early |
| The AKI | The common (the dehydration + the comorbidity) | The common (the rhabdo + the dehydration) |
| The lactic the acidosis | The variable | The severe (the exertion + the shock) |
| The hypoglycaemia | The less the common | The common (the glycogen the depletion) |
| The drugs the implicated | The anticholinergics, the diuretics, the beta-blockers, the antipsychotics | The ergogenic the aids, the stimulants (the ephedra, the MDMA) |
| The best the cooling | The evaporative (the mist + the fan) ± the ice the packs | The COLD-WATER the IMMERSION (the on-site) |
| The mortality (the treated) | The 10 to 50 per cent (the worse with the age / the comorbidity) | The below 5 per cent (with the rapid the cooling) |
The pathophysiology — the heat as the toxin
The pathophysiology — the heat as the direct the toxin + the trigger of the SIRS-like the cascade. The core above 40 degrees C → the protein the denaturation + the membrane the lipid the peroxidation → the cell the death → the systemic the inflammatory the response (the cytokine the cascade — the IL-1, the IL-6, the TNF) → the endothelial the activation + the coagulation + the complement → the multi-organ the failure (the 'sepsis from the heat').[3][7]
The cascade in the steps
- The protein the denaturation — the heat (the above 41 to 42 degrees C) the denatures the enzymes + the structural the proteins → the cell the death. The time- + the temperature-dependent (the every the minute the above 40 the worse the injury).[3][7]
- The membrane the lipid the peroxidation — the heat the damages the cell the membranes → the increased the permeability → the leak → the oedema. The direct the cytotoxicity.[7]
- The SIRS-like the response — the cytokine the cascade (the IL-1, the IL-6, the TNF-alpha) → the endothelial the activation → the NO the release → the distributive the vasodilation + the capillary the leak. The picture the indistinguishable from the septic the shock (Bouchama + Knochel 2002).[3]
- The gut the translocation — the splanchnic the ischaemia → the bacteria / the endotoxin the leak → the amplifies the inflammatory the response (the positive the feedback the 'malignant' the cycle). The heat the kills the gut the barrier.[3][7]
- The coagulation the activation — the endothelial the damage → the tissue the factor the release → the DIC (the consumption + the bleeding + the microvascular the thrombosis).[3][7]
- The multi-organ the failure — the brain (the Purkinje the cells the heat-sensitive → the cerebellar the ataxia), the liver (the centrilobular the necrosis), the kidney (the ATN from the myoglobin + the hypoperfusion), the muscle (the rhabdomyolysis), the lung (the ARDS), the heart (the myocardial the dysfunction), the coagulation (the DIC).[1][3][4]
The organ-specific the injury
- The brain — the Purkinje the cells (the cerebellum) the exquisitely the heat-sensitive → the cerebellar the ataxia (the may be the permanent). The diffuse the injury → the confusion, the coma. The cerebral the oedema. The later: the cognitive the impairment, the parkinsonism (the basal the ganglia), the seizures.[3][4]
- The liver — the centrilobular the necrosis (the zone 3) → the transaminitis (the AST / the ALT the above 1000), the coagulopathy (the impaired the synthesis), the jaundice. The usually the recovers if the patient the survives.[3]
- The kidney — the ATN from the myoglobin (the pigment the nephropathy) + the hypoperfusion (the pre-renal) + the DIC (the microvascular). The rhabdomyolysis the particularly the nephrotoxic.[1][7]
- The muscle — the rhabdomyolysis → the CK the high (the above 10,000 in the exertional), the myoglobinuria (the dipstick the blood the positive + the no the RBCs), the hyperkalaemia, the hypocalcaemia (the early — do NOT the treat unless the symptomatic), the phosphate the high.[1][7]
- The coagulation — the DIC → the PT / the aPTT the prolonged, the fibrinogen the low, the D-dimer the high, the platelets the low. The bleeding AND the thrombosis.[3]
- The lung — the ARDS (the direct the heat the injury + the aspiration + the transfusion if the massive the transfusion).[1][1]
- The heart — the myocardial the dysfunction (the stunned the myocardium), the tachycardia, the distributive the shock.[1][1]
The cooling methods in detail
The rapid the cooling — the #1 the priority. The target the below 39 degrees C as the fast as the possible (the every the minute the above 40 → the irreversible the protein the denaturation). The cooling the rate the target the at least 0.15 degrees C / the min. The do NOT the delay for the tests / the transport — the start at the point of the collapse.[1][3][5]
The cooling methods compared — the rate + the indication
| The method | The cooling the rate | The best for | The practical the notes |
|---|---|---|---|
| The cold-water the immersion (CWI) 2 to 15 degrees C | The FASTEST — 0.15 to 0.20 degrees C / min | The EXERTIONAL (the gold the standard) | The on-site / the tub; the reduces the mortality the 50 per cent to the below 5 per cent; the remove at 38.5 to 39 degrees C |
| The evaporative (the warm the mist + the fan) | ~0.1 degrees C / min | The CLASSIC / the hospital (the ICU) | The practical; the warm the water (the 15 to 25 degrees C) the mist — the NOT the ice the water (the vasoconstriction) + the continuous the fan |
| The ice the packs (the groin / the axilla / the neck) | ~0.05 degrees C / min | The adjunct / the no the other the method | The slow the alone; the rotate the sites; the better with the massage |
| The cold the IV the crystalloid (4 degrees C) | ~1 to 1.5 degrees C per 2 L | The adjunct / the dehydrated | The 4 degrees C the saline the 30 mL / kg; the never the sole the method; the cool if the shocked |
| The intragastric / the bladder the lavage | The adjunct | The refractory | The cool the saline the lavage via the NG / the urinary the catheter |
| The peritoneal the lavage | The moderate to fast | The refractory | The cool the dialysate; the invasive |
| The intravascular the catheter (the closed the loop) | The fast | The ICU (if the available) | The heat the exchange; the precise the temp the control |
| The ECMO (VA) | — | The cardiac the arrest / the severe the shock | The last the resort — the supports the circulation while the cooling |
The cold-water the immersion (CWI) — the gold the standard for the exertional
The CWI — the definitive the on-site the treatment for the exertional. The ice the bath / the tub at the 2 to 15 degrees C. The FASTEST the cooling (~0.15 to 0.20 degrees C / the min). The reduces the mortality from the ~50 per cent to the below 5 per cent. The large the athletic the surveillance → the 100 per cent the survival when the started the promptly (Casa 2015 NATA). The mantra: the 'cool the first, the transport the second' — the cool to the below 38.6 degrees C (101.5 F) before the moving the athlete.[5]
The technique. The immerse the athlete up to the neck / the shoulders in the tub of the ice the water. The stir the water (the maintains the convection). The monitor the core the temp the continuously. The REMOVE at the 38.5 to 39 degrees C to the avoid the overshoot. The myth the busted: the 'the CWI the causes the dangerous the vasoconstriction / the afterdrop' — the in the practice the high the thermal the gradient the overwhelms the vasoconstriction + the CWI the demonstrably the fastest the method.[3][5]
The evaporative the cooling — the practical the ICU the method
The evaporative — the spray the WARM / the TEPID the water the mist (the 15 to 25 degrees C) over the maximally the exposed the skin + the continuous the high-flow the fan. The WHY the warm the mist, the not the ice the water: the ice the water the causes the cutaneous the VASOCONSTRICTION → the shunts the blood the away from the skin → the REDUCES the heat the loss → the paradoxically the slows the cooling. The tepid the water the keeps the cutaneous the vessels the dilated → the sweat / the evaporation the removes the heat the efficiently. The rate ~0.1 degrees C / the min — the slightly the slower than the CWI BUT the practical in the ED / the ICU for the classic the heat stroke (the elderly, the can't the immerse). The combine with the ice the packs to the groin / the axilla / the neck + the cold the IV the fluids. The maximise the skin the exposure (the remove all the clothing) + the continuous the airflow.[1][1][4]
The ice the packs + the cold the IV the fluids
The ice the packs — to the groin, the axilla, the neck (the high-flow the vascular the areas). The slow the alone (~0.05 degrees C / the min) — the rotate the sites; the better with the massage. The adjunct the not the sole. The cold the IV the fluids — the 4 degrees C the saline the 30 mL / kg; the cools the ~1 to 1.5 degrees C per 2 L; the doubles as the resuscitation; the never the sole the method.[1][1]
The complications — the multi-organ
The complications — the 'sepsis from the heat' the multi-organ. The check + the treat the each.[1][3][7]
- The rhabdomyolysis — the CK the high (the above 10,000 in the exertional), the myoglobinuria (the dipstick the blood the positive + the no the RBCs). The AGGRESSIVE the IV the fluids (the target the urine the output the 200 to 300 mL / the hr the once the perfusion the restored). The monitor the potassium (the hyperkalaemia — the cardiac the arrest), the calcium (the early the hypo — the do NOT the treat unless the symptomatic), the phosphate. The consider the RRT if the refractory the hyperkalaemia / the acidosis / the fluid the overload.[1][7]
- The DIC — the monitor the PT / the INR / the aPTT / the fibrinogen / the D-dimer / the platelets. The transfuse the platelets / the FFP / the cryoprecipitate if the bleeding or the before the procedures. The heparin the generally the NOT the indicated (the consumption, the not the thrombosis — the unless the thrombosis the dominates).[3]
- The ARDS — the lung-protective the ventilation (the VT the 6 mL / kg the PBW, the plateau the below 30 cmH2O, the PEEP the titrated).[1][1]
- The AKI — the pre-renal (the dehydration) + the intrinsic (the ATN from the myoglobin / the hypoperfusion) + the pigment. The fluids; the RRT if the refractory.[1][1]
- The hepatic the necrosis — the centrilobular (the zone 3). The transaminitis (the above 1000). The usually the recovers if the patient the survives. The do NOT the give the paracetamol (the worsens).[3]
- The cardiac — the myocardial the dysfunction, the arrhythmias (the electrolyte, the acidosis). The noradrenaline for the shock; the correct the potassium / the magnesium.[1][1]
The NOT the antipyretics — why
The antipyretics (the paracetamol / the NSAID) the INEFFECTIVE + the potentially the harmful. The KEY the concept: the heat-stroke the hyperthermia is the NOT the fever. The in the fever, the hypothalamic the set-point is the RAISED by the prostaglandins (the PGE2) → the antipyretics (the paracetamol = the COX the inhibitor, the NSAID = the COX the inhibitor) the lower the set-point → the reduce the temperature. The in the heat stroke, the set-point is the NORMAL — the body is the simply the OVERWHELMED by the external / the exertional the heat the gain the exceeds the dissipation. The therefore the paracetamol / the NSAID the CANNOT the reduce the temperature (the no the abnormal the prostaglandin the signal to the block).[1][3][4]
The harm. The paracetamol the worsens the already-injured the liver (the hepatocyte the necrosis the hallmark). The NSAID the worsens the AKI + the bleeding the risk (the DIC). The do NOT the wait for the antipyretics — the start the external the cooling the immediately. The exam the pearl: 'the patient with the heat stroke the given the paracetamol — the no the response' → the confirms the set-point the normal; the switch to the physical the cooling.[1][4]
The dantrolene — the also the ineffective
The dantrolene the INEFFECTIVE — the heat stroke is the NOT the malignant the hyperthermia (the no the ryanodine-the-receptor the Ca2+ the leak in the skeletal the muscle). The randomised the trials the show the NO the benefit (the no the faster the cooling, the no the mortality the reduction). The do NOT the give (the wastes the time, the risk of the hepatotoxicity + the muscle the weakness). The exception the nuance: the dantrolene the occasionally the discussed if the concomitant the MH the suspected (the post-the-anaesthetic) BUT the do NOT the routine.[1][4]
The heat stroke vs the other the hyperthermia (the differential)
| The feature | The heat stroke | The malignant the hyperthermia (MH) | The neuroleptic the malignant (NMS) | The serotonin the syndrome | The sepsis (with the fever) |
|---|---|---|---|---|---|
| The trigger | The heat / the exertion | The volatile the anaesthetics / the suxamethonium | The antipsychotics (the dopamine the blockade) | The serotonergic the drugs | The infection |
| The onset | The minutes to hours | The minutes to hours (the intra-op) | The days to weeks | The hours (after the drug / the dose up) | The hours to days |
| The set-point | The NORMAL | The normal | The normal | The normal | The RAISED (the fever — the PGE2) |
| The temp | The above 40 | The rapid the rise the above 40 | The 38 to 41 | The usually the below 41 | The 38 to 41 (the fever) |
| The muscle | The rhabdomyolysis | The sustained the rigidity (the 'rigor') | The lead-the-pipe the rigidity | The clonus, the hyperreflexia | The variable |
| The sweating | The exertional: yes; the classic: no | The profuse | The variable | The diaphoresis | The variable |
| The antipyretics | The INEFFECTIVE | The ineffective | The ineffective | The ineffective | The EFFECTIVE (the reduces the fever) |
| The dantrolene | The INEFFECTIVE | The DEFINITIVE the cure | The may the help (the adjunct) | The not the indicated | The not the indicated |
| The treatment | The RAPID the COOLING | The dantrolene + the stop the trigger | The stop the drug, the cooling, the bromocriptine / the dantrolene | The stop the drug, the cyproheptadine, the benzodiazepine | The antibiotics + the source the control |
The management — the step-by-step
The management of the acute heat stroke
-
THE RECOGNISE — the core the above 40 + the CNS the dysfunction = the HEAT STROKE — (a) The DIAGNOSIS (the triad): (i) the CORE the TEMPERATURE the above 40 (the use the rectal / the oesophageal / the bladder — the NOT the oral / the tympanic — the inaccurate at the extremes; the low-reading the thermometer the may the needed). (ii) The CNS the DYSFUNCTION — the confusion, the agitation, the delirium, the ataxia (the cerebellar), the seizure, the coma (the hot + the confused = the heat stroke the until the proven the otherwise). (iii) The HOT the skin — the exertional the often the WET (the sweating the persists); the classic the often the DRY (the anhidrosis). (b) The SUBTYPE: the EXERTIONAL (the young, the fit, the exertion) vs the CLASSIC (the elderly, the chronic, the heatwave, the anticholinergics). (c) The EXCLUDE the differentials: the sepsis (the bloods / the cultures / the lactate — the heat stroke the RESEMBLES the sepsis BUT the no the obvious the source), the MH (the anaesthetic the history), the NMS (the antipsychotic), the serotonin the syndrome (the serotonergic), the thyroid the storm, the neuroleptic, the stimulant the toxicity.[1][3][4]
-
THE RAPID THE COOLING — the #1 the PRIORITY (the start IMMEDIATELY, the do NOT the delay for the tests / the transport) — (a) The PRINCIPLE: the every the minute the above 40 → the irreversible the PROTEIN the DENATURATION + the cell the death → the FASTER the cool, the better the outcome. The target: the reduce the core to the below 39 the within the 30 to 60 the min. The rate the target the at least 0.15 degrees C / the min. (b) The GOLD the STANDARD for the EXERTIONAL: the COLD-WATER the IMMERSION (CWI) — the ice the bath / the tub at the 2 to 15 degrees C. (i) The FASTEST (~0.15 to 0.20 degrees C / the min) + the REDUCES the MORTALITY the ~50 per cent to the below 5 per cent. (ii) The START the ON-SITE — the 'cool the first, the transport the second' (Casa 2015 NATA: the cool to the below 38.6 the before the moving). (iii) The REMOVE at the 38.5 to 39 to the avoid the overshoot. (c) For the CLASSIC / the ICU: the EVAPORATIVE (the warm the mist + the fan) — the spray the tepid (the 15 to 25 degrees C) the mist + the continuous the high-flow the fan; the WHY the warm (the not the ice): the ice → the vasoconstriction → the slows the cooling. (d) The ADJUNCT: the ice the packs (the groin / the axilla / the neck) + the cold the IV the fluids (4 degrees C the saline the 30 mL / kg). (e) The STOP at the 38.5 to 39 — the overshoot the hypothermia → the arrhythmia / the coagulopathy / the shivering. (f) The CONTROL the shivering (the generates the heat) — the counter-warming the extremities + the benzodiazepine (the midazolam) / the paralysis if the intubated + the severe.[1][3][5]
-
THE AIRWAY + THE BREATHING + THE CIRCULATION (the supportive) — (a) The AIRWAY: the reduced the consciousness / the coma → the intubate (the RSI — the beware the heat-related the hypotension; the ketamine / the etomidate the cautiously; the avoid the propofol in the profound the shock). The seizure → the secure the airway. (b) The BREATHING: the oxygen for the hypoxaemia; the if the ARDS → the lung-protective (the VT the 6 mL / kg, the plateau the below 30, the PEEP). (c) The CIRCULATION: the heat stroke → the volume the depletion (the sweating / the insensible) + the vasodilation + the myocardial the dysfunction → the hypotension. (i) The IV the FLUIDS — the cool the balanced the crystalloid (the doubles as the cooling); the titrate to the MAP the above 65 + the urine the output the above 0.5 mL / kg / the hr; the avoid the over-the-resuscitation (the pulmonary the oedema). (ii) The VASOPRESSORS (the noradrenaline) if the refractory the shock.[1][1][1]
-
THE TREAT the COMPLICATIONS (the 'sepsis from the heat') — (a) The RHABDOMYOLYSIS: the check the CK (the above 10,000), the urine the myoglobin (the dipstick the blood + the no the RBCs). The AGGRESSIVE the IV the fluids (the target the UO the 200 to 300 mL / the hr). The monitor the K+, the Ca2+ (the early the hypo — the do NOT the treat unless the symptomatic), the phosphate. The RRT if the refractory. (b) The DIC: the monitor the PT / the aPTT / the fibrinogen / the D-dimer / the platelets; the transfuse the platelets / the FFP / the cryoprecipitate if the bleeding; the heparin the generally the NOT. (c) The AKI: the fluids; the RRT. (d) The hepatic: the monitor the LFTs; the avoid the paracetamol. (e) The GLUCOSE: the check (the hypoglycaemia the common in the exertional — the glycogen the depletion). (f) The SEIZURES: the benzodiazepine (the lorazepam / the diazepam). (g) The VTE the prophylaxis (the immobilised).[1][1][7]
-
THE NOT TO DO (the common the dangerous the errors) — (a) The ANTIPYRETICS (the paracetamol / the NSAID) the INEFFECTIVE + the harmful: the set-point the normal; the paracetamol the worsens the liver; the NSAID the worsens the AKI + the bleeding. (b) The DANTROLENE the INEFFECTIVE: the NOT the MH. (c) The do NOT the DELAY the cooling for the transport / the investigations. (d) The do NOT the use the ice the water the mist for the evaporative (the vasoconstriction). (e) The do NOT the cool the below 38.5 (the overshoot the hypothermia). (f) The do NOT the forget the shivering the control (the generates the heat).[1][3][4]
-
THE PREVENTION (the population the intervention) — (a) The HEATWAVE the PLANNING (the classic): the early the warning, the cooling the centres, the check on the elderly / the vulnerable, the ensure the hydration + the air-conditioning, the reduce the anticholinergic / the diuretic the burden during the heatwaves. (b) The EXERTIONAL the prevention: the ACCLIMATISATION (the 7 to 14 the days the graded the heat the exposure → the up the plasma the volume, the up the sweat the rate, the down the sweat the sodium), the hydration (the beware the exertional the hyponatraemia), the schedule the exercise for the cooler the hours, the WBGT (the wet-the-bulb the globe the temperature) the monitoring, the cooling the stations, the gradual the intensity, the identify the high-the-risk (the sickle-the-cell the trait, the stimulant, the illness). (c) The DRUG the review: the stop / the reduce the anticholinergics, the diuretics, the antipsychotics in the elderly during the heatwaves.[1][3][5]
SAQ — Exertional heat stroke with rhabdomyolysis in a military recruit
10 minutes · 10 marks
A 22-year-old male military recruit collapses 8 km into a timed pack march on a humid summer day (wet-bulb globe temperature 31 degrees C). On arrival at the medical tent his core (rectal) temperature is 41.8 degrees C, GCS 12 (confused and combative), HR 152, BP 86/48, RR 34, SpO2 92 percent on room air. He is profusely diaphoretic with hot, wet skin and is trembling with rigors. Initial bloods: sodium 148, potassium 6.8, creatinine 180 (baseline 85), CK 28,400 IU/L, venous pH 7.18, lactate 7.2, INR 2.4, platelets 86, creatine kinase markedly elevated. Urine is dark tea-coloured and dipstick blood-positive with no red cells on microscopy. An ice-water immersion tub is available on-site.
SAQ — Classic (non-exertional) heat stroke in an elderly woman during a heatwave
10 minutes · 10 marks
An 82-year-old woman with dementia, hypertension and chronic kidney disease is brought by ambulance from her un-air-conditioned top-floor apartment during the third day of a city heatwave (ambient 43 degrees C). She was found unresponsive by a neighbour. On arrival: core (rectal) temperature 41.2 degrees C, GCS 8 (E2V2M4), HR 118 sinus, BP 82/46 (MAP 58), RR 28, SpO2 94 percent on room air. Her skin is hot and strikingly DRY (anhidrotic). Medications brought in by the family include furosemide 40 mg daily, amitriptyline 25 mg nocte, and temazepam. Bloods: sodium 156, creatinine 240 (baseline 120), lactate 4.6, INR 1.9, platelets 92, ALT 380. She has not urinated for the ambulance journey. The emergency department has no immersion tub but does have a cooling blanket, fans, and a high-flow misting device.
The clinical pearls
The additional the red flags
The landmark the trials + the guidelines
Casa 2015 — NATA the position the statement: the exertional the heat the illness (PMID 26381473)
Source
Journal of Athletic Training — the National Athletic Trainers' Association the position the statement
Authors
Casa DJ, DeMartini JK, Bergeron MF, et al.
Scope
The prevention, the recognition + the management of the exertional the heat the illness (the cramps, the exhaustion, the stroke)
The key the recommendation
The COLD-WATER the IMMERSION the definitive the on-site for the exertional the heat the stroke — the 'the cool the first, the transport the second'
The evidence
The large the athletic-the-programme the surveillance → the 100 per cent the survival when the CWI the started the promptly; the mortality the ~50 per cent to the below 5 per cent
The cooling the rate
The CWI ~0.15 to 0.20 degrees C / the min — the fastest the available
The clinical the bottom the line
The single the most the important the paper for the exertional the heat the stroke — the immediate the CWI the before the transport
Argaud 2007 — the Lyon 2003 the heatwave the cohort (PMID 17698677)
Source
Archives of Internal Medicine — the prospective the cohort
Authors
Argaud L, Ferry T, Le QH, et al.
Population
83 the patients with the classic (the non-the-exertional) the heat the stroke the admitted during the August 2003 the French the heatwave
28-day mortality
58 per cent
2-year mortality
71 per cent
Independent the predictors
The institutional the admission (HR 1.98), the antihypertensive (HR 2.17), the anuria (HR 5.24), the coma (HR 2.95), the cardiovascular the failure (HR 2.43)
The functional
The survivors the dramatic the functional the decline at the 1 + the 2 the years
The clinical the bottom the line
The classic the heat the stroke the NOT the benign — the very the poor the short- + the long-the-term; the aggressive + the honest the prognostication
Bouchama + Knochel 2002 — the Heat Stroke (NEJM) (PMID 12075060)
Source
New England Journal of Medicine — the definitive the review
Authors
Bouchama A, Knochel JP
The definition
The core the above 40 + the CNS the dysfunction + the multi-organ
The pathophysiology
The systemic the inflammatory the response the INDISTINGUISHABLE from the sepsis — the cytokine, the endothelial, the coagulation
The management
The RAPID the COOLING the definitive; the antipyretics + the dantrolene the ineffective
The mortality
The classic the 10 to 50 per cent; the exertional the below 5 per cent with the rapid the cooling
The clinical the bottom the line
The foundational the modern the reference — the heat stroke the 'the sepsis the from the heat'
Epstein + Yanovich 2019 — the Heatstroke (NEJM) (PMID 31216400)
Source
New England Journal of Medicine — the current-the-concepts the review
Authors
Epstein Y, Yanovich R
The scope
The updated the pathophysiology + the management of the classic + the exertional
The key the update
The reaffirms the rapid the physical the cooling; the antipyretics / the dantrolene the NO the benefit; the dantrolene the RCTs the negative
The subtype
The classic (the elderly, the drugs, the heatwave) vs the exertional (the young, the fit) — the different the mechanism, the same the endpoint
The clinical the bottom the line
The modern the companion the to the Bouchama 2002 — the same the message the reaffirmed
Leon + Bouchama 2015 — the Heat Stroke (Comprehensive Physiology) (PMID 25880507)
Source
Comprehensive Physiology — the mechanistic the review
Authors
Leon LR, Bouchama A
The scope
The detailed the molecular the pathophysiology — the heat the cytotoxicity, the SIRS, the organ the injury
The key the mechanism
The protein the denaturation (the above 41 to 42) + the lipid the peroxidation + the gut the translocation → the SIRS the indistinguishable the from the sepsis
The organ the injury
The brain (the Purkinje), the liver (the centrilobular), the kidney (the ATN), the muscle (the rhabdo), the coagulation (the DIC)
The clinical the bottom the line
The mechanistic the underpinning for the 'the sepsis the from the heat' + the multi-organ the management
The prognosis — the summary
The mortality the 10 to 50 per cent (the classic — the worse with the age / the comorbidity / the delay); the below 5 per cent the exertional with the rapid the cooling. The poor-the-prognosis the features: the prolonged the hyperthermia (the above 40 the for the above 1 to 2 the hr), the coma, the shock, the DIC, the AKI, the severe the acidosis, the elevated the lactate, the transaminitis the above 1000. The neurological the sequelae: the cerebellar the ataxia (the Purkinje — the permanent), the cognitive the impairment, the parkinsonism, the seizure — the may the persist the despite the full the systemic the recovery. The prompt the cooling (the within the 30 the min → the below 39) the reduces the dramatically.[1][3][6]
References
- [1]Lipman GS, et al. Management of Heat-Related Illness and Injury in the ICU: A Concise Definitive Review Crit Care Med, 2024.PMID 38240487
- [2]Pryor RR, et al. Heat-Related Illnesses Ann Intern Med, 2025.PMID 40569698
- [3]Bouchama A, Knochel JP Heat stroke N Engl J Med, 2002.PMID 12075060
- [4]Epstein Y, Yanovich R Heatstroke N Engl J Med, 2019.PMID 31216400
- [5]Casa DJ, et al. National Athletic Trainers' Association Position Statement: Exertional Heat Illnesses J Athl Train, 2015.PMID 26381473
- [6]Argaud L, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France Arch Intern Med, 2007.PMID 17698677
- [7]Leon LR, Bouchama A Heat stroke Compr Physiol, 2015.PMID 25880507