ICU · Environmental emergencies
Accidental Hypothermia
Also known as Hypothermia · Accidental hypothermia · Osborn waves · J waves · Rewarming · ECMO hypothermia · Not dead until warm and dead
The accidental hypothermia — the core below 35 degrees C. The severity (the mild 32 to 35, the moderate 28 to 32, the severe below 28). The clinical (the shivering → the bradycardia, the decreased the LOC, the loss of shivering, the Osborn / J waves, the VF / the asystole). The rewarming (the passive, the active the external, the active the internal — the ECMO for the severe). The handle gently (the cold heart irritable). The NOT the dead until the warm and the dead. The drugs the extended intervals (the below 30).
On this page & tools
Your progress
Saved locally on this device.
Target exams
Overview & definition
The accidental hypothermia — the core temperature below 35 degrees C. The mortality the high in the severe (the cardiac arrest from the VF / the asystole). The key principles: the handle gently (the cold heart is irritable — the VF from the rough handling), the rewarm (the method by the severity), and the not dead until warm and dead (the continue the CPR until the core the above 32 degrees C).[1][1]

The severity and the clinical
| Severity | Core temp | Clinical |
|---|---|---|
| Mild | 32-35 C | Tachycardia, tachypnoea, shivering, impaired judgment, ataxia |
| Moderate | 28-32 C | Bradycardia, decreased respiratory rate, decreased LOC, loss of shivering, AF, J waves |
| Severe | Below 28 C | Coma, fixed/dilated pupils, areflexia, severe bradycardia, VF, asystole, pulseless |
- The bradycardia, the prolonged PR/QT.[1]
- The Osborn / J waves (the junctional hump at the J point — the characteristic of the hypothermia; the size correlates with the severity).[1][1]
- The AF (the common), the VT, the VF (the below 28).[1]
The rewarming
1. Passive rewarming (the mild: 32 to 35).[1][1]
- The blankets, the warm the room, the warm fluids. The allows the endogenous the heat the production (the shivering). The rate the 0.5 to the 1 degree C/h.[1]
2. Active external rewarming (the moderate: 28 to 32).[1][1]
- The forced the warm the air (the Bair the Hugger), the radiant, the warm the blankets, the warming the mattresses. The rate the 1 to the 2 degrees C/h.[1][1]
3. Active internal / core rewarming (the severe: below 28).[1][1][1]
- The warmed IV the fluids (the 40 degrees C). The warmed the humidified the gases. The body cavity the lavage (the gastric, the bladder, the peritoneal, the pleural).[1]
- The ECMO (the most effective — the for the severe with the cardiac the arrest; the full the cardiopulmonary the bypass the alternative). The rate the 2 to the 4 degrees C/h.[1][1]
The key principles
- The handle gently. The cold heart is extremely irritable — the rough handling (the moving, the intubating, the chest the compressions) can precipitate the VF. The gentle the transfer, the minimal the manipulation.[1][1]
- The NOT the dead until the warm and the dead. The continue the CPR (if the pulseless) until the core the above 32 degrees C. The cold brain is the protected (the low the metabolic the rate → the delayed the anoxic the injury). The long the CPR the required (the hours).[1][1]
- The drugs. The below 30 degrees C → the drugs the metabolise the poorly (the adrenaline, the amiodarone — the ineffective; the NOT the give if the below 30). The above 30 → the standard the but the extended the intervals (the double). The above 35 → the standard.[1]
- The after-drop. The core continues the fall the initially the during the rewarming (the peripheral the vasodilation → the cold the blood the returns). The anticipate; the not the panic.[1][1]
- The potassium. The very high the potassium (the above 10 mmol/L) is the poor the prognostic (the pre-terminal the cellular the death → the NOT the continue the CPR).[1]
Prognosis
The mortality the high in the severe (the VF / the asystole). The ECMO rewarming the improved the survival (the 50 to the 80 per cent in the some the series). The potassium the above the 10, the asystole, the prolonged the CPR the → the worse.[1][1][1]
Red flags
Pathophysiology & thermoregulation
The body defends a narrow core temperature (about 37 °C) by balancing heat production against heat loss. Heat is produced by basal metabolism, voluntary activity, postural muscle tone, and — when the core falls — the two thermogenic mechanisms: shivering thermogenesis (rapid, ATP-driven skeletal-muscle contraction, generates heat without useful work) and non-shivering thermogenesis (predominantly brown-fat β-adrenergic oxidation, significant in infants and limited in adults). Cold exposure overwhelms these defences → the core falls → progressive, predictable organ dysfunction, the pattern of which is the basis of clinical staging.[2][4]
Three principles dominate the physiology and the exam answer: (1) the CNS is protected by the cold — cerebral metabolic rate falls ~6–7% per °C, so anoxia is tolerated far longer than in normothermia, the rationale for "not dead until warm and dead"; (2) the cold myocardium is electrically irritable — re-entry, automaticity and conduction slowing predispose to AF and, below 28 °C, VF, precipitated by rough handling; (3) enzyme and membrane function are temperature-dependent — drug clearance collapses, the coagulation cascade slows (cold coagulopathy), and the oxyhaemoglobin dissociation curve shifts left (impaired tissue O2 unloading).[2][4]
Mechanisms of heat loss — how the cold environment strips body heat
| Mechanism | Detail | Typical contribution | Clinical / management relevance |
|---|---|---|---|
| Radiation | Infrared emission from exposed skin to a cooler surrounding surface | Up to 50–60% in a still, cold room | The dominant route in still air; bare skin + cold walls/night sky = rapid loss. Insulate and cover the head |
| Convection | Moving air or water carries the warm boundary layer away, replacing it with cold | High in wind; immersion (water conducts ~25× faster than air) | Immersion hypothermia develops far faster than air exposure — minutes vs hours |
| Conduction | Direct transfer to a cooler surface in contact (ground, wet mattress, cold water) | Marked on cold ground or in cold water | Remove from ground, strip wet clothing, insulate beneath the patient |
| Evaporation | Latent heat of vaporisation from wet skin, sweat, and wet clothing | Marked in wet, windy conditions | Ethanol vasodilatation + wet clothing = evaporative loss; the classic "found collapsed outside the pub" scenario |
| Respiration | Warming and humidifying cold inspired air, lost on exhalation | ~10% baseline, more in cold dry air | Warmed, humidified inspired gases on the ventilator address this directly |
| Behavioural loss | Impaired judgement (cold, alcohol, drugs) prevents the patient seeking shelter | Major contributor in the confused/ intoxicated patient | Underlies the high incidence in alcohol intoxication and the elderly with dementia |
Thermoregulatory response to cold — the staged defence
| Core temperature | Thermoregulatory response | Net effect |
|---|---|---|
| 36–35 °C | Peripheral vasoconstriction (sympathetic) → shunts blood to the core; shivering begins | Heat conserved and generated; conscious patient feels cold and seeks warmth |
| 35–32 °C | Maximal shivering (can raise metabolic rate 2–5×); tachycardia, tachypnoea, piloerection | Endogenous heat production maximised — the window where passive rewarming (allowing shivering) can work |
| Below 32 °C | Shivering is lost below ~30–32 °C → the patient can no longer self-rewarm | Passive rewarming now fails; active external rewarming required |
| Below 28 °C | Thermoregulation abolished; metabolic rate plummets | Active internal/core rewarming mandatory |
Pathophysiological cascade of progressive hypothermia
Heat loss exceeds production
Cold exposure (or impaired thermogenesis) overwhelms shivering and vasoconstriction. Core temperature begins to fall.
CNS depression
Cerebral metabolic rate falls ~6–7% per °C. Consciousness, judgement, and then reflexes are progressively lost. Below ~30 °C the patient is comatose; pupils dilate and may become fixed — the patient appears dead though the brain is protected.
Cardiovascular irritability
Conduction slows (PR, QRS, QT prolong), pacemakers destabilise → bradycardia (resistant to atropine — the sinus node is intrinsically slowed, not vagally blocked) → atrial fibrillation (common below 33 °C) → VF (below 28 °C). The cold myocardium is exquisitely irritable: rough handling precipitates VF.
Respiratory depression
Minute ventilation falls, cough and gag reflexes are lost → hypoventilation, atelectasis, aspiration risk. Bronchorrhoea and a cold-induced ARDS-like picture may follow rewarming.
Renal — cold diuresis
Peripheral vasoconstriction centralises blood volume → the kidney "sees" volume overload → a cold-induced natriuresis and diuresis → progressive intravascular volume depletion, compounded by fluid sequestration on rewarming.
Metabolic / enzyme failure
Enzyme activity collapses (Q10 effect): insulin secretion falls and tissue sensitivity falls → hyperglycaemia; drug clearance collapses (see drug section); the coagulation cascade slows → cold coagulopathy; the oxyhaemoglobin curve shifts left → impaired tissue O2 delivery (masked hypoxia).
Cellular and terminal failure
Membrane Na+/K+ ATPase fails → intracellular Na+ and water accumulation, K+ efflux → cell swelling and hyperkalaemia. A serum K+ above 8–10 mmol/L signals pre-terminal cellular death and membrane failure — a marker of asphyxia/prolonged anoxia rather than hypothermia itself.
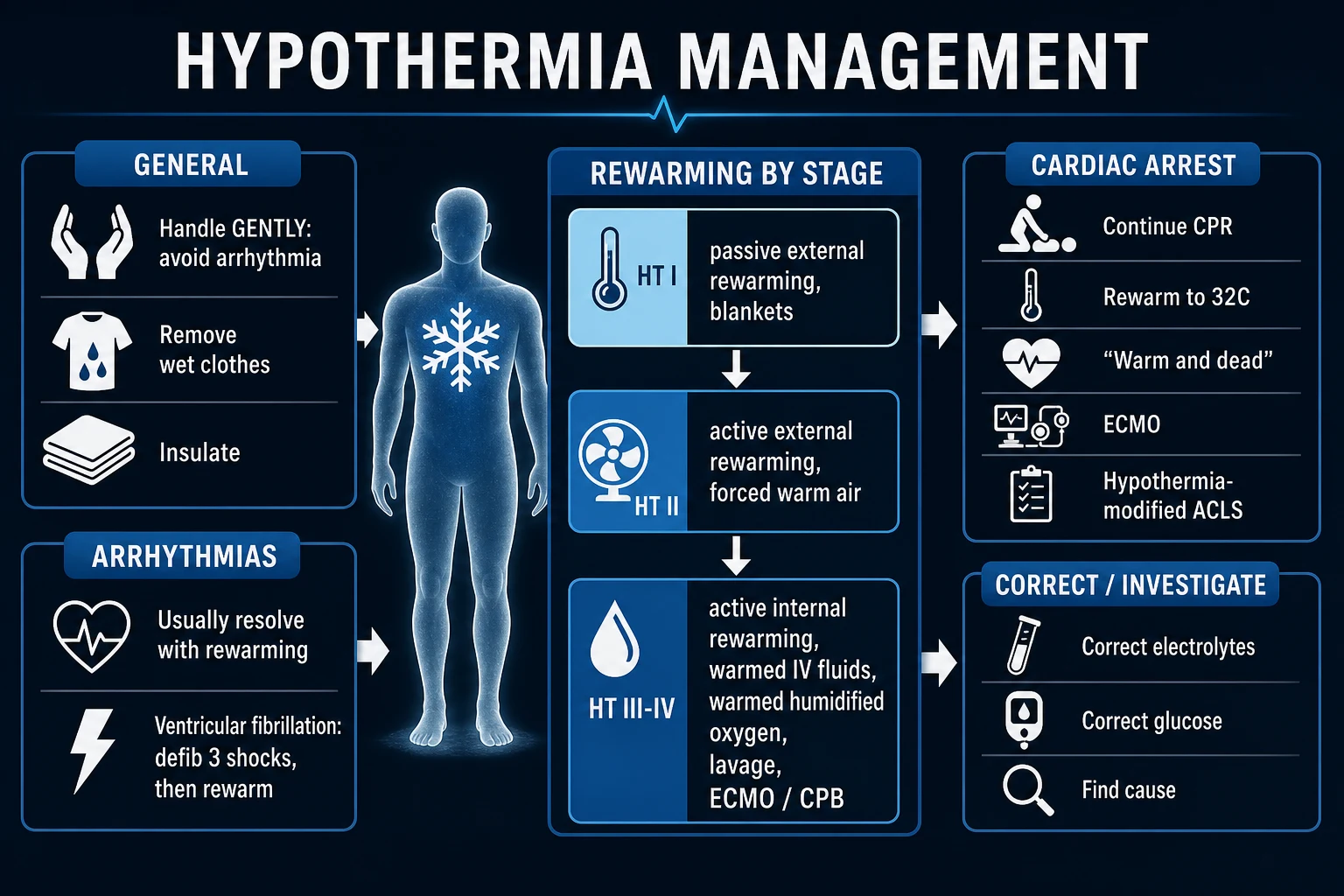
Swiss staging system (HT I–IV)
When a reliable core temperature cannot be obtained (prehospital, remote), the Swiss staging system stages hypothermia by the clinical signs alone. It is the staging promoted in the Brown NEJM review and adopted by the European Resuscitation Council and Wilderness Medical Society, and is a high-yield exam item.[2][5]
Swiss staging (Durrer) vs core-temperature classification — two systems, map them
| Swiss stage | Clinical state | Approximate core temp | Equivalent severity grade |
|---|---|---|---|
| HT I | Conscious, shivering | 35–32 °C | Mild |
| HT II | Impaired consciousness, not shivering | 32–28 °C | Moderate |
| HT III | Unconscious, vital signs present (may have atrial fibrillation) | 28–24 °C | Severe |
| HT IV | Unconscious, no vital signs (apparent death) — but not in cardiac arrest on ECLS | Below 24 °C | Profound / severe |
| HT V | Death — irreversible cardiac arrest (on ECLS with rising K+ / failing to rewarm) | — | — |
Severity by organ system — the full clinical picture at each grade
| System | Mild (32–35 °C) | Moderate (28–32 °C) | Severe (below 28 °C) |
|---|---|---|---|
| CNS | Impaired judgement, apathy, ataxia, dysarthria | Decreased LOC, drowsy → obtunded, shivering lost | Coma, areflexia, fixed/dilated pupils (brain protected — reversible) |
| Cardiovascular | Tachycardia, then relative bradycardia | Bradycardia, atrial fibrillation, Osborn J waves, hypotension | Severe bradycardia (resistant to atropine), VF, asystole, pulseless electrical activity |
| Respiratory | Tachypnoea | Bradypnoea, hypoventilation | Apnoea, loss of protective reflexes → aspiration risk |
| Metabolic | Shivering-driven hypermetabolism | Hyperglycaemia, cold diuresis → volume depletion | Enzyme failure, insulin resistance, hyperkalaemia (pre-terminal if high) |
| Coagulation | Minimal change | PT/APTT prolonged (cold coagulopathy, in-vitro artefact if sample cold) | Coagulopathy, DIC, bleeding with rewarming |
Causes & predisposition
Not every cold patient is simply cold — hypothermia is frequently secondary to an underlying disorder that impairs thermogenesis or thermoregulation. Always seek and correct the precipitant (sepsis, hypothyroidism, hypoglycaemia, intoxication).[2][4]
Primary (environmental) vs secondary (impaired thermogenesis) hypothermia
| Feature | Primary (environmental / accidental) | Secondary (impaired heat production / regulation) |
|---|---|---|
| Mechanism | Overwhelming cold exposure overwhelms normal thermoregulation | Normal thermoregulation is disabled or overwhelmed by a disease/drug |
| Typical context | Wilderness, immersion, avalanche, prolonged outdoor exposure, neonate/elderly in a cold dwelling | ICU in-patient on sedation; sepsis; endocrine failure; drug overdose; major trauma |
| Host thermoregulation | Intact, but overwhelmed | Impaired |
| Prognostic implication | Often previously well; good prognosis with rewarming (especially if young) | Prognosis driven by the underlying disease (sepsis, TBI) — often worse |
| Key action | Rewarm + scene safety | Rewarm + diagnose and treat the precipitant (sepsis screen, TFTs, glucose, drug levels) |
Predisposing factors by system — the differential of the cold ICU patient
| System | Predisposing factors |
|---|---|
| Environmental / behavioural | Cold/wet/windy exposure, immersion, avalanche, inadequate clothing, alcohol intoxication (vasodilatation + impaired judgement), homelessness, extremes of age |
| Drugs / toxins | Alcohol, sedatives, opioids, general anaesthesia, antipsychotics, β-blockers (impair shivering), muscle relaxants (abolish shivering) |
| Endocrine | Hypothyroidism / myxoedema coma, hypopituitarism, hypoadrenalism (Addisonian crisis), hypoglycaemia |
| Neurological | Traumatic brain injury (hypothalamic injury), stroke, spinal cord injury (loss of sympathetic vasoconstriction below the lesion), Parkinson's, dementia (impaired behavioural response) |
| Infective | Sepsis (redistribution + impaired thermogenesis) — "the cold septic patient" is a high-risk presentation |
| Trauma | Major trauma ("trauma triad of death": hypothermia + acidosis + coagulopathy — each worsens the others) |
| Dermatological / iatrogenic | Extensive burns, exfoliative dermatitis (loss of skin barrier → evaporative loss); prolonged surgery, massive fluid/blood resuscitation, exposed bowel in theatre; ICU sedation + paralysis + cool room |
Osborn J waves — the ECG deep dive
The Osborn wave (J wave) is the pathognomonic ECG sign of hypothermia — a positive deflection at the J point (the junction of the QRS complex and the ST segment) that gives the complex a "camel-hump" or late-delta-wave appearance. It is the single highest-yield ECG sign in this topic.[2][4]
The Osborn / J wave — what the examiner wants
| Feature | Detail |
|---|---|
| Definition | A positive deflection at the J point (QRS–ST junction), best seen in the lateral precordial (V5–V6) and inferior (II) leads |
| Named for | John Osborn (1953); also called the J wave or camel-hump sign |
| When it appears | Typically below ~32 °C, becoming more prominent as temperature falls |
| Amplitude correlates with severity | The larger the J wave, the deeper the hypothermia — a rough bedside severity gauge |
| Mechanism | An accentuated, heterogeneous repolarisation current — the inward rectifier Ito (I_Kr-like) outward current creating an early repolarisation notch; the current is normally present but becomes pathologically exaggerated when the myocardium cools |
| Pathognomonic? | Highly characteristic of hypothermia, BUT not exclusive — early repolarisation (benign, young males), Brugada syndrome, hypercalcaemia, subarachnoid haemorrhage, and ischaemia can also produce J waves. In the right clinical context (cold patient) it is effectively diagnostic |
| Reversibility | Disappears on rewarming — a reassuring sign that rewarming is working |
ECG changes in hypothermia — the full progression
| Core temperature | ECG finding |
|---|---|
| 35–32 °C | Sinus tachycardia → sinus bradycardia; PR, QRS, and QT interval prolongation (diffuse conduction slowing) |
| 32–30 °C | Osborn / J waves appear (pathognomonic); atrial arrhythmias — atrial fibrillation common |
| 30–28 °C | Progressive bradycardia (resistant to atropine); conduction blocks; premature ventricular ectopics |
| Below 28 °C | Ventricular fibrillation (spontaneous or precipitated by handling); progression to asystole |
| Any temperature | Muscle tremor artefact (shivering) on the ECG can mimic VF/VT — palpate the patient before treating an "arrhythmia" |
Rewarming strategies — the full graded ladder
Rewarming is graded by severity. The guiding principle: match the rewarming intensity to the depth of hypothermia. A patient who can still shiver (mild) can rewarm themselves if you insulate them (passive); a patient who has lost shivering (moderate) needs external heat (active external); a patient in or near arrest (severe) needs core rewarming, with extracorporeal life support (ECLS / ECMO) or cardiopulmonary bypass the definitive method.[1][2][5]
The three rewarming strategies — when, how, how fast, the catch
| Strategy | Method | Target group | Rewarming rate | Key cautions |
|---|---|---|---|---|
| 1. Passive (external) rewarming | Insulation: blankets, warm room, warm fluids; allows endogenous shivering heat production | Mild (32–35 °C), shivering, haemodynamically stable, previously well | ~0.5–1 °C/h | Requires intact shivering and an intact circulation. Fails in the moderate/severe patient who has stopped shivering |
| 2. Active external rewarming | Exogenous heat to the skin: forced warm air (Bair Hugger), radiant warmers, warm blankets, warming mattress, hot packs | Moderate (28–32 °C), or mild not responding to passive | ~1–2 °C/h | Apply to trunk first. Avoid heating the limbs preferentially (worsens after-drop). Monitor for rewarming shock and core after-drop |
| 3. Active internal / core rewarming | Warmed IV fluids (~40 °C), warmed humidified inspired gases, body-cavity lavage (gastric, bladder, peritoneal, pleural/mediastinal via chest tube), and — definitively — ECMO/ECLS or cardiopulmonary bypass | Severe (below 28 °C), especially cardiac arrest or haemodynamic instability | ECMO/CPB: ~1–2 °C/h (controlled, fastest); lavage slower | ECMO/CPB is the method of choice for the arrested hypothermic patient; supports circulation while rewarming |
Choosing the rewarming strategy — the severity-matched algorithm
Mild (HT I, 32–35 °C, shivering, stable)
PASSIVE rewarming: remove wet clothing, dry the patient, insulate with blankets in a warm room (24–28 °C), give warm oral/IV fluids if able. Reassess core temperature every 15–30 min. Target 0.5–1 °C/h. The intact shivering reflex does the work — do not over-sedate or paralyse the patient you intend to rewarm passively.
Moderate (HT II, 28–32 °C, no shivering, decreased LOC)
ACTIVE EXTERNAL rewarming: forced warm air (Bair Hugger) over the trunk, warmed blankets, radiant heat, warming mattress. Add warmed IV fluids (40 °C) and warmed humidified gases if intubated. Monitor continuously — anticipate after-drop (give active external warming to the trunk, not the limbs, to limit peripheral vasodilation). Most patients rewarmed successfully with active external + warmed fluids; escalate to internal methods if unstable.
Severe, no arrest (HT III, below 28 °C, unconscious with vital signs)
ACTIVE INTERNAL rewarming: warmed IV fluids (40 °C), warmed humidified gases, consider body-cavity lavage. TRANSFER to an ECMO-capable centre proactively. If haemodynamics deteriorate → proceed to ECLS. Handle with extreme gentleness — VF risk is maximal. Do NOT intubate roughly; the most experienced operator performs any necessary airway manoeuvre.
Severe with cardiac arrest (HT IV, below 28 °C, VF/asystole/PEA)
DEFINITIVE CORE REWARMING with ECLS (VA-ECMO) or cardiopulmonary bypass — the method of choice. Begin CPR and DO NOT STOP until the core is above 32 °C. Modified ALS: limit defibrillation attempts (see drug/defib section), withhold adrenaline below 30 °C. ECLS both rewarms and provides circulatory support — the ideal platform for prolonged CPR in hypothermia.
Rewarming complete — switch to prevention
Once normothermic, maintain with warmed fluids, warmed gases, and a normothermic environment. Reassess for the underlying cause (sepsis, endocrine, intoxication). Monitor for the complications of rewarming: arrhythmia, rewarming shock, coagulopathy, rhabdomyolysis, ARDS, and infection.
After-drop and rewarming shock — the two hazards of rewarming
| Hazard | Mechanism | Clinical effect | Prevention / management |
|---|---|---|---|
| Core after-drop | Peripheral vasodilation on rewarming returns cold, acidotic, hyperkalaemic blood from the periphery to the core → core temperature continues to fall for a period even after rewarming has started | Apparent worsening of the core temperature and acid–base status; may precipitate VF | Apply active external heat to the TRUNK (not limbs); use warmed IV fluids; do not panic — anticipate it |
| Rewarming shock | Loss of catecholamine drive (vasoconstriction) as the patient warms + relative hypovolaemia from cold diuresis and third-space losses → vasodilation → hypotension | Hypotension, shock on rewarming | Anticipate; give warmed IV fluid boluses; use vasopressors if needed; monitor closely during the rewarming phase |
| Rewarming acidosis / hyperkalaemia | Washout of lactate and K+ from previously underperfused, cold tissues into the central circulation on rewarming | Worsening acidosis, arrhythmia | Anticipate, monitor; treat significant hyperkalaemia; ECLS/haemofiltration if severe |
ECMO / ECLS vs cardiopulmonary bypass vs lavage — core rewarming compared
| Method | How it works | Advantages | Limitations |
|---|---|---|---|
| VA-ECMO / ECLS | Veno-arterial extracorporeal circuit; drains venous blood, warms and oxygenates it, returns to arterial system | Provides circulatory support while rewarming (ideal for arrest); controllable rate; percutaneous (femoral) cannulation feasible by an E-CPR team; the current method of choice | Requires a capable centre/circuit/-team; anticoagulation (though heparin-bonded circuits permit low/no heparin); resource-intensive |
| Cardiopulmonary bypass (CPB) | Central or femoral CPB via a perfusion circuit | Rapid, controlled rewarming with full circulatory support; the historic gold standard (Walpoth 1997) | Usually requires a cardiothoracic theatre/team; more invasive; less readily available than ECMO |
| Body-cavity lavage | Warmed (40 °C) sterile fluid via gastric, bladder, peritoneal, or pleural/mediastinal (chest tube) routes | Bedside-available; faster than external alone | Slower and less effective than ECLS; peritoneal lavage needs large volumes; thoracic lavage via two chest tubes (in + out) is more effective but invasive |
| Warm IV fluids + warmed gases | 40 °C crystalloid; humidified warmed inspired gases | Simple, universally available, low risk, an essential adjunct to ALL strategies | Slow; insufficient alone for severe/arrest — but should ALWAYS be added (every fluid the hypothermic patient receives must be warmed) |
"Not dead until warm and dead" — resuscitation of the arrested hypothermic patient
The central resuscitation dogma of hypothermia: a patient is not dead until warm and dead. The cold brain tolerates anoxia far longer than the warm brain (cerebral metabolic rate falls ~6–7% per °C), so prolonged CPR (hours) can be followed by full neurological recovery. Fixed dilated pupils, absent reflexes, and even asystole are NOT reliable signs of death in hypothermia.[2][3][5]
Resuscitating the arrested hypothermic patient — the algorithm
Confirm cardiac arrest and handle gently
Check for a pulse for up to 60 seconds (the cold, slow pulse can be hard to feel). If no pulse, begin CPR. Handle the patient with extreme gentleness — rough handling can precipitate VF. Do NOT move/jostle unnecessarily.
Begin CPR and do NOT stop
Begin high-quality chest compressions. CONTINUE until the core temperature is at least 32 °C. This may require prolonged CPR (potentially hours) — use mechanical compression devices if available, and activate an ECLS/E-CPR pathway early.
Modified ALS — drugs and defibrillation
Below 30 °C: WITHHOLD adrenaline/vasopressors and antiarrhythmics (ineffective and accumulate). Attempt up to THREE defibrillation shocks for VF/VT; if no response, do not repeat until the core is above 30 °C. Between 30–35 °C: give drugs at EXTENDED intervals (double the normal interval). Above 35 °C: standard ALS.
Activate definitive core rewarming (ECLS/CPB)
The definitive treatment for the arrested hypothermic patient is VA-ECMO or cardiopulmonary bypass — it both rewarms and provides circulatory support. Transport to an ECLS-capable centre, or deploy a percutaneous E-CPR team. This is the single intervention that converts prolonged CPR from futile to survivable.
Decide when to stop (the futility triggers)
Continue CPR until the core is above 32 °C AND one of the following futility criteria is met: (a) serum potassium above 8–10 mmol/L (pre-terminal cellular death, usually from asphyxia/prolonged anoxia); (b) a clearly lethal underlying cause; (c) ECLS rewarming to normothermia fails to restore a perfusing rhythm (true "warm and dead"). A potassium above 12 mmol/L or a core temperature below ~24 °C in an unwitnessed arrest with asystole carries a near-zero survival and supports ceasing CPR.
Post-resuscitation care
If return of spontaneous circulation (or ECLS support) is achieved, target normothermia (avoid hyperthermia), manage the precipitating cause, and watch for the complications: ARDS, coagulopathy, rhabdomyolysis, pancreatitis, and infection. Neurological recovery can be excellent even after hours of CPR — do not prognosticate early.
Prognostic factors in hypothermic cardiac arrest — who survives
| Factor | Better prognosis | Worse prognosis |
|---|---|---|
| Serum potassium | Below 6–8 mmol/L | Above 8–10 mmol/L (pre-terminal; reflects asphyxia/cell death) — strongest single predictor of non-survival |
| Witnessed arrest | Witnessed, rapid rescue | Unwitnessed, prolonged (especially asphyxia: drowning, avalanche burial with airway obstruction) |
| Rhythm | VF | Asystole |
| Core temperature | Higher (e.g. above 24–28 °C) | Very low (below 24 °C) with asystole — but a low temperature ALONE is NOT a reason to stop (the colder, the more protected) |
| Mechanism | Pure hypothermia (cold air) | Asphyxial hypothermia (submersion, avalanche burial, aspiration) — hypoxia precedes cooling |
| Age / comorbidity | Young, previously well | Elderly, comorbid, sepsis-driven |
| CPR to ECLS time | Short | Prolonged CPR before ECLS |
Drug & defibrillation management — the temperature-band rules
Drug metabolism and receptor responsiveness collapse in the cold. The standard ALS algorithm must be modified by core temperature band — giving adrenaline to a patient below 30 °C is not merely useless, it accumulates to toxic levels as the patient rewarms.[2][5]
Drug and defibrillation management by core temperature band
| Core temperature | Adrenaline / vasopressors | Antiarrhythmics (amiodarone) | Defibrillation |
|---|---|---|---|
| Mild (above 35 °C) | Standard | Standard | Standard |
| 30–35 °C | Extended interval — give at DOUBLE the normal interval (e.g. every 6–10 min) | Extended interval | Standard, but may be less effective; repeat as needed |
| Below 30 °C | WITHHOLD — ineffective (receptors unresponsive) and the drug accumulates (no metabolism), reaching toxic levels on rewarming | WITHHOLD — same rationale | Attempt up to THREE shocks for VF/VT; if unsuccessful, withhold further shocks and drugs until the core is above 30 °C, then resume |
| Above 35 °C (post-rewarm) | Standard ALS resumed | Standard | Standard |
Why adrenaline is withheld below 30 °C — the mechanism
Receptors are unresponsive in the cold
Adrenergic receptors and the myocardial conduction tissue are markedly less responsive at low temperature — exogenous adrenaline has little haemodynamic or rhythm-restoring effect below 30 °C.
Metabolism is abolished
Hepatic and tissue enzyme activity collapses with temperature (Q10 effect), so adrenaline, amiodarone, and lidocaine are NOT cleared — they accumulate in the plasma with each dose given.
Toxicity on rewarming
When the patient is rewarmed above 30–35 °C, the accumulated drug suddenly becomes active and is metabolised erratically, risking severe hypertension, tachyarrhythmia, and VF — the very rhythm you are trying to avoid.
Practical rule
Below 30 °C: give NO adrenaline, NO amiodarone, NO lidocaine — focus on CPR and rewarming. 30–35 °C: resume drugs at double the usual interval. Above 35 °C: standard ALS. Defibrillation may be attempted (up to three shocks) at any temperature for a shockable rhythm, but is far more likely to work above 30 °C.
Fluid management — warm everything that goes in
Every patient with hypothermia is volume-depleted through cold diuresis (cold-induced centralisation of volume → natriuresis/diuresis), third-space losses, and insensible losses. The corollary that the exam rewards: warm every fluid and blood product the patient receives — room-temperature crystalloid (~20 °C) or refrigerated blood (4 °C) actively cools the patient and can precipitate arrhythmia.[1][1][2]
Fluid management in hypothermia — the principles
| Principle | Rationale | Practice |
|---|---|---|
| Warm ALL fluids | Cold fluids lower the core further; 1 L of 4 °C blood requires ~14 kcal to warm to 37 °C (drawn from the patient) | Use a fluid/blood warmer; target fluid temperature ~40 °C. This applies to maintenance, boluses, and transfusion alike |
| Replace the cold-diuresis deficit | Cold diuresis + third-space loss → relative hypovolaemia, worsened by rewarming vasodilation (rewarming shock) | Give warmed isotonic crystalloid; titrate to perfusion/ lactate/ output. Anticipate the need during rewarming |
| Warm, humidify inspired gases | Cold dry gas steals heat and moisture from the respiratory tract | Ventilator with heated humidifier (~40 °C, 100% humidity) for the intubated patient |
| Avoid over-resuscitation | Excessive cold fluid before warming risks volume overload + arrhythmia; rewarming itself restores tone | Resuscitate to endpoints (lactate, MAP, output), not to an arbitrary volume |
| Correct glucose | Hypothermia causes hyperglycaemia (insulin resistance + reduced secretion); rewarming reverses this → hypoglycaemia risk if insulin over-given | Monitor glucose; use insulin cautiously and only if clearly indicated; expect the requirement to fall as the patient warms |
Complications of hypothermia and rewarming
The complications span every system. The arrhythmic and haematological complications are the most frequently examined.[1][1][4]
Complications by system — recognise and pre-empt
| System | Complication | Mechanism / recognition | Management |
|---|---|---|---|
| Cardiac | Atrial fibrillation | Common below ~33 °C; usually reverts on rewarming | Rewarm; rate-control rarely needed; anticoagulate if persistent after rewarm |
| Cardiac | Ventricular arrhythmia (VT/VF) | Below 28 °C; precipitated by rough handling, invasive lines, acidosis, hyperkalaemia | Modified ALS (see drug/defib section); ECLS; correct K+ and acidosis |
| Cardiac | Bradycardia resistant to atropine | The cold sinus node is intrinsically slowed, not vagally blocked — atropine does not work | Rewarm; do NOT give atropine repeatedly; pacing rarely needed, external pacing if required |
| Haematological | Coagulopathy (cold coagulopathy) | The enzymatic coagulation cascade is temperature-dependent — PT and APTT prolong IN VIVO; platelets sequester and dysfunction (also thrombocytopenia with rewarming). NB: the lab warms the sample to 37 °C, so the reported PT/APTT may look normal — the patient is still coagulopathic | Warm the patient; use blood products and tranexamic acid as guided by viscoelastic testing/clinical bleeding; correct acidosis and hypocalcaemia |
| Haematological | DIC | Tissue factor release (especially trauma/pancreatitis/sepsis-associated) | Treat the cause; component therapy; ECLS circuit anticoagulation complicates management |
| Renal | AKI / rhabdomyolysis | Cold + immobility → muscle injury; myoglobinuria → AKI; cold diuresis compounds volume depletion | IV fluid to maintain output; monitor CK and urine myoglobin; consider renal replacement if severe |
| Respiratory | ARDS / pulmonary oedema | Capillary leak on rewarming; aspiration during reduced consciousness; cold-induced bronchorrhoea | Lung-protective ventilation; treat aspiration pneumonia |
| Metabolic | Hyperglycaemia → hypoglycaemia on rewarm | Insulin resistance in the cold, reversed on warming | Cautious insulin; monitor glucose closely during rewarming |
| GI | Pancreatitis (often silent/subclinical) | Cold pancreatic injury; raised amylase common | Supportive; monitor; rarely the dominant problem |
| Infective | Pneumonia, sepsis | Immunosuppression + aspiration + invasive lines | Surveillance cultures; early antibiotics if septic; remove lines when safe |
| Musculoskeletal | Compartment syndrome, frostbite | Prolonged immobility + cold; peripheral tissue freezing | Monitor perfusion; fasciotomy if needed; frostbite managed by rapid rewarming of the affected part (water 37–39 °C) — do NOT rub |
Hypothermic coagulopathy — why the INR looks normal but the patient bleeds
The coagulation cascade is temperature-dependent
The serine proteases of the coagulation cascade (factors II, VII, IX, X) and platelet function are enzyme-driven and therefore slow as temperature falls. In the cold patient, clot formation is genuinely impaired in vivo — the basis of hypothermic coagulopathy.
The laboratory measures at 37 °C
The PT/INR and APTT are performed on the patient's plasma WARMED to 37 °C in the analyser. The assay therefore reports what the clotting would be at normal temperature — and can read as normal even though the patient, at 29 °C, is functionally coagulopathic.
Platelets are also affected
Cold causes platelet sequestration (hepatic/splenic) and reversible platelet dysfunction; thrombocytopenia often appears on rewarming. The "trauma triad of death" — hypothermia, acidosis, coagulopathy — is self-reinforcing.
Management
The definitive treatment is to WARM the patient — coagulopathy resolves with rewarming. Support with blood products and tranexamic acid if bleeding; correct the associated acidosis and ionised hypocalcaemia (which also impair clotting). Use viscoelastic testing (ROTEM/TEG) run at the patient's temperature where available.
Special situations
Hypothermia in special situations — the modifying factors
| Situation | Key modifying factor | Management point |
|---|---|---|
| Immersion / submersion (drowning) hypothermia | Cooling is rapid (water conducts heat ~25× faster than air); usually accompanied by ASPHYXIA — the dominant determinant of outcome | Treat as asphyxial arrest + hypothermia; the asphyxia (not the cold) often limits survival. ECLS if available; aggressive CPR. "Not dead until warm and dead" applies but prognosis is worse than pure hypothermia |
| Avalanche burial | Asphyxia (airway packed with snow) is the usual cause of death; hypothermia is secondary. Duration of burial and presence of an airway predict outcome | If buried more than ~35 min with a packed airway, treat as asphyxial; core temperature alone does not guide prognosis. K+ above 8 mmol/L suggests non-survivable asphyxia |
| Myxoedema coma (hypothyroidism) | Hypothermia is secondary to profound hypometabolism; often elderly, with bradycardia, hyponatraemia, hypoventilation | IV levothyroxine (and hydrocortisone — coexistent adrenal insufficiency) + passive/active rewarming + treat the precipitant. DO NOT rely on passive rewarming alone — thermogenesis is absent |
| Paediatric | High surface-area-to-mass ratio → rapid cooling; BUT children (especially young) tolerate deep hypothermia and prolonged CPR remarkably well (the basis of good outcomes in paediatric drowning/ECMO) | Aggressive resuscitation is particularly justified; the younger the patient, the more favourable the potential outcome even after prolonged arrest |
| Elderly | Impaired thermoregulation + vasoconstriction + comorbidity + drugs; often secondary hypothermia (sepsis, stroke) | Always seek and treat the precipitant; worse prognosis than primary hypothermia in the young |
| Trauma (the lethal triad) | Hypothermia + acidosis + coagulopathy are mutually reinforcing — each worsens the others and mortality rises steeply | Damage-control resuscitation: warm the patient aggressively (warm fluids, warm room, Bair Hugger, warmed blood), correct acidosis, prevent coagulopathy with early blood product/ tranexamic acid; stop the bleeding fast |
| Therapeutic hypothermia (TTM after cardiac arrest) | Intentional cooling to 32–36 °C for 12–24 h post-arrest — the controlled counterpart of accidental hypothermia | Different management goal: the patient is sedated/paralysed (shivering suppressed), actively temperature-controlled; rewarm slowly (0.25–0.5 °C/h). Not the same as accidental hypothermia, but the physiology is shared |
Prognostic scoring — the HOPE score
The HOPE score (HypOthermia in Switzerland Prognostic scorE) and the simpler ICE-IT/algorithm-based approaches estimate the probability of survival in hypothermic arrest and help decide whether to continue CPR / proceed to ECLS. The dominant message: survival can be excellent even after prolonged CPR and profound hypothermia, PROVIDED there is no lethal hyperkalaemia and the mechanism is pure hypothermia (not asphyxia).[2][3]
Prognostic markers in hypothermic arrest — the synthesis
| Marker | Significance |
|---|---|
| Serum potassium | The single most powerful predictor. Potassium above 8–10 mmol/L in a hypothermic arrest patient indicates pre-terminal cellular death (usually from asphyxia/prolonged anoxia) and predicts non-survival — supports ceasing CPR. Below this, proceed |
| Core temperature at arrest | Lower temperature does NOT mean worse prognosis (the colder the brain, the more protected). A very low temperature is NOT a reason to stop CPR |
| Mechanism | Pure hypothermia (air exposure) → good prognosis with rewarming; asphyxial hypothermia (submersion, avalanche airway obstruction) → poor prognosis |
| HOPE score | A validated multivariable score (age, sex, asphyxia, core temperature, K+, arrest rhythm, CPR quality, cooling rate) estimating survival probability — used to triage ECLS |
| ECLS availability | Access to VA-ECMO/CPB is the single biggest modifiable determinant of survival in severe hypothermic arrest |
Evidence, trials, and outcomes
Walpoth 1997 (NEJM) — long-term outcome of deep hypothermia with circulatory arrest rewarmed by CPB
Design
Long-term follow-up case series — 32 patients with accidental deep hypothermia (core below 28 °C) and circulatory arrest, rewarmed with cardiopulmonary bypass; 15 long-term survivors
Key finding
15 of 32 survived to discharge; long-term neuropsychological follow-up (mean 6.7 years) showed no or minimal cerebral impairment and no hypothermia-related reduction in quality of life
Message
Young, otherwise healthy patients can survive accidental deep hypothermia with circulatory arrest — with full neurological recovery — when rewarmed rapidly by cardiopulmonary bypass. The landmark evidence that 'not dead until warm and dead' is more than a slogan
Brown, Brugger, Boyd & Paal 2012 (NEJM) — the definitive review
Type
Comprehensive clinical review of accidental hypothermia in the New England Journal of Medicine
Key contributions
Standardised the SWISS STAGING SYSTEM (HT I–IV) for prehospital use; defined the graded rewarming strategy (passive → active external → active internal/ECLS); established the modified drug/defibrillation rules; promoted the 'not dead until warm and dead' principle and ECLS for arrest
Why it matters for exams
The most frequently cited framework for hypothermia in critical-care vivas — the staging, the rewarming ladder, the handle-gently principle, and the ECLS-for-arrest recommendation all trace here
European Resuscitation Council Guidelines 2021 — cardiac arrest in special circumstances (Paal et al.)
Type
Authoritative resuscitation guideline — the operational standard for hypothermic cardiac arrest in Europe and ANZ
Key recommendations
Withhold adrenaline below 30 °C, give at extended intervals 30–35 °C, standard above 35 °C; attempt up to three defibrillations for VF/VT then defer until above 30 °C; continue CPR until the core is at least 32 °C; use ECLS/CPB as the definitive treatment for arrest; use serum potassium (above 8 mmol/L) to judge futility
Practical role
The bedside algorithm for the arrested hypothermic patient — the source to cite for the temperature-banded drug and defibrillation rules
Accidental hypothermia outcomes with ECLS — registry data
Type
Pooled and registry data (e.g. the International Hypothermia Registry and ECLS case series) on survival in hypothermic arrest rewarmed by ECMO/CPB
Key finding
Survival to discharge with good neurological outcome of roughly 40–60% (and up to ~80% in selected pure-hypothermia, witnessed cohorts) for hypothermic arrest rewarmed by ECLS — far exceeding normothermic arrest survival. Outcome is worst with asphyxia (drowning/avalanche), asystole, and hyperkalaemia
Message
ECLS rewarming transforms the prognosis of profound hypothermic arrest; the threshold to deploy E-CPR should be low. Mortality remains dominated by the asphyxia mechanism, not the cold
Common viva questions and model answers
Hypothermia viva — the recurring questions and model answers
| Question | Model answer |
|---|---|
| "Classify hypothermia and give the clinical features of each grade." | Mild (32–35 °C): conscious, shivering, tachycardia, ataxia, impaired judgement. Moderate (28–32 °C): decreased LOC, loss of shivering, bradycardia, AF, Osborn J waves. Severe (below 28 °C): coma, fixed pupils, areflexia, VF/asystole, pulseless. Map to Swiss HT I–IV (conscious-shivering / impaired-not shivering / unconscious-vital signs / unconscious-no vital signs). |
| "What is the Osborn / J wave and what does it mean?" | A positive deflection at the J point (QRS–ST junction), pathognomonic of hypothermia, appearing below ~32 °C; amplitude correlates with severity; reversible on rewarming. Mechanism: exaggerated outward Ito repolarisation current. DDx: early repolarisation (benign), Brugada, hypercalcaemia, SAH. |
| "How would you rewarm this patient?" | Grade by severity: mild → passive (insulate, warm room, warm fluids, allow shivering), 0.5–1 °C/h; moderate → active external (Bair Hugger on trunk, warmed blankets), 1–2 °C/h, plus warmed IV fluids/gases; severe → active internal (warmed fluids 40 °C, warmed humidified gases, lavage) and, in arrest, definitive ECLS/CPB. Warm every fluid; anticipate after-drop and rewarming shock. |
| "When can you stop CPR in a hypothermic arrest?" | NOT until the core is at least 32 °C, AND a futility trigger is met: serum potassium above 8–10 mmol/L (pre-terminal cellular death), a clearly lethal cause, or failure to achieve a perfusing rhythm once normothermic on ECLS ('warm and dead'). A low temperature alone is never a reason to stop. |
| "How do you modify ALS in hypothermia?" | Below 30 °C: withhold adrenaline and antiarrhythmics (ineffective, accumulate to toxicity on rewarm); up to three defibrillation attempts then defer. 30–35 °C: drugs at double the usual interval. Above 35 °C: standard ALS. Activate ECLS/E-CPR early. |
| "Why does the INR look normal but the patient still bleeds?" | The coagulation cascade is temperature-dependent (impaired in vivo in the cold patient), but the laboratory assays the plasma warmed to 37 °C, so it reports normal clotting that does not reflect the patient's actual hypothermic coagulopathy. Treat by warming the patient + products/ tranexamic acid + correcting acidosis and hypocalcaemia. |
| "Why is the potassium high, and what does it mean?" | A serum potassium above 8–10 mmol/L reflects pre-terminal cellular death (Na/K pump failure → K+ efflux) from asphyxia or prolonged anoxia — the strongest single predictor of non-survival and a futility criterion. It is NOT caused by the cold itself. |
| "Why warm all the fluids?" | Cold diuresis makes the patient volume-deplete; room-temperature crystalloid (~20 °C) and refrigerated blood (4 °C) actively cool the patient and can precipitate arrhythmia. Warm all maintenance, bolus, and transfusion fluids to ~40 °C with a fluid warmer; warm and humidify inspired gases. |
Exam practice — SAQs
SAQ — Severe hypothermia with ventricular fibrillation arrest
10 minutes · 10 marks
A 32-year-old previously well man is brought to the emergency department unconscious after being found outdoors in winter, exposed for an estimated 8 hours. Rectal core temperature on a low-reading thermometer is 26.5 degrees C. The ECG shows prominent Osborn J waves with sinus bradycardia at 28 per min. While he is being transferred to a warming bed he suddenly develops ventricular fibrillation; no pulse is palpable. You are the ICU registrar leading the arrest.
SAQ — Rewarming strategies in accidental hypothermia
10 minutes · 10 marks
A 78-year-old woman is admitted to ICU after being found collapsed at home with the heating off for two days. Rectal core temperature is 29.2 degrees C. She is drowsy (GCS 11), not shivering, with atrial fibrillation at a ventricular rate of 50 per min and prominent Osborn J waves on the ECG. BP 96/58, lactate 2.4 mmol/L, glucose 9 mmol/L. Past history: hypertension and treated hypothyroidism; TSH and cortisol have been sent.
High-yield clinical pearls (CICM / FFICM / EDIC)
Additional red flags
References
- [1]Truong J, et al. Accidental Hypothermia in Hospitalized Adults: Risk Factors, Management Strategies, and Clinical Outcomes: A Systematic Review Cureus, 2026.PMID 41815600
- [2]Brown DJA, Brugger H, Boyd J, Paal P Selective adsorption of lattice peptides on patterned surfaces Phys Rev E Stat Nonlin Soft Matter Phys, 2012.PMID 23005152
- [3]Walpoth BH, Walpoth-Aslan BN, Mattle HP, et al. Outcome of survivors of accidental deep hypothermia and circulatory arrest treated with extracorporeal blood warming N Engl J Med, 1997.PMID 9366581
- [4]Mallet ML Pathophysiology of accidental hypothermia QJM, 2002.PMID 12454320
- [5]Paal P, van Goor H, Bottiger BW, et al. Commentary on trends in fundoplication volume for pediatric gastroesophageal reflux disease J Pediatr Surg, 2021.PMID 33773800