ICU · Gastroenterology
Acute cholecystitis in ICU: severe and complicated presentations
Also known as Acute cholecystitis · Gallbladder empyema · Gangrenous cholecystitis · Emphysematous cholecystitis · Acalculous cholecystitis
Acute cholecystitis: inflammation of gallbladder, usually from cystic duct obstruction by gallstone (90-95%). ICU-relevant severe presentations: (1) GANGRENOUS cholecystitis (wall necrosis → perforation, mortality 15-30%). (2) EMPHYSEMATOUS cholecystitis (gas-forming organisms in wall — Clostridium, E. coli — mortality 15-25%). (3) ACALCULOUS cholecystitis (10% — critically ill patients, no stones — ischaemia, biliary stasis; mortality 30-50%). (4) PERFORATION (localised abscess or free perforation with bilious peritonitis). (5) EMPYEMA (pus-filled gallbladder — surgical emergency). Severe presentations need ICU for sepsis, organ failure, post-operative care. Management: antibiotics (gram-negative + anaerobic cover), cholecystectomy (early laparoscopic for fit; percutaneous cholecystostomy for unfit/critically ill).
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Severe cholecystitis variants
| Feature | Gangrenous | Emphysematous | Acalculous | Perforated | Empyema |
|---|---|---|---|---|---|
| Pathology | Wall necrosis/ischaemia | Gas-forming organisms in wall | No stones, ischaemia/stasis | Full-thickness wall defect | Pus-filled GB |
| Population | Elderly, diabetic, vasculopaths | Diabetic (M:F 2:1) | Critically ill ICU patients | Advanced age, delayed presentation | Any |
| Imaging | Wall irregularity, sloughing | Gas in wall (plain film/CT) | Distended GB, no stones, wall thickening | Wall defect, free fluid | GB distended with debris/pus |
| Mortality | 15-30% | 15-25% | 30-50% | 30% (free) | 10-25% |
| Management | Urgent cholecystectomy | Urgent cholecystectomy + broad-spectrum abx | Percutaneous cholecystostomy first | Emergency surgery | Cholecystectomy/cholecystostomy |
Management of acute cholecystitis
- Assess severity — Tokyo Guidelines 2018 severity grading: Grade I (mild), Grade II (moderate), Grade III (severe — organ dysfunction)
- Resuscitate — IV fluids, analgesia, correct electrolytes. Sepsis protocol if septic
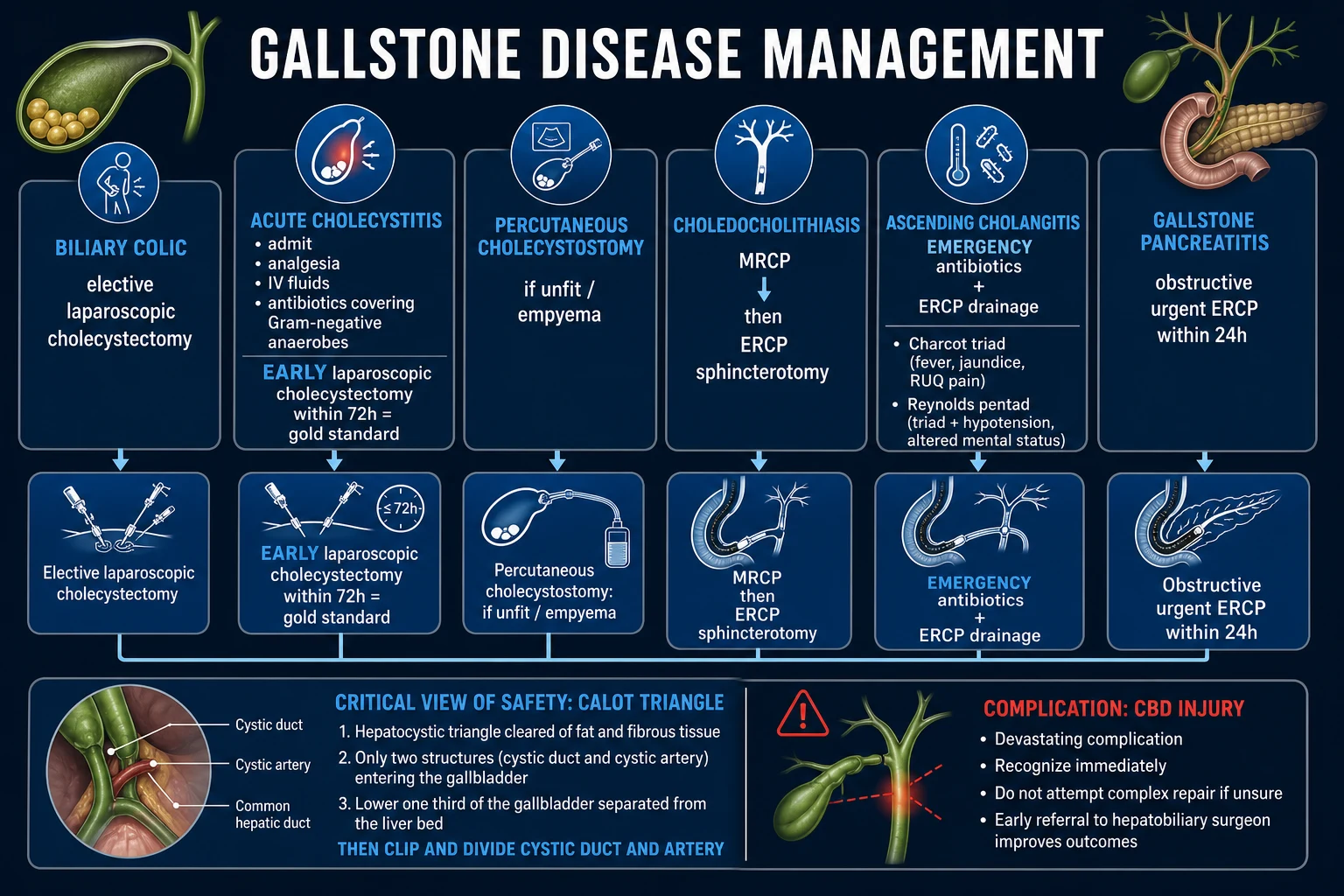
- Antibiotics — Grade I-II: amoxycillin/clavulanate OR ceftriaxone + metronidazole. Grade III/severe: piperacillin/tazobactam OR meropenem. Cover gram-negatives + anaerobes. 4-7 days (or until source control)
- Source control — within 72-96h for fit patients: Laparoscopic cholecystectomy (gold standard). Early (within index admission) reduces complications vs delayed
- Source control — for critically ill/unfit: Percutaneous cholecystostomy (drain gallbladder via catheter). Bridge to cholecystectomy (elective, 2-3 months later) or definitive in poor surgical candidates
- Manage complications — gangrene (urgent surgery), perforation (emergency surgery), empyema (drainage), sepsis (ICU support)
- ERCP if concurrent choledocholithiasis or cholangitis — clear common bile duct stones
Exam practice — SAQs
SAQ — Severe acute cholecystitis with septic shock (emphysematous variant)
10 minutes · 10 marks
A 68-year-old man with type 2 diabetes, hypertension and obesity presents with 4 days of right upper quadrant pain, fever and rigors. On examination he is confused (GCS 13), temperature 39.2 degrees C, HR 128, BP 78/46 (MAP 57) on noradrenaline 0.35 mcg/kg/min after 30 mL/kg crystalloid, RR 28, SpO2 94 percent on room air, with marked right upper quadrant tenderness and guarding. Lactate 4.8 mmol/L, WCC 28.4, CRP 320, bilirubin 35 micromol/L, creatinine 215 (baseline 90), INR 1.6, platelets 92, lipase normal. CT abdomen shows gas within the gallbladder wall, pericholecystic stranding, gallstones and a small amount of adjacent free fluid. Blood cultures are pending.
SAQ — Tokyo Guidelines 2018 diagnostic and severity grading applied to bedside decision-making
10 minutes · 10 marks
A 74-year-old woman presents with 36 hours of right upper quadrant pain, fever 38.6 degrees C and two rigors. She is alert (GCS 15), BP 96/58 (MAP 71) off vasopressors, HR 108 sinus, RR 22, SpO2 96 percent on room air. Murphy sign is positive with marked right upper quadrant tenderness. WCC 19,600, CRP 180, bilirubin 28 micromol/L, creatinine 95 (baseline 90), INR 1.1, platelets 220, lipase normal, PaO2/FiO2 380. Bedside ultrasound shows gallstones, gallbladder wall thickening 6 mm, pericholecystic fluid and a positive sonographic Murphy sign.
Clinical pearls
Red flags
Prognosis
Tokyo Guidelines 2018 validation (Yokoe 2018)
Multicentre cohort. Severity grade predicted mortality:
- Grade I (mild): mortality <1%
- Grade II (moderate): mortality 1-5%
- Grade III (severe — organ dysfunction): mortality 5-15% [1]
Complications by severity:
- Grade I: gangrene 10%, perforation 2%
- Grade II: gangrene 25%, perforation 8%, empyema 5%
- Grade III: gangrene 40%, perforation 15%, empyema 10% [1]
Percutaneous cholecystostomy success: 85-95% (technical), 75-85% (clinical improvement within 48-72h). Early laparoscopic cholecystectomy: 90% success, 10% conversion to open, 0.2-0.5% bile duct injury.
Pathophysiology
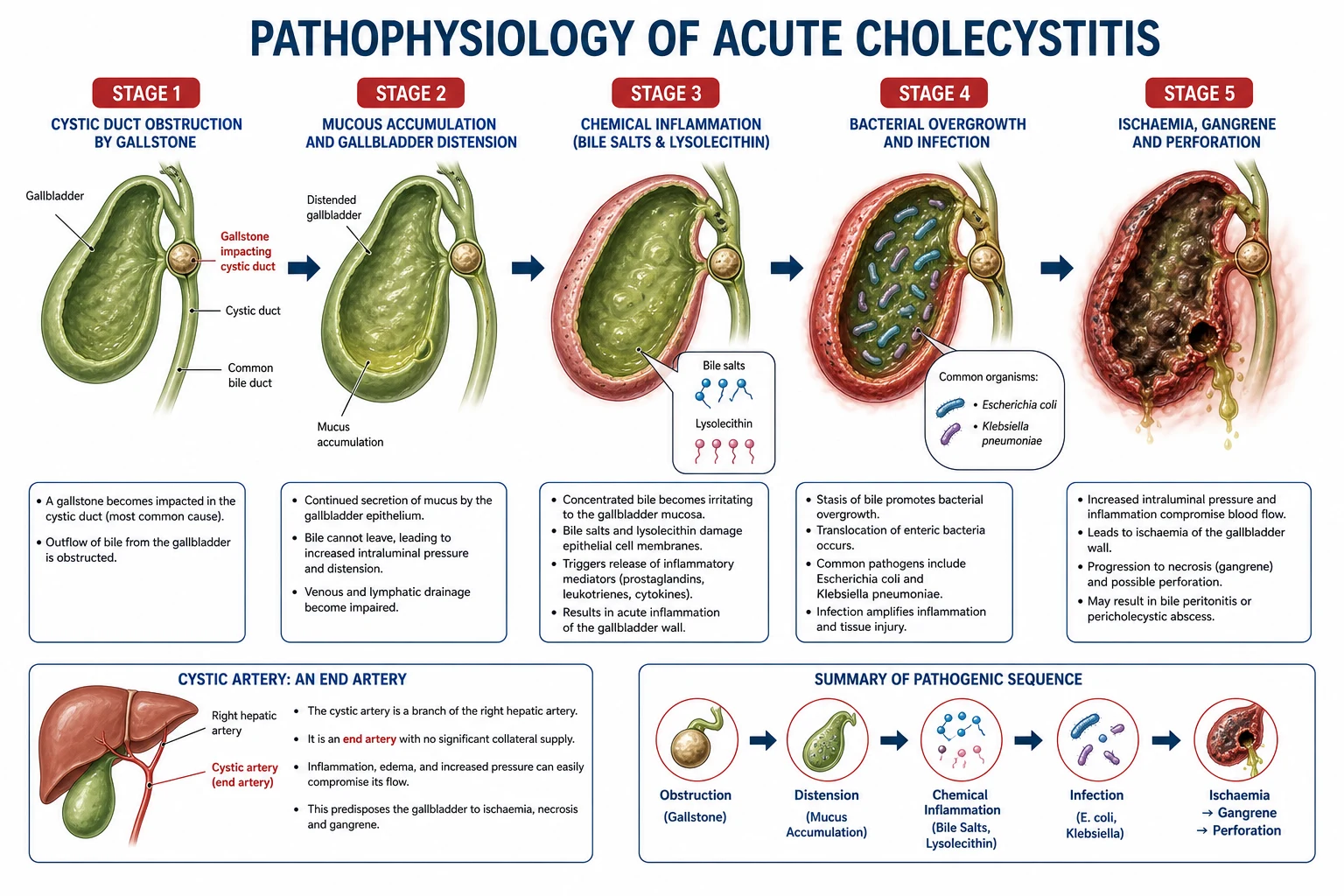
Acute calculous cholecystitis begins with persistent obstruction of the cystic duct by an impacted gallstone (usually at Hartmann's pouch or the neck), in contrast to biliary colic where the stone disimpacts and symptoms resolve within a few hours. The obstructed gallbladder continues to absorb water and electrolytes from trapped bile, concentrating it into a thick, viscid, detergent-like sludge that is directly cytotoxic to the gallbladder mucosa. Mucosal injury triggers prostaglandin release (PGE2, leukotrienes), which increases mucus secretion, amplifies inflammation, and causes pain.[7] }
The injury cascade proceeds in a predictable sequence: [1]
- Cystic duct obstruction → bile stasis and progressive gallbladder distension.
- Lymphatic and venous obstruction (rising intraluminal pressure) → wall oedema and impaired clearance of inflammatory mediators.
- Ischaemia — arterial inflow eventually compromised as intramural pressure exceeds capillary perfusion pressure; the gallbladder fundus (the most distal point of the end-arterial supply from the cystic artery) is the most vulnerable to ischaemia, which explains why gangrene and perforation most often occur at the fundus.
- Mucosal ulceration and necrosis → transmural inflammation; secondary bacterial infection (E. coli, Klebsiella, Enterococcus, Enterobacter, and anaerobes — Bacteroides, Clostridium).
- Gangrene (full-thickness wall necrosis, 10-30% of operated cases) → perforation (free bilious peritonitis or walled-off pericholecystic abscess) or empyema (frank pus).[7] }
Acalculous cholecystitis follows a different route: gallbladder ischaemia in the setting of systemic hypoperfusion (sepsis, haemorrhagic shock, low-flow states) combined with bile stasis (fasting, TPN, opioids, mechanical ventilation) and mucosal injury produces a sterile inflammatory process in which infection is secondary. Biliary sludge forms in >50% of prolonged ICU stays and provides a nidus. The ischaemia-reperfusion injury and endotoxaemia drive the histology — a necrotising, often haemorrhagic, inflammation without the typical obstructing calculus.[10] }
Emphysematous cholecystitis is a specific ischaemia-plus-infection variant: compromised blood supply permits invasion by gas-forming organisms (Clostridium perfringens, Clostridium welchii, E. coli, Klebsiella), producing gas within the gallbladder wall and lumen. The male predominance (M:F ≈ 2:1) and 50% prevalence of diabetes distinguishes it from typical gallstone disease and reflects an underlying vascular/ischaemic aetiology.[7] }
Pathophysiological cascade of acute cholecystitis
- Stone impacts at cystic duct / Hartmann's pouch — persistent obstruction (vs transient in biliary colic)
- Bile stasis + water/electrolyte absorption → concentrated, cytotoxic bile; mucosal prostaglandin release
- Gallbladder distension → rising intraluminal pressure → lymphatic then venous outflow obstruction → wall oedema
- Arterial inflow compromise → mucosal ischaemia (fundus most vulnerable — end-artery territory of cystic artery)
- Mucosal necrosis / ulceration → secondary bacterial colonisation (Enterobacteriaceae + anaerobes)
- Transmural inflammation → clinical syndrome (fever, RUQ pain, Murphy sign, leucocytosis)
- Complication branch-points: gangrene (necrosis) → perforation (free/subacute/fistula) OR empyema (pus)
Clinical presentation
The classic presentation is RUQ pain that develops over hours to days, often following a fatty meal, and is continuous and progressive (unlike the episodic, cramping pain of biliary colic that resolves spontaneously). Pain radiates to the right shoulder or interscapular area in ~25% (diaphragmatic irritation).[7] }
Murphy sign — the cardinal physical finding: deep inspiration during palpation of the RUQ elicits a catch in inspiration (inspiratory arrest) due to pain as the inflamed gallbladder contacts the examining hand. Performed with the patient supine. Sensitivity ~65%, specificity ~87% in primary studies; a sonographic Murphy sign (maximal tenderness when the ultrasound probe is positioned directly over the visualised gallbladder) is more specific for gallbladder pathology. The Murphy sign has reduced sensitivity in the elderly (around 50%).[9] }
Associated features:
- Fever (typically low-grade 38-39 °C; high fever or rigors suggest cholangitis, empyema, or gangrene).
- Leucocytosis (WBC 10-15 × 10^9/L typical; >18 × 10^9/L is a Tokyo Guidelines Grade II criterion).
- CRP elevated (>3 mg/dL is a TG18 systemic inflammatory criterion).
- Mild jaundice may occur (~20%) even without choledocholithiasis — caused by inflammatory oedema compressing the common bile duct (Mirizzi-type mechanism) or passage of small stones. Bilirubin >40 μmol/L (2.5 mg/dL) strongly suggests choledocholithiasis/cholangitis and warrants ERCP/MRCP.[3] }
- Nausea, vomiting, anorexia are nearly universal.
Acute cholecystitis vs biliary colic vs cholangitis vs pancreatitis (RUQ differentials)
| Feature | Biliary colic | Acute cholecystitis | Ascending cholangitis | Acute pancreatitis (biliary) |
|---|---|---|---|---|
| Obstruction | Transient cystic duct | Persistent cystic duct | Common bile duct | Ampullary (transient) |
| Pain duration | <6 h, episodic | Continuous, hours-days | Continuous + rigors | Epigastric, boring to back |
| Fever | Absent | Low-moderate | High, spiking | Variable |
| Jaundice | Absent | Mild/absent | Prominent (Charcot) | Variable |
| Murphy sign | Absent | Positive | May be positive | Absent |
| Hypotension/AMS | Absent | Absent (unless Grade III) | Reynolds' pentad | May be present |
| Lipase | Normal | Normal | Normal | >3 × ULN |
| First-line imaging | Ultrasound | Ultrasound | Ultrasound + MRCP/ERCP | CT |
| ERCP role | None | If CBD stone | Definitive (drainage) | If ongoing obstruction |
Atypical presentations requiring vigilance in ICU
- Elderly and diabetic patients may have minimal pain, no fever, and vague symptoms — present late with gangrene or perforation. Unexplained sepsis or delirium in an elderly diabetic may be the only clue.
- Critically ill / sedated / ventilated patients — acalculous cholecystitis is occult: unexplained fever, leucocytosis, feed intolerance, or rising liver enzymes in a patient with multi-organ failure should prompt gallbladder ultrasound.
- Postoperative / post-trauma / burns patients — same occult presentation; gallbladder imaging is part of the fever workup in the ICU.
- Immunocompromised (neutropenic, post-transplant) — may have minimal signs; high index of suspicion required. [1]
Imaging
Ultrasound — first-line
Bedside or formal ultrasound is the first-line imaging modality (sensitivity ~81%, specificity ~83% per Kiewiet meta-analysis). It is portable, radiation-free, repeatable, and ideal for the critically ill.[9] }
Diagnostic sonographic features (any one strongly suggestive; multiple features increase certainty):
- Gallstones (shadowing, mobile echogenic foci) — present in 90-95% of calculous cholecystitis.
- Gallbladder wall thickening >3-4 mm (measured in the transverse plane, anterior wall; oedematous — "halo" sign or striations suggest severe/gangrenous).
- Pericholecystic fluid (fluid in the gallbladder fossa).
- Sonographic Murphy sign — maximal tenderness when the probe is over the gallbladder (high specificity, lower sensitivity if patient has received analgesia).
- Gallbladder distension (short axis >4 cm, or >8 × 4 cm in adults; cannot be assessed if previously contracted or post-cholecystectomy).
- Intraluminal membranes / echogenic debris — sloughed mucosa, sludge, or pus suggest gangrene or empyema.
- Gas in the gallbladder wall — emphysematous cholecystitis. [1]
HIDA scan (cholescintigraphy) — gold standard for cystic duct patency
Technetium-99m HIDA (hepatobiliary iminodiacetic acid) cholescintigraphy is the most sensitive test for acute cholecystitis (sensitivity ~96%, specificity ~90% per Kiewiet). The radiotracer is taken up by hepatocytes and excreted into bile; non-visualisation of the gallbladder within 1 hour (or 3-4 hours if delayed imaging) indicates cystic duct obstruction, the defining lesion of acute cholecystitis.[9] }
Limitations in ICU: requires transport to nuclear medicine, prolonged fasting (>4-6 h), and false-positives in any state of gallbladder non-filling (prolonged fasting >24 h, severe hepatocellular disease, TPN, severe intercurrent illness, chronic cholecystitis). Morphine augmentation (constricts sphincter of Oddi, redirects tracer into cystic duct) can shorten the study and reduce false-positives. Rarely used in ICU practice but is the gold standard for equivocal cases.[7] }
CT — complications and atypical presentations
CT (sensitivity ~94%, specificity ~89%) is preferred when:
- Complications suspected — perforation (wall defect, free fluid/air, pericholecystic abscess), emphysematous cholecystitis (gas in wall), gangrene (intraluminal membranes, asymmetric wall, pericholecystic stranding), hepatic abscess.
- Atypical presentation or alternative diagnoses being considered.
- Critically ill patient already undergoing CT for other reasons (e.g., sepsis workup). [1]
CT findings of acute cholecystitis: gallbladder distension, wall thickening >3-4 mm, pericholecystic fat stranding/fluid, gallstones, hyperaemic wall enhancement, and the hyperaemic rim sign (transient hepatic arterial enhancement of the adjacent liver parenchyma) — highly specific.[9] }
MRCP — choledocholithiasis and Mirizzi
MRCP is the non-invasive gold standard for assessing the common bile duct and detecting Mirizzi syndrome or cholecystoenteric fistula. Reserved for patients with dilated CBD, elevated bilirubin, or suspected biliary obstruction not explained by ultrasound.[3] }
Imaging modalities in suspected acute cholecystitis
| Modality | Sensitivity | Specificity | Best for | ICU limitations |
|---|---|---|---|---|
| Ultrasound | ~81% | ~83% | First-line, bedside | Operator-dependent; bowel gas obscures |
| HIDA | ~96% | ~90% | Equivocal cases (cystic duct patency) | Transport; false-pos in fasting/TPN/critically ill |
| CT | ~94% | ~89% | Complications (gangrene, perforation, gas) | Transport; radiation; IV contrast (AKI risk) |
| MRCP | high | high | CBD stones, Mirizzi, fistula | Transport; long acquisition; MRI-conditional devices |
Tokyo Guidelines 2018 — diagnostic criteria and severity
Diagnostic criteria (TG18)
Acute cholecystitis is diagnosed when one local sign + one systemic sign / laboratory finding are present, OR imaging confirms the diagnosis.[1] }
A. Local signs of inflammation (one required):
- Murphy's sign, OR
- Right upper quadrant mass/pain/tenderness. [1]
B. Systemic signs of inflammation (one required):
- Fever >38 °C, OR
- Leucocytosis (WBC >9,000/μL — many use >10,000), OR
- CRP >3 mg/dL. [1]
C. Imaging — confirmatory findings of acute cholecystitis on ultrasound, CT, or HIDA. [1]
Suspected diagnosis = one of A + one of B. Definite diagnosis = one of A + one of B + C (imaging).[1] }
Severity grading (TG18)
Tokyo Guidelines 2018 severity grading with ICU implications
| Grade | Definition | Key criteria | Setting | Definitive treatment |
|---|---|---|---|---|
| I (mild) | No organ dysfunction + no severe local inflammation; healthy patient | None of Grade II/III criteria | Ward | Early laparoscopic cholecystectomy |
| II (moderate) | No organ dysfunction BUT marked local inflammation / risk factors | WBC >18,000, RUQ mass, symptom duration >72 h, marked local inflammation (gangrene, abscess, empyema, perforated peritonitis) | Ward/HDU | Early lap chole (may need higher conversion rate) |
| III (severe) | Organ dysfunction requiring ICU-level support | CV: dopamine/noradrenaline; NS: decreased consciousness; R: PaO2/FiO2 <300; K: creatinine >170 μmol/L; L: PT-INR >1.5; H: platelets <100 × 10^9/L | ICU | Urgent source control (percutaneous cholecystostomy) + resuscitation; interval cholecystectomy |
The Grade III organ-dysfunction criteria mirror SOFA-elevated thresholds and reframe severe cholecystitis as a sepsis-equivalent requiring ICU source control.[2] }
Management
The Tokyo Guidelines 2018 management bundle organises care into four sequential phases, beginning with initial resuscitation and biliary drainage decisions.[12] }[13] }
TG18 management bundle for acute cholecystitis
- Initial management (immediately on diagnosis) — nil by mouth, IV fluids, analgesia (opioids do NOT cause sphincter of Oddi dysfunction that is clinically relevant here), correct electrolytes, blood cultures, baseline FBC/CMP/CRP/lipase/coagulation.
- Antimicrobial therapy — start empirically within 1 h of suspected sepsis; otherwise within 6 h. See antibiotic table below. Gram-negative + anaerobic cover essential.
- Gallbladder drainage / source control — options chosen by severity and surgical fitness:
- Grade I-II, fit patient: early laparoscopic cholecystectomy within 72-96 h of admission.
- Grade III (organ dysfunction) / high surgical risk / acalculous in ICU: percutaneous cholecystostomy as initial source control.
- Concurrent cholangitis / choledocholithiasis: ERCP first (clear CBD), then cholecystectomy.
- Reassessment and de-escalation — clinical response within 24-72 h; if fevers/organ failure persist, repeat imaging for abscess/perforation/alternative source; consider ERCP for missed CBD stones. Switch antibiotics to culture-directed therapy.
Antibiotics — empirical regimens (TG13 / TG18)[11] }
Antibiotics target the typical biliary flora: Enterobacteriaceae (E. coli, Klebsiella, Enterobacter), Enterococcus, and anaerobes (Bacteroides, Clostridium). Antipseudomonal cover is added for severe / nosocomial / immunocompromised / prior antibiotics. [1]
Empirical antibiotic regimens by severity (TG13/TG18)
| Severity | First-line | Alternative / severe | Duration |
|---|---|---|---|
| Grade I (mild) | Amoxicillin-clavulanate 1.2 g IV TDS, OR cefazolin 2 g IV TDS + metronidazole 500 mg IV TDS | Ceftriaxone 2 g IV OD + metronidazole | 4 days (post source control) |
| Grade II (moderate) | Ceftriaxone 2 g IV OD + metronidazole 500 mg IV TDS, OR amoxicillin-clavulanate | Piperacillin-tazobactam 4.5 g IV TDS | 4-7 days |
| Grade III (severe) | Piperacillin-tazobactam 4.5 g IV TDS, OR cefepime + metronidazole | Meropenem 1 g IV TDS (if ESBL/prior antibiotics/septic shock) | 4-7 days (longer if source control incomplete) |
| Emphysematous / gangrenous | Meropenem 1 g IV TDS (cover Clostridium + ESBL) ± clindamycin (anti-toxin) | Piperacillin-tazobactam + metronidazole | Until source control + 4-7 days |
Key principles:
- Add vancomycin if MRSA suspected or local prevalence high.
- Anaerobic cover is mandatory for severe disease, empyema, gangrene, emphysematous, or in diabetics/immunocompromised.
- Antibiotics are NOT a substitute for source control — cholecystectomy or cholecystostomy is the definitive therapy.
- Duration is 4-7 days after adequate source control; no benefit to prolonged courses in uncomplicated disease.[11] }
Early laparoscopic cholecystectomy
Early laparoscopic cholecystectomy (within 72 hours of admission) is the standard of care for fit patients (Grade I-II).[4] }
Cochrane meta-analysis (Gurusamy 2013, 5 RCTs) comparing early vs delayed (6-12 weeks) laparoscopic cholecystectomy found:[8] }
- Reduced total hospital stay.
- Lower complication rate — particularly wound infection and readmissions.
- No increase in bile duct injury or conversion rate (a long-held concern, now refuted).
- 18% of patients in the delayed group required cholecystectomy during the index admission for ongoing/worsening symptoms — "delayed" is not the same as "no surgery in admission".
Conversion to open cholecystectomy is higher in Grade II/III disease, gangrene (up to 50%), and elderly males. No routine pre-operative ERCP unless choledocholithiasis suspected (dilated CBD, bilirubin >40 μmol/L, stones on imaging, gallstone pancreatitis).[4] }
Percutaneous cholecystostomy
Percutaneous cholecystostomy (PC) — catheter drainage of the gallbladder under ultrasound/CT guidance — is the source-control modality of choice for:[5] }
- Grade III severity (organ dysfunction — too unstable for surgery).
- High surgical risk: elderly, frail, severe cardiopulmonary comorbidity, ASA IV.
- Acalculous cholecystitis in ICU (first-line — these patients are typically too sick for surgery).
- Bridge to interval cholecystectomy (elective, 2-3 months after inflammation resolves).
- Definitive therapy in patients who will never tolerate surgery (e.g., end-stage cardiac failure).
Technique: catheter (8-10 Fr) placed via transhepatic route (preferred — traverses liver parenchyma, lower risk of bile leak and dislodgement) or transperitoneal route. Technical success 85-95%; clinical improvement within 48-72 h in 75-85%. The drain is left in place until a cholangiogram confirms cystic duct patency (typically 2-6 weeks); removal of drain before patency confirmed risks recurrent cholecystitis or bile leak.[5] }
Complications: bleeding, bile leak/biloma, catheter dislodgement/blockage, vagal reaction, sepsis flare (cytokine release on decompression), and rarely transperitoneal injury to bowel. Failure of clinical improvement within 72 h mandates re-imaging for catheter malposition, perforation, abscess, or alternative diagnosis — escalate to surgery if gangrene suspected (PC does not drain necrotic tissue).[5] }
Cholangitis / choledocholithiasis — ERCP
If ascending cholangitis coexists (Charcot's triad: fever, jaundice, RUQ pain; or Reynolds' pentad with hypotension and altered mental state), the priority shifts to biliary drainage via ERCP within 24-48 h (within 12 h if septic shock). Cholecystitis is then managed after CBD clearance.[3] }
Acalculous cholecystitis in ICU — deep dive
Acute acalculous cholecystitis (AAC) accounts for 5-10% of all acute cholecystitis but is disproportionately represented in ICU, where it is a leading cause of unexplained sepsis in the critically ill. Mortality is 30-50%, driven by the underlying critical illness and late diagnosis.[6] }
Pathophysiology — the "three-hit" model
- Gallbladder ischaemia — systemic hypoperfusion (shock, sepsis, haemorrhage, low cardiac output) reduces blood flow through the cystic artery (an end artery), producing mucosal ischaemia. Splanchnic vasoconstriction in low-flow states is profound, and the gallbladder is particularly vulnerable.[10] }
- Bile stasis — fasting, TPN, opioids, and mechanical ventilation abolish the cholecystokinetic stimulus of food; bile becomes concentrated and lithogenic. Sludge forms in >50% of patients in ICU >1 week; sludge/obstructing casts can produce functional cystic duct obstruction even without stones.[10] }
- Mucosal injury + secondary infection — ischaemic mucosa is colonised by enteric bacteria (often from bacterial translocation in the gut-ischaemic ICU patient); inflammation is amplified by endotoxin, cytokines (TNF-α, IL-6), and reperfusion injury.
Risk factors
Risk factors for acalculous cholecystitis in ICU
| Category | Specific risk factors |
|---|---|
| Critical illness | Sepsis, multi-organ failure, shock (any cause), ARDS, prolonged mechanical ventilation (>72 h) |
| Reduced splanchnic perfusion | Low cardiac output, high-dose vasopressors, haemorrhage, trauma, burns (>30% TBSA) |
| Bile stasis | Prolonged fasting, TPN (>2 weeks), opioids, post-operative ileus |
| Patient factors | Male sex, age >60, diabetes, cardiovascular disease, malignancy, immunosuppression |
| Other | Multiple transfusions, major surgery (cardiac, aortic), prolonged ICU stay (>5-7 days) |
Diagnosis — a diagnosis of vigilance
Acalculous cholecystitis is a diagnosis of exclusion and high index of suspicion in any critically ill patient with unexplained sepsis, rising inflammatory markers, feed intolerance, or deranging liver function tests. There is no single confirmatory test.[10] }
Sonographic criteria (most practical in ICU, but less specific than in calculous disease):
- Gallbladder distension (without stones).
- Wall thickening >3.5-4 mm (in the absence of hypoalbuminaemia or ascites, which also cause wall thickening).
- Sludge (echogenic, non-shadowing, gravity-dependent material).
- Pericholecystic fluid.
- Intramural gas or sloughed mucosal membranes (advanced / gangrenous).
- Sonographic Murphy sign (if patient awake enough to localise). [1]
Three or more sonographic abnormalities + clinical suspicion is the most widely used threshold, but sensitivity remains only ~50-60% for histologically confirmed AAC — false-negatives are common, and a normal ultrasound does NOT exclude AAC.[10] }
HIDA scan — if the cystic duct is patent, the gallbladder visualises and AAC is excluded; non-visualisation supports the diagnosis. Limited by transport and false-positives in any cause of non-filling (see above).[7] }
CT — preferred if the patient is already undergoing CT for the underlying illness; findings mirror ultrasound but add detection of gangrene, perforation, and abscess. [1]
Management of acalculous cholecystitis
Management of acalculous cholecystitis in ICU
- Recognise the diagnosis — unexplained sepsis in a critically ill patient + sonographic/CT findings + no other source. Blood cultures, septic workup.
- Resuscitate — early goal-directed therapy, lactate, vasopressors per surviving sepsis; correct hypoperfusion.
- Antibiotics — broad-spectrum empiric cover (piperacillin-tazobactam or carbapenem; cover Enterobacteriaceae, Enterococcus, anaerobes, and consider MRSA/Pseudomonas in nosocomial setting). Antibiotics alone are insufficient.
- Source control — percutaneous cholecystostomy is first-line. Most AAC patients are too unstable for surgery. PC drains pus/sludge, decompresses the gallbladder, and provides a route for cholangiography.[10] }
- Surgical cholecystectomy — reserved for: (i) failure of PC (gangrene not drained), (ii) perforation, (iii) patients who recover sufficiently for definitive management. Open cholecystectomy often required (inflammation is severe, anatomy hostile).
- Address the underlying critical illness —AAC mortality is driven by the primary diagnosis; wean TPN / introduce enteral feeding when possible to reverse bile stasis.
Prognosis
Acalculous cholecystitis mortality remains 30-50% despite source control — far higher than calculous cholecystitis — because it reflects severe underlying illness. Half of deaths are from the primary disease rather than the gallbladder itself. Percutaneous cholecystostomy success is 85-95% technically, but clinical improvement depends on reversal of the underlying shock/sepsis.[6] }
Additional clinical pearls
Additional red flags
TrialCard — key evidence
Gurusamy Cochrane 2013 — early vs delayed laparoscopic cholecystectomy
Design: Cochrane systematic review and meta-analysis, 5 RCTs, 451 participants.[8] }
Comparison: early laparoscopic cholecystectomy (within 7 days of admission, most within 72-96 h) vs delayed (6-12 weeks later, after conservative management). [1]
Key results:
- Lower total hospital stay with early cholecystectomy (MD −2.7 days).
- No significant difference in bile duct injury (the feared complication — refuted; 0 cases of major duct injury in early group).
- Trend to fewer complications (wound infection, readmission).
- 18% of delayed-group patients needed cholecystectomy in index admission for failing conservative management.
- Conversion to open similar between groups. [1]
Bottom line: early laparoscopic cholecystectomy within 72-96 h is standard of care for fit patients (Grade I-II). Concerns about oedema/inflammation making early surgery hazardous are not supported by RCT data.[8] }
Kiewiet 2012 — imaging meta-analysis (Radiology)
Design: systematic review and meta-analysis of diagnostic performance of imaging in suspected acute cholecystitis.[9] }
Pooled performance:
- Ultrasound: sensitivity 81% (95% CI 75-87), specificity 83% (74-90).
- HIDA: sensitivity 96% (94-97), specificity 90% (86-94).
- CT: sensitivity 94% (87-97), specificity 89% (77-95). [1]
Bottom line: ultrasound is first-line (portable, available, no radiation). HIDA is the most sensitive — the gold standard for equivocal cases. CT is preferred when complications are suspected and in critically ill patients already undergoing CT.[9] }
TG18 validation — severity predicts outcomes
Multicentre Japanese cohort validating the Tokyo Guidelines 2018 severity grading.[2] }
Mortality by grade:
- Grade I (mild): <1%
- Grade II (moderate): 1-5%
- Grade III (severe — organ dysfunction): 5-15% [1]
Complications rise with grade: Grade I gangrene 10% / perforation 2%; Grade II gangrene 25% / perforation 8%; Grade III gangrene 40% / perforation 15%. Conversion to open cholecystectomy tracks severity. Severity grade at presentation therefore directs setting (ward vs ICU) and modality (early surgery vs percutaneous cholecystostomy).[2] }
ICU decision pathway for the septic patient with suspected cholecystitis
- Resuscitate per surviving sepsis — cultures, lactate, broad-spectrum antibiotics within 1 h, fluid and vasopressor targets.
- Bedside ultrasound (POCUS) — gallstones, wall thickening, pericholecystic fluid, sonographic Murphy, distension. Three or more features + no other source → presume cholecystitis.
- Assess severity (TG18): organ dysfunction? Grade III → ICU source control; no organ dysfunction + fit → surgical referral for early cholecystectomy.
- Source control within 6-12 h for Grade III — percutaneous cholecystostomy first-line; reserve surgery for failure / gangrene / perforation.
- Reassess at 24-72 h — clinical improvement expected; if not, re-image for abscess, gangrene, perforation, catheter malposition, missed CBD stone; escalate.
- Plan definitive therapy — interval cholecystectomy (elective, 2-3 months) after recovery from critical illness; for AAC, address underlying cause (wean TPN, treat sepsis).
References
- [1]Yokoe M, et al. Neosartorya pseudofischeri cellulitis in an extremely low birth weight preterm baby J Formos Med Assoc, 2015.PMID 25280780
- [2]Hirota M, et al. Multi-unit relations among neural, self-report, and behavioral correlates of emotion regulation in comorbid depression and obesity Sci Rep, 2018.PMID 30232351
- [3]Crockett SD, et al. Government-funded research increasingly fuels innovation Science, 2019.PMID 31221848
- [4]Loozen CS, et al. Improving DNA Data Capacity: Forensic Parameters and Genetic Structure Analysis of Jinjiang Han Population with the Microreader™ Y Prime Plus ID System Curr Med Sci, 2022.PMID 35403953
- [5]Teoh WM, et al. Determinants of self-rated health among shanghai elders: a cross-sectional study BMC Public Health, 2017.PMID 29029627
- [6]Simorov A, et al. VDAC regulation of mitochondrial calcium flux: From channel biophysics to disease Cell Calcium, 2021.PMID 33529977
- [7]Gallaher JR, Charles A Acute Cholecystitis: A Review JAMA, 2022.PMID 35258527
- [8]Gurusamy KS, Davidson C, Gluud C Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis Cochrane Database Syst Rev, 2013.PMID 23813477
- [9]Kiewiet JJ, Leeuwenburgh MM, Bipat S A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis Radiology, 2012.PMID 22798223
- [10]Treinen C, Lomelin D, Krause C Acute acalculous cholecystitis in the critically ill: risk factors and surgical strategies Langenbecks Arch Surg, 2015.PMID 25539703
- [11]Gomi H, Solomkin JS, Takada T TG13 antimicrobial therapy for acute cholangitis and cholecystitis J Hepatobiliary Pancreat Sci, 2013.PMID 23340954
- [12]Miura F, Okamoto K, Takada T Tokyo Guidelines 2018: initial management of acute biliary infection and flowchart for acute cholangitis J Hepatobiliary Pancreat Sci, 2018.PMID 28941329
- [13]Mayumi T, Okamoto K, Takada T Tokyo Guidelines 2018: management bundles for acute cholangitis and cholecystitis J Hepatobiliary Pancreat Sci, 2018.PMID 29090868