ICU · GI/Nutrition
Acute mesenteric ischaemia
Also known as Mesenteric ischaemia · Bowel ischaemia · Intestinal infarction · Non-occlusive mesenteric ischaemia (NOMI) · SMA embolism · Mesenteric venous thrombosis
Acute mesenteric ischaemia is a life-threatening vascular emergency of the bowel. Four types: (1) SMA embolus (1 — atrial fibrillation, 50%), (2) SMA thrombosis (pre-existing atherosclerosis, 25%), (3) Non-occlusive (NOMI — low-flow state, 20%), (4) Mesenteric venous thrombosis (5%). Presents with SEVERE abdominal pain OUT OF PROPORTION to examination findings. Diagnosis: CT angiography (gold standard — shows occlusion, bowel wall thickening, pneumatosis, portal venous gas). Lactate elevated (late sign — bowel infarction). Management by type: emboli to embolectomy, thrombosis to bypass/stent, NOMI to intra-arterial papaverine, venous thrombosis to anticoagulation. Mortality 50-80% overall, highest for SMA thrombosis. WSES staging guides operative vs endovascular strategy. Time is bowel.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
The four types at a glance
SMA embolus (#1)
50% — atrial fibrillation
- Most common type
- Embolic source: atrial fibrillation (LA thrombus), post-MI mural thrombus, valvular vegetations, paradoxical (DVT + PFO), aortic atherosclerotic debris
- Sudden onset severe pain (embolus occludes a previously normal artery — no collaterals)
- Point of occlusion: usually distal to middle colic artery (spares proximal SMA territory and proximal jejunum)
- Risk factors: AF, recent MI, prosthetic valve, endocarditis
- Mortality 50-70%
SMA thrombosis
25% — atherosclerosis
- In-situ thrombosis on a ruptured atherosclerotic plaque
- Almost always at the **origin** of the SMA — sacrifices the entire SMA territory
- Often preceded by chronic mesenteric angina (post-prandial pain, food fear/sitophobia, weight loss)
- Less acute onset than embolic (collaterals from coeliac/IMA may have developed)
- Strong association with coronary, peripheral and aortic atherosclerosis
- Highest mortality of the four (70-90%)
NOMI
20% — low-flow state
- Non-Occlusive Mesenteric Ischaemia — diffuse splanchnic vasospasm, NO mechanical occlusion
- Causes: cardiogenic shock, severe heart failure, sepsis, haemodialysis, digoxin toxicity (classic), high-dose α-agonists, severe aortic stenosis/regurgitation
- Most common in ICU patients with shock on escalating vasopressors
- Angiography: diffuse spasm, "string-of-sausages" alternating calibre, narrowed origin, impaired venous filling
- Treatment: address the low-flow cause, intra-arterial **papaverine** infusion, wean vasopressors, add milrinone
- Mortality 50-80%
Mesenteric venous thrombosis
5%
- Thrombosis of the superior mesenteric vein (most common); portal/splenic veins may be involved
- Causes (Virchow triad): hypercoagulable (JAK2, protein C/S, antithrombin, FVL, antiphospholipid, malignancy), stasis (cirrhosis/portal hypertension, splenomegaly, CHF), endothelial injury (pancreatitis, intra-abdominal sepsis, surgery, IBD)
- Slower onset, less severe pain, often well compensated
- CT: venous filling defect, mesenteric stranding, ascites, thickened oedematous bowel wall
- Treatment: anticoagulation (heparin then warfarin/DOAC), investigate thrombophilia, surgery only if infarction
- Best prognosis of the four (mortality 20-30%)
Mesenteric vascular anatomy (know this for the viva)
[4] [4]Collateral circulation and the two watershed points
The bowel is normally protected by rich collaterals — failure of these is what produces ischaemia in low-flow states:[2]
- Coeliac–SMA anastomosis: the pancreaticoduodenal arcade (superior pancreaticoduodenal from the gastroduodenal artery anastomoses with the inferior pancreaticoduodenal from the SMA) around the head of the pancreas. This is the route that compensates when the SMA origin is chronically occluded.
- SMA–IMA anastomosis: the marginal artery of Drummond (runs along the mesenteric border of the colon) and the more centrally placed meandering mesenteric artery (arc of Riolan), a shorter, larger-calibre shortcut between the middle colic and left colic arteries.
- IMA–internal iliac anastomosis: via the superior, middle and inferior rectal arteries (the basis for sparing the rectum in mesenteric revascularisation).[4]
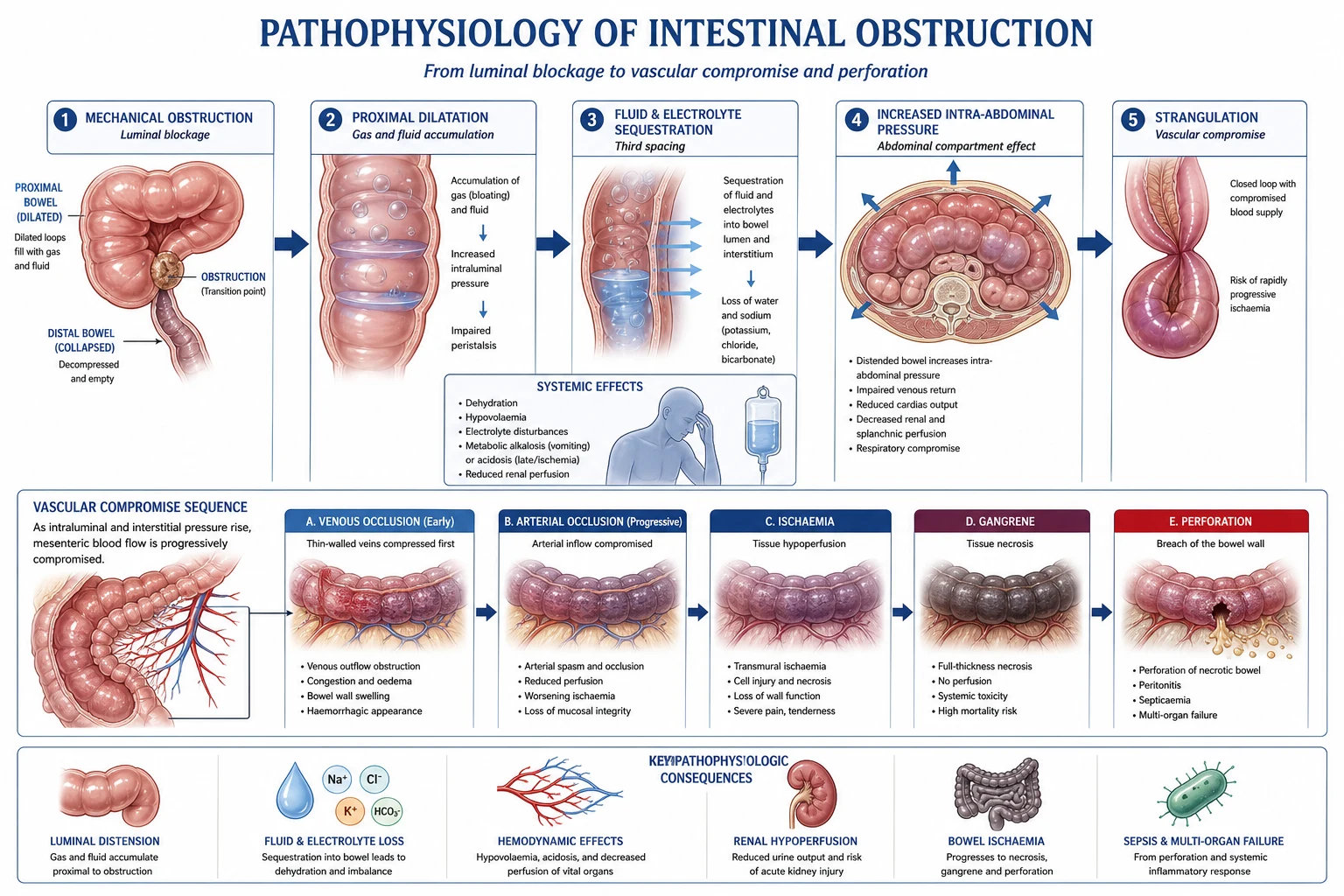
Pathophysiology — why "time is bowel"
The ischaemic cascade
Reduction in splanchnic perfusion
Arterial occlusion (embolus/thrombus), venous obstruction (outflow failure causes congestion and secondarily reduces inflow), or a low-flow state triggers the lesion. The bowel also auto-regulates poorly under shock.
Reflex mesenteric vasoconstriction
A fall in perfusion pressure activates the **sympathetically-mediated splanchnic vasoconstriction** (and the renin-angiotensin system). This is meant to preserve central blood pressure but worsens bowel ischaemia — it is the mechanism that turns a transient low-flow insult into NOMI and why α-agonists are so harmful.
Mucosal injury (first to suffer)
The mucosa has the highest metabolic demand and is fed by the most distal vasa recta. It sloughs first — producing **bloody diarrhoea** and protein loss within 1-2 h. Mucosal barrier loss allows bacterial translocation.
Reperfusion injury
Restoration of flow delivers oxygen that fuels xanthine-oxidase-driven **reactive oxygen species**, neutrophil activation, complement and cytokine release. Reperfusion can extend rather than limit injury — relevant to second-look decision-making and to the systemic inflammatory response after embolectomy.
Progression outward: mucosa to serosa
Ischaemia extends outward from mucosa to submucosa to muscularis to serosa. The muscularis becomes ischaemic around 4-6 h; transmural (full-thickness) infarction with **perforation and peritonitis** follows at ~6-10 h (highly variable). The pain paradoxically diminishes as the visceral afferents themselves become ischaemic — a worsening, not an improvement.
Transmural infarction and shock
Bacterial translocation, third-space loss, gastrointestinal bleeding, perforation and septic shock. Mortality is now chiefly driven by multi-organ failure rather than the bowel itself.
Clinical presentation — the diagnosis made at the bedside
The three clinical phases of AMI (know the timeline)
> 12 h — peritonitis and shock
Transmural infarction. Diffuse peritonism (rigidity, guarding, rebound), septic shock, metabolic acidosis with high lactate, oliguria, multi-organ failure. Surgical mortality is now dominated by MOF rather than by the bowel itself. Pneumatosis and portal venous gas are usually visible by now.
Symptoms and signs by type
SMA embolus
acute, dramatic
- Sudden catastrophic pain, no warning, patient previously well
- Pain out of proportion is most pronounced here
- Forceful bowel evacuation (diarrhoea, sometimes bloody)
- History of AF, recent MI, prosthetic valve, endocarditis
- Minimal abdominal signs early; peritonitis only once transmural
SMA thrombosis
subacute, post-prandial history
- More gradual onset over hours; may be preceded by weeks of post-prandial pain
- Classic chronic mesenteric angina history: **food fear (sitophobia)**, weight loss, post-prandial periumbilical pain 15-30 min after eating
- Epigastric bruit may be audible
- Known atherosclerotic disease (CAD, PAD, prior stroke)
- Often more diffuse tenderness at presentation (slowly progressive infarction)
NOMI
insidious in the ICU
- Patient is already critically ill — pain is often unrecognised or absent (sedated/ventilated)
- Presenting features: unexplained **rising lactate**, abdominal distension, oliguria, new metabolic acidosis, increasing vasopressor requirement
- Often first suspected on a CT performed for "septic workup"
- History of cardiogenic shock, dialysis, digoxin, escalating α-agonists
- Pain often minimal because the patient cannot report it
Mesenteric venous thrombosis
subacute, indolent
- Insidious onset over days; pain is duller and less catastrophic
- Anorexia, nausea, non-specific abdominal discomfort
- May present with complications: upper GI bleeding, ascites, or as an incidental CT finding
- Look actively for: known thrombophilia, portal hypertension/cirrhosis, recent pancreatitis, intra-abdominal sepsis, OCP/pregnancy, personal/family VTE history
- Often haemodynamically stable at presentation
Investigations — order and interpretation
Diagnostic algorithm (minutes matter)
Recognise the pattern and call the surgeon
Severe pain out of proportion OR an ICU patient with unexplained rising lactate and distension. Phone the on-call vascular/general surgeon and interventional radiology AT THE SAME TIME as ordering the CT — do not wait for a result before alerting them.
Blood panel (supportive, not diagnostic)
Venous gas (lactate, pH, base excess); FBC (WCC typically above 15); U&E, amylase/lipase (may be elevated — confusing with pancreatitis); CK and LDH (non-specific); phosphate (often raised in mucosal ischaemia); D-dimer (high sensitivity, low specificity — useful only if NORMAL, in which case AMI is very unlikely); group and save; coagulation; cross-match.
ECG
Look for AF (the commonest cause of embolic AMI), recent MI (Q waves, evolving changes), evidence of structural heart disease. Transthoracic echo at the bedside if a cardiac source is suspected.
CT ANGIOGRAPHY — the gold standard
IV contrast only, ARTERIAL and VENOUS phase, NO oral contrast (it delays diagnosis, may worsen distension and obscure vascular contrast). Request the study explicitly as "CTA mesenteric vessels — query acute mesenteric ischaemia" so the radiologist obtains the correct protocol.
Mesenteric angiography (selected)
Reserved for **therapeutic** use — selective SMA catheterisation for intra-arterial **papaverine** in NOMI, or for catheter-directed thrombolysis/thrombectomy in selected embolic occlusions without peritonism. No longer a first-line diagnostic test.
Do NOT delay
The single most defensible position is: any patient in whom AMI is genuinely suspected gets a CTA within the hour. A "wait and see" approach with serial lactates is the single largest contributor to the persistently high mortality of this disease.
CT findings — the radiology you must be able to read
Vascular (arterial phase)
the cause
- Filling defect / abrupt cut-off in the SMA — embolus typically distal to the middle colic origin
- Occlusion at the SMA origin with proximal calcified plaque — thrombosis
- Calcification and stenosis of multiple mesenteric vessels — chronic disease
- Aortic atherosclerotic debris — potential embolic source
Vascular (venous phase)
MVT
- Filling defect in the SMV / portal vein
- Mesenteric stranding and engorged vasa recta
- Splenic/portal vein thrombosis may coexist
- Ascites is common and often striking
Bowel wall
the consequence
- **Bowel wall thickening** (small bowel greater than 3 mm, colon greater than 6 mm) — the commonest but LEAST specific sign
- **Absent / diminished wall enhancement** after IV contrast — SPECIFIC for transmural ischaemia/infarction
- **"Target" / "double-halo" sign** — trilaminar enhancement (submucosal oedema between enhancing mucosa and serosa) — early, often reversible
- **Paper-thin atrophic wall** — late, ominous, indicates irreversible infarction
- Dilated, fluid-filled, atonic loops — paralytic ileus
Gas (late, grave)
transmural infarction
- **Pneumatosis intestinalis** — gas in the bowel wall (linear, bubbly or cystic). Indicates transmural infarction but is occasionally benign.
- **Portal venous gas** — gas in the intrahepatic portal branches (peripheral, branching). Very late sign; very poor prognosis.
- **Pneumoperitoneum** — perforation. Immediate laparotomy.
NOMI-specific
no mechanical occlusion
- Diffuse, often mild bowel wall thickening and dilatation
- Narrowed origins of SMA and coeliac branches
- Alternating dilatation/narrowing of mesenteric arcades ("string of sausages")
- Impaired / absent venous filling in the mesenteric phase
- Diagnosis often rests on angiographic appearances rather than CTA
Lactate and biomarkers in context
Biomarkers in acute mesenteric ischaemia
Diagnosis — the worked diagnostic approach
Diagnostic approach
Recognise the pattern
Severe abdominal pain OUT OF PROPORTION to physical findings. Patient writhing in pain but abdomen soft, non-tender (early — before infarction). Vomiting, diarrhoea (may be bloody) common. Risk factors: AF (#1), atherosclerosis, heart failure, recent MI, dialysis, digoxin, high-dose vasopressors, hypercoagulable state.
Bloods (supportive, not diagnostic)
Lactate: elevated (over 2 mmol/L) — BUT this is a LATE sign (indicates transmural infarction). Do NOT wait for lactate to rise. WBC: typically elevated (over 15). Metabolic acidosis (late). CK, amylase, LDH, phosphate may be elevated. D-dimer: non-specific but high negative predictive value.
CT angiography (GOLD STANDARD)
IV contrast, arterial and venous phase. Shows: arterial occlusion (filling defect in SMA), bowel wall thickening, pneumatosis intestinalis (air in bowel wall = infarction), portal venous gas (late, poor prognosis), mesenteric stranding (venous thrombosis). AVOID oral contrast (delays diagnosis, may worsen bowel distension).
Other imaging (if CT unavailable)
CT with IV contrast (less ideal than CTA). Mesenteric angiography (gold standard historically, but invasive — reserved for therapeutic papaverine infusion or selective thrombolysis).
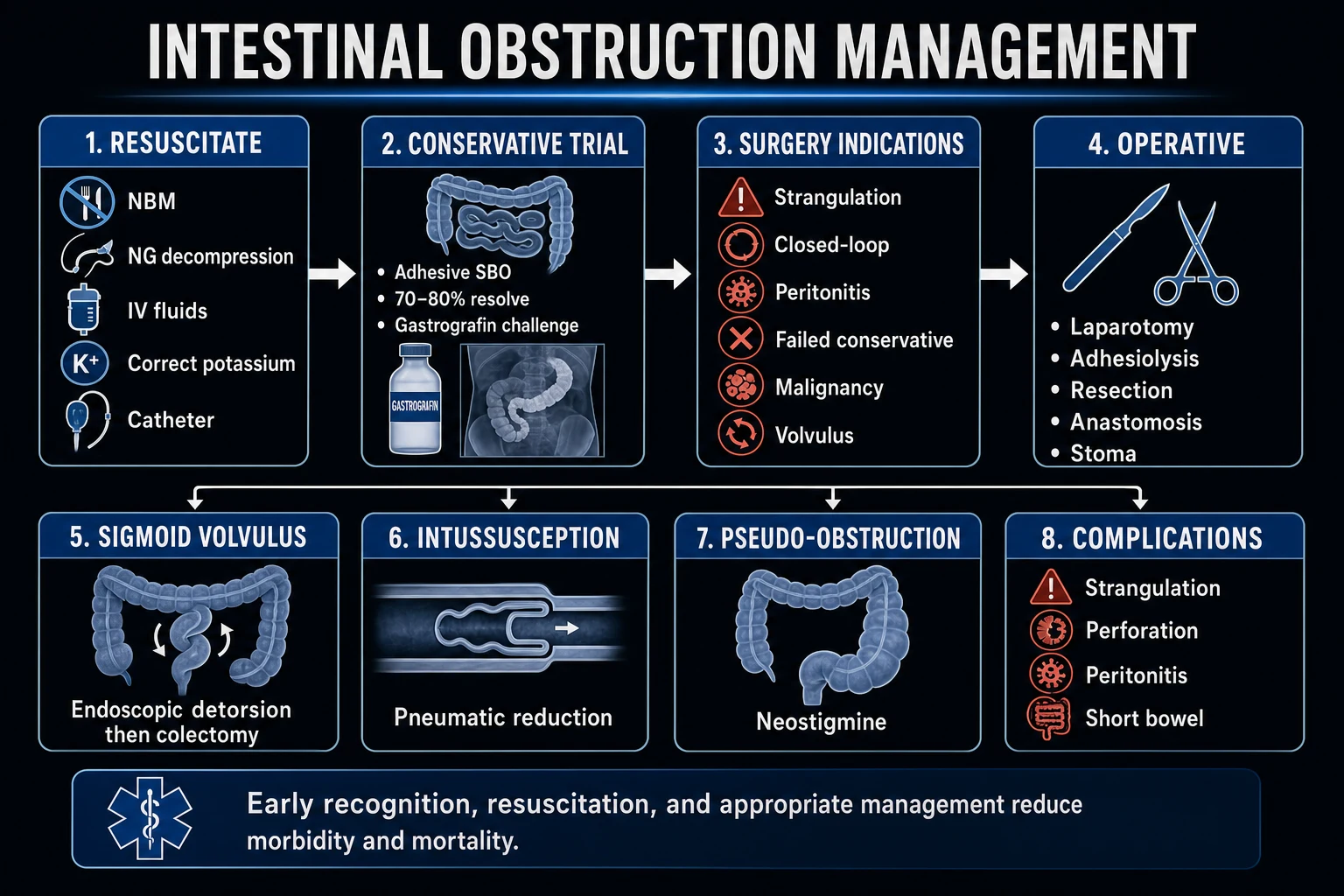
Management — the general bundle for ALL types
Mesenteric ischaemia management — applies to every phenotype
Resuscitation
ABC. IV crystalloid cautiously (avoid overload — these patients develop pulmonary oedema easily and the trial evidence in sepsis favours moderate over aggressive fluids). Correct hypotension. Vasopressors may WORSEN mesenteric perfusion — use the lowest effective noradrenaline, and add **dobutamine** (β — raises cardiac output) or **milrinone** (PDE3 inodilator) preferentially. Broad-spectrum antibiotics covering bowel flora (e.g. piperacillin-tazobactam). Nasogastric decompression. Urinary catheter.
Anticoagulation
IV unfractionated heparin (unless contraindicated by active bleeding or imminent surgery). Prevents thrombus propagation, reduces recurrent embolism and limits venous thrombus extension. Target aPTT 1.5-2.5x normal. Continue peri-operatively — do NOT stop heparin for surgery, simply time it. UFH is preferred because it is rapidly reversible with protamine. Therapeutic anticoagulation for mesenteric venous thrombosis is the definitive treatment.
Urgent surgery if infarction suspected
Indications: peritonism (rigidity, guarding — bowel is transmurally infarcted), pneumatosis or portovenous gas on CT, worsening metabolic acidosis, haemodynamic instability. Surgery: laparotomy, assess bowel viability (colour, peristalsis, palpable mesenteric pulse, Doppler, fluorescein/ICG), resect frankly infarcted segments. The "revascularise first" principle: in occlusive disease, restore flow BEFORE committing to resection, so that borderline bowel recovers. Plan a **second-look laparotomy at 24-48 h** for any doubtful segment.
Endovascular therapy (selected cases)
Intra-arterial **papaverine** (vasodilator) for NOMI — infused via SMA catheter placed during angiography. Catheter-directed **thrombolysis** or **thrombectomy** for selected cases of acute embolic occlusion WITHOUT peritonism. **Stenting** for proximal SMA stenosis/thrombosis (preferred over bypass if no peritonism and expertise available).
Manage the underlying cause
AF: anticoagulate long-term (CHA₂DS₂-VASc). Heart failure: optimise cardiac output, consider mechanical support. Digoxin toxicity: stop, consider Digifab. Sepsis: source control and resuscitation. Hypercoagulable: investigate and treat. Stop causative vasoconstrictors if possible.
Management by type — the viva-critical detail
1. SMA embolus — embolectomy first
SMA embolus
Diagnosis
Sudden severe pain in a patient with AF (or other embolic source); CTA shows an occlusion in the SMA **distal to the middle colic artery origin** (pathognomonic — proximal SMA and proximal jejunum are spared).
If no peritonism
Endovascular **thrombolysis** or **percutaneous thrombectomy** via selective SMA catheter is increasingly first-line in centres with expertise. Systemic thrombolysis is generally avoided (bleeding risk and inferior outcomes).
If peritonism OR endovascular unavailable
Surgical **embolectomy**: Fogarty balloon catheter via a transverse arteriotomy in the SMA (exposed at the root of the mesentery). Revascularise BEFORE resection. After flow is restored, observe the bowel for 15-20 min and resect only what is frankly dead.
Second-look
Plan a mandatory **second-look laparotomy at 24-48 h** to reassess borderline segments — this is not optional in most units.
Long-term
Lifelong anticoagulation (the embolic source — usually AF — has not gone away). Treat the cardiac source (rate/rhythm control, cardioversion, valvular surgery).
2. SMA thrombosis — bypass or stent
SMA thrombosis
Diagnosis
Occlusion at the SMA **origin** with adjacent atherosclerotic calcification; collateral vessels (pancreaticoduodenal arcade, arc of Riolan) may be enlarged if chronic-on-acute. Ask about food fear and weight loss.
No peritonism
Endovascular **stenting** of the SMA origin is preferred where expertise exists — lower morbidity than open bypass, immediate restoration of flow, and can be combined with thrombus aspiration.
Peritonism or endovascular failure
Surgical **bypass** from the aorta or common iliac artery to the SMA distal to the occlusion, using **reversed saphenous vein** (preferred) or PTFE. Retrograde bypass from the iliac is technically easier than antegrade from the supracoeliac aorta. Revascularise before resection; mandatory second-look.
Why this type has the worst mortality
Because the occlusion is at the origin, the **entire SMA territory** is at risk from the outset and pre-existing collaterals, even if developed, are often inadequate to prevent infarction of a large midgut segment. Mortality is 70-90%.
3. NOMI — papaverine and the low-flow state
NOMI
Recognise
ICU patient with cardiogenic shock, dialysis, digoxin toxicity or escalating α-agonists; rising lactate, distension, metabolic acidosis. CTA may show only diffuse bowel wall thickening; definitive diagnosis is often angiographic.
Angiographic hallmark
Narrowed origins of SMA and coeliac branches, alternating dilatation/narrowing of mesenteric arcades ("string of sausages"), impaired filling of peripheral mesenteric branches and sluggish venous phase.
Intra-arterial papaverine
**30-60 mg/h** of papaverine infused continuously via a catheter placed selectively in the SMA at angiography, for **24-48 h**. Repeat angiography to confirm resolution of vasospasm before withdrawal. Papaverine is metabolised on first pass through the liver, so systemic effects are minimal — but watch for hypotension and hepatic dysfunction.
Treat the underlying low-flow state
Reverse cardiogenic shock (inotropes, mechanical support if needed); stop digoxin (consider Digifab if toxicity); review the dialysis prescription (avoid intradialytic hypotension, consider sustained low-efficiency dialysis); **wean α-agonists** and substitute milrinone or dobutamine.
When to operate
Surgical exploration is reserved for those who develop peritonism (transmural infarction). Surgery does not treat the vasospasm — papaverine does.
4. Mesenteric venous thrombosis — anticoagulate and investigate
Mesenteric venous thrombosis
Diagnosis
CT venous phase shows a filling defect in the SMV (and often portal/splenic veins), mesenteric stranding, ascites and thickened congested bowel wall. Lower index of suspicion in patients with cirrhosis, pancreatitis, recent intra-abdominal sepsis, or known thrombophilia.
Anticoagulation
Therapeutic **unfractionated heparin** initially (rapidly reversible if surgery becomes necessary), transitioning to **warfarin or a DOAC for 3-6 months** (lifelong if a persistent prothrombotic state such as JAK2, antiphospholipid syndrome or active malignancy).
Investigate the cause
Full **thrombophilia screen** (protein C, protein S, antithrombin, factor V Leiden, prothrombin gene mutation, antiphospholipid antibodies, JAK2 V617F), JAK2-driven myeloproliferative workup, malignancy screen (CT chest/abdomen/pelvis, age-appropriate endoscopy), review OCP use and portal hypertension.
Surgery
Reserved for infarction / peritonism — resect frankly necrotic bowel. Transjugular intrahepatic portosystemic shunt (TIPS) or surgical shunt may be considered for extensive portal/mesenteric thrombosis with portal hypertension.
Prognosis
Best of the four (mortality 20-30%). Long-term sequelae are dominated by portal hypertension, varices and short bowel if extensive resection was needed.
WSES classification and stage-based strategy
[8]WSES stage-based management
Stage 0/I (no peritonism, no necrosis)
Medical optimisation + revascularisation (endovascular first). NOMI: papaverine. MVT: anticoagulation. Embolus/thrombosis: thrombolysis, thrombectomy or stenting. Diagnostic laparoscopy if doubt remains about viability.
Stage II (localised peritonism / localised necrosis)
Surgical exploration: revascularise FIRST in occlusive disease, then resect frankly necrotic bowel, leave borderline segments, and plan a mandatory second-look at 24-48 h. Anticoagulation continued perioperatively.
Stage III (diffuse peritonism / extensive necrosis)
Emergency laparotomy, resect all non-viable bowel, damage-control open abdomen if physiology deranged, return to theatre for second-look and definitive stoma/closure once stabilised. Mortality extremely high; palliative involvement early may be appropriate.
Pharmacology in mesenteric ischaemia — what the examiner wants
Papaverine
benzylisoquinoline opium alkaloid
- **Mechanism**: non-selective phosphodiesterase inhibitor → ↑ intracellular cAMP → smooth-muscle relaxation → arteriolar vasodilatation
- **Use**: NOMI — intra-arterial infusion 30-60 mg/h into the SMA for 24-48 h
- **Pharmacokinetics**: rapid hepatic first-pass metabolism → minimal systemic levels when infused into the SMA (some systemic effect if it refluxes)
- **Adverse effects**: systemic hypotension, hepatic dysfunction (LFTs and amylase must be monitored — pancreatitis reported), flushing
- **Practical points**: must run via a dedicated central lumen/arterial line; do not mix with heparin in the same line (precipitate); continuous infusion only
Unfractionated heparin
the workhorse
- **Mechanism**: potentiation of antithrombin III → inactivation of thrombin (IIa) and factor Xa
- **Use**: ALL arterial phenotypes (prevents propagation and recurrent embolism); the DEFINITIVE treatment for mesenteric venous thrombosis
- **Dose**: weight-based bolus then infusion; target aPTT 1.5-2.5x control
- **Advantages over LMWH in AMI**: rapid onset, rapidly reversible with protamine, does not need renal dose adjustment, easy to interrupt for surgery
- **Adverse effects**: bleeding, heparin-induced thrombocytopenia (check platelets days 5-14), osteoporosis with prolonged use
Vasopressors and the mesentery
the trade-off
- **Noradrenaline** (α > β): mesenteric vasoconstriction, raises lactate — unavoidable in septic shock, use the LOWEST effective dose
- **Adrenaline**: marked α effects, lactate elevated by direct glycolysis — confounds AMI monitoring
- **Vasopressin**: intense splanchnic vasoconstriction — AVOID if AMI suspected
- **Dobutamine** (β1): raises cardiac output and splanchnic flow — preferred inotrope in AMI
- **Milrinone** (PDE3): inodilator, reduces afterload and improves mesenteric perfusion — useful adjunct
- **Principle**: there is no safe vasopressor in AMI; the goal is to resolve shock so vasopressors can be weaned, not to find a "mesentery-friendly" agent
Chronic mesenteric ischaemia (intestinal angina) and ischaemic colitis
Chronic mesenteric ischaemia
[4]Chronic mesenteric ischaemia
Clinical syndrome
Post-prandial periumbilical pain 15-30 min after eating, **food fear (sitophobia)**, progressive weight loss, sometimes diarrhoea from mucosal ischaemia. Epigastric bruit in ~50%. Patients often undergo extensive negative GI workup before the diagnosis is made.
Diagnosis
**Duplex ultrasound**: peak systolic velocity in the SMA greater than 275 cm/s correlates with over 70% stenosis; PSV in the coeliac greater than 200 cm/s. **CTA or MRA** confirms anatomy. Catheter angiography with pressure gradient measurement reserved for equivocal cases or before intervention.
Treatment
**Prophylactic revascularisation** to prevent acute thrombotic occlusion (which carries the worst mortality of all AMI phenotypes). **Endovascular stenting** is first-line (lower morbidity); surgical bypass reserved for endovascular failure, complex anatomy or restenosis.
Why it matters in the ICU
A patient with undiagnosed chronic mesenteric angina who presents with superimposed acute-on-chronic thrombosis is the classic "SMA thrombosis" phenotype — the worst-prognosis form of AMI. Asking about food fear and weight loss in any older patient with atherosclerosis pays dividends.
Ischaemic colitis — the related but distinct entity
Ischaemic colitis
a different beast
- The MOST COMMON form of intestinal ischaemia (overall) — but usually a self-limited mucosal/submucosal event, not a surgical emergency
- Affects the COLON — classically the watershed zones (**Griffith's point** at the splenic flexure, **Sudeck's point** at the rectosigmoid); the rectum itself is usually spared (dual internal iliac supply)
- Presentation: **painless or crampy LEFT LOWER QUADRANT pain with mild-to-moderate BLOODY DIARRHOEA** within 24 h
- Common in older patients after low-flow events: dialysis, major surgery, dehydration, hypotension, marathon running, vasoactive drugs
- CT: segmental thickening of the left colon with thumbprinting; colonoscopy (if performed) shows segmental mucosal haemorrhage and ulceration
- Management: SUPPORTIVE (fluids, broad-spectrum antibiotics, bowel rest) — most resolve in 1-2 weeks. Segmental resection reserved for fulminant colitis, perforation or stricture (occurs in ~10-20%)
Acute mesenteric ischaemia (this topic)
the surgical emergency
- Affects the SMALL BOWEL (midgut) — high-grade, transmural, time-critical
- Hallmark: pain out of proportion; colon and rectum typically spared
- Surgical / endovascular emergency; mortality 50-80%
- Driven by SMA embolus/thrombus/NOMI — not the low-grade low-flow that causes ischaemic colitis
Evidence and trials
Schoots et al. systematic review
British Journal of Surgery 2004
Systematic review of cohort studies reporting survival after AMI by aetiology (embolus, thrombosis, NOMI, venous)
Key finding
Pooled mortality: SMA embolus ~54%, SMA thrombosis ~77%, NOMI ~73%, MVT ~32%. Confirmed that SMA thrombosis carries the worst prognosis and MVT the best; mortality had changed little over the preceding decades despite imaging advances
Practice change
Established the modern mortality benchmarks used in the WSES guidelines and in every exam answer
Block et al. US national inpatient analysis
Journal of Vascular Surgery 2016
Analysis of a large US national inpatient database comparing mortality of acute mesenteric artery embolism vs thrombosis
Key finding
Acute thrombosis carried significantly higher mortality than embolism, even after adjustment for comorbidity, because of the more extensive territory infarcted and later presentation
Practice change
Reinforces the need to identify chronic mesenteric angina prophylactically — the only way to reduce thrombotic AMI mortality
Endovascular-first observational studies
Vascular and Endovascular Surgery 2017 and others
Multiple single- and multi-centre cohort studies of percutaneous stenting / thrombolysis / thrombectomy for acute and acute-on-chronic occlusive AMI
Key finding
In selected patients WITHOUT peritonism, an endovascular-first strategy achieves technical success rates over 85% with lower 30-day mortality than open surgery; surgical bypass remains the rescue strategy
Practice change
Endovascular therapy now first-line for occlusive AMI without transmural infarction in centres with capability
D-dimer in AMI systematic review
European Journal of Gastroenterology and Hepatology 2017
Systematic review of D-dimer as a screening test for AMI
Key finding
Sensitivity ~95-99% but specificity only ~40-50% — a NORMAL D-dimer makes AMI very unlikely; an elevated D-dimer is non-diagnostic
Practice change
D-dimer is a rule-OUT test only; cannot be used to confirm AMI or to justify delay in CTA
2019 WSES guidelines
World Journal of Emergency Surgery 2019
International consensus guideline using modified GRADE methodology on classification, diagnosis and management of AMI
Key finding
Standardised AMI into Stages 0-III based on peritonism and radiological necrosis; endorsed CT angiography as the diagnostic gold standard; recommended endovascular-first in selected stages and the "revascularise first" principle at surgery
Practice change
WSES staging now the universal framework for AMI decision-making and a common viva structure
Prognosis
Mortality by AMI phenotype (Schoots 2004; Block 2016)
Mesenteric ischaemia outcomes — high-yield summary
Complications and the post-operative ICU course
After the operation — what kills these patients
Reperfusion injury and SIRS
Restoring flow to ischaemic bowel releases potassium, lactate, acid, cytokines and myocardial depressant factors — expect a transient cardiovascular and metabolic storm in the first hours after embolectomy/bypass. Anticipate vasopressor escalation, arrhythmia and hyperkalaemia.
Short bowel syndrome
Extensive small-bowel resection (especially loss of the ileocaecal valve and colon) produces intestinal failure: diarrhoea, dehydration, electrolyte loss, malabsorption, gallstones (loss of ileal bile salt reabsorption), and renal oxalate stones. Lifelong parenteral nutrition; refer early to an intestinal rehabilitation / transplant centre.
Anastomotic leak
Primary anastomosis in ischaemic bowel is high-risk — most surgeons favour **stoma** formation or Hartmann's-type procedures at the index operation, with reversal only after full recovery.
Abdominal compartment syndrome
Massive fluid resuscitation and bowel oedema raise intra-abdominal pressure; monitor bladder pressure and consider a prophylactic open abdomen (negative-pressure dressing) at the index operation.
Multi-organ failure and sepsis
The late cause of death in most series. Source control, lung-protective ventilation, renal replacement therapy and tailored antimicrobials drive outcome.
Mnemonics for the exam
[12] [9]Worked viva question (CICM / FFICM Second Part style)
SAQ — Acute mesenteric ischaemia in a patient with atrial fibrillation
10 minutes · 10 marks
A 72-year-old woman with permanent atrial fibrillation (on apixaban 5 mg bd, missed for 5 days post-fall), hypertension and type 2 diabetes presents to the emergency department with two hours of severe, constant periumbilical pain. She is writhing and distressed. Examination: HR 112 irregularly irregular, BP 95/60, RR 22, SpO₂ 96% room air, temperature 36.8 °C. The abdomen is soft and non-tender with active bowel sounds. Venous gas: pH 7.30, lactate 2.4 mmol/L, base excess −4. WCC 17.4, CRP 12. ECG confirms AF rate 112. An abdominal X-ray is unremarkable.
Clinical pearls
Red flags
References
- [1]Fuglseth H, Søreide K, Vetrhus M Acute mesenteric ischaemia. The British journal of surgery, 2023.PMID 36748996
- [2]Reintam Blaser A, Coopersmith CM, Acosta S Managing acute mesenteric ischaemia. Intensive care medicine, 2024.PMID 38478026
- [3]Bala M, Catena F, Kashuk J, et al. Acute mesenteric ischemia: updated guidelines of the World Society of Emergency Surgery. World journal of emergency surgery : WJES, 2022.PMID 36261857
- [4]Kougias P, Huynh TT, Lin PH Clinical outcomes of mesenteric artery stenting versus surgical revascularization in chronic mesenteric ischemia. International angiology : a journal of the International Union of Angiology, 2009.PMID 19367243
- [5]Schoots IG, Koffeman GI, Legemate DA, et al. Systematic review of survival after acute mesenteric ischaemia according to disease aetiology. The British journal of surgery, 2004.PMID 14716789
- [6]Acosta S, Salim S Management of Acute Mesenteric Venous Thrombosis: A Systematic Review of Contemporary Studies. Scandinavian journal of surgery : SJS : official organ for the Finnish Surgical Society and the Scandinavian Surgical Society, 2021.PMID 33118463
- [7]Tamme K, Reintam Blaser A, Laisaar KT, et al. Incidence and outcomes of acute mesenteric ischaemia: a systematic review and meta-analysis. BMJ open, 2022.PMID 36283747
- [8]Reintam Blaser A, Starkopf J, Björck M, et al. Diagnostic accuracy of biomarkers to detect acute mesenteric ischaemia in adult patients: a systematic review and meta-analysis. World journal of emergency surgery : WJES, 2023.PMID 37658356
- [9]Srisajjakul S, Prapaisilp P, Bangchokdee S Comprehensive review of acute small bowel ischemia: CT imaging findings, pearls, and pitfalls. Emergency radiology, 2022.PMID 35122558
- [10]Reintam Blaser A, Coopersmith CM, Acosta S Managing acute mesenteric ischaemia. Intensive care medicine, 2024.PMID 38478026
- [11]Singal AK, Kamath PS, Tefferi A Mesenteric venous thrombosis. Mayo Clinic proceedings, 2013.PMID 23489453
- [12]MacCannell KL Comparison of an intravenous selective mesenteric vasodilator with intraarterial papaverine in experimental nonocclusive mesenteric ischemia. Gastroenterology, 1986.PMID 3710084