ICU · Antimicrobial Stewardship
Acute severe community-acquired pneumonia: infection control in ICU
Also known as Infection control in ICU · Nosocomial infection prevention · ICU hygiene · Isolation precautions
Infection control in ICU prevents transmission of pathogens between patients, staff, and the environment. Core components: (1) Hand hygiene (WHO 5 Moments — single most effective measure). (2) Standard precautions (for ALL patients — gloves, gown, eye protection when exposure risk). (3) Transmission-based precautions: contact (MRSA, VRE, C. diff, MDR), droplet (influenza, RSV, pertussis), airborne (TB, measles, chickenpox). (4) Environmental cleaning (high-touch surfaces, terminal cleaning). (5) Equipment cleaning/disinfection (dedicated equipment for isolated patients). (6) Surveillance (MDR screening cultures, infection rates). (7) Staff education and audit. (8) Antimicrobial stewardship. ICU infection rate is a quality metric — lower is better.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

SAQ — outbreak investigation in the ICU
SAQ — ICU outbreak: carbapenem-resistant Klebsiella (CRE) in the ICU
10 minutes · 10 marks
Over a 5-day period, three patients in your 12-bed ICU grow carbapenem-resistant Klebsiella pneumoniae (KPC-producing) from sputum and urine cultures. Two are on the ventilator and one is on a renal replacement circuit. The unit has had hand hygiene compliance of 64% on the last audit. You are asked to lead the outbreak response.
SAQ — A bundle approach to preventing device-related infections in ICU
10 minutes · 10 marks
Your ICU has reported catheter-related bloodstream infection (CRBSI) and ventilator-associated pneumonia (VAP) rates that are above the national benchmark. The medical director asks you to design a quality-improvement programme to reduce these device-associated infections.
SAQ — MDR organism isolation and hand hygiene compliance
SAQ — Newly admitted patient with suspected multidrug-resistant (MDR) organism colonisation
10 minutes · 10 marks
A 68-year-old man is transferred from a tertiary hospital overseas to your ICU for ongoing management of ventilated respiratory failure. The referral letter flags prior isolation of carbapenem-resistant Acinetobacter baumannii (CRAB) from sputum and vancomycin-resistant Enterococcus (VRE) from rectal screening. Your ICU is at 90% occupancy with no vacant single rooms for the next 6 hours. Outline your isolation and infection-control management.
SAQ — Designing a hand hygiene quality-improvement programme for the ICU
10 minutes · 10 marks
Your 16-bed ICU's most recent independent audit shows hand hygiene compliance of 58% (target ≥80%, aspirational ≥90%). The lowest-performing moment is Moment 1 (before touching a patient) at 41%. The infection prevention committee asks you to lead a multimodal improvement programme. Outline your approach and the supporting evidence.
Clinical pearls
Red flags
ICU-acquired (nosocomial) infections — overview
[14]The chain of infection — what each control measure breaks
[2]Hand hygiene — the single most effective measure
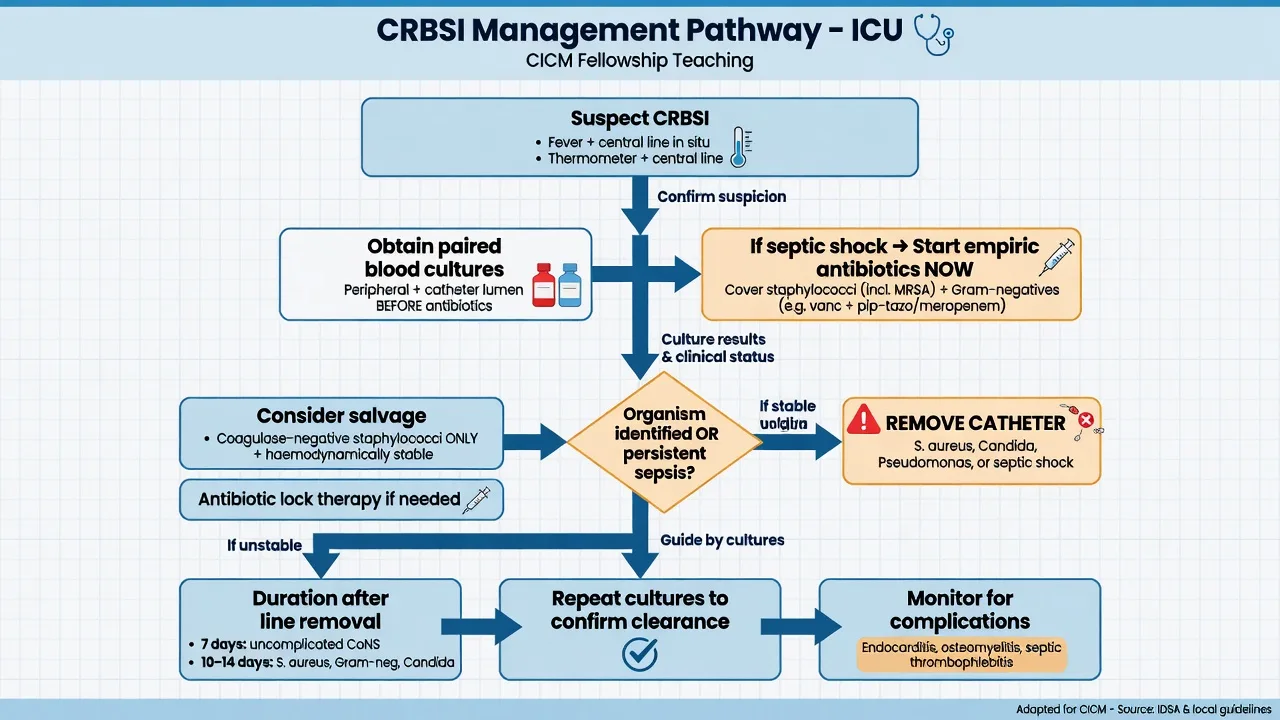
Catheter-related bloodstream infection (CRBSI / CLABSI)
Ventilator-associated pneumonia (VAP) — the prevention bundle
Catheter-associated urinary tract infection (CAUTI)
[8]Surgical site infection (SSI)
C. difficile infection (CDI) — prevention
Multidrug-resistant (MDR) organisms

Antimicrobial stewardship in the ICU
[11] [14]Environmental cleaning and disinfection
Surveillance cultures and active screening
[2] [14]Key trials and evidence
Pronovost 2006 — Michigan Keystone (CRBSI bundle)
Huang 2013 — REDUCE MRSA (universal decolonisation)
Climo 2009 — CHG bathing to reduce MRSA and VRE acquisition
Harbarth 2008 — universal MRSA admission screening
Pittet 2000 — Geneva hand-hygiene programme
Additional red flags
Prognosis and quality metrics
[14]References
- [1]Pittet D, Allegranzi B, Boyce J, et al. The World Health Organization Guidelines on Hand Hygiene in Health Care and their consensus recommendations. Infection Control and Hospital Epidemiology, 2009.PMID 19508124
- [2]Siegel JD, Rhinehart E, Jackson M, Chiarello L, HICPAC. 2007 Guideline for Isolation Precautions: Preventing Transmission of Infectious Agents in Health Care Settings. American Journal of Infection Control, 2007.PMID 18068815
- [3]Pittet D, Hugonnet S, Harbarth S, et al. Effectiveness of a hospital-wide programme to improve compliance with hand hygiene. Lancet, 2000.PMID 11073019
- [4]Lotfinejad N, Peters A, Tartari E, et al. Hand hygiene in health care: 20 years of ongoing advances and perspectives. Lancet Infectious Diseases, 2021.PMID 34331890
- [5]Pronovost P, Needham D, Berenholtz S, et al. An intervention to decrease catheter-related bloodstream infections in the ICU. New England Journal of Medicine, 2006.PMID 17192537
- [6]O'Grady NP, Alexander M, Burns LA, et al. Guidelines for the prevention of intravascular catheter-related infections. Clinical Infectious Diseases, 2011.PMID 21460264
- [7]Klompas M, Branson R, Eichenwald EC, et al. Strategies to prevent ventilator-associated pneumonia in acute care hospitals: 2014 update. Infection control and hospital epidemiology, 2014.PMID 25376073
- [8]Lo E, Nicolle LE, Coffin SE, et al. Strategies to prevent catheter-associated urinary tract infections in acute care hospitals: 2014 update. Infection Control and Hospital Epidemiology, 2014.PMID 25376068
- [9]Dubberke ER, Carling P, Carrico R, et al. Strategies to prevent Clostridium difficile infections in acute care hospitals: 2014 update. Infection Control and Hospital Epidemiology, 2014.PMID 25376069
- [10]Huang SS, Septimus E, Kleinman K, et al. Targeted versus universal decolonization to prevent ICU infection. New England Journal of Medicine, 2013.PMID 23718152
- [11]Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. Critical Care Medicine, 2021.PMID 34605781
- [12]Climo MW, Sepkowitz KA, Zuccotti G, et al. The effect of daily bathing with chlorhexidine on the acquisition of methicillin-resistant Staphylococcus aureus and vancomycin-resistant enterococci. Critical Care Medicine, 2009.PMID 19384220
- [13]Dancer SJ. Mopping up hospital infection. Journal of Hospital Infection, 1999.PMID 10549308
- [14]Storr J, Twyman A, Zingg W, et al. Core components for effective infection prevention and control programmes: new WHO evidence-based recommendations. Antimicrobial Resistance and Infection Control, 2017.PMID 28078082
- [15]Harbarth S, Fankhauser C, Schrenzel J, et al. Universal screening for methicillin-resistant Staphylococcus aureus at hospital admission and nosocomial infection in surgical patients. JAMA, 2008.PMID 18334690