ICU · Antimicrobial Stewardship
Ventilator-associated pneumonia (VAP)
Also known as Ventilator-associated pneumonia (VAP) · Hospital-acquired pneumonia (HAP) · CPIS (Clinical Pulmonary Infection Score) · VAP prevention bundle
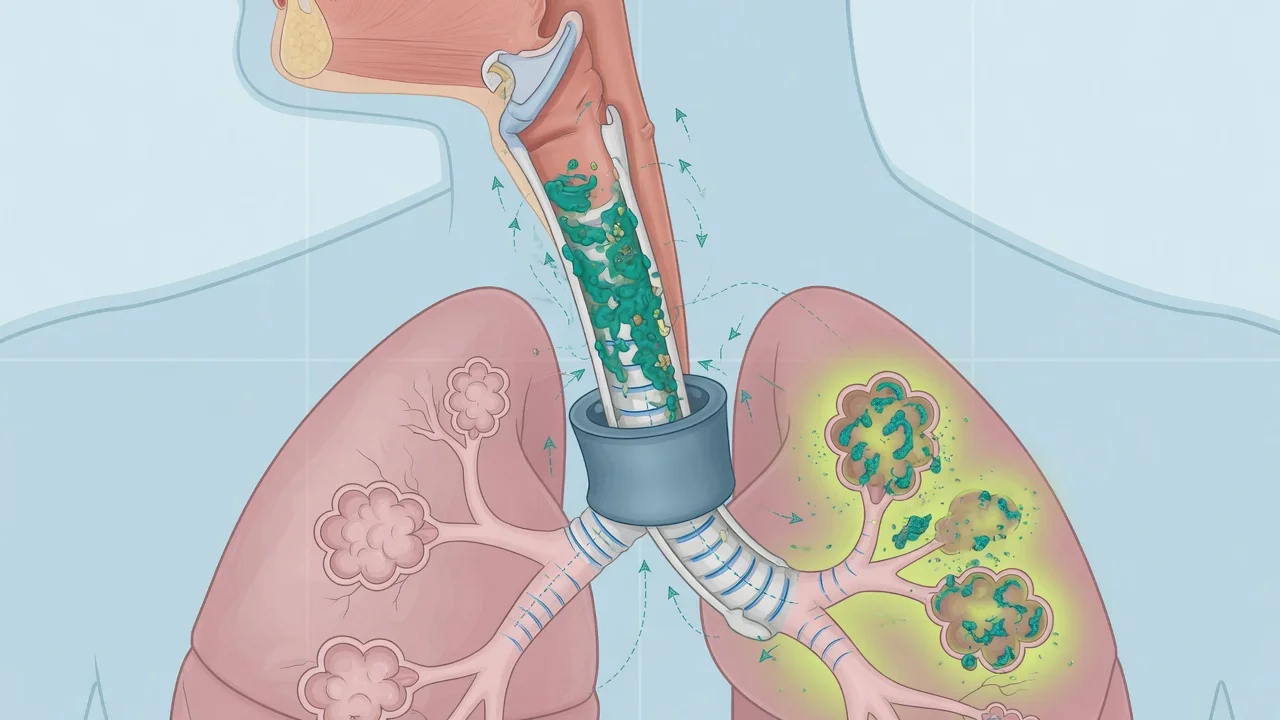
VAP is pneumonia developing 48 hours after endotracheal intubation. It is the most common ICU-acquired infection, with mortality of 13-25%. Pathogenesis: microaspiration of oropharyngeal secretions around the ETT cuff, bacterial colonisation of the ETT biofilm. Diagnosis: new/persistent infiltrate on CXR PLUS at least 2 of fever, leukocytosis, purulent secretions. CPIS 6 supports diagnosis. Microbiology: early VAP (<5 days) — S. pneumoniae, H. influenzae, MSSA. Late VAP (5 days) — MRSA, Pseudomonas, Acinetobacter, ESBL. Treatment: empiric antibiotics within 1 hour (cover MRSA + Pseudomonas), de-escalate based on cultures. Duration: 7 days standard (8 vs 15 day trial). Prevention bundle: head elevation 30-45 degrees, daily sedation interruption, oral chlorhexidine, subglottic suction ETT, DVT prophylaxis, stress ulcer prophylaxis.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Definition and pathogenesis
Definition
VAP: pneumonia developing >48 hours after endotracheal intubation and mechanical ventilation. It is distinguished from hospital-acquired pneumonia (HAP) which occurs in non-intubated patients.[1]
Pathogenesis
- Oropharyngeal colonisation: within days of intubation, the oropharynx is colonised by enteric Gram-negatives and S. aureus (loss of normal oral flora from illness, antibiotics)
- Microaspiration: secretions pool above the ETT cuff and leak around it ("channel leak") into the lower airways. This is the PRIMARY mechanism.[1]
- ETT biofilm: bacteria adhere to the ETT surface and form a biofilm — a protective extracellular matrix that shields bacteria from antibiotics and host immune cells. Biofilm fragments can be seeded distally with each breath.[1]
- Gastric colonisation: gastric acid suppression (PPI/H2 blocker for stress ulcer prophylaxis) allows bacterial overgrowth in the stomach. Gastroesophageal reflux with microaspiration contributes.
Pathogenesis in depth — the four-stage cascade
The pathogenesis of VAP can be conceptualised as a four-stage cascade that examiners expect you to articulate beyond a one-line "microaspiration" answer.[1]
The four-stage VAP cascade
Stage 1 — Loss of the oropharyngeal colonisation barrier
Within 48-72 h of ICU admission the normal oropharyngeal flora (viridans streptococci, Neisseria, anaerobes) is replaced by enteric Gram-negatives and S. aureus. Drivers: salivary flow reduction (sedation, anticholinergics, drying gases), antibiotic selection pressure, loss of cough, depressed consciousness, and proton-pump-inhibitor-induced gastric alkalinisation. The oropharynx is the FIRST reservoir.
Stage 2 — Biofilm formation on the endotracheal tube
Within 24 h of intubation a conditioning film of host proteins coats the ETT polyvinyl chloride surface; bacteria then adhere, secrete extracellular polymeric substance (EPS), and mature into a sessile biofilm. The biofilm confers up to 1000-fold resistance to antibiotics and host neutrophil clearance. Staphylococci and Pseudomonas are particularly strong biofilm formers.
Stage 3 — Microaspiration past the ETT cuff
Secretions pool in the subglottic space above the cuff and track down longitudinal folds ("channels") in the inflated cuff. Cuff pressure <20 cmH2O permits leakage; supine positioning, decreased level of consciousness, and the act of disconnecting the circuit (suctioning, transport) all increase leak. This is the DOMINANT mechanism.
Stage 4 — Inoculation and overwhelmed distal defence
Bacteria reach the sterile lower airway. Mucociliary clearance is impaired by the ETT and sedation; alveolar macrophage and neutrophil function is blunted by critical illness. Inoculum + impaired clearance = infection. Hypoalbuminaemia and pulmonary oedema further impair clearance and increase susceptibility.
The endotracheal tube as a nidus of infection
The ETT is not a passive conduit — it is the central pathogenic device in VAP. Several consequences flow from this anatomical fact:[13]
- Bypass of natural defences: the tube holds the vocal cords open, disabling the cough reflex and the glottic closure that normally protects the lower airway.
- Mucociliary injury: positive-pressure ventilation and the foreign body of the tube itself disrupt the mucociliary ladder, slowing bacterial clearance by ~50% within hours.
- Biofilm reservoir: by day 7 of intubation, >90% of ETTs have measurable biofilm. Biofilm fragments seed distal airways with each breath, each suctioning pass, and each repositioning — explaining why VAP can recur despite appropriate antibiotics.
- Cuff-channel leak: even at recommended cuff pressures (20-30 cmH2O), folds in the cuff create longitudinal channels through which contaminated subglottic fluid leaks. This is why subglottic secretion drainage and continuous cuff-pressure control work — they remove or reduce the leak.[18]
Risk factors for VAP and for MDR organisms
Risk factors divide into two distinct lists — risk of getting VAP at all, and risk of getting VAP caused by a multidrug-resistant organism. The second list drives empiric antibiotic breadth.[19]
Risk factors for VAP itself
Host and device factors
- Prolonged mechanical ventilation (each additional vent day adds 1-3% risk)
- Supine positioning (gravitational microaspiration)
- Re-intubation or unplanned extubation (forces bacterial inoculation)
- Low cuff pressure (<20 cmH2O) — measured or unmaintained
- Depressed consciousness (GCS <9) — impaired cough and swallow
- Enteral feeding (gastric overdistension, reflux)
- Severe illness: ARDS, burns, trauma, head injury
- Age >65, COPD, smoking, hypoalbuminaemia
- PPI use (gastric bacterial overgrowth)
- Paralysis, deep sedation (no spontaneous ventilation)
Risk factors for MDR pathogens
Drives broad-spectrum empiric therapy
- Late-onset VAP (>5 days after intubation / hospital day >4)
- Prior IV antibiotic exposure in last 90 days
- Septic shock at the time of VAP onset
- ARDS preceding the VAP episode
- Acute renal replacement therapy prior to VAP
- Prolonged ICU stay (>5 days)
- Known colonisation with MDR organism (MRSA, ESBL, CRE, Acinetobacter)
- Immunosuppression (neutropenia, transplant, chemotherapy, steroids)
- Structural lung disease (bronchiectasis, CF) — Pseudomonas risk
The 2016 IDSA/ATS guideline uses any one of the MDR risk factors above (or recent IV antibiotics) as the trigger for broad-spectrum empiric therapy with MRSA and dual anti-pseudomonal cover.[19]
Classification: early vs late VAP
VAP classification by onset (click each)
>=5 days after intubation
Caused by MDR organisms: MRSA, Pseudomonas aeruginosa, Acinetobacter baumannii, ESBL-producing Enterobacteriaceae, Stenotrophomonas maltophilia. Requires broad-spectrum empiric therapy with de-escalation.
Microbiology
Early VAP (<5 days)
Community-type organisms
- Streptococcus pneumoniae
- Haemophilus influenzae
- MSSA (methicillin-sensitive S. aureus)
- Moraxella catarrhalis
- Usually antibiotic-sensitive
- Empiric: ceftriaxone or amoxicillin-clavulanate
Late VAP (>=5 days)
MDR organisms
- MRSA (methicillin-resistant S. aureus)
- Pseudomonas aeruginosa
- Acinetobacter baumannii
- ESBL-producing Enterobacteriaceae (E. coli, Klebsiella)
- Stenotrophomonas maltophilia
- Empiric: vancomycin/linezolid + anti-pseudomonal beta-lactam
Microbiology in depth — Trouillet and the predictors of MDR
The single most influential study on VAP microbiology is the Trouillet cohort (Bichat-Claude Bernard, 135 episodes).[20] It showed that the probability of MDR VAP rises in a predictable, additive way with three risk factors:
Trouillet — probability of MDR VAP
The three independent predictors were (1) mechanical ventilation >7 days, (2) prior antibiotic use, and (3) prior broad-spectrum antibiotic use. This is the bedside heuristic examiners cite when asked "how do you predict MDR VAP?".[10]
Organism-specific pitfalls
[5] [4] [12]Polymicrobial infection
VAP is polymicrobial in 25-40% of cases — a S. aureus + Gram-negative pair, or a Pseudomonas + Acinetobacter co-infection in the long-stay patient. Send ETA and blood cultures before antibiotics. A polymicrobial culture is not contamination if it meets quantitative thresholds — it reflects co-existing lower-airway infection.[7]
Diagnosis
Clinical criteria
The traditional clinical diagnosis requires ALL of:[1]
- New or progressive infiltrate on CXR
- PLUS at least 2 of:
- Fever >38C or hypothermia <36C
- Leukocytosis (>12,000/mm3) or leukopenia (<4,000/mm3)
- Purulent tracheal secretions (increased volume or change in character)[4]
Clinical Pulmonary Infection Score (CPIS)
The CPIS (maximum 12) combines 6 parameters:[6]
| Parameter | 0 points | 1 point | 2 points |
|---|---|---|---|
| Temperature (C) | 36.5-38.4 | 38.5-38.9 | <36 or >39 |
| Blood leukocytes (mm3) | 4,000-11,000 | <4,000 or >11,000 | + bands >50% |
| Tracheal secretions | None/rare | Non-purulent | Purulent + |
| Oxygenation (PaO2/FiO2) | >240 or ARDS | — | <240 (no ARDS) |
| Pulmonary radiography | No infiltrate | Diffuse/patchy | Localised |
| Semi-quantitative culture | None/pathogenic | 1+ pathogenic | 2+ pathogenic |
CPIS >6 at baseline or after 72 hours supports VAP diagnosis and the need for continued antibiotics.[6]
Microbiological sampling
Endotracheal aspirate (ETA)
Non-invasive — first-line
- Simple, quick, non-invasive
- High sensitivity (misses few VAPs)
- Low specificity (colonisation vs infection)
- Quantitative culture: >10^6 CFU/mL = significant
- Preferred in most ICUs
Bronchoalveolar lavage (BAL)
Invasive — more specific
- Requires bronchoscopy or mini-BAL catheter
- Higher specificity (fewer false positives)
- Quantitative culture: >10^4 CFU/mL = significant
- Use if ETA results ambiguous or patient not responding
- Higher cost and risk (hypoxaemia, bleeding)
Protected specimen brush (PSB)
A third option used selectively — a telescoping catheter with a protected brush is advanced through a bronchoscope (or as a blind catheter), brushes distal airways, and is cultured quantitatively.[9]
- Quantitative threshold: >10³ CFU/mL = significant (lowest of the three because the brush samples a tiny volume).
- Specificity: highest of the three techniques (lowest false-positive rate from colonisation).
- Sensitivity: ~80-90% — can miss focal or sampled-segment-negative VAP.
- Use: when BAL is non-diagnostic but suspicion persists; in research; where ETA repeatedly shows mixed colonising flora.[3]
Quantitative vs qualitative cultures — does it change outcome?
The Fagon RCT randomised suspected VAP to an invasive strategy (PSB/BAL with quantitative thresholds directing antibiotics) vs a non-invasive strategy (clinical criteria + qualitative ETA cultures).[9] The invasive strategy reduced 14-day mortality (16% vs 26%) and antibiotic use at 14 days — but later multicentre studies were less positive, and the Cochrane review found no mortality difference between quantitative and qualitative strategies.[17][3]
Invasive (BAL/PSB, quantitative)
Specificity-led
- Higher specificity — fewer false positives from colonisation
- Drives de-escalation more confidently — antibiotics can be stopped if below threshold
- May reduce unnecessary antibiotic exposure
- Cost: bronchoscopy time, hypoxaemia, bleeding, sampling error
- Use when ETA repeatedly equivocal or patient not responding
Non-invasive (ETA, semi-quantitative)
Sensitivity-led — first-line in most ICUs
- Simple, quick, non-bronchoscopic — bedside on every patient
- High sensitivity — few VAPs missed
- Lower specificity — colonisation vs infection harder to distinguish
- Threshold: >10⁶ CFU/mL (or 10⁵ in some units) for significance
- Preferred pragmatic approach; pair with clinical + CPIS assessment
The 2016 IDSA/ATS guideline does not mandate either approach — both are acceptable, and the choice should follow unit protocol and expertise.[19]
Biomarkers in VAP diagnosis and stewardship
No single biomarker confirms or excludes VAP — they are adjunctive to clinical assessment, CPIS, and culture. They are most useful for stopping antibiotics, not for starting them.[18]
Procalcitonin (PCT)
Best-studied biomarker
- Rises in bacterial infection (and in non-infective systemic inflammation — interpret in context)
- Low and falling PCT supports stopping antibiotics (PRORATA, Bouadma 2010 — reduced antibiotic days without excess mortality)
- A single value is rarely diagnostic; serial trends are more useful
- False low: localised infection, early presentation, immunosuppression
- False high: trauma, surgery, burns, pancreatitis, cardiogenic shock
C-reactive protein (CRP)
Less specific
- Slower kinetics than PCT; non-specific for infection
- A rising CRP on antibiotics raises concern for treatment failure or source-control failure
- Cheaper and more widely available than PCT
sTREM-1 (soluble triggering receptor on myeloid cells-1)
Research-edge
- Upregulated on neutrophils and monocytes in response to bacterial products
- High sTREM-1 in BAL fluid supports VAP diagnosis in some studies
- Not in routine clinical use — performance varies between assays and populations
Mid-regional pro-adrenomedullin (MR-proADM)
Prognostic
- Marker of endothelial dysfunction and adrenomedullin pathway activation
- Higher values predict mortality and need for vasopressors
- Prognostic, not diagnostic — used in sepsis-stratification research
Management
Empiric antibiotic therapy
START WITHIN 1 HOUR of clinical suspicion. Delay in appropriate therapy increases mortality by ~7% per day.[2]
Empiric antibiotic selection algorithm
Assess risk factors for MDR organisms
Risk factors: late VAP (>5 days), prolonged ICU stay, recent antibiotics (last 90 days), septic shock at VAP onset, ARDS preceding VAP, acute renal replacement therapy prior to VAP. Presence of ANY risk factor = broad-spectrum empiric therapy.
Early VAP without MDR risk factors
Narrow spectrum: ceftriaxone 2g IV daily OR amoxicillin-clavulanate 1.2g IV TDS OR ertapenem 1g IV daily (if ESBL risk). Duration: 7 days. No MRSA or Pseudomonas cover needed.
Late VAP or any MDR risk factor
Broad spectrum: TWO anti-pseudomonal agents (piperacillin-tazobactam 4.5g IV TDS OR meropenem 1g IV TDS OR ceftazidime 2g IV TDS) PLUS MRSA cover (vancomycin 25-30 mg/kg loading then 15-20 mg/kg BD OR linezolid 600mg IV BD). Add a second anti-pseudomonal agent (aminoglycoside or fluoroquinolone) if high-risk MDR or known Pseudomonas colonisation.
De-escalate when culture results available
48-72 hours: review ETA/BAL culture results. Narrow therapy to the narrowest effective agent. Stop MRSA cover if no MRSA. Stop double anti-pseudomonal if susceptible to single agent. This is the most important antimicrobial stewardship intervention.
Duration: 7 days
8 vs 15-day trial (JAMA 2003): equivalent clinical outcomes at 28 days. 7 days reduces antibiotic exposure and resistance selection. EXCEPTION: non-fermenting Gram-negatives (Pseudomonas, Acinetobacter, Stenotrophomonas) — may need 7-8 days (higher recurrence rate). S. aureus — 7 days if uncomplicated.
Specific organism considerations
[8]Vancomycin vs linezolid for MRSA VAP
A recurring exam question. The Wunderink 2012 randomised study compared linezolid vs dose-adjusted vancomycin for MRSA nosocomial pneumonia.[15]
Vancomycin
The traditional default
- Glycopeptide — bactericidal (slowly)
- AUC/MIC is the PK/PD target (AUC 400-600 mg·h/L) — trough 15-20 mg/L is a surrogate
- Loading 25-30 mg/kg; then 15-20 mg/kg BD/QID adjusted to trough
- Nephrotoxicity (especially with concurrent piperacillin-tazobactam — AIN)
- Infusion reactions (red-man syndrome), phlebitis
- Skin penetration poor; alveolar penetration is only ~25% of serum
- Outcome worsens as vancomycin MIC rises towards 2 mg/L ("MIC creep")
Linezolid
Better lung penetration — possible VAP edge
- Oxazolidinone — bacteriostatic against staphylococci
- Excellent tissue and epithelial lining fluid penetration (~100%+ of serum)
- Fixed dose 600 mg IV/PO BD — no renal adjustment, no TDM
- Thrombocytopenia (and anaemia, leukopenia) after >14 days — check FBC
- Serotonin syndrome with SSRIs/MAOIs; peripheral and optic neuropathy in long courses
- Wunderink 2012: trend to better clinical cure and lower mortality in MRSA subset
- Bacteriostatic — caution in bacteraemia/endocarditis (controversial)
Exam line: "For documented MRSA VAP, linezolid is preferred by many intensivists because of superior lung penetration and a signal of benefit in Wunderink 2012; vancomycin remains acceptable with AUC-guided dosing. Avoid teicoplanin/daptomycin (daptomycin is inactivated by lung surfactant)."[15]
Special situations
[9] [2] [18] [17]Prevention: the VAP bundle
VAP prevention bundle (evidence-based)
Head of bed elevation 30-45 degrees
Reduces microaspiration by gravity. The single most effective and simplest intervention. Audit compliance — it is often suboptimal.
Daily sedation interruption + spontaneous breathing trial
Reduces duration of mechanical ventilation (fewer days intubated = lower VAP risk). Pair with delirium assessment (CAM-ICU).
Oral care with chlorhexidine
0.12% or 0.2% chlorhexidine mouthwash every 8-12 hours. Reduces oropharyngeal bacterial load. Cochrane review: reduces VAP incidence.
Subglottic secretion drainage
Use an ETT with a subglottic suction port (HI-LO Evac tube). Continuous or intermittent suction removes contaminated secretions above the cuff. Overview of reviews: significant VAP reduction.
DVT and stress ulcer prophylaxis
Enoxaparin 40 mg SC daily (DVT prophylaxis). PPI or H2 blocker (stress ulcer prophylaxis) — but note: PPIs may increase gastric bacterial colonisation.
Hand hygiene
WHO "5 Moments" for hand hygiene. Alcohol-based hand rub before and after every patient contact. Single most effective infection control measure.
Avoid unnecessary intubation
Use NIV where possible (COPD exacerbation, cardiogenic pulmonary oedema). Each day of intubation increases VAP risk by ~1-3%.
Early mobilisation
Reduce immobility-associated complications. Patients who mobilise within 72h have shorter ventilation duration.
Prevention evidence — what works, what is controversial
Strong evidence — recommended
Bundle components
- Head of bed elevation 30-45° (audit compliance — often suboptimal in practice)
- Daily sedation interruption paired with spontaneous awakening trial (Awakening and Breathing Controlled trial — reduces ventilation days)
- Subglottic secretion drainage (HI-LO Evac ETT) — reduces early-onset VAP particularly
- Hand hygiene — WHO "5 Moments"; single most effective infection-control measure
- Shortest possible duration of ventilation (early extubation, NIV where feasible)
- Early mobilisation within 72 h (Schweickert 2009 RCT — more ventilator-free days)
- DVT prophylaxis (enoxaparin) — required by the bundle but indirect effect on VAP
- Avoid unplanned re-intubation — re-intubation dramatically increases VAP risk
Controversial — conditional
Use selectively
- Oral chlorhexidine — Labeau 2011 meta showed reduced VAP incidence but NO mortality benefit; some signal of INCREASED mortality (CHX Trialists Collaboration). 2016 IDSA/ATS: consider, but not mandated.
- Selective digestive decontamination (SDD) / oropharyngeal decontamination (SOD) — reduces VAP and may reduce mortality in low-resistance settings; concerns about resistance selection limit use outside low-endemicity units
- Silver-coated ETT (NASCENT trial, Kollef 2008) — reduced VAP incidence but no mortality benefit; cost and uncertain cost-effectiveness limit routine use
- Stress ulcer prophylaxis — PPI reduces GI bleeding but increases gastric colonisation and possible pneumonia; restrict to patients at HIGH bleeding risk (mechanical ventilation >48 h + coagulopathy, shock, major burns, brain injury)
- Probiotics — small signal of reduced VAP; PROSPECT trial pending at time of writing; not yet standard
- Continuous cuff-pressure control — Nseir 2015 meta suggests VAP reduction; not universally deployed
Not recommended
Evidence absent or harmful
- Routine systemic antibiotic prophylaxis for VAP (selects resistance; no outcome benefit)
- Sucralfate over PPI for stress ulcer prophylaxis UNLESS bleeding risk is very low (PPI prevents more bleeds)
- Topical antibiotic rotation protocols without stewardship oversight
- Regular circuit changes — closed-suction systems and "change only when visibly soiled" are as safe as scheduled changes
- Prolonged supine positioning for nursing procedures (always return to semi-recumbent)
The "ventilator bundle" — origin and audit
The bundle concept was popularised by the Institute for Healthcare Improvement (IHI) in the early 2000s and adapted for VAP from Pronovost's central-line bundle model. The crucial operational point: bundles only work if every component is delivered to every patient every day — compliance with all elements simultaneously (an "all-or-none" measure) is far harder than compliance with each element individually. Audit and feed compliance back to the team.[11]
Prognosis
VAP outcomes
Key evidence — landmark trials in VAP
Chastre, Wolff, Fagon — PNEUMA trial (JAMA 2003, PMID 14625336)
Fagon, Chastre — Invasive vs non-invasive diagnostic strategy (Ann Intern Med 2000, PMID 10766680)
Kress, Pohlman, Hall — Daily sedation interruption (NEJM 2000, PMID 10816184)
Girard — Awakening and Breathing Controlled (ABC) trial (Lancet 2008, PMID 18191684)
Schweickert — Early physical and occupational therapy (Lancet 2009, PMID 19446324)
Kollef — NASCENT silver-coated ETT trial (JAMA 2008, PMID 18714060)
Labeau — Oral antiseptics to prevent VAP (Lancet ID 2011, PMID 21798809)
Wunderink — Linezolid vs vancomycin for MRSA nosocomial pneumonia (CID 2012, PMID 22247123)
Bouadma — PRORATA procalcitonin-guided antibiotic duration (Lancet 2010, PMID 20097417)
Berton — Quantitative vs qualitative respiratory cultures in VAP (Cochrane 2014, PMID 25354013)
Kalil — 2016 IDSA/ATS HAP/VAP Clinical Practice Guideline (CID 2016, PMID 27418577)
Exam practice
SAQ — Early-onset VAP
10 minutes · 10 marks
A 55-year-old woman is admitted to ICU for Guillain-Barré syndrome and requires intubation on day 3 for progressive respiratory failure. On day 5 of ventilation she develops fever 38.6°C, a rise in WCC from 9 to 14 ×10⁹/L, and increased purulent ETT secretions. CXR shows a new right middle lobe infiltrate. She has had no prior antibiotics and no ICU admission in the last 90 days.
SAQ — Late-onset VAP
10 minutes · 10 marks
A 68-year-old man has been in ICU for 9 days after emergency laparotomy for perforated diverticulitis. He is intubated and ventilated. He develops fever 38.7C, purulent tracheal secretions, and new right lower lobe infiltrate on CXR. WBC 16,000. He has been on piperacillin-tazobactam for 5 days for intra-abdominal sepsis.
Clinical pearls
Red flags
References
- [1] Torres A, Cilloniz C, Ferrer M, et al. Ventilator-associated pneumonia in adults: a narrative review. Intensive care medicine, 2020.PMID 32157357
- [2]Chastre J, Wolff M, Fagon JY, et al. Comparison of 8 vs 15 days of antibiotic therapy for ventilator-associated pneumonia in adults: a randomized trial. JAMA, 2003.PMID 14625336
- [3]Corrêa Rde A, Luna CM, Anjos JC, et al. Quantitative culture of endotracheal aspirate and BAL fluid samples in the management of patients with ventilator-associated pneumonia: a randomized clinical trial. Jornal brasileiro de pneumologia : publicacao oficial da Sociedade Brasileira de Pneumologia e Tisilogia, 2014.PMID 25610505
- [4]Caroff DA, Li L, Muscedere J, et al. Subglottic secretion drainage for preventing ventilator-associated pneumonia: an overview of systematic reviews. Infection control and hospital epidemiology, 2020.PMID 32051169
- [5]Serry C, Kautz DD, Ptaszynski M, et al. Oral hygiene care for critically ill patients to prevent ventilator-associated pneumonia: a review. American journal of infection control, 2020.PMID 33368159
- [6]Pagotto C, Dal Cortivo N, Romano F, et al. The Clinical Pulmonary Infection Score Combined with Procalcitonin and Lung Ultrasound. Diagnostics (Basel), 2024.PMID 38790587
- [7]Cosimi RA, Beik N, Kubiak DW, et al. Ceftaroline for Severe Methicillin-Resistant Staphylococcus aureus Infections: A Systematic Review. Open forum infectious diseases, 2017.PMID 28702467
- [8]Pang Z, Raudonis R, Glick BR, et al. Pseudomonas aeruginosa: pathogenesis, virulence factors, antibiotic resistance, interactions with host. Biotechnology advances, 2022.PMID 35752612
- [9]Fagon JY, Chastre J, Wolff M, et al. Invasive and noninvasive strategies for management of suspected ventilator-associated pneumonia. A randomized trial. Annals of internal medicine, 2000.PMID 10766680
- [10]Kress JP, Pohlman AS, O'Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. New England Journal of Medicine, 2000.PMID 10816184
- [11]Girard TD, Kress JP, Fuchs BD, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial). Lancet, 2008.PMID 18191684
- [12]Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet, 2009.PMID 19446324
- [13]Kollef MH, Afessa B, Anzueto A, et al. Silver-coated endotracheal tubes and incidence of ventilator-associated pneumonia: the NASCENT randomized trial. JAMA, 2008.PMID 18714060
- [14]Labeau SO, Van de Vyver K, Brusselaers N, Vogelaers D, Blot SI. Prevention of ventilator-associated pneumonia with oral antiseptics: a systematic review and meta-analysis. Lancet Infectious Diseases, 2011.PMID 21798809
- [15]Wunderink RG, Niederman MS, Kollef MH, et al. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: a randomized controlled study. Clinical Infectious Diseases, 2012.PMID 22247123
- [16]Bouadma L, Luyt CE, Tubach F, et al. Use of procalcitonin to reduce patients' exposure to antibiotics in intensive care units (PRORATA trial): a multicentre randomised controlled trial. Lancet, 2010.PMID 20097417
- [17]Berton DC, Kalil AC, Cavalcanti M, Teixeira PJ. Quantitative versus qualitative cultures of respiratory secretions for clinical outcomes in patients with ventilator-associated pneumonia. Cochrane Database of Systematic Reviews, 2014.PMID 25354013
- [18]Nseir S, Lorente L, Ferrer M, et al. Continuous control of tracheal cuff pressure for VAP prevention: a collaborative meta-analysis of individual participant data. Annals of Intensive Care, 2015.PMID 26603289
- [19]Kalil AC, Metersky ML, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and American Thoracic Society. Clinical Infectious Diseases, 2016.PMID 27418577
- [20]Trouillet JL, Chastre J, Vuagnat A, et al. Ventilator-associated pneumonia caused by potentially drug-resistant bacteria. American Journal of Respiratory and Critical Care Medicine, 1998.PMID 9476869