ICU · Infectious diseases
Fulminant Clostridioides difficile colitis: surgery, fidaxomicin, and bezlotoxumab
Also known as Fulminant C. difficile · C. difficile colitis · Pseudomembranous colitis · Toxic megacolon C. diff · Fidaxomicin · Bezlotoxumab
Clostridioides difficile infection (CDI) ranges from mild diarrhoea to FULMINANT colitis (toxic megacolon, perforation, septic shock). FULMINANT CDI: severe colitis with hypotension, ileus, megacolon (6 cm on imaging), perforation, or septic shock — mortality 30-50%. RISK FACTORS: age 65, antibiotics (broad-spectrum — clindamycin, fluoroquinolones, cephalosporins), PPIs, chemotherapy, IBD, recent hospitalisation. DIAGNOSIS: stool toxin (GDH + toxin EIA, or nucleic acid amplification), flexible sigmoidoscopy (pseudomembranes — if ileus precludes stool). TREATMENT: (1) INITIAL: fidaxomicin 200 mg PO BD x 10 days (preferred — MODIFY trial — lower recurrence) or vancomycin 125 mg PO QID x 10 days. (2) FULMINANT: vancomycin 500 mg PO/NG QID + IV metronidazole 500 mg TID + vancomycin enema (if ileus). (3) SURGERY: subtotal colectomy for perforation, refractory toxic megacolon, worsening sepsis despite 5+ days medical therapy. (4) BEZLOTOXUMAB (monoclonal anti-toxin B — MODIFY II — reduces recurrence in high-risk). (5) RECURRENCE: fidaxomicin, vancomycin taper, faecal microbiota transplant (FMT).
On this page & tools
Your progress
Saved locally on this device.
Target exams
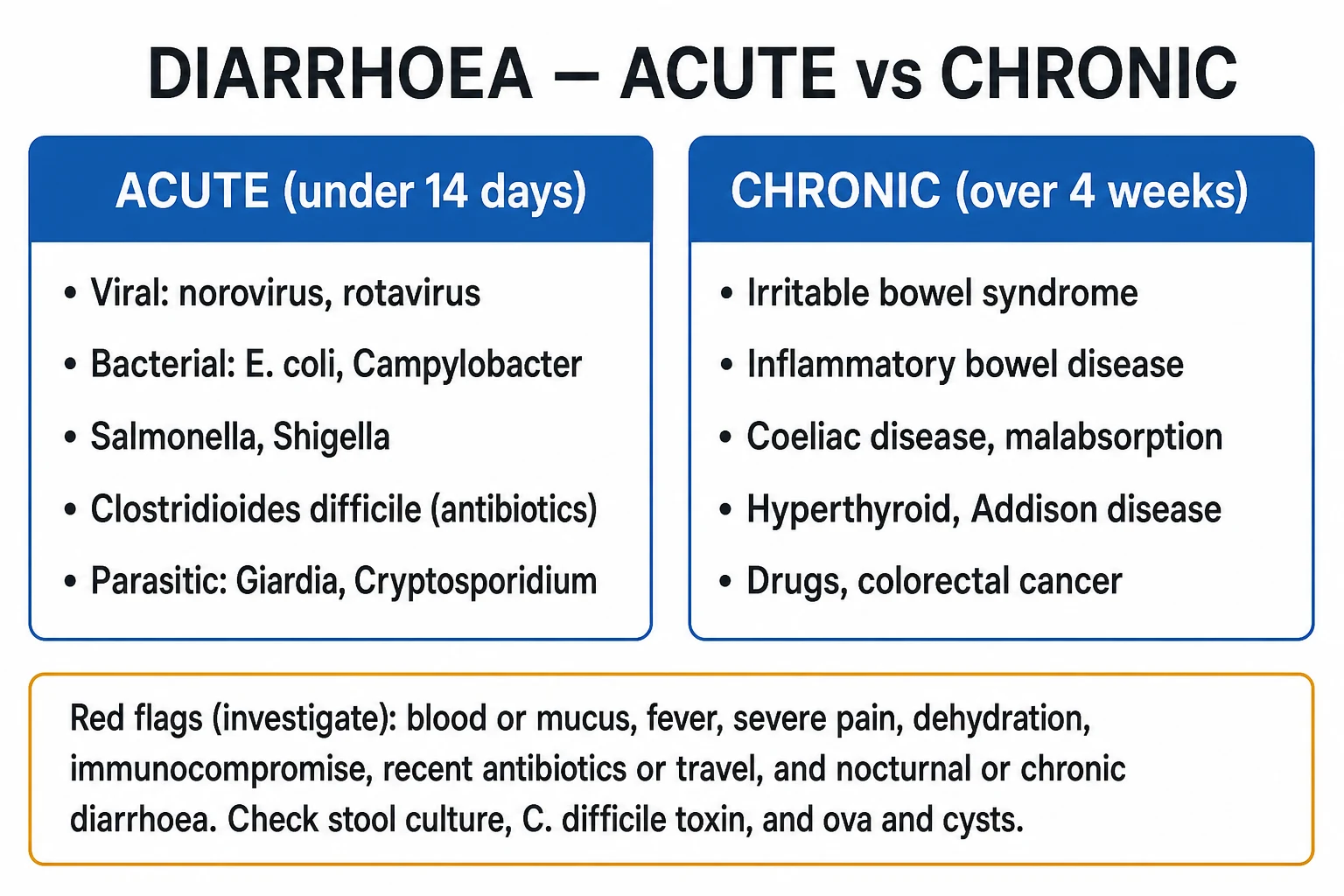
Red flags

SAQ — fulminant C. difficile colitis
SAQ — Fulminant C. difficile colitis: medical and surgical management
10 minutes · 10 marks
A 72-year-old woman is day 8 of ceftriaxone for a urinary tract infection. She has had profuse watery diarrhoea for 3 days and now presents confused, hypotensive (MAP 52 mmHg), tachycardic (HR 128) and with a distended, diffusely tender abdomen. WBC 38 x10^9/L, lactate 6.2 mmol/L, creatinine 210 micromol/L, albumin 22 g/L. AXR shows a dilated transverse colon to 7.5 cm with thumbprinting. Stool is positive for C. difficile toxin.
SAQ — Recurrent C. difficile: fidaxomicin, bezlotoxumab and faecal microbiota transplant
10 minutes · 10 marks
A 68-year-old man has had three episodes of C. difficile infection in 4 months (initial episode plus two recurrences), each treated with vancomycin. He has just completed a course and is clinically stable. He asks about further preventive options.
Clinical pearls
Red flags
Prognosis
Fulminant C. difficile evidence and outcomes
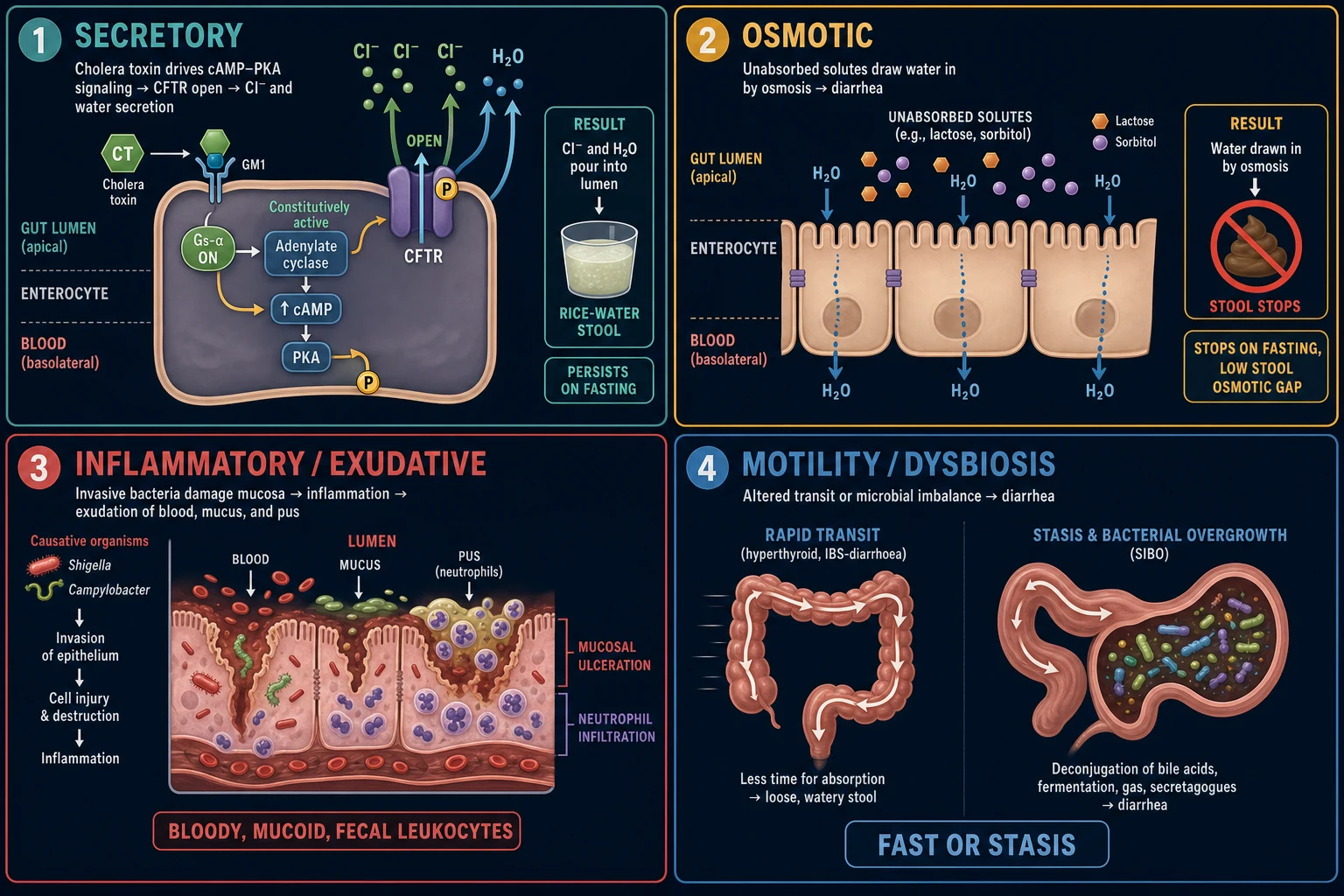
Pathophysiology — toxins A/B and the inflammatory cascade
[3]Pathophysiology — spores, germination and the colonic microbiome
[2]AGA / IDSA / ESCMID severity criteria compared
[4] [4]Pharmacology — fidaxomicin, vancomycin, metronidazole, bezlotoxumab
[2] [2] [3]Surgery — subtotal colectomy vs loop ileostomy with colonic lavage
[4] [4] [2]Special populations — IBD, neutropenia, pregnancy, post-transplant
[6]Diagnostics deep dive
[4] [4]Faecal microbiota transplant (FMT) — details and modern approaches
[6]ICU considerations — septic shock, AKI, electrolyte, nutrition
[4]Infection control and prevention
[6] [3]Prognosis and outcomes
Outcomes and prognostic factors in fulminant CDI
Pitfalls and high-yield exam rapid-recall
[3] [3]Landmark trials and guidelines — at a glance
References
- [1]Johnson S, Lavergne V, Skinner AM, et al. Clinical Practice Guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 Focused Update Guidelines on Management of Clostridioides difficile Infection in Adults. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 2021.PMID 34164674
- [2]Guery B, Menichetti F, Anttila VJ, et al. Extended-pulsed fidaxomicin versus vancomycin for Clostridium difficile infection in patients 60 years and older (EXTEND): a randomised, controlled, open-label, phase 3b/4 trial. The Lancet. Infectious diseases, 2018.PMID 29273269
- [3]Goldstein EJC, Citron DM, Gerding DN, et al. Bezlotoxumab for the Prevention of Recurrent Clostridioides difficile Infection: 12-Month Observational Data From the Randomized Phase III Trial, MODIFY II. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 2020.PMID 31883370
- [4]Singh A, Clark S The outcome of surgery in fulminant Clostridium difficile colitis. Colorectal disease : the official journal of the Association of Coloproctology of Great Britain and Ireland, 2006.PMID 16784480
- [5]Bauer MP, Kuijper EJ, van Dissel JT, et al. European Society of Clinical Microbiology and Infectious Diseases (ESCMID): treatment guidance document for Clostridium difficile infection (CDI). Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases, 2009.PMID 19929973
- [6]Shaukat A, Drekonja DM, Huang Y, et al. Efficacy and Safety of Fecal Microbiota Transplant for Prevention of Recurrent Clostridioides difficile Infection. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 2025.PMID 40260582