ICU · Infectious Diseases
Acute severe community-acquired pneumonia: Legionella
Also known as Legionella pneumophila · Legionnaires disease · Atypical pneumonia · Pontiac fever · Legionellosis
Legionella pneumophila is a gram-negative facultative intracellular pathogen that causes two syndromes: Pontiac fever (a mild self-limiting flu-like illness, no pneumonia) and Legionnaires' disease (severe atypical CAP — 2-10% of sporadic CAP, 2-3x higher ICU admission rate than pneumococcal CAP). It is acquired by inhalation of aerosolised water from cooling towers, spa pools, hot-water systems, showers, fountains and nebulisers; there is NO person-to-person spread. The organism is fastidious — it requires buffered charcoal yeast extract (BCYE) agar supplemented with L-cysteine and iron, and does NOT grow on routine blood/Chocolate agar. Clinical clues suggesting Legionella over pneumococcus: hyponatraemia (SIADH, Na <130), diarrhoea (50-70%), confusion/altered mental status (30-50%), relative bradycardia, fever 39C, hepatic dysfunction, myalgia, no upper-respiratory prodrome. Diagnosis rests on the urinary antigen (detects serogroup 1 = ~80% of clinical disease; rapid, specific) with culture on BCYE, respiratory PCR and paired serology as adjuncts. Treatment: a fluoroquinolone (levofloxacin 750 mg or moxifloxacin 400 mg daily) OR a macrolide (azithromycin 500 mg daily) for 5-10 days (14 days traditional, 21 days if immunocompromised); beta-lactams are INEFFECTIVE because the organism is intracellular. Mortality is 5-10% when treated in the community but 25-40% in ICU-admitted severe disease. Legionellosis is NOTIFIABLE — report to public health for source identification and outbreak detection.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Microbiology and pathogenesis
Pathogenic cascade — from aerosol to intracellular replication
1. Inhalation of contaminated aerosol
Susceptible hosts inhale aerosolised water droplets (1-5 micron droplet nuclei reach the alveoli) containing *L. pneumophila*. Classic sources: **cooling towers** (the single most common outbreak source), **evaporative condensers, spa pools / hot tubs, warm-water showers, decorative fountains, nebulisers and respiratory therapy equipment filled with tap water, mister/spray devices in supermarkets, dental water lines, and (rarely) water-birth pools**. **There is NO person-to-person transmission** — every case is acquired independently from an environmental source. The infectious dose depends on host susceptibility; smokers, the immunocompromised and those >50 years are markedly more susceptible.<Cite id="3" /><Cite id="6" />
2. Alveolar deposition and complement opsonisation
Bacteria reach the terminal bronchioles and alveoli, are opsonised by complement (C3b) and antibody, and are taken up by alveolar macrophages — but, unlike most pathogens, Legionella **subverts the macrophage** rather than being killed by it. The organism binds complement receptors and the macrophage surface, and is internalised by a novel uptake mechanism ("coiling phagocytosis") that avoids triggering the oxidative burst.
3. Formation of the Legionella-containing vacuole (LCV)
Inside the macrophage, Legionella resides in a membrane-bound **Legionella-containing vacuole (LCV)** that **evades fusion with lysosomes and the endocytic pathway**. Instead the LCV recruits ribosome-studded endoplasmic reticulum and mitochondria — disguising itself as a benign ER-derived compartment. The bacterium thereby escapes the acidic, enzyme-rich lysosomal killing that destroys most ingested microbes.<Cite id="2" />
4. Dot/Icm type IV secretion system injects >300 effectors
The decisive virulence determinant is the **Dot/Icm (defective in organelle trafficking / intracellular multiplication) type IVB secretion system** — a syringe-like apparatus that injects more than **300 effector proteins** into the host macrophage cytoplasm. These effectors collectively hijack host vesicle trafficking, recruit ER, inhibit apoptosis, suppress autophagy and remodel the LCV membrane — converting the macrophage into a permissive replication niche.
5. Intracellular replication and host-cell lysis
Within the protected LCV, Legionella replicates abundantly (8-12 hour doubling time), using host amino acids and lipids as fuel. When nutrients are exhausted, the bacteria differentiate into a **virulent, motile, transmissive form** (expressing flagella and cytotoxins), **lyse the host macrophage**, and are released to infect neighbouring cells — repeating the cycle and producing the characteristic patchy, peribronchiolar, multilobar inflammatory infiltrate.
6. Host immune response — cell-mediated immunity dominates
Because Legionella is intracellular, **humoral antibody is relatively unhelpful** — clearance depends on **cell-mediated immunity** (activated macrophages via IFN-γ from Th1/CD4+ T-cells and CD8+ cytotoxic T-cells). This explains (a) the populations at risk (impaired T-cell immunity = transplant, steroids, HIV), (b) why recovery produces only **serogroup-specific, non-protective antibody** (reinfection occurs), and (c) the granulomatous, macrophage-rich histology.
Epidemiology and environmental sources
[3] [6]Legionnaires' disease outbreaks cluster geographically — the 'rolling epidemic'
Retrospective epidemiological analysis of national outbreak surveillance data
Population: All reported Legionnaires' disease outbreaks and sporadic cases over multiple years in a high-income setting
Key finding
Outbreaks recur in small geographic areas (often the same cooling tower or plumbing system) over successive years, producing a 'rolling epidemic' pattern. Single cases are frequently the sentinel of an unrecognised cluster.
Clinical features
Suggestive features
Differentiate from typical CAP
- Hyponatraemia (SIADH — very common, Na <130)
- Diarrhoea (50-70% of cases — watery, non-bloody)
- Confusion/altered mental status (30-50%)
- Relative bradycardia (HR slower than expected for the temperature)
- High fever >39C (often >40C)
- Hepatic dysfunction (elevated ALT/AST, often disproportionate to illness)
- Myalgia, headache (may be severe, retro-orbital)
- No upper respiratory prodrome (no sore throat, coryza — unlike viral illness)
- Mild renal dysfunction, microscopic haematuria, proteinuria
- Hypophosphataemia and elevated CK (rhabdomyolysis) in severe disease
Risk factors
Who gets Legionella
- Immunocompromise (transplant, steroids, HIV, haematological malignancy)
- Smoking (impaired mucociliary clearance — strongest modifiable risk)
- COPD and chronic lung disease
- Age >50, male sex
- Travel (hotel stays, cruise ships — cooling towers)
- Recent hospital or healthcare facility exposure (nosocomial)
- Construction/demolition adjacent to cooling towers
- Spa-pool / hot-tub exposure
Two syndromes of legionellosis — Pontiac fever vs Legionnaires' disease
Pontiac fever (the mild form)
A **non-pneumonic, self-limiting flu-like illness** (fever, myalgia, headache, malaise) with incubation **24-72 hours** (short). No chest infiltrates. Attack rate is very high (>90% of exposed people fall ill) because it does not require deep alveolar deposition — likely a toxic/inflammatory reaction to inactivated bacteria rather than true infection. **Resolves spontaneously in 2-5 days without antibiotics.** Same organism, very different clinical expression. Most commonly recognised in outbreaks (the original 1968 Pontiac, Michigan outbreak in a health department).<Cite id="6" />
Legionnaires' disease (the severe form)
A **necrotising, multilobar atypical pneumonia** with incubation **2-10 days** (median ~6 days). The clinical picture combines systemic inflammation (high fever, rigors, myalgia, headache, confusion) with progressive respiratory failure and the multi-organ "Legionella fingerprint" — **diarrhoea, hyponatraemia, hepatic dysfunction, relative bradycardia, microscopic haematuria, encephalopathy**. Attack rate is low (<5% of exposed susceptible people) because it requires deep alveolar inoculation plus a permissive host. Untreated mortality approaches 25-40% in those needing ICU.<Cite id="2" /><Cite id="3" />
Diagnosis
Diagnostic workup — what to send, and what each test tells you
Urinary antigen (first-line, rapid)
Detects the soluble lipopolysaccharide antigen of **L. pneumophila serogroup 1** in urine — the cause of ~80% of disease. **Rapid (within hours), highly specific (~99%)**, can be performed on a spot urine sample, and remains positive for days to weeks after onset (even after antibiotics start). Sensitivity ~70-80% for serogroup 1 disease. **Does NOT detect other serogroups or non-pneumophila species** — a negative test in a compatible illness must be pursued with culture/PCR/serology. This is the single most useful test in suspected Legionnaires' disease.
Respiratory culture on BCYE agar (gold standard)
Send **sputum, endotracheal aspirate, BAL or lung tissue** plated on **buffered charcoal yeast extract (BCYE) agar** supplemented with L-cysteine and iron. Colonies appear in **3-5 days** (up to 10). **Will NOT grow on blood agar or Chocolate agar** — a "no growth" routine sputum culture in a compatible illness should prompt the lab to add BCYE. Culture is essential for (a) confirmation when urinary antigen is negative, (b) species/serogroup identification, and (c) **molecular typing (sequence-based typing, SBT)** for public-health outbreak source-tracking. Avoid contamination with tap water during sample handling (tap water can contain Legionella and give a false-positive culture).<Cite id="2" />
Nucleic acid amplification (PCR) on respiratory samples
**Multiplex respiratory PCR** detects *Legionella* spp. (not just serogroup 1) in sputum/BAL with high sensitivity and specificity, and returns within a day. Useful when (a) urinary antigen is negative but suspicion is high, (b) non-serogroup-1 or non-pneumophila disease is suspected, and (c) the patient is already on antibiotics (culture yield falls, PCR may still be positive). Does not provide a live isolate for typing.
Serology — paired acute and convalescent titres
A **4-fold or greater rise** in indirect immunofluorescent antibody titre between an acute sample (within the first week) and a convalescent sample (3-6 weeks later) confirms the diagnosis — but this is **retrospective** and does not guide acute management. A single high titre (e.g. >1:256) is supportive but not diagnostic. Send an acute serum in ALL suspected cases so a convalescent rise can be documented later — useful for epidemiology and for culture-negative cases.
Blood cultures (often negative — but send them)
Legionella is **rarely bacteraemic by conventional culture** (and will not grow on standard blood-culture bottles without special media). Blood cultures are nonetheless sent to **exclude a concomitant typical pathogen** (pneumococcus, *S. aureus*) — co-infection does occur and changes empiric cover. A positive *conventional* blood culture argues AGAINST Legionella as the sole cause.
Imaging and ancillary bloods
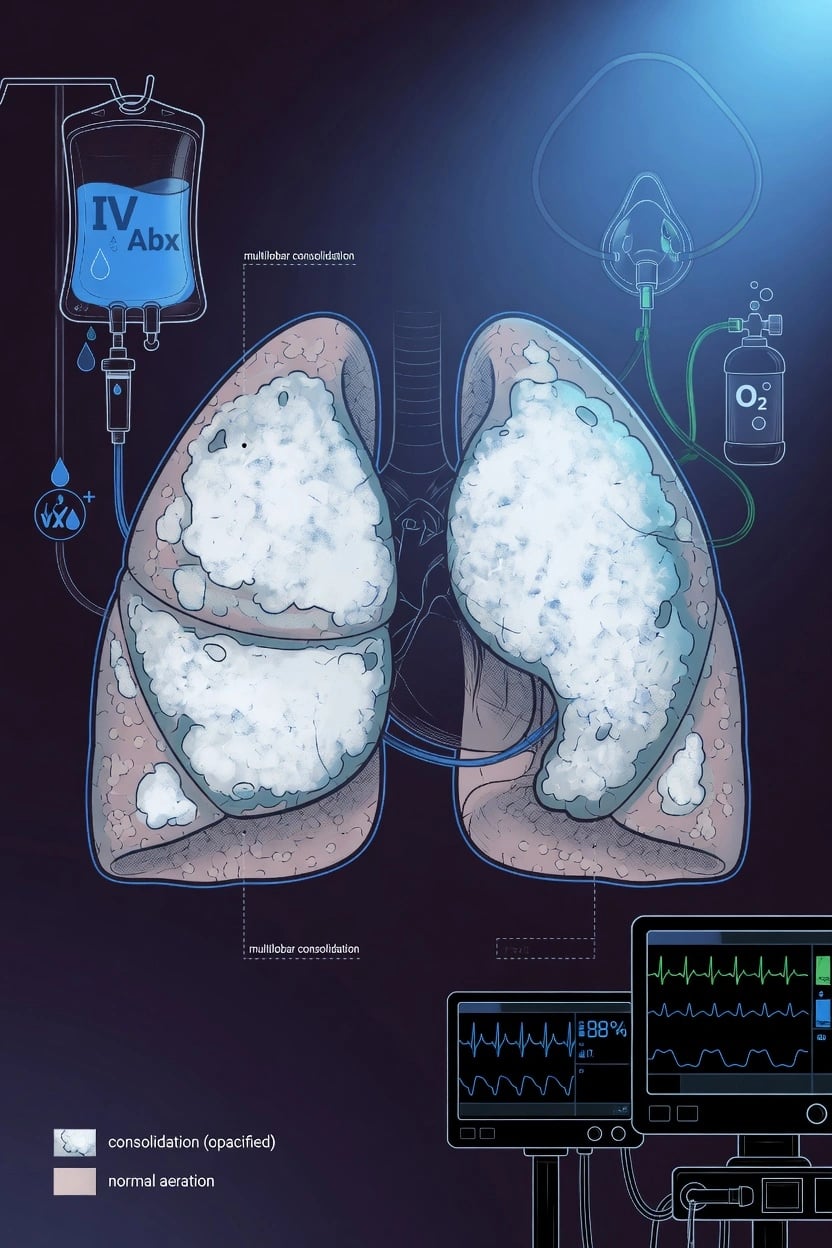
**CXR**: patchy, often **multilobar** consolidation that may begin as a single lobe and progress rapidly; **pleural effusion is common (~40%)**; **cavitation is rare in the immunocompetent** but can occur in the immunocompromised. **CT chest** better defines the patchy, nodular, peribronchiolar infiltrates and small effusions. **Bloods**: hyponatraemia (Na <130, SIADH), deranged LFTs (ALT/AST 2-3x normal without jaundice), elevated CK (rhabdomyolysis), microscopic haematuria/proteinuria, mild renal dysfunction, often **lymphopenia early**. CRP and procalcitonin may be high but are non-specific.<Cite id="3" />
Management
Legionella management protocol
Diagnosis
Urinary antigen: detects Legionella pneumophila serogroup 1 (~80% of cases). Rapid (within hours), specific. Does NOT detect other serogroups or species. PCR (sputum/BAL): detects all serogroups and species. Serology: 4-fold rise in antibody titre between acute and convalescent (3-6 weeks apart) — retrospective. Culture: on BCYE (buffered charcoal yeast extract) agar — slow (3-5 days), special media, gold standard. Send: urinary antigen + respiratory PCR + culture on BCYE + serology (acute and convalescent).
Antibiotic therapy
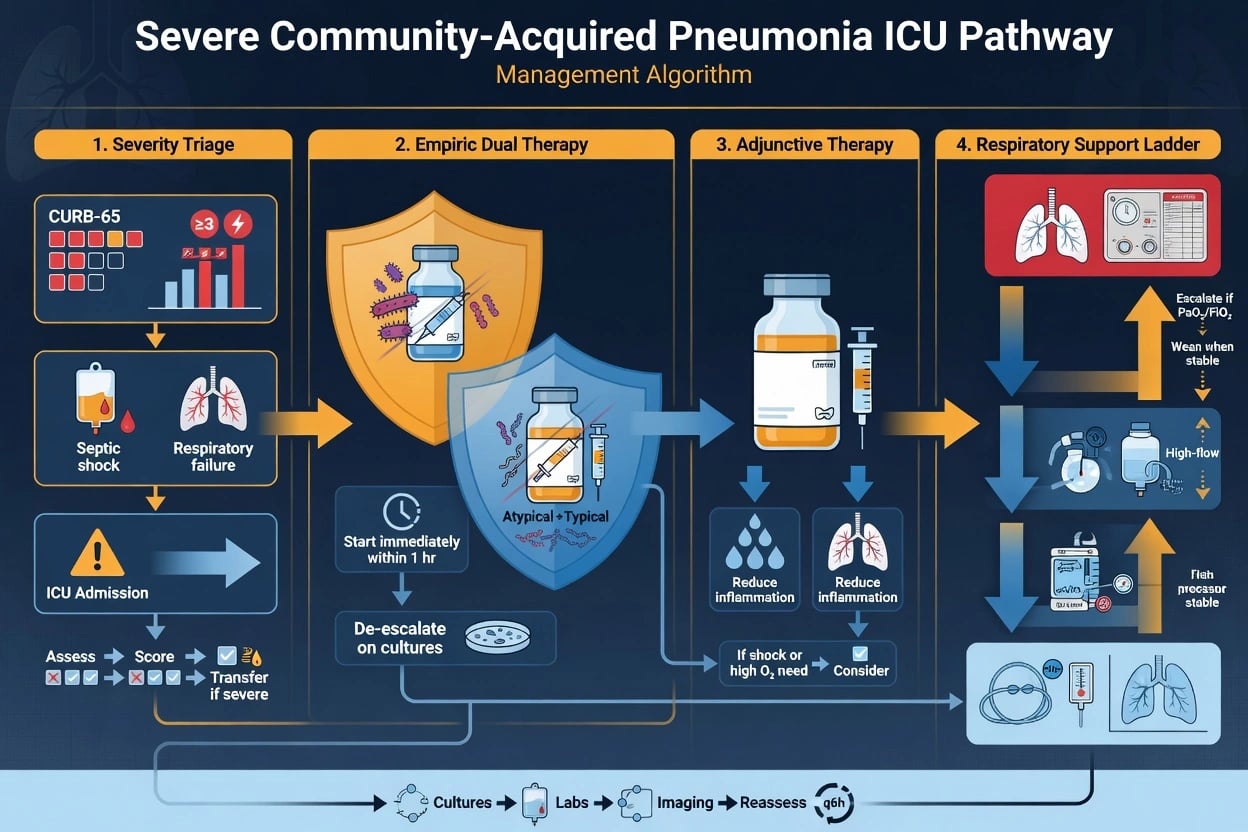
Macrolide: azithromycin 500 mg IV/PO daily (clarithromycin 500 mg BD is an alternative). OR Fluoroquinolone: levofloxacin 750 mg daily OR moxifloxacin 400 mg daily. **Duration 5-10 days** for azithromycin/levofloxacin/moxifloxacin in immunocompetent mild-moderate disease; extend to **14 days** for traditional regimens or severe disease; **21 days if immunocompromised** (transplant, steroids, HIV) or if there is endocarditis, abscess or cavitation. Fluoroquinolones may be slightly more effective (better intracellular penetration, faster defervescence in observational data). DO NOT use beta-lactams (Legionella is intracellular — beta-lactams do not reach intracellular concentrations). DO NOT use as sole agent if co-infection with typical bacteria suspected — combine with ceftriaxone until Legionella confirmed.<Cite id="5" />
Supportive ICU care
Ventilation if respiratory failure (lung-protective). Vasopressors if septic shock. Fluids (cautious — SIADH common, risk of hyponatraemia worsening). Correct hyponatraemia (fluid restrict if SIADH, or 3% hypertonic saline if seizures/coma). Monitor hepatic function, renal function and CK (rhabdomyolysis may need renal replacement therapy). Corticosteroids: no proven specific role; manage as for any severe CAP / ARDS.
Public health notification
Legionellosis is **NOTIFIABLE** in virtually all jurisdictions. A single confirmed case must be reported to public health. They investigate: cooling towers, water systems, spa pools, fountains near the case; environmental sampling and Legionella culture of water sources; molecular typing (sequence-based typing) to match clinical and environmental isolates; active case-finding for other cases (outbreak detection); disinfection of the source (hyperchlorination, superheat-and-flush, copper-silver ionisation).<Cite id="9" />
Fluoroquinolones vs macrolides for Legionnaires' disease
Prospective observational cohort comparing fluoroquinolones (levofloxacin) with macrolides (clarithromycin/azithromycin)
Population: Adults with confirmed Legionnaires' disease (urinary antigen and/or culture positive) requiring hospital admission
Key finding
Fluoroquinolone-treated patients had **shorter time to defervescence (median ~2 vs ~4-5 days)**, shorter length of stay, and fewer complications (especially in severe disease). Clinical cure rates were high in both arms (>95%) for non-severe disease; in severe ICU disease the fluoroquinolone arm trended toward lower mortality, though the comparison is observational (no randomisation).
Severity, complications and prognosis
[1] [3] [2] [3]Comparison with other severe pneumonias
[1] [2]Special populations
Special situations and modifications
Pregnancy
Pregnant women are not at markedly increased risk of Legionella specifically (unlike influenza). **Azithromycin** is the preferred agent (safety data in pregnancy; macrolides are not teratogenic). **Avoid fluoroquinolones** (cartilage/arthropathy concerns) and tetracyclines. Manage SIADH and rhabdomyolysis as usual; remember physiological pregnancy changes lower Na slightly.<Cite id="3" />
Immunocompromised (transplant, steroids, haematological malignancy, HIV)
At markedly increased risk of severe, cavitating, bacteraemic Legionella — and of disease caused by **non-serogroup-1 strains and non-pneumophila species**, so the urinary antigen is more often falsely negative. **Treat for 21 days**. Prefer a **fluoroquinolone** (levofloxacin) for the deeper intracellular penetration; beware drug interactions with calcineurin inhibitors (macrolides raise tacrolimus/cyclosporin levels via CYP3A4 — fluoroquinolones interact less). Send respiratory PCR and BCYE culture; image for cavitation. Consider co-pathogens (Pneumocystis, CMV, Aspergillus).<Cite id="2" />
Severe Legionella with ARDS
**Lung-protective ventilation** (Vt 6 mL/kg PBW, plateau <30 cmH2O); **prone positioning** for moderate-severe ARDS (PaO2/FiO2 <150); **venovenous ECMO** for refractory hypoxaemia (PaO2/FiO2 <80 despite optimisation). Conservative fluid strategy. Corticosteroids for ARDS have no Legionella-specific evidence but standard ARDS adjuncts apply.<Cite id="1" />
Nosocomial Legionella
A hospital cluster implies a **contaminated hospital water system**. Switch to **sterile water for all respiratory therapy devices and nebulisers** (never tap water); restrict showers; hyperchlorinate or superheat-and-flush the hot-water system; install copper-silver ionisation or point-of-use filters on high-risk units (transplant, haematooncology, ICU). Notify public health; active case-finding among recent inpatients.<Cite id="3" /><Cite id="9" />
Australasian note — Legionella longbeachae
In Australia and New Zealand, ***L. longbeachae*** (acquired from **potting mix / compost**, not cooling towers) causes a substantial minority of cases. The **urinary antigen is negative** (it detects only *L. pneumophila* serogroup 1) — diagnosis requires PCR or culture on BCYE. Gardeners (and especially older smokers) should wear gloves and a mask and open potting mix outdoors. Treatment is identical (fluoroquinolone or macrolide).<Cite id="3" />
SAQ — severe CAP: Legionella pneumophila
SAQ — Severe CAP due to Legionella pneumophila
10 minutes · 10 marks
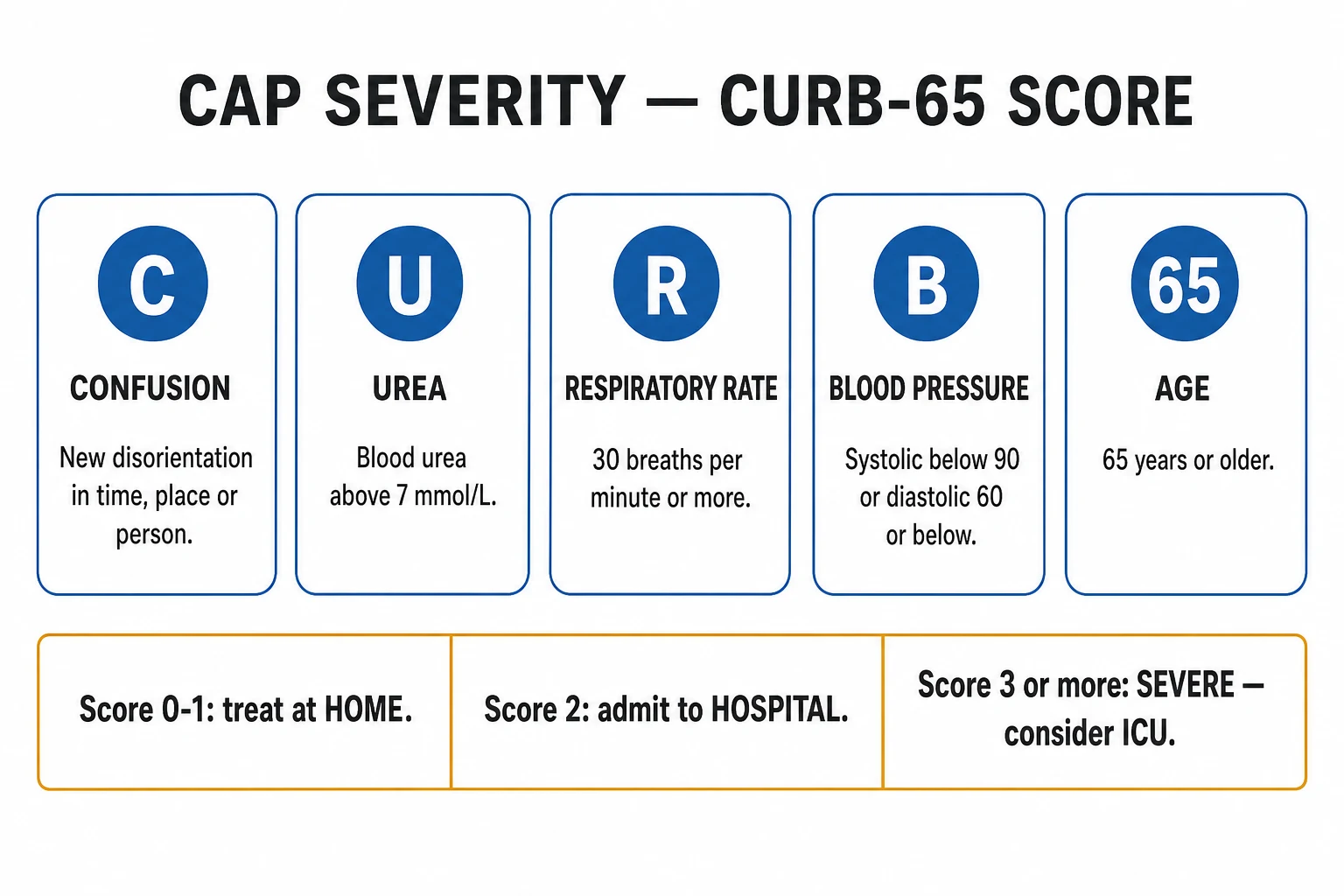
A 58-year-old male smoker presents with a 3-day history of high fever (39.5C), dry cough, confusion, profuse watery diarrhoea and abdominal pain. He returned 5 days ago from a cruise. Examination reveals a RR 32, SpO2 90% on room air, BP 96/60, HR 88 (relative bradycardia), and bilateral crackles. Na 126 mmol/L, AST 180 U/L, creatinine 165 micromol/L, CK 1500 U/L. Chest X-ray shows patchy multilobar consolidation. CURB-65 score is 4.
SAQ — Legionella outbreak investigation and public health
10 minutes · 10 marks
Over 2 weeks, four patients from the same suburb are admitted with severe pneumonia; three have positive Legionella urinary antigen. Public health requests your assistance in identifying the source.
SAQ — Management of severe Legionella pneumonia in an immunocompromised ICU patient
10 minutes · 10 marks
A 62-year-old man 14 months post-renal transplant (on tacrolimus, mycophenolate and prednisolone 10 mg daily) is admitted with a 4-day illness of fever 39.6C, dry cough, profuse watery diarrhoea and progressive confusion. Legionella urinary antigen is positive. In the ED he deteriorates: RR 36, SpO2 88% on a 15 L non-rebreather, BP 84/50 requiring noradrenaline 0.4 mcg/kg/min after 2 L crystalloid. He is intubated for ARDS (PaO2/FiO2 95). Na 123 mmol/L, CK 4400 U/L, creatinine 310 micromol/L (baseline 145), ALT 240 U/L, phosphate 0.45 mmol/L. CT chest shows bilateral patchy consolidation with a small left effusion and no cavitation.
SAQ — Urinary antigen diagnosis: when the test misleads
10 minutes · 10 marks
A 70-year-old male heavy smoker and keen gardener presents from regional New Zealand with a 5-day history of fever 39.2C, dry cough, myalgia, diarrhoea and confusion. He has been opening bags of commercial potting mix without gloves or a mask over the preceding fortnight. Examination: RR 30, SpO2 89% on air, BP 102/64, HR 92. Na 128 mmol/L, ALT 160 U/L, CK 900 U/L, lymphopenia. CXR shows patchy multilobar consolidation. CURB-65 is 4. The Legionella urinary antigen returned from the regional lab is NEGATIVE. The clinical team are about to discontinue atypical cover.
Clinical pearls
Pitfalls
Red flags
References
- [1]Niederman MS, Torres A. Severe community-acquired pneumonia. European Respiratory Review, 2022.PMID 36517046
- [2]Cunha BA, Burillo A, Bouza E. Legionnaires' disease. Lancet, 2016.PMID 26231463
- [3]Phin N, Parry-Ford F, Harrison T, et al. Epidemiology and clinical management of Legionnaires' disease. Lancet Infectious Diseases, 2014.PMID 24970283
- [4]Carratala J, Garcia-Vidal C. An update on Legionella. Current Opinion in Infectious Diseases, 2010.PMID 20051846
- [5]Sabria M, Pedro-Botet ML, Gomez J, et al. Fluoroquinolones vs macrolides in the treatment of Legionnaires disease. Chest, 2005.PMID 16162735
- [6]Hamilton KA, Prussin AJ 2nd, Ahmed W. Outbreaks of Legionnaires' disease and Pontiac fever 2006-2017. Current Environmental Health Reports, 2018.PMID 29744757
- [7]Schuetz P, Haubitz S, Christ-Crain M. Hyponatremia and anti-diuretic hormone in Legionnaires' disease. BMC Infectious Diseases, 2013.PMID 24330484
- [8]Cunha BA, Cunha CB. Legionnaire's disease: a clinical diagnostic approach. Infectious Disease Clinics of North America, 2017.PMID 28159178
- [9]MacIntyre CR, Dyda A, Bui CM. Rolling epidemic of Legionnaires' disease outbreaks in small geographic areas. Emerging Microbes and Infections, 2018.PMID 29559643