ICU · Infectious Diseases
Acute severe community-acquired pneumonia: MRSA pneumonia
Also known as MRSA pneumonia · Community-acquired MRSA pneumonia · PVL-positive S. aureus · Necrotising pneumonia · Healthcare-associated MRSA pneumonia · Staphylococcal necrotising pneumonia
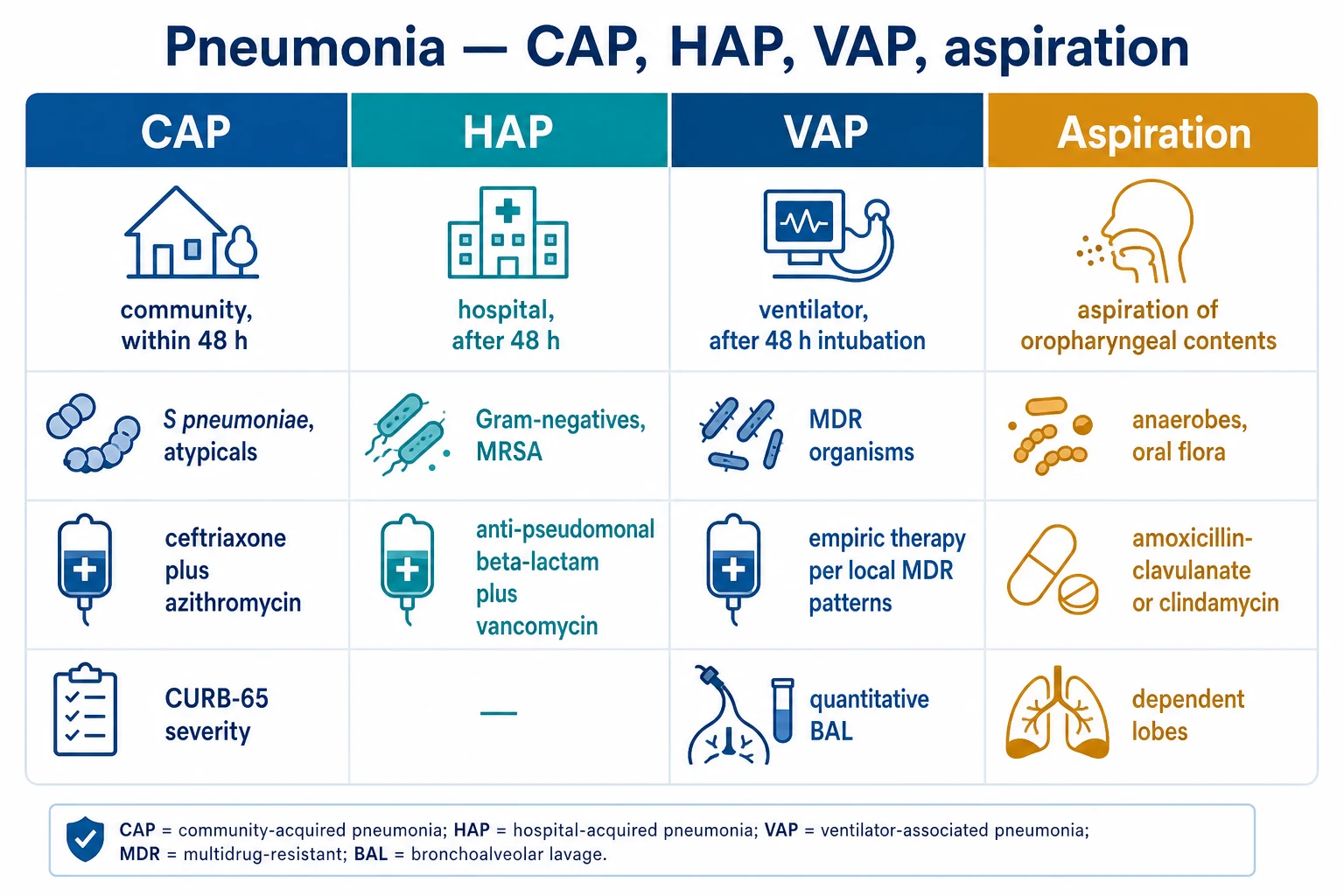
MRSA pneumonia in ICU: two epidemiologically and mechanistically distinct syndromes — healthcare-associated (HA-MRSA, nosocomial, multidrug resistant, SCCmec types I–III, lacks PVL) and community-acquired (CA-MRSA, often PVL-positive, SCCmec types IV–V, highly virulent, necrotising). Resistance is mediated by the mecA/mecC gene encoding PBP2a (penicillin-binding protein 2a) — an altered transpeptidase with low affinity for all beta-lactam antibiotics, rendering the entire beta-lactam class (including carbapenems) ineffective. Risk factors: post-influenza viral pneumonia (1 risk for CA-MRSA), recent hospitalisation (<90 days), IV antibiotics (<90 days), nursing home residence, haemodialysis, central venous catheter, IVDU, known MRSA colonisation, skin/soft tissue infection (CA-MRSA), age >65, immunocompromise. Presentation: severe CAP with rapid progression, multilobar infiltrates, cavitation (necrotising — hallmark of PVL-positive strains), haemoptysis, bacteraemia (20-30%), septic shock, leucopenia. Diagnosis: nasal swab PCR screening (high negative predictive value), sputum/blood culture, PVL gene detection (PCR for lukS-PV/lukF-PV), echocardiography for all bacteraemia. Treatment: vancomycin (loading 25-30 mg/kg, target trough 15-20 mg/L or AUC/MIC 400-600) OR linezolid 600 mg IV/PO BD (PREFERRED for pneumonia — superior epithelial lining fluid penetration, inhibits toxin production) OR clindamycin (if susceptible + as adjunct for toxin suppression in PVL-positive disease). Duration: 7-14 days (longer if bacteraemia, endocarditis, metastatic infection). Always search for metastatic infection (vertebral osteomyelitis, psoas/epidural abscess, endocarditis). Mortality: MRSA CAP 20-50% (PVL-positive necrotising disease highest).
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Pathophysiology — the mechanism of methicillin resistance
Resistance cascade — from gene to phenotype
1. Acquisition of SCCmec
SCCmec is a mobile genetic cassette integrated into a conserved chromosomal attachment site (orfX) near the replication origin. It carries the mecA/mecC complex plus recombinase genes (ccr) enabling excision/integration. Five major SCCmec types exist (I–V): the large (34–67 kb) types **I–III** carry additional resistance determinants (tetracycline, aminoglycosides, macrolides, heavy metals) and are characteristic of **HA-MRSA**; the small (20–30 kb) types **IV and V** carry little but mecA and are characteristic of **CA-MRSA**, allowing rapid spread.<Cite id="10" />
2. mecA transcription and PBP2a expression
mecA is transcribed into PBP2a (76 kDa). Expression is regulated by the **mecI/mecR1** repressor-inducer system and cross-talk with the **blaI/blaR1** beta-lactamase regulatory system. Exposure to any beta-lactam cleaves the membrane sensor MecR1/BlaR1, releasing a cytoplasmic domain that cleaves the repressor MecI — derepressing mecA transcription. This is why the resistance phenotype is reliably induced by beta-lactam exposure (though PBP2a is also expressed constitutively in many strains).<Cite id="3" />
3. PBP2a bypasses drug-inactivated native PBPs
Native PBPs (PBP1-4) catalyse the transpeptidation that cross-links peptidoglycan — the reaction beta-lactams block. Beta-lactams acylate these PBPs at their serine active site with high affinity (the beta-lactam ring is a D-Ala-D-Ala mimic). PBP2a’s active-site serine is **>100-fold less acylated** by beta-lactams because of a narrower, conformationally constrained binding cleft (the "allosteric" pocket is closed). PBP2a therefore continues cross-linking peptidoglycan, rescuing the cell wall when native PBPs are inactivated. Result: growth in the presence of otherwise lethal beta-lactam concentrations.<Cite id="10" />
4. Co-resistance: beta-lactamase (blaZ)
Most MRSA strains additionally carry the **blaZ** beta-lactamase gene on a plasmid or transposon, conferring resistance to penicillins by enzymatic hydrolysis. blaZ and the mecA regulatory systems interact — beta-lactamase induction pathways can co-activate PBP2a. This is a layered defence: blaZ degrades penicillins extracellularly; PBP2a survives whatever penicillin/cephalosporin/carbapenem reaches the membrane. The one beta-lactam that overcomes both is **ceftaroline**.<Cite id="13" />
5. Toxin armamentarium (especially CA-MRSA / PVL-positive)
Beyond resistance, virulence determines clinical severity. **Panton-Valentine leukocidin (PVL)** — a bicomponent synergohymenotropic toxin (LukS-PV + LukF-PV) — forms octameric pores in neutrophil and macrophage membranes, causing leukocyte lysis, massive inflammatory mediator release (leukotrienes, proteases, DAMPs) and haemorrhagic necrosis. PVL-positive strains cause **necrotising pneumonia** with cavitation, haemoptysis, and very high mortality. Other toxins: **alpha-haemolysin (Hla)** (pore-forming, injures alveolar epithelium and endothelium), **leukocidin AB (LukAB)**, **phenol-soluble modulins (PSMs)**, and **toxic shock syndrome toxin-1 (TSST-1)** / enterotoxins. Linezolid and clindamycin suppress these toxins by inhibiting bacterial protein synthesis.<Cite id="8" /><Cite id="9" />
Two epidemiological syndromes — HA-MRSA vs CA-MRSA
[10] [11]Risk factors — when to add empiric MRSA cover
Risk factors for MRSA pneumonia (ATS/IDSA 2019 criteria)
Prior MRSA colonisation or infection
The single strongest predictor. A known MRSA-positive nasal swab, prior MRSA SSTI, or bacteraemia within the past year markedly increases the probability of MRSA as the pneumonia pathogen. **Nasal surveillance PCR** has a high negative predictive value (>95%) for MRSA pneumonia — a negative screen supports withholding empiric MRSA cover in low-prevalence settings (with the caveat that ~25% of MRSA pneumonia is non-nasal).<Cite id="1" /><Cite id="15" />
Post-influenza pneumonia (#1 risk for CA-MRSA)
**Influenza damages ciliated epithelium, paralyzes mucociliary clearance, and disables alveolar macrophage phagocytosis** — converting the airway into a permissive niche for invasive *S. aureus*. S. aureus (incl. MRSA and PVL-positive strains) is the **single most common cause of post-influenza bacterial pneumonia** and carries the highest mortality. ANY severe CAP during influenza season, especially with a preceding viral prodrome and rapid deterioration with cavitation, mandates empiric MRSA cover PLUS oseltamivir.<Cite id="12" />
Healthcare exposure (HA-MRSA risk)
Hospitalisation ≥48 h within the last **90 days**, residence in a nursing home or long-term care facility, recent IV antibiotic therapy, **haemodialysis**, home wound care, or presence of an indwelling central venous catheter. These exposures select for the multidrug-resistant hospital strains (SCCmec I–III).<Cite id="7" />
Severe CAP with specific features
ATS/IDSA 2019 recommend empiric MRSA cover when severe CAP features coexist with any of: cavitation on imaging, **multilobar infiltrates**, empyema, or fulminant course with septic shock. Even WITHOUT classic risk factors, the radiographic phenotype of necrotising multilobar disease is sufficiently suggestive of PVL-positive S. aureus to justify empiric anti-MRSA therapy.<Cite id="1" />
Injection drug use (IVDU)
IVDU patients have high rates of MRSA colonisation, recurrent skin abscesses (often USA300/ST93), haematogenous seeding (septic emboli, tricuspid endocarditis, septic pulmonary emboli) and are at risk of both CA-MRSA necrotising pneumonia and metastatic staphylococcal infection. Send blood cultures and arrange echocardiography.<Cite id="3" />
Skin/soft tissue infection (SSTI) preceding or concurrent
A recent SSTI abscess (classically PVL-positive CA-MRSA — "spider-bite"-like lesion) in the patient or household contacts strongly suggests CA-MRSA as the pneumonia pathogen, particularly if necrotising. Ask about household contacts, athletes, military recruits, and overcrowded living conditions.<Cite id="9" />
Other host factors
Age >65, immunocompromise (neutropenia, transplant, HIV, immunosuppressive therapy), chronic lung disease (bronchiectasis, CF), diabetes mellitus, renal failure, malignancy. These increase both colonisation risk and severity.<Cite id="3" />
Clinical features
Presentation of severe MRSA pneumonia
HA-MRSA — subacute nosocomial
Typically a hospitalised or recently discharged patient (often ventilated, post-surgical, or with devices). Onset over days: new fever, purulent respiratory secretions, rising inflammatory markers, new/worsening infiltrates on CXR (often multilobar), increasing oxygen requirement. Bacteraemia in 20-30%. May progress to septic shock. Cavitation can develop but is less dramatic than in PVL-positive disease.
CA-MRSA / PVL-positive necrotising — fulminant
Classically a **young, previously healthy** patient, often 2-4 days after an influenza-like illness. Triphasic: viral prodrome (fever, myalgia, cough) → transient improvement → catastrophic deterioration. Hallmarks: **high fever**, **haemoptysis** (blood-tinged or frank blood), **septic shock** within hours, **multilobar infiltrates** progressing to **cavitation and pneumatocele formation**, **leucopenia** (ominous — reflects overwhelming sepsis/PVL-mediated leukocyte lysis), rapid progression to ARDS. Mortality 40-50% despite optimal therapy.<Cite id="8" />
Radiographic phenotype
**CXR/CT**: multilobar, often bilateral, patchy or confluent consolidation; **cavitation** (thick- or thin-walled) develops over days; **pneumatoceles** (thin-walled cysts, may rupture → pneumothorax); **pleural effusion** (often empyema — send pleural fluid for Gram stain/culture); occasionally pneumatocele rupture causes **pyopneumothorax**. The combination of multilobar infiltrates + cavitation + pneumatocele + effusion in a young patient with haemoptysis is virtually pathognomonic for PVL-positive staphylococcal necrotising pneumonia.<Cite id="8" /><Cite id="12" />
Bacteraemia and metastatic seeding
**20-30% bacteraemic.** Persistent bacteraemia (>2-3 days on appropriate therapy) demands search for: **endocarditis** (~25% of S. aureus bacteraemia — TOE required), **vertebral osteomyelitis / discitis**, **psoas abscess**, **epidural abscess** (cord compression!), **septic arthritis**, **splenic/renal abscess**, **septic pulmonary emboli**, **septic thrombophlebitis**. MRSA bacteraemia carries ~1.5-2x the mortality of MSSA bacteraemia.<Cite id="14" />
Severity and scoring
Calculate **CURB-65 or SMART-COP/SMART-CO** for CAP severity (latter preferred in ANZ for ICU triage). Assess **qSOFA/SOFA**, lactate, organ failures. PVL-positive necrotising pneumonia frequently meets **ARDS criteria** (PaO2/FiO2 <300, bilateral infiltrates) requiring lung-protective ventilation. Most of these patients belong in ICU from the outset.<Cite id="1" />
Diagnosis
[8]Diagnostic workup
Lower respiratory tract sampling
**Good-quality expectorated sputum** (<10 squamous epithelial cells/low-power field, >25 neutrophils/LPF) — Gram stain shows **Gram-positive cocci in clusters** (S. aureus classic morphology). If intubated: **endotracheal aspirate, BAL, or protected specimen brush** — quantitative cultures (BAL >10^4 CFU/mL) have higher specificity for true infection. Semi-quantitative is acceptable. Send BEFORE antibiotic changes where possible.<Cite id="1" />
Blood cultures (two sets) before antibiotics
Bacteraemia in 20-30%. **Positive blood cultures = independent mortality risk factor** and mandates a longer course and metastatic workup. Repeat every 48-72 h until negative. Persistent bacteraemia suggests endocarditis, deep abscess, septic thrombophlebitis, or inadequate source control (e.g. empyema, infected line).<Cite id="3" /><Cite id="14" />
Methicillin susceptibility testing
Phenotypic: **cefoxitin disk diffusion** or **oxacillin broth microdilution** (MIC). Genotypic: **mecA/mecC PCR** (rapid, definitive). All confirmed S. aureus from a sterile site should have susceptibility reported. Note: ceftaroline and ceftobiprole susceptibility is reported separately (active against PBP2a) — but NOT first-line for severe pneumonia.<Cite id="3" />
Nasal swab PCR screening (high NPV)
**Anterior nares PCR for MRSA** has a **negative predictive value >95%** for MRSA HAP/VAP and is used to **de-escalate** empiric vancomycin/linezolid in low-risk patients. A POSITIVE nasal swab does NOT prove MRSA is the pneumonia pathogen (colonisation ≠ infection), so it cannot be used alone to confirm MRSA pneumonia. Increasingly used in **antimicrobial stewardship** pathways.<Cite id="1" /><Cite id="7" />
PVL gene detection
PCR for **lukS-PV/lukF-PV** genes on sputum or blood isolate. Identifies the **necrotising phenotype**. PVL-positive MRSA = necrotising pneumonia, haemoptysis, high mortality, rationale for linezolid/clindamycin (toxin suppression). PVL positivity also raises the question of household/contact screening and decolonisation.<Cite id="8" /><Cite id="9" />
Echocardiography (TOE preferred)
ALL S. aureus bacteraemia requires echocardiography — **TOE preferred** (sensitivity ~90-95% vs TTE ~40-60% for vegetations, and TOE detects paravalvular and metastatic complications). Up to **25% of S. aureus bacteraemia has endocarditis** — many of these are occult on TTE. Repeat if high suspicion persists.<Cite id="3" /><Cite id="14" />
Imaging for metastatic infection
In bacteraemic or persistently febrile disease: **CT abdomen/pelvis** (psoas, splenic, renal, hepatic abscess), **MRI spine** (vertebral osteomyelitis/discitis, epidural abscess — the modality of choice), **CT chest** (cavitation, empyema, septic emboli). Positively seek metastatic foci — missing an epidural abscess can cause irreversible cord injury.<Cite id="3" />
Biomarkers — procalcitonin, CRP
Procalcitonin is typically high in bacterial MRSA pneumonia (distinguishes from pure viral), but does NOT reliably distinguish MRSA from MSSA or other bacteria. Use **trends** to guide duration (PCT-guided stopping when falls >80% from peak or <0.5 ng/mL — though necrotising/bacteraemic disease warrants a full fixed course). CRP and WBC are nonspecific; **leucopenia in PVL-positive disease is ominous**.<Cite id="1" />
Management
MRSA pneumonia management
Empiric MRSA cover
Add vancomycin (25-30 mg/kg loading, then trough 15-20 mg/L or AUC/MIC 400-600) OR linezolid (600 mg IV/PO BD) when MRSA risk factors are present: prior MRSA colonisation, recent hospitalisation/IV antibiotics, nursing home, dialysis, central line, post-influenza, IVDU, severe CAP with cavitation/multilobar. Continue empirically until cultures exclude MRSA (48-72 h). The ATS/IDSA 2019 severe CAP regimen adds MRSA cover to standard CAP therapy (ceftriaxone + macrolide or respiratory fluoroquinolone).<Cite id="1" />
Linezolid vs vancomycin — the central decision
**Linezolid 600 mg IV BD is PREFERRED** for MRSA pneumonia. Advantages: (1) **100% oral bioavailability** — seamless IV-to-PO switch. (2) **Superior lung penetration** — epithelial lining fluid (ELF) concentration **far exceeds serum** (vancomycin ELF is ~25% of serum). (3) **Suppresses toxin production** (PVL, alpha-haemolysin) by inhibiting 70S ribosomal initiation — important in PVL-positive necrotising pneumonia. (4) **No nephrotoxicity** (unlike vancomycin). (5) No therapeutic drug monitoring. Wunderink 2012 RCT and pooled meta-analyses show **improved clinical cure and a survival trend** vs vancomycin. CAUTION: **thrombocytopenia** (weekly FBC, especially >14 days), **serotonin syndrome** (MAO inhibition — avoid with serotonergic drugs/MAOIs), **peripheral & optic neuropathy** and **lactic acidosis** with prolonged use. BacteriOSTATIC.<Cite id="2" /><Cite id="6" />
Vancomycin dosing and monitoring
If vancomycin used: **loading dose 25-30 mg/kg** (for severe infection — achieves rapid therapeutic level), then trough-guided dosing (target **trough 15-20 mg/L**). Modern consensus (2020 ASHP/IDSA): target **AUC/MIC 400-600** (Bayesian dosing software) — AUC-based dosing reduces nephrotoxicity vs trough-only. Vancomycin issues: **nephrotoxicity** (significantly worse with concurrent **piperacillin-tazobactam** — switch to cefepime/ceftriaxone where possible), **red man syndrome** (infusion-related histamine release — slow infusion over ≥60 min, NOT an IgE allergy), slow tissue penetration, and concern over **MIC creep** / hVISA (heteroresistant intermediate S. aureus) in MIC >1.5 mg/L strains.<Cite id="3" /><Cite id="7" />
Clindamycin and combination toxin-suppression
For **PVL-positive necrotising pneumonia**, add or use **clindamycin 600-900 mg IV TDS** if the strain is susceptible (D-test negative — no inducible resistance). Clindamycin is a ribosomal inhibitor that **suppresses PVL and other exotoxin production** even at sub-inhibitory concentrations. Use as an **adjunct** to vancomycin or linezolid in fulminant toxin-mediated disease — NOT as monotherapy (bacteriostatic, resistance risk). Some units also consider **IVIG** (neutralising anti-PVL antibodies) in refractory toxin-mediated shock, though evidence is observational.<Cite id="8" /><Cite id="9" />
Duration and complications
Duration: **7-14 days** for uncomplicated MRSA pneumonia; longer if **bacteraemia** (≥14 days from first negative culture), **endocarditis** (4-6 weeks), **osteomyelitis** (6 weeks), **metastatic abscess** (until source controlled). Blood cultures: repeat every 48-72 h until negative. Echocardiogram: ALL S. aureus bacteraemia (TOE preferred — 25% have endocarditis). Monitor for: metastatic infection (vertebral, psoas, epidural, septic emboli), empyema, pneumatocele, ARDS, AKI (vancomycin).<Cite id="3" />
Wunderink 2012 — Linezolid vs vancomycin in MRSA nosocomial pneumonia (pivotal RCT)
Multicentre, randomised, double-blind, controlled trial
Population: Adults with nosocomial pneumonia (HAP/VAP) with proven MRSA (n=448 with MRSA in the per-protocol analysis)
Key finding
Pre-specified, prospectively defined analysis of the subset with proven MRSA: linezolid produced a **significantly higher clinical cure rate** (57.6% vs 46.6%, treatment difference 11.0%; 95% CI 0.5-21.6) and a statistically significant **survival advantage at 60 days** (84.1% vs 71.7%; p=0.033). Nephrotoxicity was significantly lower with linezolid.
Wunderink 2003 — Pooled analysis of two linezolid vs vancomycin HAP studies
Prospectively defined, pooled analysis of two phase III randomised, double-blind trials
Population: Patients with Gram-positive nosocomial pneumonia, including a subset with MRSA (n=59 with proven MRSA)
Key finding
In the MRSA subset, linezolid was associated with **higher clinical cure** (59% vs 36%) and a **survival advantage** (80% vs 64%, p=0.03) vs vancomycin. This was the earliest signal that linezolid may outperform vancomycin specifically in MRSA pneumonia.
Kato 2021 — Meta-analysis of vancomycin vs linezolid in proven MRSA pneumonia
Systematic review and meta-analysis (10 studies, n=1592 patients with culture-proven MRSA pneumonia)
Population: Hospitalised adults with culture-proven MRSA pneumonia (HAP/VAP and CAP)
Key finding
Linezolid was associated with a **significantly higher clinical cure rate** (RR favouring linezolid) and a trend toward lower mortality. Nephrotoxicity was significantly lower with linezolid; thrombocytopenia more frequent with linezolid (as expected).
Gillet 2002 — PVL-positive S. aureus necrotising pneumonia (landmark case-control)
Case-control study from France comparing PVL-positive vs PVL-negative S. aureus pneumonia
Population: Young, previously immunocompetent patients with severe, rapidly progressive, necrotising pneumonia
Key finding
PVL-positive strains caused **fulminant necrotising pneumonia** with characteristic features (high fever, haemoptysis, multilobar infiltrates, cavitation, leucopenia, septic shock). **Mortality was very high (~40-75%)** and affected previously healthy young patients. PVL-negative strains caused far less necrosis and lower mortality.
Complications and metastatic infection
[3] [14]Mortality and prognosis
[3] [14]Prevention
Preventing MRSA pneumonia
Influenza vaccination (#1 modifiable risk)
Annual inactivated influenza vaccine for everyone >6 months — priority for >65, pregnant, chronic disease, immunocompromised, healthcare workers, ICU/aged-care staff. Prevents the post-influenza state that predisposes to S. aureus necrotising pneumonia. Herd immunity in healthcare workers protects vulnerable patients.<Cite id="12" />
Pneumococcal vaccination
PCV13/15/20 + PPSV23 per age/risk schedules — reduces invasive pneumococcal disease (a post-influenza co-pathogen and a cause of necrotising CAP that can mimic MRSA).<Cite id="1" />
Decolonisation (selected cases)
For patients with recurrent MRSA SSTI or in outbreak settings: **nasal mupirocin BD ×5 days + chlorhexidine body washes**. Effectiveness is partial and transient; not routine for single-episode pneumonia, but considered for households of PVL-positive strains and before elective surgery in known carriers.<Cite id="3" />
Infection control
**Contact precautions** + single room for known/suspected MRSA. Hand hygiene, gloves/gowns, dedicated equipment. Active surveillance cultures (nares) on ICU admission in high-prevalence settings to direct isolation and decolonisation. Antimicrobial stewardship to limit selection pressure.<Cite id="7" />
Source control and device stewardship
Remove infected central lines, drain abscesses and empyema, debride necrotic tissue. Daily review of device necessity (central lines, endotracheal tubes, urinary catheters) — minimise duration to reduce nosocomial MRSA acquisition.<Cite id="7" />
Special populations
Special situations and modifications
Neutropenic / haematology / transplant
High risk of severe MRSA infection. Empiric vancomycin/linezolid with broad Gram-negative cover (anti-pseudomonal beta-lactam). Linezolid preferred where thrombocytopenia permits; watch FBC closely. Add antifungal ( mould-active azole/echinocandin) if persistent fever. Coordinate with haemato-oncology/infectious diseases.
Pregnancy
Vancomycin is the preferred anti-MRSA agent in pregnancy (long safety record). Linezolid is category C — use only if benefit outweighs risk (avoid if possible, especially first trimester). Clindamycin is generally acceptable if susceptible. Treat aggressively — necrotising pneumonia is a maternal and fetal emergency.
Renal failure / dialysis
Vancomycin dosing must be AUC-guided (post-haemodialysis levels). **Linezolid is preferred** — no renal dose adjustment needed for the standard 600 mg BD (metabolites accumulate but not problematic in short courses; reduce to 600 mg OD only if CrCl <30 with prolonged use). Avoid aminoglycoside combinations.
Endocarditis or metastatic seeding
If bacteraemia, endocarditis, or deep abscess: switch to **bactericidal** therapy (vancomycin ± rifampicin/gentamicin for synergy in endocarditis/device infection; consider ceftaroline). Duration 4-6 weeks for endocarditis, 6 weeks for osteomyelitis. Surgical source control is paramount. Linezolid is NOT preferred for documented bacteraemia (bacteriostatic, lower bloodstream sterilisation).<Cite id="3" />
Pediatrics
PVL-positive CA-MRSA necrotising pneumonia occurs in children. Linezolid (10 mg/kg TDS <12y, 600 mg BD >12y), vancomycin (15 mg/kg q6h, trough 15-20), clindamycin (10 mg/kg TDS-QDS if susceptible). Corticosteroids and IVIG sometimes used in fulminant toxin-mediated disease. Aggressive lung-protective ventilation for ARDS.<Cite id="8" />
SAQ — MRSA pneumonia: necrotising post-influenza
SAQ — Necrotising post-influenza MRSA (PVL-positive) pneumonia
10 minutes · 10 marks
A 24-year-old previously well man is admitted to ICU 5 days after an influenza-like illness that briefly improved before rapidly worsening. He is septic (MAP 60, HR 140, RR 38, SpO2 88% on 15 L via non-rebreather), coughing blood-stained sputum. CXR shows dense multilobar consolidation with early cavitation. Influenza A PCR is positive. Blood cultures grow gram-positive cocci in clusters at 8 hours. He was discharged from hospital 2 months ago after an appendectomy.
SAQ — Hospital-acquired MRSA ventilator-associated pneumonia
10 minutes · 10 marks
A 68-year-old man is on day 12 of mechanical ventilation for a severe COPD exacerbation. He develops a new fever, purulent tracheal secretions, rising FiO2 requirement and new infiltrates on CXR. He has been on broad-spectrum antibiotics for the last 7 days. He was previously colonised with MRSA on nasal swab.
Clinical pearls
Red flags
References
- [1]Metlay JP, Waterer GW, Long AC, Anzueto A, et al. Diagnosis and treatment of adults with community-acquired pneumonia. An official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. American journal of respiratory and critical care medicine, 2019.PMID 31573350
- [2]Wunderink RG, Niederman MS, Kollef MH, Shorr AF, et al. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: a randomized, controlled study. Clinical infectious diseases, 2012.PMID 22247123
- [3]Liu C, Bayer A, Cosgrove SE, Daum RS, et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clinical infectious diseases, 2011.PMID 21217178
- [4]Wunderink RG, Rello J, Cammarata SK, Croos-Dabrera RV, et al. Linezolid vs vancomycin: analysis of two double-blind studies of patients with methicillin-resistant Staphylococcus aureus nosocomial pneumonia. Chest, 2003.PMID 14605050
- [5]Rubinstein E, Cammarata S, Oliphant T, Wunderink R, et al. Linezolid (PNU-100766) versus vancomycin in the treatment of hospitalized patients with nosocomial pneumonia: a randomized, double-blind, multicenter study. Clinical infectious diseases, 2001.PMID 11170948
- [6]Kato H, Hagihara M, Asai N, Shibata Y, et al. Meta-analysis of vancomycin versus linezolid in pneumonia with proven methicillin-resistant Staphylococcus aureus. Journal of global antimicrobial resistance, 2021.PMID 33401013
- [7]Kalil AC, Metersky ML, Klompas M, Muscedere J, et al. Executive summary: management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clinical infectious diseases, 2016.PMID 27521441
- [8]Gillet Y, Issartel B, Vanhems P, Fournet JC, et al. Association between Staphylococcus aureus strains carrying gene for Panton-Valentine leukocidin and highly lethal necrotising pneumonia in young immunocompetent patients. Lancet, 2002.PMID 11888586
- [9]Lina G, Piémont Y, Godail-Gamot F, Bes M, et al. Involvement of Panton-Valentine leukocidin-producing Staphylococcus aureus in primary skin infections and pneumonia. Clinical infectious diseases, 1999.PMID 10524952
- [10]Enright MC, Robinson DA, Randle G, Feil EJ, et al. The evolutionary history of methicillin-resistant Staphylococcus aureus (MRSA). Proceedings of the National Academy of Sciences USA, 2002.PMID 12032344
- [11]Strauß L, Stegger M, Akpaka PE, et al. Origin, evolution, and global transmission of community-acquired Staphylococcus aureus ST8. Proceedings of the National Academy of Sciences of the United States of America, 2017.PMID 29158405
- [12]Chung DR, Huh K. Novel pandemic influenza A (H1N1) and community-associated methicillin-resistant Staphylococcus aureus pneumonia. Expert review of anti-infective therapy, 2015.PMID 25578884
- [13]Low DE, File TM Jr, Eckburg PB, Talbot GH, et al. FOCUS 2: a randomized, double-blinded, multicentre, phase III trial of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in community-acquired pneumonia. Journal of antimicrobial chemotherapy, 2011.PMID 21482568
- [14]Cosgrove SE, Sakoulas G, Perencevich EN, Schwaber MJ, et al. Comparison of mortality associated with methicillin-resistant and methicillin-susceptible Staphylococcus aureus bacteremia: a meta-analysis. Clinical infectious diseases, 2003.PMID 12491202
- [15]Self WH, Wunderink RG, Williams DJ, Barrett TW, et al. Comparison of clinical prediction models for resistant bacteria in community-onset pneumonia. Academic emergency medicine, 2015.PMID 25996620