ICU · Infectious Diseases
Acute severe pneumonia: bacteraemia and metastatic infection
Also known as Bacteraemic pneumonia · Metastatic infection from pneumonia · Endocarditis from bacteraemia · Septic emboli
Bacteraemia complicates 10-25% of CAP cases and significantly increases mortality (2-3x). Most common organisms causing bacteraemia: S. pneumoniae (1, 60-70%), S. aureus (including MRSA — highest metastatic risk), Haemophilus influenzae. Bacteraemia enables metastatic seeding to distant sites: endocarditis (25% of S. aureus bacteraemia), meningitis, vertebral osteomyelitis, septic arthritis, psoas abscess, splenic abscess. Management: prolonged antibiotic course (14 days minimum for S. aureus bacteraemia), repeat blood cultures until negative, search for metastatic foci (echocardiogram, imaging), source control if identified. Persistent bacteraemia 72h despite appropriate antibiotics: search for deep focus.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

SAQ — bacteraemic pneumonia
SAQ — Bacteraemic pneumococcal pneumonia with septic shock
10 minutes · 10 marks
A 64-year-old man with alcohol use disorder and asplenia (post-trauma splenectomy 5 years ago, no vaccinations since) presents with a 2-day history of rigors, pleuritic chest pain and confusion. He is in septic shock (MAP 55, lactate 5.0), SpO2 90% on room air, RR 32, with right lower lobe consolidation. Blood cultures drawn at ED grow gram-positive diplococci at 9 hours.
SAQ — Staphylococcus aureus bacteraemia from pneumonia
10 minutes · 10 marks
A 56-year-old woman with diabetes and a long-term haemodialysis tunnelled catheter presents with severe CAP and grows methicillin-sensitive Staphylococcus aureus (MSSA) in blood cultures. Echocardiogram shows a 1.2 cm vegetation on the aortic valve.
Clinical pearls
Red flags
Significance — why a positive blood culture changes everything
A positive blood culture in a patient with pneumonia transforms the illness from a localised pulmonary infection into a systemic, disseminated disease. Bacteraemia is documented in roughly 10–25% of all community-acquired pneumonia (CAP) admissions and in 30–60% of severe CAP requiring ICU. The haematogenous spread that defines bacteraemia is what creates the two features that make it dangerous: (1) a 2–3-fold higher mortality than non-bacteraemic CAP, and (2) the capacity for metastatic seeding of distant organs — endocarditis, meningitis, osteomyelitis, septic arthritis, and abscesses.[1][7]
The mortality signal is consistent across decades and continents. Non-bacteraemic pneumococcal pneumonia carries an inpatient mortality around 4–8%, whereas bacteraemic pneumococcal pneumonia mortality is 15–25%; in ICU-admitted bacteraemic CAP it may exceed 30%. The excess mortality is driven by septic shock, metastatic foci, and the higher virulence of organisms that achieve bloodstream invasion.[1]
For the exam, the single most important framing is: bacteraemic pneumonia is not just "pneumonia with a positive culture" — it is a bloodstream infection that happens to have entered through the lung, and it must be managed as a bacteraemia with mandatory search for metastatic seed.[7]
Epidemiology — who gets bacteraemic, and with what
Predisposing factors for bloodstream invasion
[7]Causative organisms
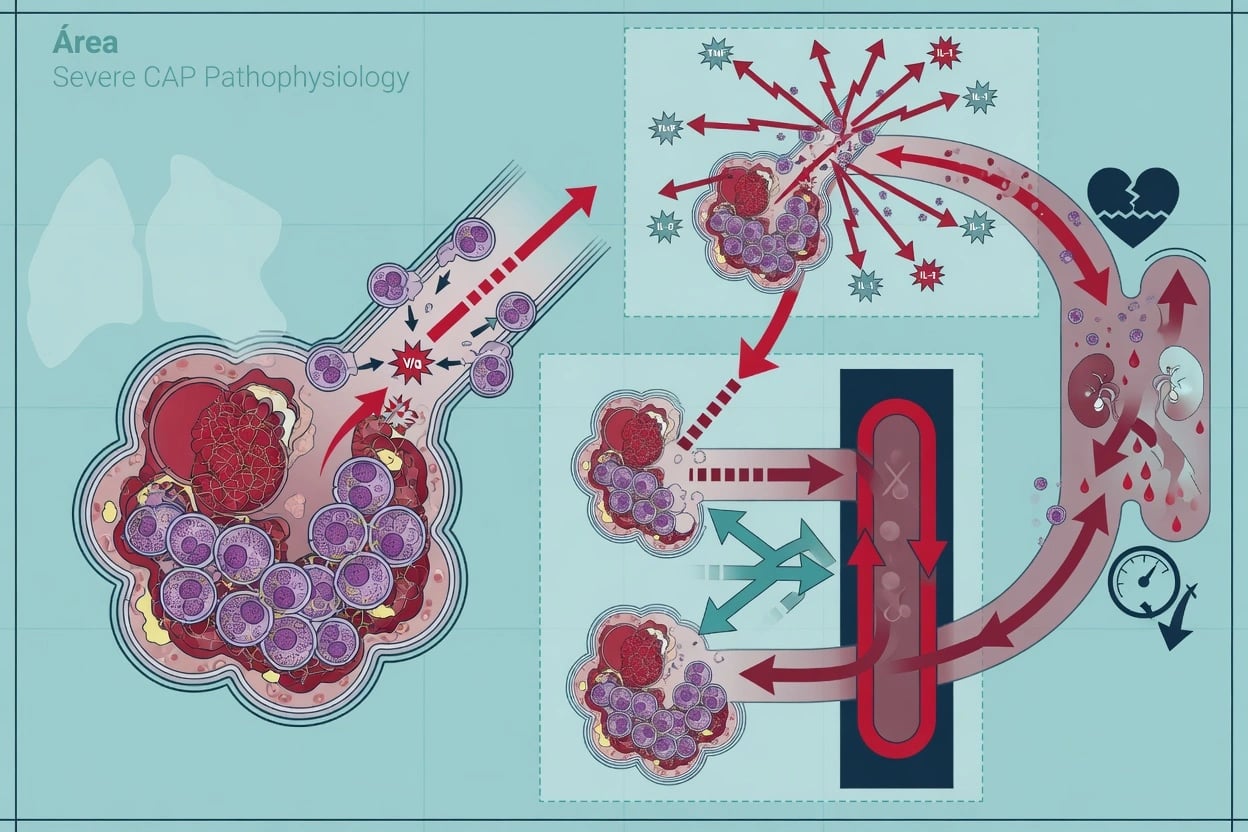
[2]Pathophysiology — how a lung infection becomes a bloodstream infection
Bacteraemia arises when the pathogen overwhelms local pulmonary defences and breaches the alveolar–capillary barrier. The sequence is: alveolar colonisation → intra-alveolar multiplication with neutrophil influx → disruption of the alveolar epithelium and basement membrane → entry into the pulmonary capillaries and lymphatics → systemic circulation. Once in the bloodstream, the organism's fate depends on the interaction between inoculum size, organism virulence, and host clearance (opsonisation, complement, splenic function).[6]
Metastatic seeding occurs when circulating organisms lodge in distant tissues. S. aureus is the master of metastasis because it expresses an armamentarium of adhesins (microbial surface components recognising adhesive matrix molecules — MSCRAMMs) that bind to fibrinogen, fibronectin, and platelets, allowing it to adhere to damaged endothelium, prosthetic material, and vegetations. The pneumococcus, by contrast, is far less adhesive to cardiac valves — hence endocarditis is uncommon (1–5%) and, when it occurs, tends to be a fulminant, acute, rapidly destructive process on a previously normal valve (often aortic).[3][4]
The practical consequence: the organism matters as much as the bacteraemia. A pneumococcal bacteraemia is largely treated with a standard-duration beta-lactam and a low-intensity metastatic search; a staphylococcal bacteraemia mandates echocardiography, prolonged therapy, and an active hunt for deep foci.[6]
Metastatic infection — ALWAYS look, the exam will ask
The cardinal rule of bacteraemic pneumonia: document clearance and search for metastatic foci. Metastatic infection is missed because the primary disease (pneumonia, septic shock) dominates the clinical picture. The intensivist's job is to keep asking, "Where else has it gone?"[6]
[6]Diagnosis — confirming bacteraemia and proving clearance
Blood cultures — technique and timing
Blood culture strategy in suspected bacteraemic pneumonia
Draw cultures BEFORE antibiotics
Two sets from two separate venepunctures, ideally before antibiotic exposure. Each hour delay to antibiotics increases mortality in septic shock, so do not delay therapy >45 min — but a single set drawn rapidly is better than none. Inoculate 8–10 mL per bottle (adult), both aerobic and anaerobic. Skin antisepsis with chlorhexidine/alcohol; allow to dry. Avoid femoral site (contamination).
Add ancillary diagnostics
Sputum Gram stain/culture, urinary antigen tests (pneumococcal and Legionella), respiratory viral PCR (influenza, SARS-CoV-2, RSV). In intubated patients, send endotracheal aspirate or BAL. Procalcitonin baseline (elevated >2 ng/mL supports bacterial/bacteraemic infection). Serum lactate to stratify severity.
Repeat cultures at 48–72 h
Repeat blood cultures every 48–72 h until negative to DOCUMENT CLEARANCE. Time to clearance is itself prognostic: S. aureus bacteraemia persisting >3 days despite appropriate therapy is an independent predictor of metastatic infection and mortality. Persistent positivity mandates the metastatic work-up (see above).
Trigger the metastatic work-up
If (a) organism is S. aureus or Pseudomonas, (b) bacteraemia persists >72 h, or (c) there is clinical/echo suspicion — perform: TOE, MRI spine if back pain, CT abdomen/pelvis for psoas/intra-abdominal abscess, MRI brain if neurological signs. The search is guided by symptoms but the default in S. aureus is TOE for everyone.
Define duration by clearance and focus
Day 1 of therapy = first day of negative blood cultures (for staphylococci) OR first day of appropriate therapy (for pneumococcus). Total duration is then set by organism and focus: pneumococcus 7–14 days, S. aureus uncomplicated 14 days minimum, endocarditis 4–6 weeks, osteomyelitis 6 weeks.
What a positive culture tells you
[3]Predicting bacteraemia when cultures are pending
[2]Management — antibiotics, source control, and the "complete the course" principle
Empiric therapy for suspected bacteraemic CAP
Management of bacteraemic pneumonia — the first 72 hours
Resuscitate and give antibiotics within 1 hour
Sepsis Six / Hour-1 bundle: oxygen to target SpO2 92–96% (88–92% in COPD), IV crystalloid 30 mL/kg for hypotension/lactate ≥4, early noradrenaline for vasoplegia, blood cultures drawn before antibiotics, broad-spectrum beta-lactam ± macrolide. Each hour of delay to appropriate antibiotics increases mortality in bacteraemic septic shock.
Choose empiric cover that captures the likely organism
Severe CAP: beta-lactam (benzylpenicillin, ceftriaxone, or cefotaxime) + macrolide (azithromycin/clarithromycin), OR respiratory fluoroquinolone (moxifloxacin) if penicillin-allergic. ADD anti-staphylococcal cover (flucloxacillin ± vancomycin/linezolid) if post-influenza, known MRSA, cavitation, IVDU, or rapidly progressive infiltrates. ADD anti-pseudomonal cover if bronchiectasis/CF/recent hospitalisation.
De-escalate at 48–72 h on culture results
Narrow to organism-directed therapy once sensitivities return: pneumococcus → benzylpenicillin/amoxicillin or ceftriaxone; MSSA → flucloxacillin (cefazolin alternative); MRSA → vancomycin (AUC 400–600) or linezolid (preferred for pneumonia). Do not continue broad empiric cover once the organism is known — antibiotic stewardship reduces resistance and C. difficile.
Confirm clearance with repeat cultures
Repeat blood cultures every 48–72 h until negative. For S. aureus, day 1 of therapy is the first day of a NEGATIVE culture; counting from here avoids under-treatment. Persistent bacteraemia >72 h triggers imaging for a deep focus (TOE ± CT/MRI).
Source control
Remove infected central lines (especially for S. aureus, Pseudomonas, Candida — organisms that form biofilm). Drain empyema/abscess, debride necrotic tissue, remove infected prosthetic hardware. Source control is as important as antibiotics in S. aureus bacteraemia.
Set total duration by organism and focus
Pneumococcus: 7–14 days. H. influenzae: 7–10 days. Uncomplicated MSSA bacteraemia: minimum 14 days. S. aureus with endocarditis: 4–6 weeks; osteomyelitis: 6 weeks; prosthetic valve IE: ≥6 weeks. Extend if metastatic focus, slow clearance, or immunocompromise. The era of automatic 7-day courses does NOT apply to staphylococcal bacteraemia.
Key management pitfalls
Prognosis — what determines who survives
Mortality by organism and setting
[7]Predictors of poor outcome
[2]Special situations
Post-influenza bacteraemic pneumonia
Secondary bacterial pneumonia (classically S. aureus, also pneumococcus, H. influenzae) is the major cause of death in influenza pandemics. In the 2009 H1N1 and subsequent seasonal epidemics, post-influenza S. aureus CAP was bacteraemic in 30–50% and carried 30–50% mortality. PVL-positive CA-MRSA is particularly devastating. The lesson: in any severe CAP during influenza season, add anti-staphylococcal cover empirically (vancomycin or linezolid + flucloxacillin).[2]
Asplenic / hyposplenic bacteraemia
Overwhelming post-splenectomy infection (OPSS) is most often pneumococcal, with a mortality of 50–70%. The classic teaching: a previously well asplenic patient collapses, bacteraemic, within 24–48 h of a flu-like illness. Prevention is everything: pneumococcal (PCV13 then PPSV23), Hib, meningococcal (ACWY + B) vaccines at least 2 weeks pre-elective splenectomy; lifelong standby antibiotics (amoxicillin or penicillin V); patient alert card and "fever = emergency, inject antibiotics then hospital" education.[1]
Bacteraemia in cirrhosis
Cirrhotic patients have impaired reticuloendothelial clearance and a high rate of spontaneous bacteraemia. Pneumococcal CAP in cirrhosis is commonly bacteraemic and may present as spontaneous bacterial peritonitis (SBP) from haematogenous seeding. Send ascitic fluid for cell count and culture in any febrile cirrhotic patient.[1]
Immunocompromise (neutropenia, transplant, anti-TNF)
Bacteraemic CAP in the immunocompromised broadens the differential to Pseudomonas and other GNB. Empiric cover must include anti-pseudomonal beta-lactam; consider adding a second agent. See the neutropenic sepsis topic.[1]
The evidence base
Severe community-acquired pneumonia — current ICU standard (Martin-Loeches & Torres, PMID 36517046)
Staphylococcus aureus bacteraemia — the complete review (Lodise et al, PMID 34402722)
AHA Infective Endocarditis Statement (Baddour et al, PMID 25977745)
ESC 2015 Infective Endocarditis Guidelines (Habib et al, PMID 26341945)
Exam-ready summary
[2]References
- [1]Martin-Loeches I, Torres A. Severe community-acquired pneumonia. Intensive care medicine, 2022.PMID 36517046
- [2]Asgeirsson H, Thalme A, Weiland O Staphylococcus aureus bacteraemia and endocarditis - epidemiology and outcome: a review. Infectious diseases (London, England), 2018.PMID 29105519
- [3]Baddour LM, Wilson WR, Bayer AS, et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation, 2015.PMID 26373316
- [4]Cahill TJ, Prendergast BD Infective endocarditis. Lancet (London, England), 2016.PMID 26341945
- [5]Fowler VG Jr, Sanders LL, Kong LK, et al. Infective endocarditis due to Staphylococcus aureus: 59 prospectively identified cases with follow-up. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 1999.PMID 10028079
- [6]Corey GR Staphylococcus aureus bloodstream infections: definitions and treatment. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 2009.PMID 19374581
- [7]Luján M, Gallego M, Belmonte Y, et al. Influence of pneumococcal serotype group on outcome in adults with bacteraemic pneumonia. The European respiratory journal, 2010.PMID 20150202