ICU · infectious-diseases
Pneumonia in the Immunocompromised Patient — Comprehensive ICU Management
Also known as Pneumonia in the immunocompromised host · Opportunistic pneumonia · Pulmonary infiltrates in the cancer patient · Pneumonia in transplant recipients · Pneumonia in haematological malignancy · Invasive pulmonary aspergillosis · Pneumocystis jirovecii pneumonia · CMV pneumonitis
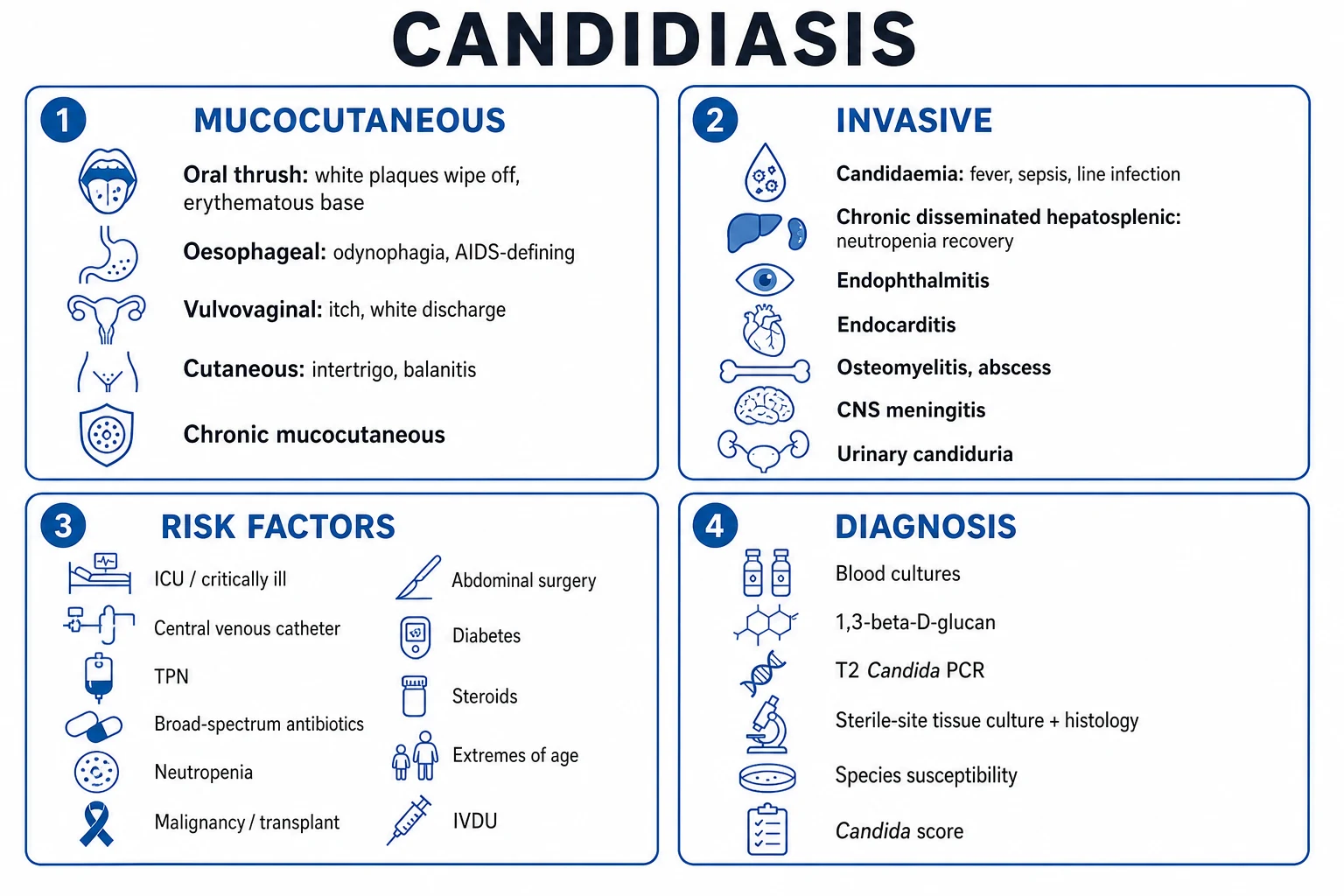
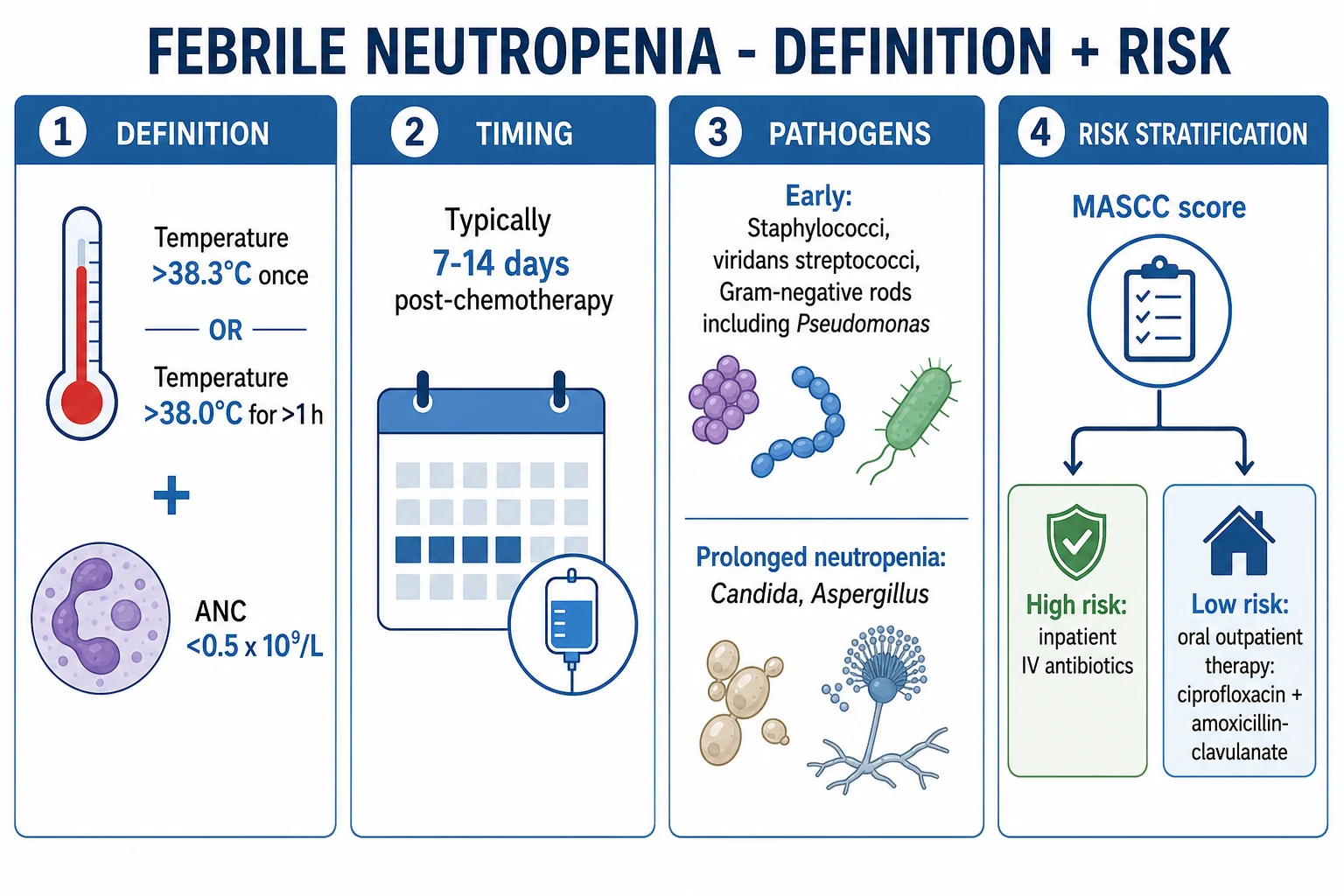
Pneumonia in the immunocompromised host (non-HIV) — haematological malignancy, stem-cell/solid-organ transplant, prolonged steroids, cytotoxic chemotherapy, biologics. The pathogen spectrum is dictated by the SPECIFIC IMMUNE DEFECT: (1) NEUTROPENIA (post-chemo, <0.5 x 10^9/L) - Pseudomonas aeruginosa, other gram-negative bacilli, invasive pulmonary aspergillosis, Candida, mucositis-related viridans streptococci; (2) T-CELL DEFECT (transplant calcineurin inhibitors, fludarabine, alemtuzumab) - Pneumocystis jirovecii (PCP), CMV, Legionella, Nocardia, Cryptococcus, mycobacteria; (3) B-CELL / HUMORAL DEFECT (CLL, myeloma, post-rituximab) - encapsulated bacteria — Streptococcus pneumoniae, Haemophilus influenzae; (4) PROLONGED STEROIDS (20 mg/day prednisone 4 weeks) - PCP, Nocardia, Aspergillus. The intensivist's task: (1) classify the immune defect, (2) get a diagnostic BAL EARLY (galactomannan for Aspergillus, (1-3)-beta-D-glucan for PCP/fungal, CMV PCR, respiratory virus panel, bacterial + fungal + mycobacterial culture), (3) start BROAD EMPIRIC THERAPY — anti-pseudomonal beta-lactam + empiric antifungal (caspofungin for Candida, voriconazole for suspected mould) + ganciclovir if CMV likely + co-trimoxazole if PCP possible + reduce immunosuppression, (4) prefer NIV over intubation (lower VAP/mortality), (5) prophylaxis — co-trimoxazole (PCP), posaconazole (Aspergillus), valganciclovir (CMV). Mortality 20-50% — far higher than immunocompetent CAP. Early appropriate (pathogen-directed) therapy is the single biggest modifiable determinant of survival.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

Overview
The cardinal principle is that the immune defect predicts the pathogen, and the pathogen predicts the therapy. A neutropenic leukaemia patient 10 days post-induction with a cavitating lung lesion has invasive aspergillosis until proven otherwise; a renal transplant recipient 3 months post-operatively on tacrolimus with diffuse ground-glass infiltrates and hypoxaemia out of proportion to the CXR has PCP or CMV until proven otherwise. Unlike CAP — where a syndromic "cover typicals + atypicals" approach is adequate — immunocompromised pneumonia demands a structured, defect-specific differential and an early invasive diagnostic (bronchoalveolar lavage), because the consequences of treating the wrong pathogen for 48-72 hours are fatal, and because half of these patients have an organism (fungal, viral, opportunistic) that no routine empiric antibiotic will reach.[2]
The immune-defect framework — pathogens follow the defect
[5] [5]Diagnostic approach — image, sample, send the full panel
Early chest imaging and an invasive diagnostic (BAL) are the two highest-yield manoeuvres. Do not manage immunocompromised pneumonia "empirically only" — the diagnosis is almost never made on clinical grounds alone, and empiric therapy that misses a mould or a virus is fatal.[5]
Imaging
- High-resolution CT chest is the imaging modality of choice (chest X-ray is normal or non-specific in up to 50% early). Get a CT within hours of admission.
- Halo sign — nodule surrounded by ground-glass attenuation = alveolar haemorrhage around an area of angioinvasive mould = invasive pulmonary aspergillosis (classic in neutropenia).[6]
- Air-crescent sign — crescent of air rimming a necrotic nodule = late angioinvasive aspergillosis (appears as neutrophils recover).
- Reversed halo / atoll — central ground-glass with peripheral consolidation = organising pneumonia; can be PCP or Mucorales.
- Diffuse bilateral ground-glass = PCP or CMV (also drug-induced pneumonitis, pulmonary haemorrhage).
- Tree-in-bud = endobronchial spread — bacterial bronchopneumonia, Nocardia, mycobacteria.
- Multiple nodules ± cavitation = Aspergillus, Nocardia, Cryptococcus, septic emboli, metastatic infection.
Bronchoalveolar lavage — the single most important diagnostic test
BAL is indicated early (within 24-48 h) in any immunocompromised patient with pulmonary infiltrates of unclear aetiology, or who fails to respond to 48-72 h of empiric therapy. It carries a low complication rate (bleeding in thrombocytopenic patients — transfuse platelets to keep >50 before scope) and a diagnostic yield of 40-70%.[2]
Serum biomarkers complement BAL: serum galactomannan (OD index >=0.5, twice) is a useful screen for invasive aspergillosis in neutropenic patients; serum (1-3)-beta-D-glucan is elevated in PCP and deep fungal infection (negative in Cryptococcus/Mucorales); LDH is characteristically very high in PCP; 1,3-beta-D-glucan + procalcitonin help separate fungal/viral from bacterial. Blood cultures (2 sets + line cultures) are still mandatory — bacteraemia with Pseudomonas or Candida changes duration and prognosis.[2]
Management protocol — the first 24 hours
[2]Empiric therapy by suspected syndrome
The empiric regimen is built by layering agents onto an anti-pseudomonal backbone according to the most likely pathogen(s) implied by the immune defect and imaging. Start broad, then narrow within 48-72 h using BAL results.[6]
Respiratory support — prefer NIV, avoid intubation when possible
[2]The evidence base (Antonelli 2000, Azoulay trials): in immunocompromised patients with pulmonary infiltrates and hypoxaemia, early NIV lowered the intubation rate and 90-day mortality compared with standard oxygen ± intubation. The message for the exam: reach for the BiPAP mask before the laryngoscope — but recognise NIV failure early (rising respiratory rate, rising PaCO2, falling pH, exhaustion) and intubate without delay.[2]
Prophylaxis — prevent the predictable
Prophylaxis is the single most effective intervention against opportunistic pneumonia and should be audited on every immunocompromised ICU admission (patients are often non-adherent or the prophylaxis was stopped).[1][4]
[1]SAQ — defect-driven differential in the allogeneic HSCT recipient
SAQ — Defect-driven differential and diagnostic approach in an immunocompromised lung
10 minutes · 10 marks
A 60-year-old man is day +90 after allogeneic haematopoietic stem-cell transplant for AML. He is on tacrolimus and prednisolone 1 mg/kg/day for grade II skin GVHD. Co-trimoxazole was stopped two weeks ago because of neutropenia. He presents with five days of dry cough, exertional dyspnoea and fever (38.9°C). On room air his SpO2 is 88% with an A-a gradient of 50 mmHg; the chest X-ray is subtly hyperinflated and unremarkable. High-resolution CT chest shows diffuse bilateral ground-glass opacification without nodules or cavitation.
SAQ — CMV pneumonitis in a high-risk solid-organ transplant recipient
SAQ — CMV pneumonitis in a D+/R- kidney transplant recipient
10 minutes · 10 marks
A 35-year-old man is two months after deceased-donor kidney transplant (donor CMV IgG-positive, recipient CMV IgG-negative). His immunosuppression is tacrolimus, mycophenolate mofetil and prednisolone. He was admitted for biopsy-proven acute cellular rejection one week ago and received a methylprednisolone pulse. He now has five days of fever, malaise, progressive dyspnoea, leucopenia (WCC 1.8 ×10^9/L) and thrombocytopenia. CT chest shows diffuse bilateral ground-glass opacities and scattered small nodules. Plasma CMV PCR is 350,000 IU/mL and bronchoalveolar lavage transbronchial biopsy shows cytomegalic cells with characteristic intranuclear owl's-eye inclusions.
Clinical pearls
Red flags
[2] [2]Prognosis
[3]The most powerful modifiable prognostic factor is early appropriate, pathogen-directed therapy, which is itself contingent on early invasive diagnosis. Host factors that compound mortality are severe neutropenia of long duration, high-intensity immunosuppression (GVHD, recent T-cell-depleting therapy), mechanical ventilation, multi-organ failure, and the underlying malignancy/transplant status.[1]
Key trials and evidence
ECIL-5 guidelines — Pneumocystis pneumonia in haematological malignancy and HSCT (PMID 27550990 / 27550991)
IDSA 2016 Aspergillosis guidelines — Patterson TF, et al. (PMID 27365388)
Maschmeyer & Donnelly — managing lung infiltrates in haematological malignancy (PMID 26729577)
Examiner densification notes
[1] [3]References
- [1]Cordonnier C, Cesaro S, Maschmeyer G, et al. Pneumocystis jirovecii pneumonia: still a concern in patients with haematological malignancies and stem cell transplant recipients (ECIL-5). J Antimicrob Chemother, 2016.PMID 27550990
- [2]Maschmeyer G, Donnelly JP. How to manage lung infiltrates in adults suffering from haematological malignancies outside allogeneic haematopoietic stem cell transplantation. Br J Haematol, 2016.PMID 26729577
- [3]Lehners N, Tabatabai J, Prifert C, et al. Long-term shedding of influenza virus, parainfluenza virus, respiratory syncytial virus and nosocomial epidemiology in patients with hematological disorders. PLoS One, 2016.PMID 26866481
- [4]Fishman JA. Pneumocystis jiroveci. Semin Respir Crit Care Med, 2020.PMID 32000290
- [5]Alanio A, Hauser PM, Lagrou K, et al. ECIL guidelines for the diagnosis of Pneumocystis jirovecii pneumonia in patients with haematological malignancies and stem cell transplant recipients. J Antimicrob Chemother, 2016.PMID 27550991
- [6]Patterson TF, Thompson GR 3rd, Denning DW, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis, 2016.PMID 27365388