ICU · Infectious Diseases
Acute severe community-acquired pneumonia: pneumonia in immunocompromised non-HIV patients
Also known as Pneumonia in transplant recipients · Pneumonia in haematological malignancy · Pneumonia in steroid-treated patients · Opportunistic pneumonia
Pneumonia in non-HIV immunocompromised patients (transplant, haematological malignancy, steroids, biologics) has broader pathogen spectrum and higher mortality than CAP in immunocompetent patients. Organisms depend on type and timing of immunosuppression: early post-transplant (1 month): hospital-acquired (Gram-negative, MRSA). 1-6 months: opportunistic (CMV, PCP, Aspergillus, Nocardia, Legionella). 6 months: community-acquired (same as immunocompetent) + recurrent opportunistic. Management: broad empiric coverage (covers typical + atypical + opportunistic), BAL for diagnosis (send comprehensive panel: bacterial, viral, fungal, mycobacterial), reduce immunosuppression if possible, consider adjunctive therapies (G-CSF for neutropenia, IVIG for humoral deficiency). Mortality 20-50%.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags

SAQ — pneumonia in the neutropenic transplant patient
SAQ — Pulmonary infiltrate in a neutropenic stem-cell transplant patient
10 minutes · 10 marks
A 48-year-old man is day 18 after allogeneic stem-cell transplant for AML. His ANC is 0.1 x10^9/L. He has been febrile (39C) on broad-spectrum meropenem for 4 days and now develops pleuritic chest pain, haemoptysis and a new oxygen requirement (SpO2 90% on room air). CT chest shows several nodules, one with a surrounding 'halo' of ground-glass opacification. Serum galactomannan index is 0.7. He is on fluconazole prophylaxis.
SAQ — CMV pneumonitis post-lung transplant
10 minutes · 10 marks
A 55-year-old man, 3 months after bilateral lung transplant, presents with a 5-day history of fever, dry cough, progressive dyspnoea and leucopenia. He is on tacrolimus, mycophenolate and prednisolone, and valganciclovir prophylaxis. CT chest shows diffuse bilateral ground-glass opacities and multiple small nodules. BAL CMV PCR is positive at 250,000 IU/mL; transbronchial biopsy shows cytomegalic cells with viral inclusions.
Clinical pearls
Red flags
Categories of immune defect — the framework that predicts the pathogen
The single most useful mental model for the immunocompromised lung is to map the specific immune defect to the class of pathogen it fails to control. A "broad-spectrum everything" approach is a starting point, but the differential narrows rapidly once you ask: what arm of immunity is missing, and for how long?[2]
Neutropenic
Phagocyte defect
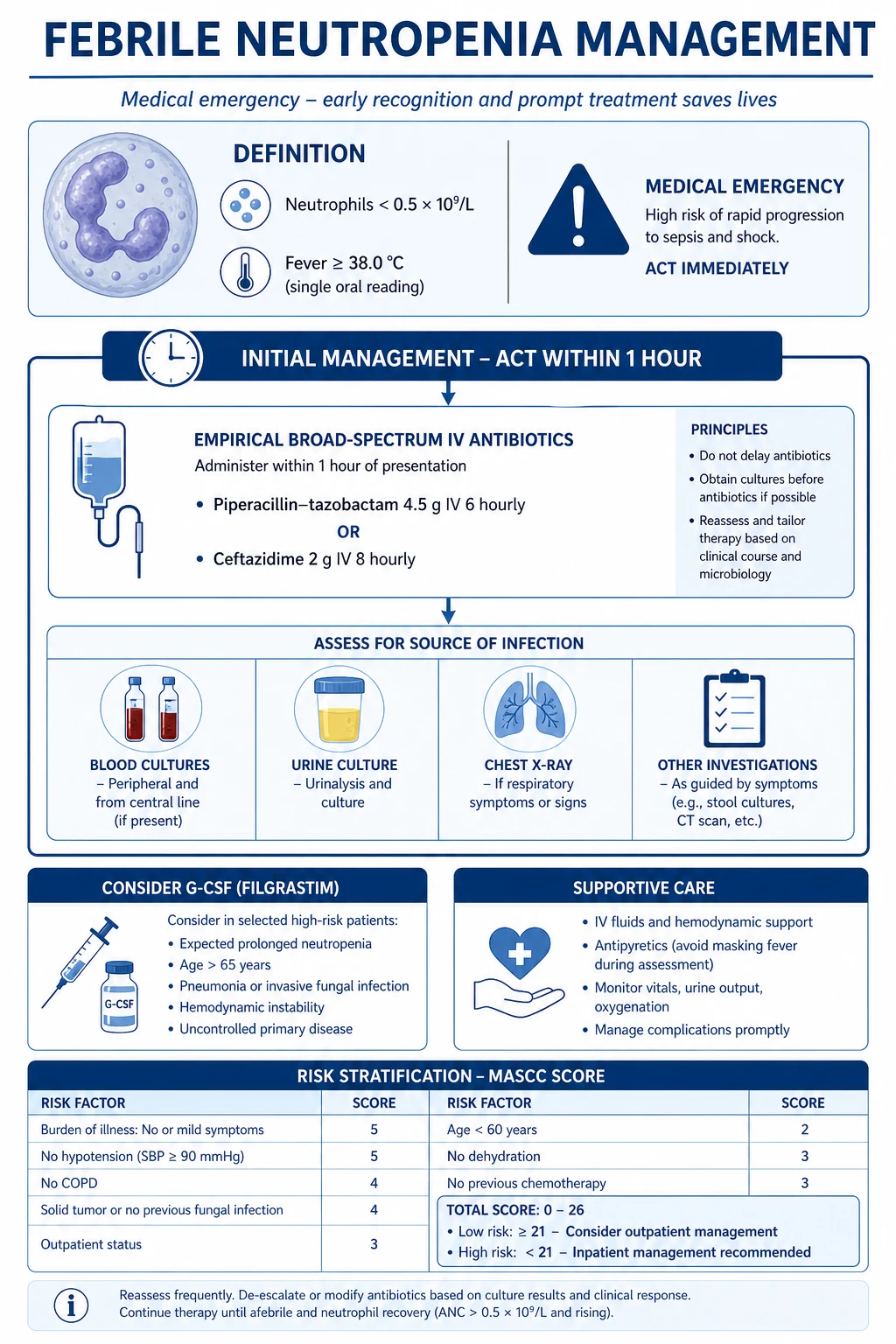
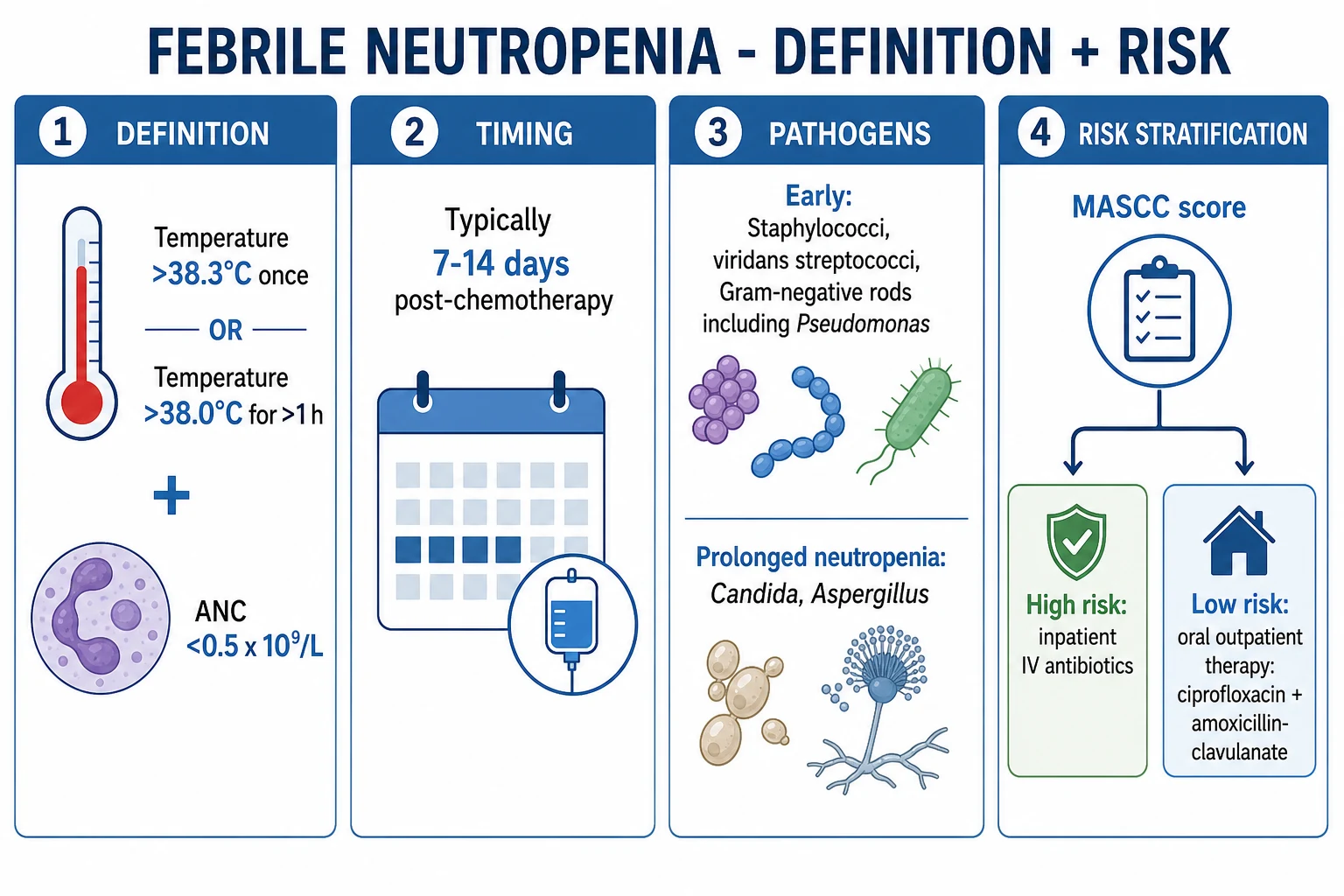
- Absolute neutrophil count <0.5 × 10⁹/L (or <1.0 with predicted nadir <0.5) — the classic chemo / HSCT window
- Causes: cytotoxic chemotherapy for AML/MDS induction, allo-HSCT pre-engraftment, aplastic anaemia, severe aplastic drug reactions (clozapine, anti-thyroidals), congenital neutropenia
- Risk proportional to depth (<0.1 catastrophic) and duration (>7-10 days = mould territory)
- Signature pathogens: Pseudomonas aeruginosa, E. coli, Klebsiella, other enteric Gram-negatives; Staph aureus, viridans streptococci, coag-neg staph; then INVASIVE MOULDS — Aspergillus, Mucorales — once neutropenia is prolonged
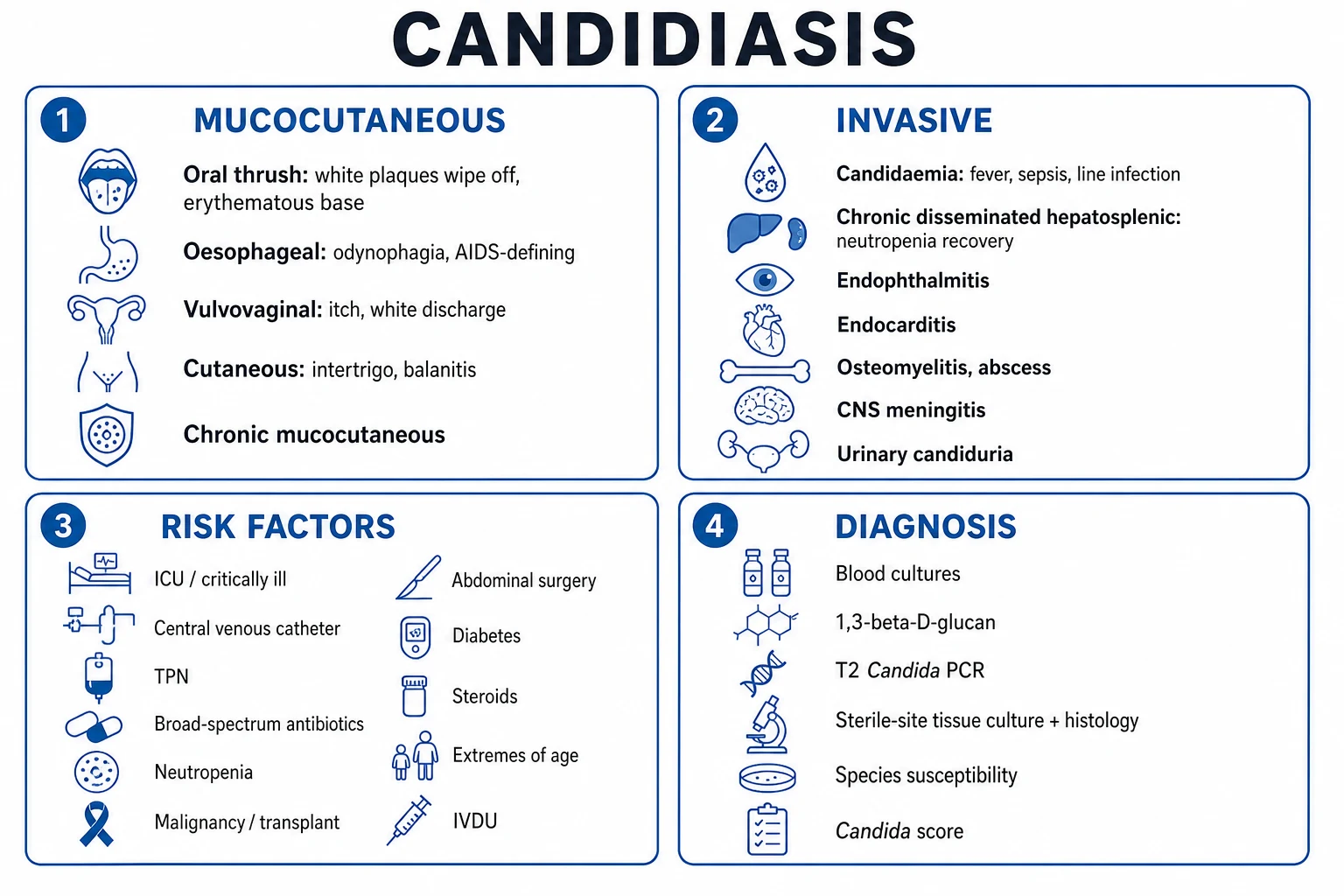
- Candida once mucosal barrier breached (mucositis, CVC); septate acute-angle hyphae = Aspergillus; broad ribbon-like non-septate hyphae = Mucorales
- Physical findings muted — no pus, minimal sputum, dull chest — because neutrophils are absent; a "dry" infiltrate on imaging is a clue
Humoral / B-cell
Antibody defect
- Defective opsonisation of encapsulated extracellular bacteria
- Causes: multiple myeloma, CLL, lymphoma, nephrotic syndrome, protein-losing enteropathy, post-rituximab (B-cell depletion, hypogammaglobulinaemia for 6-12 months), post-CD19 CAR-T, CVID, X-linked agammaglobulinaemia
- Signature pathogens: Streptococcus pneumoniae, Haemophilus influenzae type b, Neisseria meningitidis, Moraxella, Campylobacter, enteroviruses (chronic meningoencephalitis), Giardia
- Check serum immunoglobulins (IgG, IgA, IgM) and specific vaccine antibody responses; many centres give replacement IVIG when IgG is low and infections recurrent
- Functional hyposplenism (sickle cell, coeliac, post-rituximab) behaves like asplenia — see splenectomised column
T-cell / cellular
Cell-mediated defect
- Defective intracellular pathogen control — the opportunistic "big five" live here
- Causes: solid organ transplant on calcineurin inhibitors + antimetabolites + steroids; allo-HSCT especially with GVHD; high-dose corticosteroids (>20 mg prednisolone >4 weeks, or equivalent); anti-TNF biologics (infliximab, adalimumab, etanercept); purine analogues (fludarabine, cladribine, clofarabine); alemtuzumab; HIV/AIDS (covered in a separate topic)
- Signature pathogens: Pneumocystis jirovecii, CMV (and other herpesviruses), Nocardia, Cryptococcus, Toxoplasma gondii; also Listeria, Salmonella, endemic mycoses (Histoplasma, Coccidioides), mycobacteria (TB and NTM)
- CD4 lymphocytopenia (absolute or drug-induced) is the common thread — <200 cells/microL is the classic PCP/toxoplasma threshold
Splenectomised / asplenic
Opsonisation + filter loss
- Loss of splenic macrophage clearance of opsonised bacteria + impaired IgM response to encapsulated organisms
- Causes: surgical splenectomy (trauma, ITP, hereditary spherocytosis), functional hyposplenism (sickle cell, post-chemo, coeliac, radiation), post-rituximab (transient)
- Signature syndrome: OVERWHELMING POST-SPLENECTOMY INFECTION (OPSI) — encapsulated bacteria, minutes-to-hours progression, DIC, Waterhouse-Friderichsen (adrenal haemorrhage), mortality up to 50-70%
- Classic organisms: Streptococcus pneumoniae (~50-90%), Haemophilus influenzae type b, Neisseria meningitidis; also Capnocytophaga canimorsus (dog bites), Babesia, malaria (severe)
- Howell-Jolly bodies on blood film = functional asplenia; prophylaxis = vaccines (pneumococcal, Hib, meningococcal ACWY + B, influenza annually) + penicillin V 500 mg BD (lifelong in high-risk)
Barrier / device
Anatomic defect
- Mucositis (chemo), central venous catheter, recent surgery, endotracheal tube, urinary catheter
- Signature: Staphylococcus aureus (incl. MRSA), coagulase-negative staph (line), enteric Gram-negatives, Candida (mucosal/line), anaerobes (aspiration)
- Often coexists with neutropenia — line removal + broad cover; think Staph lugdunensis (virulent coag-neg) with line infection
The pathogen calendar — timing after transplantation
For the solid-organ transplant or allogeneic HSCT recipient, the interval since transplant is a powerful predictor. Three classic windows:[2]
Post-transplant infection timeline (solid organ / HSCT)
0 to 1 month
DONOR-DERIVED and NOSOCOMIAL infections dominate. Hospital-acquired / ventilator-associated pneumonia (Pseudomonas, Acinetobacter, ESBL/CRE enteric Gram-negatives, MRSA), candidaemia from central lines, donor-transmitted (e.g. donor Aspergillus, TB, West Nile, lymphocytic choriomeningitis). Wound and anastomotic infections (especially liver, pancreas, lung transplants). Empiric cover mirrors nosocomial sepsis: anti-pseudomonal beta-lactam ± MRSA agent.
1 to 6 months
THE OPPORTUNISTIC WINDOW — peak immunosuppression. This is where CMV (1-4 months), PCP (2-6 months), EBV/PTLD, invasive aspergillosis and other moulds, Nocardia, Cryptococcus, Toxoplasma, endemic mycoses (reactivation), BK/JC viruses, and Listeria appear. Empiric therapy must reach for the opportunists: add co-trimoxazole cover (PCP/Nocardia/Toxoplasma), consider ganciclovir if CMV-positive, add a mould-active azole (voriconazole/isavuconazole) if neutropenic or steroid-heavy.
> 6 months
COMMUNITY-ACQUIRED pneumonia re-emerges (S. pneumoniae, H. influenzae, respiratory viruses, Legionella, atypicals) PLUS late opportunistic infection in those still heavily immunosuppressed (chronic rejection treatment, GVHD, ongoing high-dose steroids). Cryptococcus, CMV colitis/retinitis, and JC virus (PML) cluster here. Empiric therapy approaches standard CAP therapy but maintain opportunistic suspicion.
After HSCT specifically
Pre-engraftment (<day +30): neutropenic moulds and mucositis-related bacteraemia. Early post-engraftment (+30 to +100): CMV, PCP, adenovirus, HHV-6, early Aspergillus. Late (>+100): if chronic GVHD on heavy immunosuppression — encapsulated bacteria (functional asplenia post-hypersplenism), PCP, late CMV/EBV-PTLD, and respiratory viruses cause severe disease. Pneumococcal re-vaccination after HSCT follows a 3-dose Prevnar then Pneumovax schedule.
Neutropenic pneumonia — the invasive-mould paradigm
In the profoundly neutropenic patient (ANC <0.5, especially <0.1, for >7-10 days) a new pulmonary infiltrate is invasive mould until proven otherwise. The two rivals are Aspergillus (far commoner) and the Mucorales (Rhizopus, Mucor, Lichtheimia) — distinguishing them is decisive because Mucorales are intrinsically resistant to voriconazole.[3]
Aspergillus
Septate acute-angle hyphae
- Invasive pulmonary aspergillosis (IPA) — angioinvasive: vessel invasion → thrombosis, infarction, haemorrhagic nodules
- CT: halo sign (nodule with ground-glass halo = haemorrhage) early (<5 days), evolving to AIR-CRESCENT sign (late, ~day 10-14, neutrophil recovery)
- Diagnosis: serum + BAL galactomannan (Aspergillus cell wall polysaccharide; BAL > serum sensitivity), beta-D-glucan positive, culture/histology with septate acute-angle hyphae invading tissue
- First-line: voriconazole (or isavuconazole). Alternatives: liposomal amphotericin B, posaconazole, echinocandin as salvage combination
- Mortality 40-60% in the neutropenic/HSCT setting even with treatment
Mucorales
Broad ribbon non-septate
- Pulmonary mucormycosis — even more angioinvasive; rapidly progressive, frequently complicated by vascular invasion, cavitation, and (classic) reversal-halo sign on CT
- INHERENTLY RESISTANT to voriconazole and fluconazole — voriconazole PROPHYLAXIS failure in a mould-suspected patient raises Mucorales concern
- Risk factors: prolonged profound neutropenia, diabetic ketoacidosis (rhino-orbital-cerebral form), deferoxamine/iron overload, glucocorticoids
- Diagnosis: tissue biopsy with broad, ribbon-like, pauci-septate hyphae branching at right angles; galactomannan and beta-D-glucan are NEGATIVE (useful discriminator); culture difficult
- Treatment: urgent SURGICAL DEBRIDEMENT (where feasible) + high-dose LIPOSOMAL AMPHOTERICIN B (5-10 mg/kg/day); isavuconazole as step-down; reverse immunosuppression; consider salvage posaconazole. Mortality very high (50-85%)
Candida lung
Rare primary pneumonia
- TRUE primary Candida pneumonia is RARE — most "Candida in sputum/BAL" is colonisation; diagnosis requires tissue invasion on biopsy
- Think haematogenous dissemination (chronic disseminated candidiasis, hepatosplenic) with multiple nodules in a post-engraftment patient, or follow-up of candidaemia
- Treat per susceptibility: echinocandin (caspofungin/micafungin/anidulafungin) first-line; step down to fluconazole/voriconazole if stable and susceptible
Bacterial / viral
Do not forget
- Gram-negative bacteraemia (Pseudomonas, E. coli, Klebsiella, Stenotrophomonas) still causes a third of neutropenic lung infiltrates; viridans streptococci (mucositis) cause shock
- Respiratory viruses (RSV, influenza, parainfluenza, adenovirus, metapneumovirus) are devastating in neutropenia — send multiplex PCR
- CMV reactivation may coexist with mould — always send CMV PCR alongside galactomannan
Invasive pulmonary aspergillosis — diagnostic and therapeutic detail
IPA diagnostic pathway (revised EORTC/MSG + ESCMID/ECMM/ERS)
Recognise the host
Prolonged profound neutropenia (AML/MDS induction, allo-HSCT), high-dose corticosteroids (≥0.3 mg/kg prednisolone-equivalent for ≥3 weeks is the modern ECIL threshold for PCP; mould risk rises steeply above ~1 mg/kg), GVHD, lung/liver transplant, advanced COPD on steroids, critical illness with influenza or COVID-19 (IAPA/CAPA — increasingly recognised).
Clinical features
Pleuritic chest pain, haemoptysis (mild to massive — angioinvasion), new pleural rub, dry cough, fever refractory to broad-spectrum antibiotics, and a clinical picture "worse than the X-ray".
CT chest — early (first 1-7 days)
HALO SIGN: a solid nodule surrounded by a ground-glass halo of haemorrhagic infarction — the classic early IPA finding (seen in up to 90% of neutropenic IPA within 5 days). Multiple nodules, wedge-shaped peripheral infarcts, segmental/subsegmental consolidation.
CT chest — late (after ~10-14 days, neutrophil recovery)
AIR-CRESCENT sign: separation of necrotic lung from viable parenchyma — indicates recovery but also a window of risk for catastrophic haemoptysis.
Galactomannan
Aspergillus cell-wall polysaccharide detected by Platelia EIA. SEND BOTH serum AND BAL — BAL galactomannan is markedly more sensitive (optical index cutoff ≥1.0). False-POSITIVE with piperacillin-tazobactam and amoxicillin-clavulanate (historical contamination, now rare), and with Bifidobacterium/Penicillium in gut (neonates). False-NEGATIVE with mould-active prophylaxis (posaconazole, isavuconazole).
Beta-D-glucan
Pan-fungal marker (Aspergillus, Candida, Pneumocystis; NOT Mucorales or Cryptococcus). False-positives: IVIG, albumin, gauze/dialysis cellulose, certain antibiotics. Useful as a rule-out; combined with galactomannan it strengthens IPA probability.
Histopathology / culture
Definitive (proven) IPA requires tissue showing septate acute-angle-branching hyphae invading parenchyma WITH consistent culture/molecular identification. BAL cytology and transbronchial biopsy raise yield. A "probable" diagnosis (host + clinical + mycological) is the working standard and justifies full treatment.
Start therapy at first suspicion
Do not wait for proof — empiric/pre-emptive mould-active therapy while diagnostic workup proceeds. Each day of delay increases mortality.
IPA treatment protocol
First-line: voriconazole
Loading 6 mg/kg IV BD × 2 doses, then 4 mg/kg IV BD (or 200-300 mg PO BD when tolerating). Voriconazole improved survival and response vs amphotericin B in the landmark Herbrecht NEJM trial (53% vs 32% satisfactory response; survival 71% vs 58%). Therapeutic drug monitoring essential (target trough 1-5.5 mg/L) — metabolism is CYP2C19-dependent (genetic polymorphism → 20-fold variability).
Alternative first-line: isavuconazole
Loading 200 mg BD × 6 doses (2 days), then 200 mg OD. SECURE trial: non-inferior to voriconazole for IPA/mucormycosis, BETTER tolerated (no visual disturbance, fewer hepatotoxic discontinuations, shorter QT). Mould-active INCLUDING Mucorales. Fewer CYP interactions than voriconazole.
Salvage / combination
Liposomal amphotericin B 3-5 mg/kg/day IV. Echinocandin (caspofungin) as salvage add-on (weak evidence). Combination voriconazole + echinocandin may help in extensive disease. Surgical resection for localised cavitating lesions with haemoptysis risk.
Duration
Minimum 6-12 weeks; continue until clinical/radiological resolution AND immune reconstitution (ANC recovery, immunosuppression tapered). Step IV→oral once tolerating and improving. Secondary prophylaxis if immunosuppression continues.
Reverse immunosuppression
Reduce steroids as rapidly as the underlying disease allows; G-CSF/GM-CSF for neutrophil recovery; manage GVHD. The single biggest determinant of outcome is immune reconstitution.
Monitor response
Repeat galactomannan (trend should fall), CT (look for resolution of halo/consolidation; new air-crescent = recovery not failure), inflammatory markers. Persistent fever + rising galactomannan = reassess for Mucorales or resistance.
Voriconazole vs amphotericin B for invasive aspergillosis (Herbrecht, NEJM 2002)
Randomised open-label multicentre trial, 277 patients
Population: Proven/probable invasive aspergillosis (mostly haematological malignancy, neutropenia, HSCT)
Key finding
Voriconazole superior: satisfactory response 53% vs 32% (absolute difference +21%). Survival at 12 weeks 71% vs 58%. Fewer severe adverse events.
Practice change
Voriconazole became first-line therapy for invasive aspergillosis — better outcomes and survival than amphotericin B, with less nephrotoxicity.
Antifungal agents compared in the immunocompromised lung
Voriconazole
Aspergillus first-line
- Aspergillus first-line; activity vs Scedosporium, Fusarium; NO Mucorales
- Visual disturbances (~30% — bright lights, colour changes, reversible), hepatotoxicity, photosensitivity, skin cancer (squamoproliferative — sun protection mandatory), periostitis (fluoride)
- CYP2C19 polymorphism — THERAPEUTIC DRUG MONITORING essential (trough 1-5.5 mg/L)
- MAJOR interactions with CNIs (tacrolimus dose ~halve; cyclosporine to one-third), sirolimus (contraindicated), warfarin, opioids
Isavuconazole
Mould incl. Mucorales
- Aspergillus AND Mucorales — broadest mould cover of the azoles
- Better tolerated than voriconazole; SHORTENS QT (unique — safe in long-QT; avoid in familial short-QT); fewer visual/hepatic effects
- Fewer CYP interactions than voriconazole but still interacts with CNIs (less dramatically) and rifampicin (contraindicated)
- No routine TDM required; convenient OD dosing after load
Posaconazole
Prophylaxis / Mucorales
- Mould-active INCLUDING Mucorales; prophylaxis mainstay in AML/MDS induction and GVHD (NEJM 2007 Cornely — reduced invasive fungal infection and improved survival vs fluconazole/itraconazole)
- Oral suspension absorption food- and pH-dependent (need acidic stomach — avoid PPIs, take with fatty meal); the delayed-release tablet and IV give reliable levels
- Use as prophylaxis OR step-down therapy; TDM advisable on suspension
Liposomal amphotericin B
Broad incl. Mucorales
- Broadest spectrum mould (Aspergillus, Mucorales, endemic mycoses, Leishmania)
- 3-5 mg/kg/day IV (up to 10 mg/kg/day for Mucorales); liposomal formulation markedly less nephrotoxic than deoxycholate
- Toxicity: nephrotoxicity (additive with CNIs), electrolyte wasting (K, Mg), infusion reactions, anaemia
- Pre-medicate; monitor U&E and Mg; saline loading reduces nephrotoxicity
Echinocandins
Candida / salvage
- Caspofungin, micafungin, anidulafungin — inhibit beta-1,3-glucan synthase
- First-line for invasive candidiasis/candidaemia; SALVAGE (combination) for refractory aspergillosis
- NOT effective alone for Aspergillus or Mucorales as primary therapy; INEFFECTIVE for Pneumocystis (trophozoite lacks target) and Cryptococcus
- Well tolerated; hepatic dose adjustment (caspofungin) for moderate Child-Pugh C
Posaconazole prophylaxis in neutropenic AML/MDS (Cornely, NEJM 2007)
Randomised double-blind multicentre trial, 602 patients
Population: Patients receiving chemotherapy for AML or MDS with prolonged neutropenia
Key finding
Posaconazole reduced invasive fungal infection (2% vs 8%) — driven by fewer invasive aspergillosis — and significantly improved overall survival (survival 87% vs 82% at 100 days).
Practice change
Posaconazole prophylaxis in high-risk neutropenic AML/MDS reduces invasive mould infection and improves survival — the evidence base for routine prophylaxis in this group.
Pneumocystis jirovecii pneumonia in the non-HIV host — what is different
PCP is covered in depth in its own topic; the points below are the non-HIV-specific distinctions the examiner expects you to know.[2]
Risk in non-HIV
Higher inflammatory burden
- Prednisolone-equivalent ≥20 mg/day for ≥4 weeks (classic), or ≥0.3 mg/kg/day for ≥3 weeks (newer ECIL/AST threshold)
- Solid organ transplant (especially lung, heart-lung), allo-HSCT (peak 1-6 months, GVHD), anti-TNF biologics, rituximab, fludarabine/cladribine, idiopathic CD4 lymphocytopenia
- Most centres give universal co-trimoxazole prophylaxis for 6-12 months post-SOT (lifelong in lung) and post-HSCT until ≥6 months post-engraftment (longer with GVHD)
Presentation
More acute than HIV-PCP
- Onset over DAYS (not the weeks typical of HIV-PCP) — lower organism burden but brisker neutrophilic inflammation
- Often presents straight to ICU with respiratory failure — diagnosis frequently delayed because PCP is not suspected
- CXR may be normal early; CT shows patchy ground-glass (often sparing subpleural regions)
- Pneumothorax / cystic changes common and dangerous in the ventilated patient
Diagnosis
BAL yield lower
- LOWER organism burden → induced sputum and BAL sensitivity LOWER than in HIV — may need transbronchial biopsy
- Beta-D-glucan elevated (also in Candida/Aspergillus — not specific); LDH often high and trends with disease
- BAL PCR highly sensitive but cannot distinguish colonisation from disease — use with cytology/immunofluorescence
Mortality
30-50% — worse than HIV
- Non-HIV PCP mortality 30-50% (vs 10-20% in HIV) despite lower organism burden — inflammation kills
- Higher intubation rates; once ventilated, mortality approaches 50-60%
- Lower threshold to treat empirically and to add steroids; consider broader/longer steroid taper to avoid rebound
PCP management — the ICU essentials
Co-trimoxazole (TMP-SMX) — first-line
High-dose 15-20 mg/kg/day of the TRIMETHOPRIM component (≈ 75-100 mg/kg/day sulfamethoxazole), IV or PO, for 21 days. Typically 4 double-strength (800/160) tablets QID for a 70 kg adult. Switch to oral when tolerating and improving. Monitor: FBC (marrow suppression), U&E (hyperkalaemia from TMP amiloride-like distal tubular effect, AKI), LFTs, glucose. Side effects: rash incl. SJS, crystalluria, hepatitis.
Add CORTICOSTEROIDS if PaO₂ <70 mmHg or A-a gradient >35
Prednisolone 40 mg BD × 5 days → 40 mg OD × 5 days → 20 mg OD × 11 days (total 21 days, matching the antibiotic course), OR methylprednisolone 30/30/15 mg IV equivalents if NBM. Give WITH the first antibiotic dose — do not wait. Mechanism: blunts the inflammatory alveolitis provoked by organism lysis at days 3-5. Reduces mortality and need for ventilation in moderate-severe PCP (Cochrane). In non-HIV PCP consider a slower taper to avoid rebound.
NIV / HFNO preferred over intubation
Immunocompromised patients with hypoxaemic respiratory failure do better with non-invasive strategies (lower VAP). HFNO and NIV (CPAP/BiPAP) both reasonable; if intubated use lung-protective ventilation (Vt 6 mL/kg PBW, Pplat <30, driving pressure <15), permissive hypercapnia, prone for refractory hypoxaemia.
Alternatives (sulfa allergy / failure)
Primaquine 30 mg PO daily + clindamycin 600 mg IV Q6H (check G6PD first — haemolysis); pentamidine 4 mg/kg IV daily (nephrotoxic, pancreatic — hyper/hypoglycaemia, QT, infusion hypotension — reserve); atovaquone 750 mg PO BD (mild only); dapsone + TMP (check G6PD).
Treat empirically first, diagnose within 24-72 h
In the hypoxic patient do NOT delay therapy for bronchoscopy — start co-trimoxazole + steroids immediately. BAL yield is preserved for 48-72 h after starting therapy. Send comprehensive BAL panel: PCP immunofluorescence/PCR, CMV/HSV/respiratory viral PCR, bacterial culture, galactomannan, AFB/mycobacterial, Nocardia.
CMV pneumonitis and the other T-cell opportunists
CMV pneumonitis
1-4 months post-transplant
- Peak 1-4 months post-SOT (especially lung — donor-positive/recipient-negative D+/R− highest risk) and post-HSCT; also during rejection treatment (anti-thymocyte globulin, high-dose steroids)
- Bilateral interstitial/ground-glass infiltrates, fever, leucopenia, thrombocytopenia, transaminitis; may coexist with PCP
- Diagnosis: BAL CMV PCR (quantitative) + shell-vial culture + intranuclear inclusions on cytology/biopsy. CMV DNAaemia supports but pneumonia needs BAL. Distinguish asymptomatic shedding (low PCR) from true pneumonitis (high PCR, inclusions)
- Treat: ganciclovir 5 mg/kg IV BD × 14-21 days (reduce dose for renal function); add IVIG in some HSCT-CMV pneumonitis protocols; valganciclovine 900 mg BD PO for step-down. Resistance → foscarnet (nephrotoxic) or cidofovir
- Prophylaxis: valganciclovir 900 mg OD for D+/R− and high-risk; pre-emptive therapy guided by PCR surveillance is an alternative strategy
Nocardia
Aerobic filamentous bacterium
- T-cell defect (transplant, steroids, anti-TNF) + pulmonary nodules/cavitation + CNS lesions = Nocardia until proven otherwise
- CT: nodules (often multiple), cavitation, consolidation, reticulonodular pattern; CUTANEOUS dissemination possible
- CNS DISSEMINATION COMMON (~one-third) — always image the brain (MRI) when Nocardia is found in the lung
- Treatment: high-dose co-trimoxazole (TMP 15 mg/kg/day) ± imipenem or amikacin for severe/disseminated; prolonged 6-12 months. Check species (N. cyriacigeorgica, N. farcinica — the latter more drug-resistant)
Cryptococcus
Encapsulated yeast
- T-cell defect (transplant, HIV, idiopathic CD4 lymphocytopenia); reactivation from inhaled environmental source
- Pulmonary: nodules, consolidation, cavitation, sometimes lymphadenopathy; may be asymptomatic
- CSF involvement (cryptococcal meningitis) MUST be excluded — lumbar puncture with cryptococcal antigen + culture + opening pressure; serum/BAL cryptococcal antigen sensitive
- Treatment (per IDSA 2010): amphotericin B + flucytosine induction, fluconazole consolidation/maintenance. Isolated mild pulmonary disease may respond to fluconazole alone. Manage raised ICP (therapeutic LPs)
Toxoplasma gondii
CNS + lung
- Reactivation in CD4 <100 (HIV, transplant, idiopathic CD4 lymphocytopenia); usually CNS but pneumonitis/disseminated disease occurs
- Ring-enhancing CNS lesions (basal ganglia, corticomedullary junction) on MRI; pulmonary infiltrates with interstitial pattern
- Diagnosis: PCR (blood/CSF/BAL), serology (IgG reflects latent infection — not diagnostic of active disease), brain biopsy if uncertain
- Treatment: pyrimethamine + sulfadiazine + leucovorin (folinic acid) × ≥6 weeks; co-trimoxazole is an alternative; prophylaxis is co-trimoxazole (also covers PCP/Nocardia) — which is why PCP prophylaxis also prevents toxoplasmosis
Diagnostic approach — BAL is the cornerstone
Diagnostic workup of pulmonary infiltrates in the immunocompromised host
Non-invasive first
Blood cultures (×2 sets, including from any central line), serum galactomannan, beta-D-glucan, cryptococcal antigen, CMV/EBV PCR, respiratory virus multiplex PCR (nasopharyngeal ± sputum), serum LDH, 1,3-beta-D-glucan. Urine pneumococcal and Legionella antigen. Consider interferon-gamma release assay / TB screening. Blood cryptococcal antigen and Toxoplasma IgG if CD4 <100.
High-resolution CT chest
Do EARLY (before empiric therapy distorts radiology) and BEFORE bronchoscopy. Pattern recognition: HALO sign → Aspergillus; REVERSE-HALO → Mucorales; ground-glass sparing subpleura → PCP; nodules + cavitation + CNS lesions → Nocardia; peribronchovascular tree-in-bud → atypical/mycobacterial; lobar consolidation → bacterial; miliary → TB/fungal dissemination.
Bronchoscopy with BAL — the key procedure
Send a COMPREHENSIVE panel from the most affected lobe (or wedge several lobes): (1) bacterial culture + Gram stain; (2) respiratory virus multiplex PCR; (3) CMV/HSV/VZV/EBV PCR + shell-vial culture; (4) PCP immunofluorescence/PCR; (5) galactomannan (BAL GM ≥1.0 supportive of IPA); (6) fungal culture + smear; (7) AFB smear/culture + mycobacterial NAAT (Xpert MTB/RIF + line probe for NTM); (8) Nocardia (modified acid-fast, culture on specific media); (9) cytology (malignancy, inclusions, haemosiderin-laden macrophages for DAH). Consider transbronchial biopsy for non-HIV PCP and organising pneumonia.
When to add biopsy
Transbronchial biopsy raises yield for PCP (non-HIV, lower burden), organising pneumonia, malignancy, drug pneumonitis, DAH. Surgical lung biopsy considered when BAL non-diagnostic and the patient can tolerate it — balanced against immunosuppression and mechanical ventilation. Cryobiopsy improves diagnostic yield with less crush artefact.
Do not delay therapy
In the deteriorating immunocompromised patient, start broad empiric therapy while diagnostic workup proceeds — BAL yield is preserved for 48-72 h after starting antibacterials, and mould-active azoles do not abolish galactomannan immediately. De-escalate as data return.
Halo sign
Early invasive aspergillosis
- Solid nodule surrounded by ground-glass halo of haemorrhagic infarction
- Seen in up to 90% of neutropenic IPA within first 5 days
- Resolves as neutrophils recover; evolves to air-crescent
- Differential: angioinvasive Mucorales, organising pneumonia, viral haemorrhagic pneumonia, Wegener granulomatosis, haemorrhagic metastases
Reverse-halo / bird-nest
Mucorales
- Focal round area of ground-glass surrounded by a ring of consolidation
- Strongly associated with pulmonary mucormycosis (vs Aspergillus halo sign)
- May evolve to multiple concave cavities — angioinvasive and rapidly progressive
Ground-glass sparing subpleura
PCP
- Patchy perihilar ground-glass with relative SUBPLEURAL SPARING
- Useful discriminator from pulmonary oedema (perihilar, dependent) and organising pneumonia (peripheral)
- Pneumatoceles → pneumothorax risk in severe disease
Tree-in-bud
Airway-centred
- Small centrilobular nodules with branching — endobronchial spread
- Think: atypical bacteria (Mycoplasma, Chlamydia), mycobacteria (TB/NTM), aspiration, viral bronchiolitis, Nocardia, Aspergillus airway-invasive form
Multiple nodules + CNS lesions
Nocardia/Toxoplasma
- Pulmonary nodules with cavitation + brain abscesses = Nocardia (or Toxoplasma)
- ALWAYS image the brain when Nocardia identified in the lung — CNS involvement changes therapy and duration
Empiric therapy — building a sensible broad cover
Empiric antimicrobial bundle for the undifferentiated immunocompromised pneumonia
Core antibacterial backbone
Anti-pseudomonal beta-lactam: piperacillin-tazobactam 4.5 g IV Q6H (extended infusion), OR cefepime 2 g IV Q8H, OR meropenem 1 g IV Q8H (carbapenem if prior resistant colonisation or severe sepsis). Covers enteric Gram-negatives including Pseudomonas and many ESBL producers.
Add MRSA cover if …
Add vancomycin 15-20 mg/kg IV BD (trough 15-20) OR linezolid 600 mg BD if: known MRSA colonisation, recent healthcare exposure, severe necrotising/cavitating pneumonia, haemodynamic instability, or line infection. Linezolid penetrates lung better than vancomycin and covers MRSA pneumonia well; watch thrombocytopenia and serotonin syndrome (prolonged use).
Add atypical cover
Azithromycin 500 mg OD OR a respiratory fluoroquinolone (moxifloxacin 400 mg OD) — covers Legionella, Mycoplasma, Chlamydia, and many atypicals that behave aggressively in immunosuppression.
Add PCP cover if T-cell defect
Co-trimoxazole high-dose (TMP 15-20 mg/kg/day) if the infiltrate is consistent with PCP (bilateral ground-glass) and the host is at risk — this also covers Nocardia and Toxoplasma. If only "covering the possibility," prophylaxis-dose co-trimoxazole is inadequate; use treatment dose if PCP is genuinely suspected.
Add antifungal if neutropenic / steroid-heavy / halo on CT
Empiric mould-active azole: voriconazole (load 6 mg/kg BD ×2 then 4 mg/kg BD) or isavuconazole (load 200 mg BD ×6 then 200 mg OD). Choose isavuconazole if Mucorales is on the differential or if voriconazole interactions (CNI) are problematic. Alternatively, caspofungin as a "less toxic" empiric choice if Candida is the main concern. Liposomal amphotericin B if prior mould prophylaxis breakthrough.
Add antiviral if CMV possible
Ganciclovir 5 mg/kg IV BD if CMV pneumonitis is plausible (D+/R−, 1-4 months post-transplant, high PCR) pending BAL CMV PCR results. Also send respiratory virus PCR and treat influenza/RSV/COVID-19 with oseltamivir/antivirals per protocol.
De-escalate within 48-72 h
As BAL/CT/data return, narrow to the pathogen(s) identified. The cost of prolonged broad cover is resistance, C. difficile, and drug toxicity; the cost of inadequate cover is mortality. Reassess daily with the microbiology and infectious diseases teams.
Adjunctive and source-control measures
Adjunctive therapy bundle
Reduce immunosuppression
The single most influential intervention. Taper steroids as fast as the underlying disease allows; reduce calcineurin inhibitor target levels with the transplant team; manage GVHD with the haematology team. Balance against graft rejection / GVHD flare — individualised, multidisciplinary.
G-CSF / GM-CSF for neutropenia
G-CSF (filgrastim) 5 microg/kg/day shortens neutropenia in chemotherapy-induced neutropenia and is recommended for high-risk febrile neutropenia. GM-CSF (sargramostim) is sometimes preferred for fungal infection (augments macrophage/monocyte function) and post-HSCT engraftment. Not universally used — follow local protocol and malignancy-specific guidelines (ASCO/IDSA).
IVIG for humoral deficiency
Replacement IVIG (400-600 mg/kg every 3-4 weeks) for hypogammaglobulinaemia (myeloma, CLL, post-rituximab, post-HSCT with chronic GVHD) with recurrent sinopulmonary infection. Specific (hyperimmune) IVIG added in some CMV/RSV protocols. Check baseline IgG; avoid volume overload.
Source control
Remove infected central venous catheters (catheter-related bloodstream infection), drain empyema/abscess, debride mucormycosis surgically (where feasible), resect localised cavitating Aspergillus with haemoptysis risk. Surgical debridement is part of cure in mucormycosis — antifungals alone are often insufficient.
Vaccinate during convalescence
Once stable, ensure the immunocompromised patient is on the correct vaccination schedule (pneumococcal conjugate + polysaccharide, Hib, meningococcal ACWY + B, influenza annually, COVID-19, recombinant zoster, HBV). Avoid LIVE vaccines (MMR, varicella, yellow fever, BCG, oral polio, intranasal influenza) while immunosuppressed. Post-HSCT re-vaccination follows a staged schedule.
ICU supportive bundle
Conservative/restrictive fluid strategy (the immunocompromised lung is ARDS-pattern and oedema-sensitive), VTE prophylaxis (LMWH — these patients are pro-thrombotic), stress-ulcer prophylaxis if intubated/coagulopathic, glycaemic control (steroids), early enteral nutrition, and careful attention to drug-drug interactions (azole ± CNI ± antiplatelet ± acid suppression ± chemotherapy).
Respiratory support in the immunocompromised patient
HFNO
First-line bridge
- High-flow nasal cannula delivers up to 60 L/min with controlled FiO₂, low-level PEEP (~3-5 cmH₂O), washout of dead space, and humidification — comfortable and tolerated
- Useful bridge or definitive support in moderate hypoxaemic respiratory failure; lower intubation risk than standard oxygen in immunocompromised (Florali / Lemiale 2020)
- Monitors: watch for rising respiratory rate, falling SpO₂, thoracoabdominal asynchrony — escalate early; do not persist if clearly failing
NIV (CPAP/BiPAP)
Avoids intubation/VAP
- Non-invasive ventilation reduces intubation and mortality vs standard oxygen in immunocompromised hypoxaemic respiratory failure (classic 2001 Hilbert RCT)
- Especially valuable when the cause is rapidly reversible (PCP, pulmonary oedema, atelectasis) and VAP would be devastating
- Caution in profound hypoxaemia, copious secretions, encephalopathy, or facial injury — risks include delayed intubation and aspiration
- HFNO vs NIV: Florali (Lemiale 2020) found no clear superiority of HFNO over standard oxygen as primary; NIV remains valuable. Escalation pathway: HFNO → NIV → intubation
Invasive ventilation
Last resort
- When HFNO/NIV fail (rising RR, falling SpO₂, exhaustion, rising CO₂, encephalopathy) — intubate early rather than late
- Lung-protective: Vt 6 mL/kg PBW, Pplat <30, driving pressure <15; permissive hypercapnia; prone positioning for refractory hypoxaemia; consider ECMO in severe refractory ARDS
- Beware PEEP and pneumothorax in PCP cystic disease; suction/physiotherapy for atelectasis; minimise sedation to allow early mobilisation
ECMO
Refractory rescue
- Veno-venous ECMO for refractory severe ARDS despite lung-protective/prone ventilation — reasonable in immunocompromised patients with potentially reversible disease (PCP, viral pneumonia) and acceptable long-term prognosis
- Bleeding risk amplified by thrombocytopenia, coagulopathy, and antifungal-induced platelet dysfunction; case-by-case decision with multidisciplinary team
Oxygenation strategy in immunocompromised ARF — the Florali family (Lemiale, CCM 2020)
Randomised multicentre trial and ancillary analyses of oxygenation strategies in immunocompromised ICU patients
Population: Critically ill immunocompromised patients (haematological malignancy, solid tumour, transplant, immunosuppressive drugs) with acute respiratory failure
Key finding
HFNO did not significantly reduce day-28 mortality vs standard oxygen, but subgroup analyses informed escalation strategy: NIV remains valuable, and a structured HFNO → NIV → intubation pathway is safe. Intubation remains necessary in ~40% of immunocompromised ARF.
Practice change
In immunocompromised respiratory failure, use a staged non-invasive-first strategy (HFNO and/or NIV) with a LOW threshold to intubate if failing — early appropriate antibiotics and lung-protective ventilation if intubated drive outcome.
Non-infectious pulmonary infiltrates — do not be fooled
Up to a third of pulmonary infiltrates in the immunocompromised are NON-infectious. BAL helps differentiate.[2]
Drug-induced pneumonitis
Iatrogenic
- Methotrexate, bleomycin (dose-dependent, oxygen worsens — avoid high FiO₂), busulfan, cyclophosphamide, amiodarone (phospholipidosis), nitrofurantoin, checkpoint inhibitors (pneumonitis — corticosteroid-responsive)
- Pattern: NSIP, OP, hypersensitivity, or diffuse alveolar damage; BAL lymphocytic with eosinophilia sometimes
- Stop the offending drug; corticosteroids for severe/checkpoint-inhibitor pneumonitis
Radiation pneumonitis
Post-RT / recall
- Within RT field (or recall with subsequent drugs e.g. checkpoint inhibitors); ground-glass/consolidation confined to the irradiated area
- Corticosteroid responsive; distinguish from infection (which can coexist)
Graft-vs-host disease (GVHD)
Allo-HSCT
- Pulmonary GVHD is controversial but organised pneumonia and bronchiolitis obliterans are recognised late complications of chronic GVHD
- Bronchiolitis obliterans: irreversible obstructive pattern, mosaic attenuation on CT; treat with immunomodulation and supportive care
Diffuse alveolar haemorrhage (DAH)
HSCT / vasculitis
- Post-HSCT (around engraftment), vasculitis (ANCA, anti-GBM), lupus, severe thrombocytopenia; haemoptysis may be ABSENT
- BAL: progressively bloodier return across sequential aliquots; cytology shows haemosiderin-laden macrophages
- Treat the cause; high-dose steroids for inflammatory DAH; correct coagulopathy and thrombocytopenia
Engraftment syndrome / IRIS
Post-HSCT / post-ART
- Capillary leak, fever, pulmonary infiltrates around neutrophil engraftment (auto-HSCT, post-CAR-T); IRIS after starting ART or reducing immunosuppression
- Corticosteroid responsive; rule out infection first
Malignancy / PTLD
EBV-driven
- Pulmonary lymphoma, leukaemic infiltration, post-transplant lymphoproliferative disorder (EBV-driven, especially in heavy immunosuppression)
- Persistent infiltrates not responding to antimicrobials; LDH very high; biopsy for histology and EBV-ISH
- Reduce immunosuppression, rituximab ± chemo; EBV DNA surveillance guides early intervention
Splenectomised / asplenic — OPSI is an emergency
[3]Prophylaxis — preventing the predictable
PCP
Co-trimoxazole
- Universal for solid-organ transplant 6-12 months (lifelong lung/heart-lung), allo-HSCT until ≥6 months post-engraftment (longer with GVHD), steroids ≥20 mg/day ≥4 weeks, anti-TNF
- Co-trimoxazole 1 SS (800/160) daily or 1 DS 3×/week. Alternatives: dapsone (check G6PD), atovaquone, aerosolised pentamidine (upper-lobe breakthrough)
- BONUS: also covers Nocardia, Toxoplasma, many pneumocystis-resistant organisms — first-line for multi-pathogen prophylaxis
CMV
Valganciclovir / pre-emptive
- D+/R− mismatch highest risk; choose prophylaxis (valganciclovir 900 mg OD × 3-6 months) OR pre-emptive therapy (weekly PCR surveillance, treat at threshold)
- Lung transplant highest risk of CMV pneumonitis; many centres prophylax longer
- Toxicity: marrow suppression, renal impairment; interacts with azoles and mycophenolate
Mould (Aspergillus/Mucor)
Posaconazole/isavuconazole
- Posaconazole prophylaxis in AML/MDS induction, allo-HSCT with GVHD, prolonged neutropenia (Cornely NEJM 2007 — reduced mould infection and improved survival)
- Some lung/liver transplant centres use universal prophylactic mould cover early
- Breakthrough on posaconazole → suspect Mucorales (resistant) or non-fumigatus Aspergillus or insufficient levels (TDM)
Encapsulated bacteria
Vaccines ± penicillin
- Asplenia/functional hyposplenism: pneumococcal (conjugate + polysaccharide), Hib, meningococcal ACWY + B; lifelong penicillin V in high-risk
- Post-HSCT re-vaccination schedule begins ~6 months post-transplant (earlier with Flu)
Viral
Antivirals
- Aciclovir/valaciclovir for HSV/VZV prophylaxis post-HSCT/SOT early period
- Influenza/COVID-19/RSV vaccination annually (inactivated only while immunosuppressed); palivizumab/nirsevimab for RSV in select paediatric/HSCT groups
Additional high-yield clinical pearls
Red flags — the must-not-miss list
Exam practice — viva-style questions
[3]Summary answer (for the oral exam)
"Pneumonia in the non-HIV immunocompromised patient carries a far broader pathogen spectrum and a 20-50% mortality, and the key to the differential is to map the specific immune defect to the class of pathogen it fails to control — neutropenia opens the door to Gram-negatives, Candida and the invasive moulds Aspergillus and Mucorales; a T-cell defect from transplant, high-dose steroids or anti-TNF biologics brings Pneumocystis, CMV, Nocardia, Cryptococcus and Toxoplasma; a humoral defect from myeloma, CLL or rituximab invites the encapsulated bacteria; and asplenia risks overwhelming post-splenectomy infection with pneumococcus, Hib and meningococcus. Timing further refines the differential: in the first month after transplant nosocomial and donor-derived organisms dominate, from one to six months the opportunistic window opens, and after six months community-acquired organisms re-emerge alongside late opportunists. I would obtain blood cultures, an early CT chest, and a comprehensive bronchoalveolar lavage panel covering bacterial, viral — including CMV, HSV and respiratory viruses — fungal with galactomannan and beta-D-glucan, mycobacterial and Nocardia testing, while starting broad empiric therapy with an anti-pseudomonal beta-lactam such as piperacillin-tazobactam, vancomycin or linezolid if MRSA is plausible, an atypical cover agent, and then layering in co-trimoxazole for PCP if a T-cell defect is present, a mould-active azole such as voriconazole or isavuconazole if neutropenic or if there is a halo sign, and ganciclovir if CMV is plausible. For invasive aspergillosis voriconazole is first-line with therapeutic drug monitoring, isavuconazole is a well-tolerated alternative that also covers Mucorales, and any breakthrough on voriconazole prompts me to switch to liposomal amphotericin B and consider surgery. For PCP I would give high-dose co-trimoxazole for twenty-one days and add corticosteroids whenever the PaO₂ is under seventy millimetres of mercury. Throughout, I would reduce immunosuppression with the transplant or oncology team, use G-CSF for neutropenia and IVIG for humoral deficiency, prefer non-invasive respiratory support to avoid ventilator-associated pneumonia but intubate early with lung-protective settings if failing, employ a conservative fluid strategy, and remember that up to a third of infiltrates are non-infectious — drug pneumonitis, radiation, graft-versus-host disease, diffuse alveolar haemorrhage, post-transplant lymphoproliferative disorder and immune reconstitution syndromes — all of which bronchoscopy and biopsy help to distinguish."[3]
References
- [1]Niederman MS, Torres A. Severe community-acquired pneumonia. European Respiratory Review, 2022.PMID 36517046
- [2]García-Martínez A, Woc-Colburn L Immunocompromised host pneumonia: a shifting landscape of risk. Current opinion in pulmonary medicine, 2026.PMID 41783951
- [3]Herbrecht R, Denning DW, Patterson TF, et al. Voriconazole versus amphotericin B for primary therapy of invasive aspergillosis. New England Journal of Medicine, 2002.PMID 12167683
- [4]Patterson TF, Thompson GR 3rd, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 2016.PMID 27365388
- [5]Cornely OA, Maertens J, Winston DJ, et al. Posaconazole vs. fluconazole or itraconazole prophylaxis in patients with neutropenia. New England Journal of Medicine, 2007.PMID 17251531
- [6]Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 2011.PMID 21258094
- [7]Ullmann AJ, Aguado JM, Arikan-Akdagli S, et al. Diagnosis and management of Aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clinical Microbiology and Infection, 2018.PMID 29544767
- [8]De Pauw B, Walsh TJ, Donnelly JP, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clinical Infectious Diseases, 2008.PMID 18462102
- [9]Lemiale V, Mokart D, Mayaux J, et al. Oxygenation Strategy During Acute Respiratory Failure in Critically-Ill Immunocompromised Patients: The randomized controlled Florali study. Critical Care Medicine, 2020.PMID 32706556
- [10]Perfect JR, Dismukes WE, Dromer F, et al. Clinical practice guidelines for the management of cryptococcal disease: 2010 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 2010.PMID 20047480
- [11]Ruhnke M, Behre G, Buchheidt D, et al. Diagnosis of invasive fungal diseases in haematology and oncology: 2018 update of the recommendations of the infectious diseases working party of the German society for haematology and medical oncology (AGIHO). Mycoses, 2018.PMID 30098069