ICU · Infectious Diseases
Acute severe community-acquired pneumonia: post-influenza bacterial pneumonia
Also known as Post-influenza pneumonia · Bacterial superinfection · Staphylococcal pneumonia post-influenza
Post-influenza bacterial pneumonia is a devastating complication — influenza virus damages respiratory epithelium → secondary bacterial invasion. Most common organisms: Staphylococcus aureus (1, including MRSA and PVL-positive strains — causes necrotising pneumonia with high mortality), Streptococcus pneumoniae (2), Haemophilus influenzae. Presents as: initial viral illness (fever, myalgia, cough) → transient improvement → sudden deterioration (high fever, dyspnoea, septic shock, multilobar infiltrates, cavitation). Diagnosis: influenza PCR + sputum/blood cultures + urinary antigens. Treatment: antiviral (oseltamivir) + broad-spectrum antibiotics (cover MRSA — add vancomycin/linezolid) + supportive ICU care. Mortality: 20-40%.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Clinical features
Post-influenza pneumonia presentation
Phase 1: Viral influenza (days 1-5)
Fever, myalgia, headache, dry cough, sore throat, coryza. Typical influenza. May be improving or at peak.
Phase 2: Transient improvement (days 3-7)
Fever resolves or partially improves. Patient feels better. BUT: bacteria are colonising damaged epithelium.
Phase 3: Sudden deterioration (days 5-10)
Recurrent high fever, worsening dyspnoea, productive cough (purulent or bloody sputum), septic shock, rapid progression on CXR (multilobar infiltrates, cavitation — especially with S. aureus). This is the bacterial superinfection phase — MEDICAL EMERGENCY.
Pathophysiology
Mechanistic cascade — how influenza primes for bacterial superinfection
1. Direct epithelial destruction
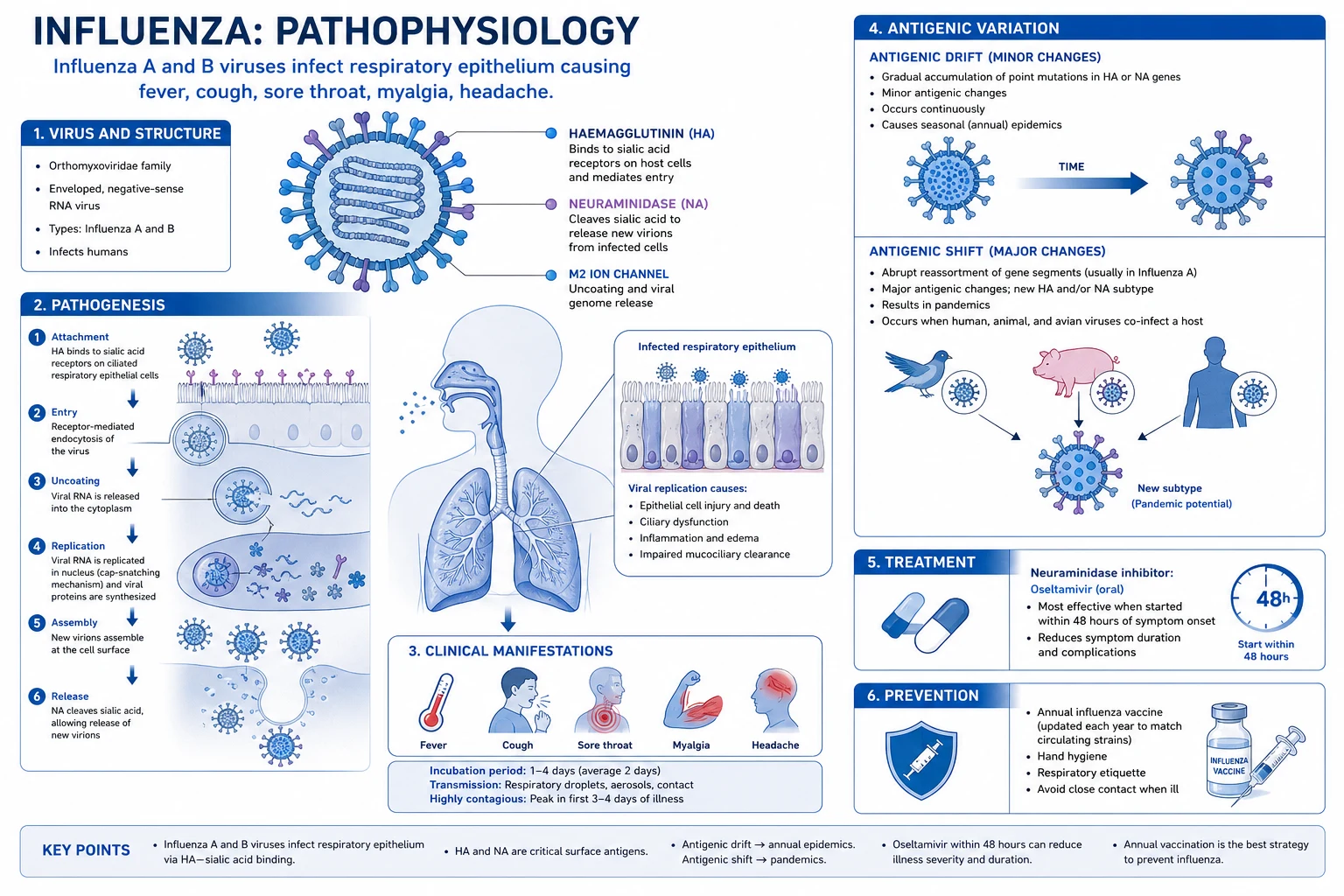
Influenza infects ciliated columnar epithelial cells via α2,6-linked sialic acid receptors (tracheobronchial tree in humans). Viral replication causes cell lysis and sloughing → denuded basement membrane. Desquamation exposes extracellular matrix proteins (fibronectin, laminin) — to which S. aureus and S. pneumoniae bind via surface adhesins (e.g. Panton-Valentine leukocidin, pneumococcal surface proteins). Loss of the physical barrier is the first permissive event.<Cite id="3" /><Cite id="6" />
2. Mucociliary paralysis
Influenza reduces ciliary beat frequency and disrupts the mucus blanket. Damaged cilia cannot sweep bacteria upward. S. aureus and pneumococci trapped in the airway are not cleared — they multiply at the epithelial surface. Even a single virally-injured region can seed contiguous lung segments.<Cite id="4" />
3. Alveolar macrophage and neutrophil dysfunction
Influenza-infected alveolar macrophages show impaired phagocytosis of opsonised bacteria and suppressed respiratory burst. Neutrophil recruitment is delayed, and recruited neutrophils are functionally exhausted (reduced oxidative killing). IFN-γ from the antiviral Th1 response paradoxically down-regulates scavenger receptor MARCO on macrophages — reducing pneumococcal uptake. The innate immune cell that should kill bacteria is now dysfunctional.<Cite id="5" /><Cite id="9" />
4. Viral neuraminidase unmasks bacterial receptors
Influenza neuraminidase cleaves sialic acid residues on the host cell surface — exposing cryptic receptors that pneumococci and S. aureus exploit for adhesion. This is the molecular basis for the synergy: a viral enzyme directly enhances bacterial colonisation. It is also the reason neuraminidase inhibitors (oseltamivir) may reduce secondary bacterial infection.<Cite id="4" />
5. Immune dysregulation — type I IFN and IL-10
The antiviral type I/II interferon response drives a Th1 cytokine milieu that, while antiviral, suppresses antibacterial Th17-mediated neutrophil recruitment in the lung. IL-10 produced during the convalescent phase further dampens macrophage function. The result: a transient post-viral "immune paralysis" window during which bacteria gain a foothold — the mechanistic correlate of the clinical biphasic course.<Cite id="5" /><Cite id="9" />
6. Tissue destruction and toxin-mediated necrosis
Once S. aureus (especially PVL-positive) establishes infection, it secretes PVL, α-haemolysin and other cytotoxins that destroy neutrophils and alveolar cells → haemorrhagic, necrotising pneumonia with cavitation and pneumatocele formation. Pneumolysin from S. pneumoniae produces similar direct cytotoxicity. The histological picture is haemorrhagic necrotising bronchopneumonia.<Cite id="4" />
Common organisms
[4] [1] [4]PVL-positive S. aureus post-influenza — the lethal phenotype
Observational / case series of necrotising pneumonia in young healthy adults
Population: Previously well adolescents and young adults with influenza-like illness → rapid respiratory failure
Key finding
Mortality 30-50%; characteristic findings: multilobar infiltrates, cavitation, pneumatoceles, haemoptysis, leucopenia/leucocytosis, high fever, septic shock. PVL toxin (a bicomponent pore-forming cytotoxin) lyses neutrophils, releasing proteases that worsen tissue destruction.
Diagnosis
Diagnostic workup — what to send, what it tells you
Viral diagnosis (confirm influenza)
Nasopharyngeal swab (or BAL/tracheal aspirate if intubated) for influenza **PCR / multiplex respiratory viral panel** — detects influenza A and B, subtypes H1, H3, H1N1pdm09. Send EARLY (within first few days of illness) — sensitivity falls as viral shedding declines. Rapid antigen tests have lower sensitivity (~50-70%) — a negative rapid test does NOT exclude influenza in a sick patient; send PCR. During peak influenza season, a compatible syndrome with positive household contacts supports empiric treatment even before PCR result.<Cite id="7" /><Cite id="8" />
Bacterial diagnosis (identify the superinfecting organism)
**Sputum Gram stain and culture** (good-quality sample, <10 epithelial cells/low-power field) — look for Gram-positive cocci in clusters (S. aureus) or pairs/diplococci (pneumococcus). **Blood cultures** (two sets) BEFORE antibiotics — bacteraemia occurs in 20-30% of S. aureus cases and is an independent mortality risk factor. **Lower respiratory samples** (BAL/protected specimen brush) if intubated — higher yield, less contamination. **Urinary antigens**: pneumococcal and Legionella — rapid but pneumococcal antigen misses many cases.<Cite id="1" /><Cite id="2" />
Biomarkers — procalcitonin (PCT)
Procalcitonin helps **distinguish bacterial superinfection from pure viral illness** and guides antibiotic duration. Pure influenza typically produces low/normal PCT; a rising PCT in a deteriorating patient strongly suggests bacterial superinfection. However — influenza itself can transiently elevate PCT, so interpret trends, not single values. PCT-guided algorithms (e.g. stop antibiotics when PCT falls >80% from peak or <0.5 ng/mL) shorten antibiotic duration safely. **CRP and WBC** are nonspecific but trend with infection; leucopenia in S. aureus necrotising pneumonia is an ominous sign.<Cite id="4" />
Imaging
**Chest X-ray**: multilobar infiltrates, often patchy. Look for cavitation, pneumatoceles (thin-walled cysts), pleural effusion, pneumothorax. **High-resolution CT**: defines extent, reveals cavitation and empyema earlier than CXR, identifies pneumatoceles. **Point-of-care ultrasound**: B-lines, consolidation with air-bronchograms, pleural effusion — useful at bedside. Radiographic deterioration often outpaces clinical deterioration in S. aureus necrotising pneumonia — repeat imaging.<Cite id="1" />
Special tests once S. aureus isolated
**Methicillin susceptibility** (MRSA vs MSSA) — determines vancomycin/linezolid necessity. **PVL gene testing** (PCR for lukS-PV/lukF-PV) — identifies the necrotising phenotype. **Echocardiography** (transthoracic, transoesophageal if bacteraemic) — exclude endocarditis and metastatic foci. **Repeat blood cultures** at 48-72h — persistent bacteraemia suggests endocarditis, deep abscess, or inadequate source control (e.g. empyema).<Cite id="1" />
Severity scoring and resuscitation status
Calculate **CURB-65 or SMART-COP** (latter preferred for ICU triage). Assess **qSOFA/SOFA**, lactate (marker of hypoperfusion and mortality), organ failure pattern. Identify early who needs ICU (mechanical ventilation, vasopressors) vs ward. Post-influenza S. aureus with septic shock or ARDS demands ICU from the outset.<Cite id="1" />
Management
[2]Post-influenza pneumonia management
Antiviral therapy
Oseltamivir 75 mg PO BD for 5 days (or longer if immunocompromised). Start IMMEDIATELY if influenza suspected/confirmed (even if >48h from onset — may still benefit). Mechanism: neuraminidase inhibitor — prevents viral release from infected cells. Reduces: viral shedding, duration of symptoms, risk of complications. Especially important in: severe/complicated influenza, immunocompromised, pregnant, ICU patients.
Broad-spectrum antibiotics with MRSA cover
Ceftriaxone 2g IV + azithromycin 500 mg IV (cover S. pneumoniae, H. influenzae, atypicals) PLUS vancomycin (25-30 mg/kg loading) OR linezolid 600 mg BD (cover MRSA — S. aureus is #1 cause of post-influenza pneumonia). Linezolid preferred for pneumonia (better lung penetration, covers PVL-positive strains). Continue MRSA cover until cultures negative (48-72h) if MRSA risk factors absent.
Source identification
Influenza PCR (nasopharyngeal swab — type A/B, subtyping). Sputum culture + blood cultures (bacteraemia common with S. aureus — 20-30%). Urinary antigens (pneumococcal, Legionella — rule out other causes). PVL testing if S. aureus isolated (PVL-positive = necrotising pneumonia, higher mortality). CXR/CT: look for cavitation (S. aureus), multilobar involvement, pleural effusion.
Supportive ICU care
Mechanical ventilation (lung-protective — often severe ARDS-like physiology). Vasopressors (septic shock common). Fluids (cautious — capillary leak). Consider corticosteroids (controversial — some benefit in severe influenza pneumonia). Monitor for: ARDS, metastatic infection (S. aureus — endocarditis, osteomyelitis, septic emboli), empyema, pneumatocele (S. aureus).
Empiric antibiotic strategy — covering MRSA and the typical CAP pathogens
Initial empiric regimen (severe post-influenza CAP, ICU)
**Vancomycin** 25-30 mg/kg IV loading then 15-20 mg/kg q8-12h (target trough 15-20 mg/L or AUC/MIC 400-600) **OR linezolid** 600 mg IV/PO BD. PLUS a beta-lactam covering pneumococcus and H. influenzae: **ceftriaxone** 2g IV daily **OR cefotaxime** 2g IV TDS **OR (if penicillin-allergic/anaphylaxis) moxifloxacin** 400 mg IV daily. PLUS atypical cover: **azithromycin** 500 mg daily **OR a respiratory fluoroquinolone** (covers atypicals — moxifloxacin/levofloxacin do both). The minimum in suspected post-influenza S. aureus pneumonia: vancomycin/linezolid + ceftriaxone + (azithromycin or moxifloxacin).<Cite id="1" /><Cite id="8" />
Why linezolid over vancomycin in necrotising S. aureus pneumonia
Linezolid: superior lung epithelial lining fluid penetration (~5x vancomycin); orally bioavailable; **suppresses toxin (including PVL, α-haemolysin) production** by inhibiting ribosomal 70S initiation — relevant in PVL-mediated necrotising pneumonia. Downsides: thrombocytopenia (especially >14 days), serotonin syndrome with serotonergic drugs/MAOIs, peripheral/optic neuropathy with prolonged use, lactic acidosis. Vancomycin: nephrotoxic (worse with concurrent piperacillin-tazobactam), slower bacterial killing, requires level monitoring. IDSA: either acceptable; linezolid often preferred in severe necrotising disease.<Cite id="1" />
Antiviral — oseltamivir
**Oseltamivir 75 mg PO BD for 5 days** (longer if immunocompromised or critically ill with ongoing viral replication — up to 10 days). For critically ill or malabsorbing: **enteric oseltamivir via NG** (absorbed even in ICU patients). In renal failure: reduce to 75 mg OD if CrCl 30-60, 30 mg OD if CrCl 10-30. Influenza A/H1N1pdm09 universally sensitive to oseltamivir; adamantanes (amantadine) NOT recommended (high resistance). **Baloxavir** (cap-dependent endonuclease inhibitor — single dose) is an alternative in some settings. Start **immediately — do not wait for PCR** in suspected severe influenza.<Cite id="7" /><Cite id="8" />
De-escalation
Once organism + susceptibility known (typically 48-72h): (1) MRSA excluded → **stop** vancomycin/linezolid; continue ceftriaxone +/- azithromycin. (2) MSSA confirmed → **switch** vancomycin/linezolid to flucloxacillin/nafcillin/cefazolin (beta-lactams are bactericidal and superior for MSSA). (3) MRSA confirmed → continue vancomycin OR linezolid. (4) Influenza PCR negative AND community exposure pattern excludes flu → consider stopping oseltamivir. **Continue empiric cover** until cultures definitive — do not narrow prematurely in deteriorating patients.<Cite id="1" />
Duration of therapy
S. aureus pneumonia: minimum **7 days** for uncomplicated MSSA, **14-21 days** for MRSA, bacteraemic, necrotising, or complicated by metastatic infection/empyema/endocarditis. S. pneumoniae: 7-10 days. H. influenzae: 7 days. **Prolonged bacteraemia** (>2-3 days on appropriate therapy) mandates search for endocarditis, septic thrombophlebitis, deep abscess, or osteomyelitis. Use **procalcitonin-guided stopping** if uncomplicated.<Cite id="1" />
Adjunctive therapy and supportive care
**Lung-protective ventilation** (Vt 6 mL/kg PBW, plateau <30 cmH2O) — ARDS-pattern physiology common. **Vasopressors** for septic shock — noradrenaline first-line, add vasopressin, consider hydrocortisone 200 mg/day for refractory shock. **Conservative fluid strategy** (capillary leak worsens pulmonary oedema). **Corticosteroids**: controversial — dexamethasone/methylprednisolone may reduce mortality in severe influenza pneumonia (some observational data) but routine use NOT recommended and may increase secondary infection. **IVIG**: considered in PVL-mediated toxin effect (neutralises toxin) — unproven. **Source control**: drain empyema, decompress pneumatoceles if expanding/infected.<Cite id="1" /><Cite id="4" />
Mortality and prognosis
[3] [1] [4]Complications
[1] [4]Prevention
Preventing post-influenza pneumonia
Influenza vaccination
Most effective prevention. **Annual inactivated influenza vaccine** for everyone >6 months, with priority for: >65 years, pregnant women, chronic medical conditions, immunocompromised, healthcare workers, ICU/aged-care staff. Vaccination reduces: influenza infection, severity, hospitalisation, and post-influenza bacterial pneumonia. Herd immunity in healthcare workers protects vulnerable patients.<Cite id="7" />
Pneumococcal vaccination
**Pneumococcal conjugate vaccine (PCV13/15/20)** + **polysaccharide vaccine (PPSV23)** per age/risk schedules. Reduces invasive pneumococcal disease including post-influenza pneumococcal pneumonia. Recommended for >65, chronic disease, asplenia, immunocompromise.<Cite id="3" />
Antiviral prophylaxis and early treatment
**Oseltamivir 75 mg OD** for post-exposure prophylaxis in high-risk household contacts during influenza season. **Early oseltamivir** (within 48h of symptom onset) for symptomatic high-risk patients reduces complication risk. In ICU patients, treat regardless of onset duration.<Cite id="8" />
Infection control
**Droplet precautions** for suspected/confirmed influenza. Hand hygiene, masking, isolation. Healthcare worker vaccination + masking during peak influenza reduces nosocomial spread to vulnerable ICU patients.<Cite id="7" />
Special populations
Special situations and modifications
Pregnancy
Pregnant women have 4-7x risk of severe influenza. **Oseltamivir is safe in all trimesters** and should not be withheld. Prefer beta-lactams (ceftriaxone) and vancomycin/linezolid (both safe). Avoid moxifloxacin if possible (animal arthropathy concerns, though human data reassuring). Vaccinate in pregnancy — protects mother and infant (transplacental antibody) for first 6 months of life.<Cite id="8" />
Immunocompromised (transplant, neutropenic, HIV)
Broader empiric cover: add **Pseudomonas cover** (piperacillin-tazobactam or meropenem + anti-Pseudomonal beta-lactam) and consider **antifungal cover** if prolonged neutropenia or steroid use. Prolonged viral shedding — extend oseltamivir. Send BAL for respiratory panel including Pneumocystis, CMV, Aspergillus galactomannan. High-dose corticosteroid therapy blunts fever and inflammation — maintain high suspicion.<Cite id="4" />
Elderly and aged-care residents
Atypical presentation — may have minimal fever, confusion, falls. High mortality. Aggressive empiric therapy warranted. Vaccination is critical; considerate aged-care outbreak management (cohorting, antiviral prophylaxis of contacts).<Cite id="7" />
Severe influenza with ARDS
Lung-protective ventilation; prone positioning; **venovenous ECMO** for refractory hypoxaemia (PaO2/FiO2 <80 despite optimisation). EOLIA-era criteria. Influenza-associated ARDS has similar outcomes to other viral ARDS. Conservative fluid strategy reduces ventilator days.<Cite id="1" />
Comparison with other severe pneumonias
[1] [3]SAQ — post-influenza bacterial pneumonia
SAQ — Post-influenza necrotising Staphylococcal pneumonia
10 minutes · 10 marks
A 31-year-old previously well woman presents in mid-winter with a 7-day history of influenza-like illness (fever, myalgia, dry cough) that had begun to improve, followed by abrupt deterioration: high fever, pleuritic chest pain, copious blood-streaked sputum and progressive dyspnoea. On arrival she is septic (MAP 58, HR 142, RR 36, SpO2 88% on 15 L via non-rebreather), and CXR shows multilobar consolidation with early cavitation. Influenza A PCR is positive.
SAQ — PVL-positive community-acquired MRSA pneumonia
10 minutes · 10 marks
A 19-year-old man with a recent history of recurrent boils presents with rapidly progressive respiratory failure, high fever, haemoptysis and septic shock 3 days after a flu-like illness. CXR shows multilobar patchy consolidation with multiple areas of cavitation. Nasal MRSA swab is positive. Blood cultures grow S. aureus sensitive to clindamycin and vancomycin.
Clinical pearls
Pitfalls
Red flags
References
- [1]Martin-Loeches I, Torres A. Severe community-acquired pneumonia. Intensive care medicine, 2022.PMID 36517046
- [2]Martin-Loeches I, van Someren Gréve F, Schultz MJ Bacterial pneumonia as an influenza complication. Current opinion in infectious diseases, 2017.PMID 27984245
- [3]Morens DM, Taubenberger JK, Fauci AS Predominant role of bacterial pneumonia as a cause of death in pandemic influenza: implications for pandemic influenza preparedness. The Journal of infectious diseases, 2008.PMID 18710327
- [4]Rynda-Apple A, Robinson KM, Alcorn JF Influenza and Bacterial Superinfection: Illuminating the Immunologic Mechanisms of Disease. Infection and immunity, 2015.PMID 26216421
- [5]Sun K, Metzger DW Inhibition of pulmonary antibacterial defense by interferon-gamma during recovery from influenza infection. Nature medicine, 2008.PMID 18438414
- [6]Uyeki TM, Hui DS, Zambon M, et al. Influenza. Lancet (London, England), 2022.PMID 36030813
- [7]Uyeki TM Influenza. Annals of internal medicine, 2021.PMID 34748378
- [8]Harper SA, Bradley JS, Englund JA, et al. Seasonal influenza in adults and children--diagnosis, treatment, chemoprophylaxis, and institutional outbreak management: clinical practice guidelines of the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America, 2009.PMID 19281331
- [9]Engler RJM, Nelson MR Host immune responses to influenza infection and vaccines: Lessons learned for all viral pandemic challenges. Annals of allergy, asthma & immunology : official publication of the American College of Allergy, Asthma, & Immunology, 2020.PMID 32564928