ICU · Infectious Diseases
Sepsis in the immunocompromised host
Also known as Immunocompromised sepsis · Febrile neutropenia sepsis · Sepsis in cancer/transplant patients
Immunocompromised patients with sepsis have different pathogens, atypical presentations, and higher mortality than immunocompetent patients. Categories: neutropenic (chemotherapy — see neutropenic sepsis topic), cellular (HIV, transplant — T-cell defects), humoral (multiple myeloma, CLL — B-cell defects), splenectomised (encapsulated organisms), corticosteroid-treated. Atypical presentations: may lack fever (blunted inflammatory response), may have subtle signs. Broader empiric antibiotic coverage needed. Consider: opportunistic infections (PCP, CMV, fungal, mycobacterial, viral). Principles: (1) early broad-spectrum antibiotics (within 1 hour), (2) aggressive resuscitation, (3) identify and treat opportunistic pathogens, (4) consult infectious diseases/immunology.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags


Overview — why the immunocompromised host breaks the rules
Sepsis in the immunocompromised patient is not standard sepsis with a few extra bugs bolted on. The blunted inflammatory response obscures the diagnosis, the specific immune defect dictates a predictable but far broader pathogen spectrum, opportunist infections (PCP, CMV, moulds, mycobacteria, Strongyloides) must be anticipated and treated with targeted therapy, the host has less physiological reserve, and mortality is several-fold higher. The two non-negotiable SSC principles are unchanged — antibiotics within one hour and aggressive resuscitation — but the choice of antibiotics is broadened and layered according to the immune defect, and the work-up must include the opportunistic panel (viruses, mould biomarkers, parasites) from the first hour.[1][2]
Immunocompetent vs immunocompromised sepsis — what changes
| Feature | Immunocompetent host | Immunocompromised host |
|---|---|---|
| Fever response | Reliable sign | Often absent or blunted (neutropenia, steroids, uraemia, age) — afebrile sepsis is common |
| Typical pathogens | Community pyrogens (S. pneumoniae, S. aureus, gram-negatives) | Defect-specific spectrum + opportunists (PCP, CMV, Aspergillus, mycobacteria, Strongyloides) |
| Inflammatory markers | CRP/procalcitonin rise reliably | May be normal despite overwhelming infection |
| Time to decompensation | Hours | Can be minutes (OPSI, neutropenic Gram-negative shock) |
| Empiric cover | Typical + atypical (one beta-lactam +/- macrolide) | Layered: anti-pseudomonal + antistaphylococcal +/- antifungal +/- antiviral +/- PCP cover |
| Diagnostic sampling | Cultures +/- urinary antigens | Cultures + viral PCRs + galactomannan/beta-D-glucan + parasite serology +/- early BAL |
| Respiratory support | Intubate for failure | Prefer NIV first — lower intubation and mortality in immunocompromised respiratory failure |
| ICU mortality | 10-20% | 30-60%; rises further with neutropenia, transplant, mechanical ventilation |
Types of immunodeficiency and organisms

Neutropenic
Chemotherapy/bone marrow transplant
- Neutrophils <0.5 → Gram-negative (Pseudomonas), Gram-positive (Staph, Strep), fungal (Candida, Aspergillus if prolonged)
- See dedicated neutropenic sepsis topic (81)
- Empiric: piperacillin-tazobactam (anti-pseudomonal)
Cellular (T-cell)
HIV, transplant, steroids
- HIV: PCP, toxoplasmosis, CMV, cryptococcus, mycobacterium avium, mycobacterium tuberculosis
- Transplant (on immunosuppression): CMV, EBV, BK virus, PCP, invasive fungal
- Steroids: PCP, strongyloides hyperinfection, fungal, listeria, legionella
- Empiric: broaden beyond standard — consider adding antiviral, antifungal, PCP cover
Humoral (B-cell)
Myeloma, CLL, splenectomised
- Multiple myeloma, CLL: encapsulated organisms (pneumococcus, Haemophilus)
- Splenectomised/asplenic: OVERWHELMING post-splenectomy infection (OPSI)
- OPSI organisms: Streptococcus pneumoniae (#1), Neisseria meningitidis, Haemophilus influenzae, Capnocytophaga canimorsus (dog bite), Babesia (parasite)
- OPSI: rapid progression, multi-organ failure, DIC, mortality up to 50%
- Empiric: ceftriaxone (cover encapsulated) + vancomycin (if possible MRSA)
Management
Immunocompromised sepsis management
Early broad-spectrum antibiotics (within 1 hour)
Broaden empiric coverage based on immunodeficiency type. Neutropenic: piperacillin-tazobactam. Cellular: add antiviral (acyclovir if HSV/VZV, ganciclovir if CMV), antifungal (echinocandin if prolonged neutropenia or steroids), consider PCP cover (co-trimoxazole if respiratory symptoms + CD4 <200). Humoral/splenectomised: ceftriaxone (cover encapsulated). Add vancomycin if line infection/MRSA.
Aggressive resuscitation
Standard SSC Hour-1 bundle: 30 mL/kg crystalloid, vasopressors for MAP >65, noradrenaline first-line. However: immunocompromised patients may have LESS physiologic reserve — decompensate faster. Consider earlier ICU admission and invasive monitoring.
Extensive diagnostic workup
Blood cultures (multiple sets, from all line lumens + peripheral). Urine, sputum, stool cultures. Viral PCR (CMV, EBV, HSV, VZV, respiratory panel). Beta-D-glucan, galactomannan (fungal). Strongyloides serology (if from endemic area + on steroids). Atypical pathogens: Mycoplasma, Legionella, Chlamydia. Consider bronchoalveolar lavage (BAL) if respiratory failure.
Reduce immunosuppression
Reduce (not stop) immunosuppressive medications if possible. Caution: abrupt cessation may cause rejection (transplant) or flare of underlying disease. Consult transplant/rheumatology. Corticosteroids: may need STRESS DOSE (hydrocortisone 100 mg Q8H) if hypothalamic-pituitary-adrenal axis suppressed.
Source control
Drain infected collections. Remove infected central lines. Debride infected tissue. Treat specific opportunistic infection (CMV: ganciclovir. PCP: co-trimoxazole + steroids if hypoxic. Fungal: echinocandin/amphotericin. Strongyloides: ivermectin + albendazole).
Consider adjunctive therapies
IV immunoglobulin (IVIG) for humoral deficiency. G-CSF for neutropenia. Granulocyte transfusions (rare — severe refractory Gram-negative/fungal sepsis with profound neutropenia). Haematopoietic growth factors. Plasmapheresis (rare — for toxin-mediated or autoimmune complications).
Categories of immunocompromise — the complete defect framework
The single highest-yield exam manoeuvre is to classify the immune defect before prescribing, because the defect predicts the pathogen and the pathogen predicts the therapy. Six categories cover virtually every ICU patient with impaired host defence.[2]
The six categories of immunocompromise — defect, cause, and signature pathogens
| Category | Mechanism / typical cause | Signature bacterial pathogens | Signature opportunists |
|---|---|---|---|
| 1. Neutropenia (ANC <0.5 x 10^9/L, severe <0.1) | Cytotoxic chemotherapy (AML/ALL induction), pre-engraftment HSCT, severe aplastic anaemia, drug-induced agranulocytosis | Pseudomonas aeruginosa (the #1 killer), gram-negative bacilli (ESBL E. coli, Klebsiella, Stenotrophomonas), viridans streptococci (mucositis), coag-neg staph (lines) | Invasive pulmonary aspergillosis, Candida, Mucorales (prolonged neutropenia), HSV reactivation |
| 2. T-cell / cellular deficiency | HIV/ADS, solid-organ or allogeneic HSCT on calcineurin inhibitors, fludarabine/cladribine, alemtuzumab, anti-thymocyte globulin, high-dose steroids | Legionella, Listeria monocytogenes, Nocardia, Salmonella, mycobacteria (TB and NTM) | PCP, CMV, Cryptococcus, endemic mycoses, community respiratory viruses |
| 3. B-cell / humoral deficiency | Multiple myeloma, CLL, post-rituximab, primary antibody deficiency (CVID, XLA), protein-losing states | Encapsulated organisms — S. pneumoniae, H. influenzae, Neisseria | Enterovirus/parechovirus (chronic), Giardia; some PCP risk with severe deficit |
| 4. Complement / terminal-pathway deficiency | Congenital C5-C9 deficiency, eculizumab (anti-C5) for PNH/aHUS/atypical HUS; C3/C4 deficiency | Neisseria (meningococcusaemia — recurrent, fulminant); encapsulated organisms | Pneumococcal and Neisseria bacteraemia; sepsis with low-grade initial signs |
| 5. Splenectomy / functional asplenia | Surgical splenectomy, sickle cell disease (autoinfarction), coeliac disease, post-splenectomy trauma; radiation | Encapsulated — S. pneumoniae (#1), N. meningitidis, H. influenzae, Capnocytophaga canimorsus; Babesia, Plasmodium (parasitaemia uncontrolled) | OPSI — overwhelming, DIC, Waterhouse-Friderichsen, mortality up to 50-70% |
| 6. Biologic / targeted immunotherapy | Anti-TNF (infliximab, adalimumab), anti-CD20 (rituximab), anti-IL-6/IL-17/IL-23, integrin blockers, immune-checkpoint-related immunosuppression for irAEs | TB reactivation (anti-TNF), Legionella, Listeria, Pseudomonas (post-rituximab) | HBV reactivation (rituximab), PCP (anti-TNF), mould, JC virus (natalizumab — PML) |
Pathogen patterns by immune defect — what to cover empirically
Pathogen-to-defect mapping that drives empiric coverage
| Immune defect | Bacteria to cover | Virus to cover | Fungus to cover | Parasite to cover |
|---|---|---|---|---|
| Neutropenia | Anti-pseudomonal beta-lactam +/- vancomycin/linezolid (line, mucositis, MRSA) | HSV/VZV prophylaxis if seropositive | Echinocandin or mould-active azole if persistent fever >4-7 days | — |
| T-cell (HIV) | Standard CAP cover + atypicals; Listeria cover if CNS signs | CMV, HSV, VZV, respiratory viruses | Cryptococcus (serum/CSF CrAg); PCP if CD4 <200 | Toxoplasma (CD4 <100); Strongyloides; Cryptosporidium, Microsporidium |
| T-cell (transplant) | Anti-pseudomonal + Nocardia/Legionella | CMV (esp D+/R-), EBV, BK, adenovirus, respiratory viruses | PCP, Aspergillus, Cryptococcus | Strongyloides if from endemic area |
| B-cell / humoral | Encapsulated — ceftriaxone; + vancomycin if meningitis/possible MRSA | Enterovirus (severe) | — | — |
| Complement / on eculizumab | Meningococcal cover (ceftriaxone +, in fulminant, + penicillin-resistant strains); vaccinate ACWY + B | — | — | — |
| Splenectomy / asplenic | Ceftriaxone empirically (+ vancomycin if meningitis) — encapsulated | — | — | Babesia (clindamycin + azithromycin), malaria cover if exposed |
| Anti-TNF biologic | TB (send GeneXpert); Legionella, Listeria, standard CAP | HBV if at risk | PCP, mould if steroids stacked | Strongyloides if endemic |
| Rituximab | Encapsulated (secondary hypogammaglobulinaemia) + Pseudomonas (late) | HBV reactivation (lamivudine/entecavir prophylaxis), enterovirus | — | — |
The neutropenic patient — the prototype
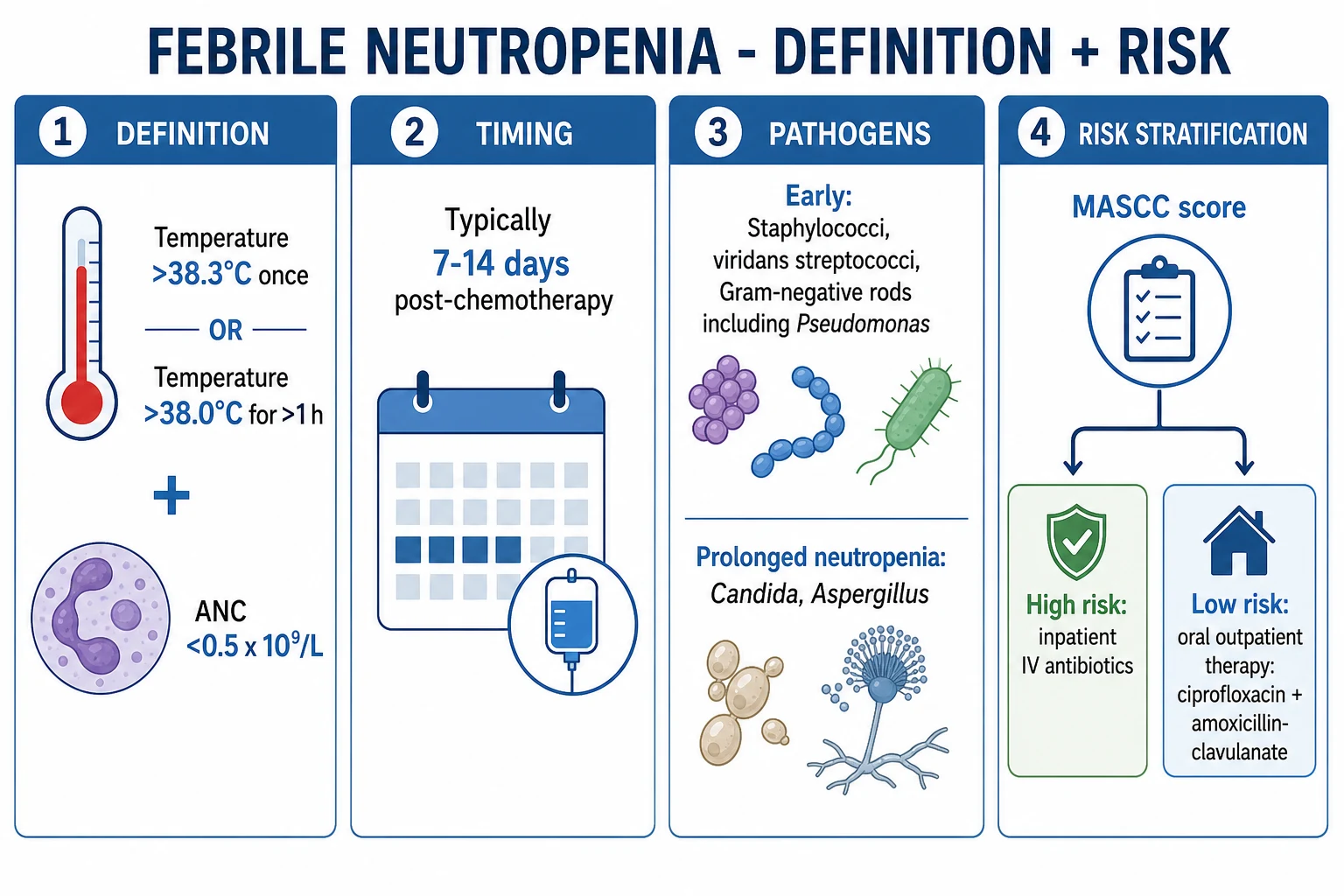
Neutropenia (ANC <0.5 x 10^9/L, or <1.0 and falling) is the highest-volume immunocompromised-sepsis presentation in ICU. The cardinal rule is that fever in a neutropenic patient is a medical emergency — but the corollary is that neutropenic patients can be septic without fever (blunted response), so hypotension, confusion, tachypnoea, or a rising lactate in a cytopenic patient must be treated identically.[3]
- Antipseudomonal beta-lactam within 1 hour — piperacillin-tazobactam 4.5 g IV q6h is first-line; alternatives cefepime 2 g q8h, or meropenem 1 g q8h if ESBL/severe sepsis. Do NOT delay for cultures; draw cultures then dose immediately.
- Add vancomycin/linezolid for suspected line infection, mucositis, MRSA, or haemodynamic instability.
- Persistent fever >4-7 days or recurrent fever after initial defervescence → add empiric mould-active antifungal (voriconazole for Aspergillus; liposomal amphotericin B if Mucorales possible).[7]
- G-CSF shortens neutropenia (controversial survival benefit; consider in profound prolonged neutropenia).
- See the dedicated neutropenic sepsis topic for the full IDSA algorithm.[3]
Cellular (T-cell) deficiency — HIV and transplant
T-cell defects unlock intracellular opportunists. The CD4 count in HIV and the time since transplant are the two predictive levers. [1]
HIV — opportunistic infection risk stratified by CD4 count
| CD4 count (cells/µL) | Infections to anticipate |
|---|---|
| >500 | Community infections only; Kaposi sarcoma if HHV-8 |
| 200-500 | Oral candidiasis, TB (any CD4), bacterial pneumonia, Mycobacterium avium early |
| <200 | PCP (pneumocystis), Toxoplasma gondii (CNS), Cryptococcus, Histoplasma, coccidioidomycosis |
| <100 | Toxoplasmic encephalitis (ring lesions), cryptococcal meningitis |
| <50 | CMV (retinitis, colitis), disseminated MAC, disseminated Strongyloides (if steroid-stressed), progressive multifocal leukoencephalopathy (JC virus) |
The transplant timeline — when each pathogen peaks (Fishman net-state model)
| Period after transplant | Dominant immune defect | Characteristic pathogens |
|---|---|---|
| Month 1 | Neutropenia + mucositis + lines + surgical site | Hospital-acquired: gram-negative bacilli (incl. Pseudomonas), staphylococci, Candida, early Aspergillus, HSV reactivation; donor-derived (rare) |
| Months 1-6 | Cellular immunodeficiency (induction + maintenance IS) | PCP (if no prophylaxis), CMV, Aspergillus, Nocardia, Cryptococcus, adenovirus, HHV-6 |
| Beyond 6 months | Partial immune reconstitution | Community-acquired (S. pneumoniae, H. influenzae) + recurrent opportunists if rejection/GVHD needs intensified immunosuppression |
Humoral (B-cell) deficiency
Multiple myeloma and CLL are the classic ICU presentations; both impair antibody quantity and quality, and both frequently follow rituximab or are themselves treated with it. The defect is against encapsulated organisms because opsonisation fails. Empiric cover = a third-generation cephalosporin (ceftriaxone); add vancomycin if meningitis or possible MRSA. Consider IVIG for secondary hypogammaglobulinaemia in recurrent infection.[2]
Complement and terminal-pathway deficiency
Congenital deficiency of C5-C9 (the membrane attack complex) and pharmacological blockade with the anti-C5 monoclonal eculizumab/ravulizumab (used in PNH, atypical HUS, refractory myasthenia and NMOSD) cripple killing of Neisseria — these patients suffer recurrent or fulminant meningococcaemia and must be vaccinated (conjugate MenACWY + MenB) and on penicillin prophylaxis. In an asplenic/eculizumab patient presenting septic, cover Neisseria empirically (ceftriaxone; add a second agent in refractory shock) and notify the lab — the organism may be non-groupable.[4]
Splenectomy / asplenia and overwhelming post-splenectomy infection (OPSI)
Functional or anatomical asplenia removes the spleen's filtering, opsonin (tuftsin/properdin) production, and IgM-memory-B-cell response to encapsulated organisms. The lifetime risk of OPSI is ~5%, and once it declares it progresses from fever to multi-organ failure and death within hours, with mortality 38-70% even in ICU.[4]
OPSI — the exam-answer framework
| Feature | Detail |
|---|---|
| Top organism | Streptococcus pneumoniae (50-90% of cases); then N. meningitidis, H. influenzae type b |
| Other classic organisms | Capnocytophaga canimorsus (dog/cat bite — can be fatal within hours), Salmonella, Babesia microti (parasitaemia), Plasmodium |
| Presentation | Non-specific prodrome (fever, rigors, myalgia, vomiting/vague abdominal pain) → fulminant septic shock + Waterhouse-Friderichsen (adrenal haemorrhage) + DIC + purpura fulminans |
| Empiric therapy | Ceftriaxone 2 g IV (+ vancomycin if meningitis/meningococcaemia with beta-lactam allergy); add clindamycin to suppress pneumococcal toxin in purpura fulminans; adalumumab/IVIG considered |
| Prevention (the audit point) | Vaccinate (pneumococcal, MenACWY + MenB, Hib) ideally >2 weeks pre-elective splenectomy; lifelong penicillin V prophylaxis; patient-held emergency antibiotics; alert bracelet; rabid patient education ("fever = emergency"). Sickle cell and coeliac patients are functionally asplenic — apply the same standards.[4] |
Biologic and targeted immunotherapy
Biologic agents and their infection signatures
| Agent class | Example | Characteristic infection risk |
|---|---|---|
| Anti-TNF-alpha | Infliximab, adalimumab, etanercept | TB reactivation (often disseminated/extrapulmonary), HBV reactivation, Legionella, Listeria, Salmonella, fungal (PCP, histoplasmosis) |
| Anti-CD20 | Rituximab, obinutuzumab | HBV reactivation (fatal — pre-screen and prophylax with entecavir/lamivudine), late Pseudomonas/encapsulated bacteraemia from secondary hypogammaglobulinaemia, enterovirus, JC virus |
| Anti-IL-6 / IL-17 / IL-23 / integrin | Tocilizumab, secukinumab, ustekinumab, vedolizumab | Increased GI/perforation-related sepsis; natalizumab → PML (JC virus); modest bacterial/fungal risk |
| Anti-C5 | Eculizumab, ravulizumab | Fulminant meningococcaemia (see complement section) |
| CD38 / SLAMF7 | Daratumumab (myeloma), elotuzumab | Secondary hypogammaglobulinaemia — encapsulated organisms; interfere with blood-typing crossmatch |
| Checkpoint inhibitors (the inverse — cause autoimmunity) | Nivolumab, pembrolizumab | Patients are usually immunocompetent for infection, but treatment of severe irAEs with high-dose steroids/infliximab renders them iatrogenically immunocompromised — then apply the steroid/anti-TNF risk above |
The 1-hour rule and timing of antibiotics
The SSC Hour-1 bundle applies unchanged to the immunocompromised host — indeed the evidence for urgency is even stronger, because these patients decompensate faster and because each hour of delay in appropriate therapy multiplies mortality.[1]
The first hour — what must happen
0-15 min — measure lactate, blood cultures x2 (peripheral + every lumen), start broad empiric antibiotics
Do NOT delay antibiotics for cultures. The yield of cultures taken <1 h after antibiotics is still acceptable, but the cost of delayed antibiotics in neutropenia/transplant sepsis is death. Antibiotics within 1 hour is the hard target.
15-45 min — resuscitate: 30 mL/kg crystalloid, noradrenaline to MAP >65
Immunocompromised hosts have less reserve — earlier vasopressors and invasive monitoring. Cap refill, lactate clearance guide further fluid. Avoid fluid overload (transplant/marrow-failure patients often have low oncotic pressure + cardiac comorbidity).
Within 1 h — broad-spectrum, defect-tailored antibiotics administered
Neutropenic: anti-pseudomonal beta-lactam. T-cell/HIV/transplant: add antiviral (ganciclovir if CMV), antifungal (echinocandin/mould-active azole), PCP cover (co-trimoxazole if CD4 <200 + respiratory). Humoral/splenic: ceftriaxone. Complement/asplenic: ceftriaxone + consider *Neisseria* cover. Add vancomycin/linezolid for line, mucositis, MRSA.
1-6 h — opportunistic work-up sent
Beta-D-glucan, galactomannan; CMV/EBV/HSV/VZV/respiratory virus PCR; *Strongyloides* serology (before steroids in endemic patients); urinary Legionella/pneumococcal antigen; *Cryptococcus* CrAg; imaging (CT chest/abdo); early BAL if respiratory failure.
6-24 h — source control and ID consult
Drain/remove lines/debride as needed (see source-control challenges). Contact infectious diseases, haematology/transplant, and clinical microbiology early — drug interactions (azole + calcineurin inhibitor), antifungal/antiviral dosing, and de-escalation all require specialist input.
Empiric antibiotic approach — broader than standard
Standard CAP sepsis cover (one beta-lactam +/- macrolide) is inadequate in the immunocompromised host. Build the regimen by layering onto an antipseudomonal backbone according to the defect and the syndrome — then de-escalate within 48-72 h as diagnostics return.[2][3]
Layered empiric therapy by suspected syndrome
| Backbone (always) | Add when... | Agent(s) to add |
|---|---|---|
| Antipseudomonal beta-lactam (pip-tazo 4.5 g q6h, cefepime 2 g q8h, or meropenem 1 g q8h) | Line infection, mucositis, MRSA, shock | Vancomycin or linezolid (linezolid preferred if VRE/renal; both cover MRSA) |
| + backbone | Persistent neutropenic fever >4-7 d, halo sign, positive galactomannan | Mould-active antifungal — voriconazole (first-line Aspergillus), isavuconazole, or liposomal amphotericin B (if Mucorales possible). Echinocandin (caspofungin) if Candida more likely[7][9] |
| + backbone | T-cell defect/steroids + diffuse ground-glass + hypoxaemia | Co-trimoxazole (high-dose, TMP 15-20 mg/kg/day) ± adjunctive steroids (prednisone 40 mg BD) for severe PCP (PaO2 <70)[8] |
| + backbone | 1-4 months post-SOT/HSCT, rising CMV PCR, diffuse infiltrates | Ganciclovir 5 mg/kg IV q12h (renally adjust); add IVIG in severe CMV |
| + backbone | Mucositis, HSV/VZV seropositive, dermatomal rash | Aciclovir 5 mg/kg IV q8h (HSV/VZV); valganciclovir if CMV |
| + backbone | Influenza/RSV/paraflu on respiratory panel | Oseltamivir (influenza, give even >48 h in immunocompromised); ribavirin for RSV in HSCT |
| + backbone | Humoral/splenic/complement defect | Ceftriaxone 2 g IV (encapsulated/Neisseria); + vancomycin if meningitis |
| + backbone | Endemic-area patient about to receive steroids | Empiric ivermectin (200 mcg/kg x2 doses) if Strongyloides hyperinfection suspected |
Atypical coverage (intracellular organisms — Legionella, Mycoplasma, Chlamydia) is added with a macrolide or respiratory fluoroquinolone when T-cell defects, anti-TNF therapy, or a compatible syndrome (hyponatraemia, diarrhoea, confusion, hepatitis) raise the possibility.[2]
Source control challenges
Source control in the immunocompromised host is harder and higher-stakes: thrombocytopenia and coagulopathy complicate drainage and surgery; neutropenic gut mucositis and graft-versus-host disease blur infection with non-infective transmural inflammation; the patient cannot mount an abscess wall, so collections are often ill-defined; and stopping immunosuppression risks graft rejection or GVHD. [1]
Source-control problems and how to solve them
| Source / problem | Challenge | Practical solution |
|---|---|---|
| Central line | Most neutropenic/transplant patients are line-dependent; removal threatens access | Remove infected tunnelled lines (clinical sepsis, tunnel/pocket infection, S. aureus/Pseudomonas/Candida bacteraemia); exchange over wire only if no alternative and stable. Antibiotic lock for uncomplicated line bacteraemia |
| Neutropenic enterocolitis (typhlitis) | Right-lower-lobe bowel-wall thickening; can perforate; platelets preclude surgery | Bowel rest, NGT, broad-spectrum anaerobic cover (meropenem + metronidazole); surgery only for perforation/refractory bleeding; transfuse platelets to >50 before any procedure |
| Invasive fungal sinus/lung disease | Angioinvasion → thrombosis → drug penetration failure; surgery risks thrombocytopenia | Urgent surgical debridement is mandatory for Mucorales and refractory Aspergillus (medical therapy alone fails); correct platelets/coagulopathy pre-op; liposomal amphotericin B high-dose |
| Perianal infection (haematology) | Rapid necrosis; pain out of proportion; surgical debridement vs neutropenia | Broad-spectrum anaerobic + Gram-negative cover; do not perform DRE; early surgical review; debridement deferred until count recovery only if localised/non-necrotising |
| Catheter/abdominal collections | Thrombocytopenia limits percutaneous drainage | Transfuse platelets to >50 and correct INR; image-guided drainage preferred over open surgery; interventional radiology central to the team |
| CNS toxoplasmosis / abscess | Brain biopsy risk vs diagnostic certainty | Empiric anti-toxoplasma therapy if ring lesions + CD4 <100 + seropositive; biopsy if atypical or non-responsive at 2 weeks |
Diagnostic work-up
Sample everything, from every site, early. The diagnosis in immunocompromised sepsis is rarely made on clinical grounds alone, and the empiric regimen is deliberately broad precisely because the pathogen cannot yet be named. [1]
The diagnostic panel for immunocompromised sepsis
| Sample / test | Detects | Notes |
|---|---|---|
| Blood cultures x2-3 + every line lumen | Bacteraemia, fungaemia; line-vs-systemic infection (differential time to positivity) | Before antibiotics if possible, but never delay therapy; mycobacterial blood cultures if transplant/HIV |
| Urinalysis + culture | Urinary source; Candida | Sterile pyuria in neutropenia does not exclude UTI |
| Stool (C. difficile PCR, culture, ova/cysts/parasites, Crypto/Microsporidium) | Diarrhoeal source | C. difficile common after broad antibiotics/chemo |
| Respiratory virus PCR | Influenza, RSV, paraflu, adenovirus, metapneumo, SARS-CoV-2 | Send on ALL immunocompromised with respiratory signs |
| CMV/EBV/HSV/VZV/BK PCR | Reactivated herpesviruses | Quantitative; syndrome correlation required (shedding ≠ disease) |
| Serum galactomannan | Invasive aspergillosis (screen in neutropenia) | OD index >=0.5 twice; false-positive with pip-tazo (historically), mucositis |
| Serum (1->3)-beta-D-glucan | PCP, broad fungal | >=80 pg/mL positive; NEGATIVE in Cryptococcus and Mucorales |
| BAL (early, 24-48 h) | Full panel: bacterial/fungal/AFB culture, galactomannan, beta-D-glucan, CMV PCR + cytology, PCP PCR, Nocardia, respiratory virus | Highest-yield single test for pulmonary infiltrates of unclear cause; transfuse platelets >50 first |
| CSF (if no coagulopathy/raised ICP) | Meningitis/encephalitis — bacterial, cryptococcal (CrAg), viral (HSV/enterovirus/CMV), AFB | Strongyloides and Toxoplasma serology; neuroimaging first if focal signs |
| Strongyloides serology | Past exposure (hyperinfection risk if steroids given) | Send BEFORE high-dose steroids in any endemic-area patient; treat with ivermectin |
| CT chest + abdomen/pelvis | Source; halo sign (Aspergillus), reversed halo (Mucor/PCP), typhlitis, collections | CT chest is more sensitive than CXR early; abdominal CT for typhlitis/collections |
Biomarkers and their limits
CRP and procalcitonin may be normal in neutropenic and steroid-treated patients despite overwhelming infection — a normal value must never reassure. The fungal biomarkers (galactomannan, beta-D-glucan) are powerful but each has a critical failure mode the exam tests.[7]
Biomarker pitfalls in the immunocompromised host
| Marker | What it detects | Key limitation / pitfall |
|---|---|---|
| CRP | Acute inflammation | Blunted by neutropenia, steroids, uraemia; can be normal in fatal sepsis |
| Procalcitonin | Bacterial infection | Falsely low with severe immunosuppression; rises with steroids; not reliable to withhold antibiotics here |
| Galactomannan (serum/BAL) | Aspergillus cell-wall antigen | BAL >=1.0 highly specific; serum >=0.5 screen. False-positive (pip-tazo historically, gut translocation, Penicillium/Histoplasma). Does not detect Mucorales |
| (1->3)-beta-D-glucan | Broad fungal + PCP | Negative in Cryptococcus and Mucorales (no beta-D-glucan in their cell wall). False-positive with albumin/immunoglobulin, haemodialysis, gauze exposure |
| LDH | Non-specific tissue injury | Very high in PCP; also in malignancy, PE, haemolysis |
| CrAg (serum/CSF) | Cryptococcus | Positive in serum with dissemination; CSF CrAg + India ink for meningitis |
Non-infectious mimics — do not escalate antibiotics blindly
Up to a quarter of immunocompromised patients with "sepsis" and pulmonary/constitutional syndromes have a non-infectious cause; reflexively broadening antibiotics for a deteriorating patient with a non-infective process is a classic fatal error. Reaching for the BAL/CT and the drug history (not another antibiotic) is the correct move.[2]
Non-infectious mimics of sepsis in the immunocompromised
| Mimic | Clue | Action |
|---|---|---|
| Drug-induced pneumonitis | Bleomycin, busulfan, methotrexate, checkpoint inhibitors; temporal relationship | BAL cytology (lymphocytic/eosinophilic), stop offending drug, steroids |
| Engraftment syndrome / diffuse alveolar haemorrhage | Around neutrophil recovery post-HSCT; bloody BAL | Supportive; steroids for DAH; transfuse platelets |
| Graft-versus-host disease of gut/lung | Allogeneic HSCT; rash, diarrhoea, cholestasis | Biopsy; intensify or adjust immunosuppression |
| Tumour lysis / leukaemic/lymphomatous infiltrates | Cytopenias, high LDH, high urate; nodular/diffuse infiltrates | Cytoreduction, rasburicase, hydration |
| Check-point inhibitor adverse events | Recent ICI; pneumonitis, colitis, hepatitis, hypophysitis, myocarditis | High-dose steroids, infliximab/mycophenolate; rule out infection first |
| Transfusion-related / volume overload / TRALI | Peri-transfusion; bilateral infiltrates | Diurese, supportive; exclude infection |
| Pulmonary embolism / infarction | Hypercoagulability of malignancy, asplenia | CTPA; anticoagulate |
Adjunctive and supportive therapy
Adjunctive therapies in immunocompromised sepsis
| Therapy | Indication | Rationale / dose |
|---|---|---|
| Stress-dose hydrocortisone | Septic shock + chronic steroid use (HPA-axis suppression) | Hydrocortisone 50 mg IV q6h (or 100 mg q8h) until shock resolves — these patients cannot mount a cortisol response |
| Adjunctive steroids | Severe PCP (PaO2 <70 or A-a gradient >35) | Prednisone 40 mg BD x5d → 40 mg OD x5d → 20 mg OD to day 21; reduces inflammatory lung injury at organism lysis[8] |
| G-CSF / GM-CSF | Profound prolonged neutropenia | Shortens neutropenia; survival benefit uncertain; consider in profound (<0.1) prolonged neutropenia and invasive fungal disease |
| IVIG | Humoral deficiency (CVID, myeloma), severe enterovirus, toxin-mediated | Replacement dosing for hypogammaglobulinaemia (IgG trough <4 g/L) |
| Granulocyte transfusion | Refractory gram-negative/fungal sepsis + profound neutropenia not recovering | Rare; HLA-matched donors; transient; risks (TRALI, alloimmunisation) |
| CMV-specific / donor lymphocytes | Refractory CMV post-HSCT | Adoptive T-cell therapy for drug-resistant CMV |
| Anti-toxin therapy | Purpura fulminans / TSS (pneumococcal, staphylococcal) | Clindamycin (suppress toxin), IVIG; source control |
| Plasma exchange | TTP/HUS, toxin-mediated, fulminant autoimmune | Rare; specific indications only |
Respiratory support — prefer NIV over intubation
Immunocompromised patients who require intubation have disproportionately high mortality; the landmark RCTs (Hilbert 2001, Antonelli 2000) showed that early NIV reduced intubation rates and improved survival in immunocompromised patients with pulmonary infiltrates and hypoxaemic respiratory failure. Reach for the BiPAP mask before the laryngoscope — but recognise NIV failure (rising PaCO2, falling pH, exhaustion, copious secretions, shock, altered consciousness) and intubate without delay.[5][6]
Respiratory support ladder
| Strategy | Indication | Rationale / caution |
|---|---|---|
| HFNC | Moderate hypoxaemia, cooperative | Comfortable, permits pulmonary toilet; reasonable first step |
| NIV (CPAP/BiPAP) | PaO2/FiO2 <300, pulmonary infiltrates | First-line — reduces intubation and mortality in immunocompromised ARF. Contraindicated if airway unprotected, copious secretions, agitation, shock, severe acidosis |
| Invasive ventilation | NIV failure, airway/shock, severe ARDS | High mortality (40-60%); lung-protective (Vt 6 mL/kg, Pplat <30), prone for severe ARDS, consider V-V ECMO |
Reduce the "net state of immunosuppression"
No antimicrobial regimen cures an infection in a patient whose immune suppression stays maximal (Fishman's central concept). Where feasible, taper steroids, lower calcineurin-inhibitor targets, and interrupt biologics — always in dialogue with the transplant/haematology team to balance against graft rejection and GVHD. This is the single most important host-side manoeuvre.[2]
Prognosis
Mortality by host factor and pathogen in immunocompromised sepsis
| Factor / pathogen | ICU mortality | Comment |
|---|---|---|
| Overall immunocompromised sepsis | 30-50% | 2-3x immunocompetent sepsis |
| Neutropenic sepsis (appropriate early therapy) | 10-20% | Halved by antibiotics within 1 h; rises with delay |
| Invasive pulmonary aspergillosis (neutropenia) | 40-60% | Improved by early voriconazole; rises with dissemination |
| Mucormycosis | 50-80% | Needs surgery + amphotericin |
| CMV disease (HSCT) | 30-50% | Worse in D+/R- mismatch, ganciclovir resistance |
| OPSI (asplenic) | 38-70% | Minutes-to-hours progression; prevention is key |
| Need for mechanical ventilation | 40-70% | Strongest single poor-outcome marker — argues for early NIV |
| Delayed appropriate therapy | 2-3x higher | Driven by failure to broaden cover or obtain early diagnostics |
The most powerful modifiable prognostic factor is early, appropriate, pathogen-directed therapy, contingent on early invasive diagnosis. Host factors that compound mortality are prolonged profound neutropenia, high-intensity immunosuppression (GVHD, recent T-cell depletion), mechanical ventilation, multi-organ failure, and the underlying malignancy/transplant status.[1][2]
Key trials and evidence
Surviving Sepsis Campaign 2021 — sepsis in special populations (Evans L, et al. PMID 33529977)
Source
Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign International Guidelines 2021. Intensive Care Med 2021;47(11):1181-1247
Key principle 1
The Hour-1 bundle (lactate, blood cultures, broad-spectrum antibiotics, 30 mL/kg crystalloid, vasopressors) applies to immunocompromised patients — urgency is greater, not less
Key principle 2
Stress-dose corticosteroids recommended for septic shock with ongoing vasopressor requirement; essential if chronic steroid use has suppressed the HPA axis
Key principle 3
Empiric antimicrobial choice must account for atypical/opportunistic pathogens and local resistance; broaden, then de-escalate on microbiology
Clinical bottom line
The framework for sepsis in 'special populations' — neutropenic, transplant, HIV, asplenic — that governs the approach in this topic
Hilbert 2001 — NIV in immunosuppressed patients with pulmonary infiltrates (PMID 11172189)
Source
Hilbert G, Gruson D, Vargas F, et al. N Engl J Med 2001;344:481-487. RCT, 52 immunosuppressed patients with pulmonary infiltrates, fever, acute respiratory failure
Key result 1
Early NIV reduced the need for endotracheal intubation (12/26 vs 20/26; P=0.03)
Key result 2
Reduced serious complications (P=0.02) and ICU mortality (10/26 vs 18/26; P=0.03)
Clinical bottom line
The trial underpinning the 'NIV before intubation' rule in immunocompromised hypoxaemic respiratory failure
Antonelli 2000 — NIV in solid-organ transplant recipients with ARF (PMID 10647766)
Source
Antonelli M, Conti G, Bufi M, et al. JAMA 2000;283:235-241. RCT, 40 SOT recipients with hypoxaemic acute respiratory failure
Key result 1
NIV reduced intubation rate (20% vs 70%; P=0.002) and ICU mortality (20% vs 50%; P=0.05)
Key result 2
Fewer ventilator-associated pneumonias and shorter ICU stay in the NIV group
Clinical bottom line
Confirms, in transplant recipients specifically, that early NIV improves outcome — avoid intubation where possible
Herbrecht 2002 — voriconazole vs amphotericin B for invasive aspergillosis (PMID 12396811)
Source
Herbrecht R, Denning DW, Patterson TF, et al. N Engl J Med 2002;347:408-415. RCT, 277 patients with invasive aspergillosis
Key result 1
Voriconazole improved survival at 12 weeks (70.8% vs 57.9%; P=0.05) and response rates
Key result 2
Voriconazole was better tolerated and is now first-line therapy for invasive pulmonary aspergillosis
Clinical bottom line
Established voriconazole as first-line for invasive aspergillosis in neutropenia/transplant — the flagship mould in immunocompromised sepsis
IDSA 2016 Aspergillosis guidelines — Patterson TF, et al. (PMID 27365388)
Source
Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update. Clin Infect Dis 2016;63(4):e1-e60
Key principle 1
Voriconazole is first-line therapy; isavuconazole and liposomal amphotericin B are alternatives. Therapeutic drug monitoring of voriconazole (trough 1-5.5 mg/L) is essential
Key principle 2
Diagnosis combines host factors + clinical features + mycological evidence (galactomannan, culture/histology)
Clinical bottom line
Defines the diagnostic-treatment framework for invasive aspergillosis — a leading opportunist in neutropenic and transplant sepsis
ECIL-5 — PCP in haematological malignancy and HSCT (Cordonnier C, et al. PMID 27550990)
Source
Cordonnier C, Cesaro S, Maschmeyer G, et al. Fifth European Conference on Infections in Leukaemia (ECIL-5). J Antimicrob Chemother 2016;71(9):2386-2393
Key principle 1
PCP carries 30-60% mortality in non-HIV immunocompromised hosts — higher than in HIV
Key principle 2
Universal co-trimoxazole prophylaxis for at-risk patients is the single most effective preventive measure
Key principle 3
Adjunctive steroids in severe PCP (PaO2 <70) reduce mortality from inflammatory lung injury at organism lysis
Clinical bottom line
Treat clinically-suspected PCP immediately (do not wait for confirmation); prophylaxis adherence is the audit point
IDSA febrile-neutropenia guideline 2011 — Freifeld AG, et al. (PMID 21205790)
Source
Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update. Clin Infect Dis 2011;52(4):e56-e93
Key principle 1
All febrile neutropenic patients receive prompt broad-spectrum empiric therapy covering gram-negative (incl. Pseudomonas) and gram-positive pathogens
Key principle 2
Risk-stratify high vs low risk to guide setting (inpatient vs outpatient) and duration of therapy
Clinical bottom line
The reference standard for neutropenic sepsis empiric therapy — antipseudomonal beta-lactam within 1 hour
BCSH asplenia guideline — Davies JM, et al. (PMID 21988145)
Source
Davies JM, Lewis MP, Wimperis J, et al. Review of guidelines for the prevention and treatment of infection in patients with an absent or dysfunctional spleen. Br J Haematol 2012;155(3):308-317
Key principle 1
Lifelong risk of overwhelming post-splenectomy infection (OPSI) — pneumococcus dominant, mortality 38-70%
Key principle 2
Three prevention pillars: vaccination (pneumococcal, MenACWY + MenB, Hib), antibiotic prophylaxis (penicillin V), and patient education with emergency antibiotics and alert bracelet
Clinical bottom line
In asplenic/eculizumab patients presenting septic, give ceftriaxone empirically without waiting — minutes matter
SAQ — Asplenic sepsis (OPSI) and immunocompromised respiratory failure
SAQ — Overwhelming post-splenectomy infection in an asplenic patient
10 minutes · 10 marks
A 56-year-old man presents to the ED with a 6-hour history of fever, rigors, myalgia and vomiting. He had a splenectomy 4 years ago following trauma. He is confused, BP 78/40, HR 132, RR 32, SpO2 93% on room air, and has widespread purpuric skin lesions. Lactate 6.2 mmol/L, INR 2.1, platelets 34 x10^9/L. A peripheral smear shows gram-positive diplococci. He takes penicillin V prophylaxis intermittently and has no written record of vaccination.
SAQ — Hypoxaemic respiratory failure in a renal transplant recipient
10 minutes · 10 marks
A 48-year-old woman, 4 months after deceased-donor kidney transplant on tacrolimus, mycophenolate and prednisone 10 mg daily, is admitted with a 5-day history of progressive dyspnoea, dry cough and fever 38.4C. She is hypoxaemic (SpO2 88% on room air, PaO2 54 mmHg on 6 L nasal prongs), with bilateral diffuse ground-glass infiltrates on CT chest. LDH 780 U/L, beta-D-glucan positive at 230 pg/mL, serum galactomannan negative. CRP 42, procalcitonin 0.3. She has not had CMV PCR sent.
Clinical pearls
Red flags
Deeper-dive clinical pearls — the second fourteen
Additional red flags
[1]References
- [1]Evans L, Rhodes A, Alhazzani W, et al. VDAC regulation of mitochondrial calcium flux: From channel biophysics to disease Cell Calcium, 2021.PMID 33529977
- [2]Geerlinks FG, et al. Notum palmitoleoyl-protein carboxylesterase regulates Fas cell surface death receptor-mediated apoptosis via the Wnt signaling pathway in colon adenocarcinoma Bioengineered, 2021.PMID 34402722
- [3]Freifeld AG, Bow EJ, Sepkowitz KA, et al. Regulation of cofilin phosphorylation and asymmetry in collective cell migration during morphogenesis Development, 2011.PMID 21205790
- [4]Davies JM, Lewis MP, Wimperis J, et al. Review of guidelines for the prevention and treatment of infection in patients with an absent or dysfunctional spleen: prepared on behalf of the British Committee for Standards in Haematology by a working party of the Haemato-Oncology task force Br J Haematol, 2011.PMID 21988145
- [5]Hilbert G, Gruson D, Vargas F, et al. Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure N Engl J Med, 2001.PMID 11172189
- [6]Antonelli M, Conti G, Bufi M, et al. Does treatment with antenatal glucocorticoids for the risk of premature delivery contribute to ketoacidosis in pregnant women with diabetes who receive continuous subcutaneous insulin infusion (CSII)? Arch Intern Med, 2000.PMID 10647766
- [7]Patterson TF, Thompson GR 3rd, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America Clin Infect Dis, 2016.PMID 27365388
- [8]Cordonnier C, Cesaro S, Maschmeyer G, et al. Pneumocystis jirovecii pneumonia: still a concern in patients with haematological malignancies and stem cell transplant recipients J Antimicrob Chemother, 2016.PMID 27550990
- [9]Herbrecht R, Denning DW, Patterson TF, et al. Cost effectiveness: pro the value of economic information in medical decision-making Amyotroph Lateral Scler Other Motor Neuron Disord, 2002.PMID 12396811